
Abstract
Introduction
Congenital malformations of the right atrium—aneurysms and diverticula
Topic Description
Although each of these anomalies is well known, there are still significant discrepancies in diagnosis. At the same time, there is no essential difference in the postnatal management of patients with right atrial aneurysms or diverticula. Treatment mode varies between centers and is selected individually depending on the presence of symptoms.
Discussion
We discuss the problems of terminology, ultrasound criteria and prenatal differential diagnosis, anatomic and histological features and current limitations for the accurate diagnosis of right atrial aneurysms and diverticula in utero. As a clinical example, we describe a case of right atrial appendage aneurysm diagnosed in a fetus.
Conclusions
Considering the prenatal diagnostic difficulties and similar management of such patients after birth, we suggest avoiding the use of exact terms in the fetus, leaving the precise diagnosis for the postnatal period.
Keywords
Introduction
Congenital right atrial (RA) aneurysm is a rare heart defect originating from the free atrial wall or the RA appendage. 1 The true frequency and the natural course of RA aneurysm remain unclear. It is found in all age groups including fetuses but most cases are diagnosed in the third or fourth decades of life. Many individuals have no clinical signs. This anomaly is often revealed as an incidental finding during cardiac imaging, autopsy or cardiac surgery performed for other reasons. Among those who have symptoms, the clinical manifestations are variable and nonspecific and include arrhythmia, palpitations, chest pain, shortness of breath and fatigue. Early diagnosis of this anomaly is extremely important because of serious complications such as supraventricular arrhythmia, thrombosis and sudden death.1–3
With advancing ultrasound technologies, cases of RA aneurysm diagnosis in children are increasing. However, cases of prenatal diagnosis of this pathology still remain the exception.4–8
Prenatal diagnosis
Timely prenatal diagnosis aids patient management including the place for birth, mode of delivery and the planning of appropriate medical care for the newborn. It is possible in the early second trimester; 9 however, half of the RA aneurysm cases are detected during a third trimester scan. Commonly, it is the only finding; however, fetal hydrops has been described in some cases.7,10
RA aneurysm can be attributed to the congenital malformations of the right atrium (CMRA) which also include RA diverticula. Ultrasound diagnosis of CMRA is based on the identification of the isolated enlarged RA or its appendage in the absence of additional cardiac lesions. Differential diagnosis includes cor triatriatum dexter, tricuspid or pulmonary valve pathology, presence of intracardiac shunts and other conditions with RA dilatation. 11 The most common malformation from which CMRA should be differentiated is Ebstein’s anomaly, where cardiomegaly, disproportional RA enlargement and reduction of the right ventricular cavity can also be observed. 10
Differential diagnosis between the forms of CMRA—aneurysm and diverticulum—is a more challenging task, which must start with a clear understanding of the definitions.
Aneurysm or diverticulum—Definitions
According to the commonest definitions, aneurysm is a broad base dilatation of the atrium wall, while diverticulum is a saccular structure that has a narrow entry (ostium) into the atrium. 12 In practice, these differences appear to be blurred as these terms are often used interchangeably. In the most extensive review of patients with RA pathology presented by Binder et al., CMRA are divided into RA dilatation, single and multiple diverticula. 11 Malik et al. refer to the congenital RA anomalies cor triatriatum, Ebstein’s anomaly and RA aneurysm and do not use the term “diverticulum”. 13 Morrow et al. use both of them—“aneurysm (diverticulum)”. 14 Additionally, there are terms “idiopathic RA dilatation” and “congenital enlargement of the RA”, which are synonymous with “RA aneurysm”; 15 however, some authors use them as a synonym for “diverticulum”. 16
Aneurysm or diverticulum—Histology
The histological description sometimes does not correspond to the term used in the publication. Aneurysms tend to be fibrous with a few or even absent muscle fibers when compared with the three normal layers (endocardium, myocardium and pericardium) of diverticula.5,6,17 However, similar characteristics can be found in publications about RA diverticula with the point of view that it is the diverticulum that does not contain all layers of the atrial wall, since it connects to the RA through a defect in its thinned free wall or atrial appendage.18–20 There is also opinion that congenital aneurysms may represent the “fibrous diverticula”. 21
Aneurysm or diverticulum—Ultrasound criteria
Aneurysmal dilatation of the RA usually has wide communication with the right atrium and thin walls. There is often one chamber, representing dilated RA, its appendage with the part of RA or both. Diverticulum-type dilatation is characterized by the presence of the narrow ostium. Usually two chambers of the RA can be seen—the RA itself, which could be of normal size, and pathological outpouching represents the diverticulum. The size of the cavity does not play an important role in the differential diagnosis.
Contractility of the outpouching could be an additional diagnostic marker. Contraction of the complete outpouching (not only the neck/ostium area) simultaneously with the true chamber indicates that it is a diverticulum. In the case of paradoxical contractions or absence of contractile activity, an aneurysm has to be considered. 17
Aneurysm or diverticulum—In practice
Nevertheless, prenatal differential diagnosis of CMRA forms still remains a difficult task which is clearly demonstrated by our clinical example (with patient consent and Local Ethics Committee approval).
