
Abstract
Introduction
The purpose of this study was to identify attitudes, beliefs and common practices of hand therapists in Australia regarding assessment and management of base of thumb osteoarthritis.
Methods
Monthly emails with a link to a 57-item cross-sectional survey were sent to members of the Australian Hand Therapy Association between November 2015 and February 2016. The survey included a case scenario of a patient with base of thumb osteoarthritis with questions about assessment and non-pharmacological and non-surgical treatment interventions for this case. Participants also rated their agreement with a series of 20 attitude and belief statements on a 6-point Likert scale. Data underwent descriptive analysis.
Results
A total of 124 therapists accessed the survey, of which 77 (62%) returned completed answers and 47 (38%) partially completed it. The majority were occupational therapists (n = 92, 74%), and the remaining were physiotherapists. The most common clinical assessment methods used for base of thumb osteoarthritis were palpation (96%), range of motion (90%), the grind test (85%), and pain on opposition across the palm (82%). The commonly reported treatments included a combination of orthosis prescription (92%), pain education (78%), heat (75%) and exercise (74%).
Conclusion
The findings highlight commonly used assessment tools and treatments for a typical patient with base of thumb osteoarthritis. Despite the low response rate, there is consistency among general treatment for base of thumb osteoarthritis. Variation exists within the specifics of exercise and orthosis prescription. The results of the survey reflect the lack of standardised recommendations for the management of base of thumb osteoarthritis.
Introduction
Osteoarthritis (OA) is a chronic disorder which has a major impact on quality of life and high economic burden. 1 It is the most common type of arthritis and one of the leading causes of disability worldwide. 2 The hand joints are most frequently affected, with a prevalence of radiographic hand OA (43%) greater than hip and knee OA combined (11% and 24%). 3 Among the different subtypes of hand OA, the prevalence of radiographic base of thumb OA is reported as high as 33% in postmenopausal women. 4 Clinically, OA at the base of the thumb represents a particular challenge to health professionals because of its disabling symptoms and the limited efficacy of treatment options.
Individuals with hand OA experience not only pain but also significant functional limitations including difficulties with fine motor tasks such as writing, handling or fingering small objects. 5 Patients commonly describe problems with household tasks such as wringing out wash cloths and opening jars or bottles. 6 Maximal grip strength has been demonstrated to be reduced by 10% in older adults with symptomatic hand OA impacting functional tasks such as carrying a 10 lb (4.5 kg) bundle. 5
There is a paucity of research demonstrating the most effective treatments for hand OA, in particular, base of thumb OA. There is evidence of modest treatment effects to support the role of non-surgical therapies in the management of hand OA. 7 Recommendations published in 2007 indicated the largest treatment effects for topical non-steroidal anti-inflammatory drugs (NSAIDs) and orthoses for the treatment of hand OA. 8
There is moderate evidence to support hand exercises to increase grip strength, function and range of movement as well as to decrease pain. 9 However, a recent randomised trial comparing exercise versus no exercise showed no significant between-group difference in the proportion of responders according to the criteria recommended by OMERACT/OARSI to characterise a responder at six-month follow-up. 10
The use of orthotics is a well-tolerated and effective treatment for improving pain in those with base of thumb OA. 11 It has been shown to improve pain, with no influence on hand function or strength. 12 These findings conflict with an earlier systematic review in 2010, which concluded that there is moderate evidence to support the use of CMC orthotics for increasing grip strength. 9
Only a few high-quality studies exist which address the treatment of base of thumb OA. 12 Given the limited evidence available and somewhat contradictory findings, together with the lack of agreement between current recommendations (specifically for base of thumb OA), it is likely that clinical practice for this condition will vary. There are no studies reporting current clinical practice for base of thumb OA in Australia.
The purpose of this study was to identify attitudes, beliefs and common practices of occupational therapists and physiotherapists practising in Australia with expertise in hand therapy regarding their assessment and non-pharmacological/non-surgical treatments for base of thumb OA. This information is important to understand better how clinicians with expertise in hand therapy currently address this condition, as well as identify gaps and areas for potential improvement.
Methods
Physiotherapists and occupational therapists who were members of the Australian Hand Therapy Association (AHTA, Australia’s only professional association representing practitioners of hand therapy) who had authorised to receive emails from AHTA were approached via email to participate in a cross-sectional survey. The survey was sent out through AHTA, and the online survey remained open for a period of four months (November 2015 to February 2016). Participants were initially contacted in November 2015, and three email reminders were sent out in December 2015, January 2016 and February 2016.
Because of changes in membership numbers during this period, an average of 627 (range: 611–636) surveys were sent out in each round. The therapists who completed the survey were asked to disregard any subsequent email reminders. An email link to the electronic survey, and a participation information sheet was sent from the AHTA to members.
Eligibility criteria to complete the survey were assessed by the first question of the survey. Participants were eligible to complete the survey if they reported treating patients aged 45 years and above with chronic pain at the base of the thumb, and had assessed and treated at least one of such cases in the past six months. The study was approved by the University of Sydney Human Resources and Ethics Committee (ref: 2015/802).