A 22-year-old primigravida with non-contributive history was referred to our department at 20.4 gestational weeks due to the RA anomaly.
The diagnostic algorithm included an assessment of the heart chambers, atrioventricular valves, outflow tracts and systemic and pulmonary venous connections. Particular attention was paid to the heart rate and rhythm, myocardial thickness and contractility as well as the presence of regurgitation of the valves. A thorough assessment of the other organs and systems was performed to identify extracardiac malformations, vascular shunts, tumors and signs of hydrops or heart failure. For the pathological outpouching, its location, size, the presence of the ostium and contractile activity were noted.
The fetal heartbeat was rhythmic. The RA communicated with a thin-walled chamber through the clearly visible ostium. This outpouching was similar in size to the left ventricle and compressed the right ventricle. The sizes of the atria were comparable. No distinct RA appendage was seen. Otherwise, the anatomy of the heart chambers, atrioventricular valves and great arteries was normal without signs of intracardiac thrombus (Figure 1, Video 1). There was no restriction of right ventricular inflow or outflow. The walls of the abnormal cavity contracted rhythmically but non-synchronous with atria or ventricles (Videos 1 and 2). No other cardiac malformations or extracardiac anomalies were seen.

Fetal ultrasound at 20.4 weeks gestation. Right atrial appendage aneurysm (*) on different cardiac views. (a) Note the narrow connection of the pathological outpouching with the right atrium (arrow) and compressed right ventricle. (b) Note the thin wall of the aneurysm (white arrow) and the size of the abnormal chamber comparing with the atria and ventricles. RA: right atrium; LA: left atrium; LV: left ventricle; RV: right ventricle.
The precise diagnosis in this case was difficult. An additional contracting chamber with a narrow ostium characterized our finding as a diverticulum but paradoxical contractions and the thin walls of the cavity allowed us to classify it as an aneurysm.
The final diagnosis, RA appendage aneurysm, was made after birth using echocardiography and computed tomographic angiography (Figure 2). Postnatal clinical signs included dyspnea and fatigability. On the 10th day of life, the neonate developed tachycardia (up to 188 bpm) without rhythm disturbance. Surgical treatment was performed on the 15th day of life after the onset of ventricular hypocontractility and circulatory deficiency. RA appendage plasty, opening and plication of the aneurysm walls, was performed. Histological data confirmed the diagnosis. A month after the operation, the infant’s condition was satisfactory. The girl has since been under cardiologist observation and received antiarrhythmic therapy due to the first signs of Wolff-Parkinson-White syndrome. A year later, she is thriving without drug treatment and has no physical activity limitations.
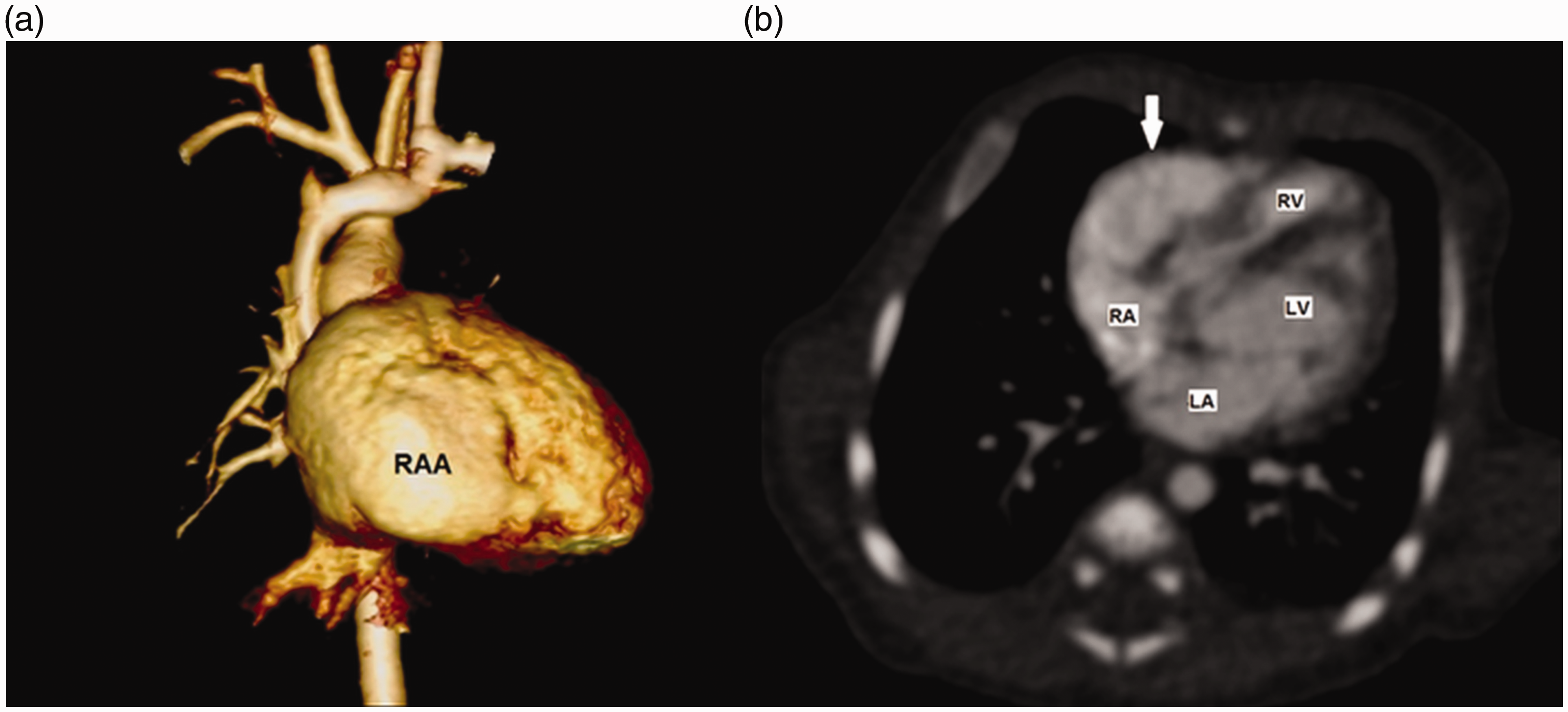
CT angiography of the newborn. (a) 3D reconstruction. Aneurysmal dilatation of the right atrial appendage (RAA). (b) Axial scan. Right atrial appendage aneurysm (white arrow). RA: right atrium; LA: left atrium; LV: left ventricle; RV: right ventricle.
Aneurysm or diverticulum—Anatomic and histological nuances
In the context of the differential diagnosis of CMRA forms, it is important to remember the atrial appendage, which often remains the “forgotten part” of the heart. The appendage of the RA is a triangular pocket-shaped part of its anterolateral surface delineated from the rest of the atrium by the crescent-shaped muscular ridge. Its inner surface is covered with muscular bundles (musculi pectinati) that alternate with thin, almost transparent sections of the appendage wall without muscle fibers. 22
These anatomical features determine the ultrasound picture of RA aneurysms. Most often there is a marked dilatation of both the RA and its appendage or significant enlargement of the RA appendage itself.4,6,8 However, the pathological process could involve not so much the appendage base and/or the part of the free RA wall as the RA appendage body and the apical part. 23 In this case, the neck of appendage can mimic the ostium of the diverticulum, and pectinate muscles can help to preserve some contractility of the pathological chamber. Such an ultrasound picture may be mistakenly regarded as a diverticulum.
It is also essential to understand there are two histological types of diverticula. The muscular type has all the classic features of a diverticulum, while the fibrous type is characterized by the presence of the connective tissue and a few (or absent) muscle fibers. Fibrous forms show either an akinetic or dyskinetic contractile function and usually a wider neck. 24 These subtypes are described only for cardiac ventricles. To our knowledge, there are no publications about the same diverticula subtypes for the atria or the methods which can help in differential diagnosis. Therefore, even if fibrous diverticula can be found in the atria too, they seem to be indistinguishable from congenital aneurysms.
Aneurysm or diverticulum—Current limitations
To date there are less than 50 publications about CMRA including fetuses, children or adults. Prenatal cases of RA or its appendage aneurysms are limited and there are no reports about the prenatal diagnosis of RA diverticula. There is no consensus in terms and presentation of each of these anomalies. A detailed description of the heart chambers and histological data are not always shown. So the existing knowledge is not always sufficient to make an accurate diagnosis prenatally.
Furthermore, there is no essential difference in the postnatal management of patients with RA aneurysms or diverticula. Treatment mode varies between centers and includes expectant management, anticoagulant and antiarrhythmic agents intake, nonspecific therapy or surgical treatment.1,3 Regardless of the precise prenatal diagnosis, the newborn should be under cardiologist observation. The necessity and type of surgical correction are determined individually, depending on the size of the pathological outpouching and the presence of clinical symptoms.3,11,25
Conclusions
Arguably, there is little value in trying to distinguish between RA aneurysm and diverticulum prenatally. Given the number of difficulties, precise definitions are best avoided in favor of a general term that combines both diagnoses (e.g. “CMRA” or “RA outpouching, more likely aneurysm/diverticulum”). This information alone will be enough for safe and appropriate perinatal management including place of delivery and immediate aftercare for the newborn. The final diagnosis could be made postnatally using additional visualization techniques and/or histological examination of the postoperative material.
Footnotes
Acknowledgements
The authors thank professor Moshe Bronshtein and professor Philippe Jeanty for assistance and support.
Contributors
OI contributed with ultrasound data, wrote the first draft of the manuscript, reviewed and analyzed the literature and wrote the final version. YuS contributed with ultrasound data and drafting the article. YuT contributed with catamnesis data and drafting the article. AZ contributed with postnatal images and data analysis. AK contributed with intraoperative and histological data and analysis of the literature. All authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
This work has been approved by Local Ethics Committee of Moscow Regional Research Institute of Obstetrics and Gynecology (JRB #06004245), Moscow, Russia. Permission from patient(s) or subject(s) obtained in writing for publishing their case report: yes. Permission obtained in writing from patient or any person whose photo is included for publishing their photographs and images: yes.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
OI.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.