Survey
A customised web-based survey delivered using the Survey Gizmo® platform was developed by 13 clinicians and OA researchers (including hand therapists, physiotherapists and rheumatologists). The survey was adapted from one used previously to assess the management of knee OA by physiotherapists in the United Kingdom, 13 and its development was an iterative process whereby drafts were discussed by the group and the survey subsequently refined based on consensus.
The final survey (available upon request) comprised 57 questions organised into three main sections. The first section collected information about the participants’ demographics, experience and expertise in the field of hand therapy. The second section presented a clinical case scenario about a typical patient with base of thumb OA (Box 1). This case was developed by the co-authors (clinicians, physiotherapists and occupational therapists) with expertise in the field of hand therapy. Case study. A 63-year-old woman was referred from her GP due to thumb pain which began insidiously three years ago and has steadily worsened over time. Her GP told her that she has osteoarthritis. She is anxious about the possibility of increasing loss of hand function and feels that her pain is going to get worse. She is concerned that there is not a lot she can do to prevent this, especially as she remembers her mother was crippled by arthritis in her hands in later life. Your patient has not had any previous treatment for her thumb problem, and her health is generally good, although she is overweight, and is on daily medication for hypertension. She is a retired receptionist, lives with her partner and babysits her four-year-old grandson two days per week while her daughter works. Today, she rates the intensity of her thumb pain as 3 out of 10 (on a scale where 0 is no pain and 10 is worse imaginable pain). Pain is increased to 6/10 and aggravated by opening jars, buttons, chopping vegetables, turning keys, pegging and pulling on tights. She is limited in her ability to perform her daily activities and can only vacuum for 10 min before she has to stop. She finds some relief from applying heat and takes over-the-counter Paracetamol when she needs it, which is around twice per week. Her thumb feels stiff first thing in the morning, which eases following a hot shower and gently exercising her hands, after approximately 20 min. On examination, the base of her thumb looks swollen and subluxed. There is slight wasting of her thenar eminence and tightness of web space, resulting in her MP joint hyperextending when she tries to reach around a large jar. She is able to oppose the tip of her thumb to the tip of her ring finger but reports pain when touching the little finger. She cannot put her hand flat on the table as her thumb seems to be in the way, and it is painful when she tries to lean on an extended wrist because of this. There is no scaphotrapeziotrapezoidal joint or wrist involvement.
Following the case study, questions about the participants’ initial clinical assessment and treatment of this hypothetical patient were presented. The survey used multiple choice answers, check boxes (participants were able to select more than one option) and open-ended questions to provide greater detail. The third section aimed to assess therapists’ attitudes and beliefs about exercise and orthosis prescription for base of thumb OA. For this, a list of 20 statements was used, and participants asked to rate their agreement with each of the statements on a six-point Likert scale ranging from 1 to 6 (1 = totally disagree; 6 = totally agree).
Data analysis
Data were exported from the Survey Gizmo® platform into an Excel spreadsheet. Data underwent descriptive analysis. VD carried out the initial data analysis, and SRR verified it. Data from the partial responses were combined with the complete responses for the participant characteristics, common clinical assessment tools and most common treatment approaches. Frequencies were tabulated for the responses from the closed questions, and the most frequent responses were presented as percentages, irrespective of whether the participant had fully or partially completed the survey. Due to the diversity of responses to the open-ended questions, we were unable to group the responses, and qualitative analysis was unfeasible. For checkbox-type questions, responses were presented for each option available. The level of agreement for each of the attitudes and belief statements were calculated and presented in bar graphs as survey participants who totally/largely agreed, totally/largely disagreed or agreed/disagreed to some extent with the provided statements.
Results
Of the average of 627 emails sent to members of the AHTA in each survey mailing round, an average of 348 (range: 321–383) (56%) were opened. In total, 124 (20%) therapists accessed the survey, of which 77 (12%) surveys were returned complete and 47 (8%) were partially completed.
The overall sample (n = 124) included responses from 92 occupational therapists (74%) and 32 physiotherapists (26%). The majority of participants were female (90%) and worked exclusively in a non-public health setting (65%). Forty-four per cent of respondents reported having 6 to 15 years of experience in hand therapy, and thirty-three per cent of respondents report having over 16 years of experience in hand therapy. Thirty-eight per cent of respondents reported that they treated patients with chronic thumb pain very frequently (at least two cases per week).
Seventy-one per cent reported completing postgraduate training specifically in the field of hand therapy, and 24% were Certified Hand Therapists. Almost half of the participants reported undertaking day or weekend courses with no formal assessment (41%) or courses or modules with formal assessments (44%). Specific training in the manufacturing of orthoses had been undertaken by 69% of respondents with over half (60%) completing day or weekend courses.
Clinical assessment
The majority of participants reported that they would refer the case study’s patient for radiographs of the first CMC joint at the initial visit (n = 85, 74%). The common clinical assessment tools chosen by respondents for the clinical case scenario are presented in Table 1. Physical measures were used by the majority of participants as part of their assessment. The most commonly used physical measures were palpation, thumb range of motion (CMC and metacarpophalangeal (MCP) joints), the grind test of the CMC joint and pain provoked by the opposition of the thumb across the palm.
Common clinical assessment tools for thumb OA.
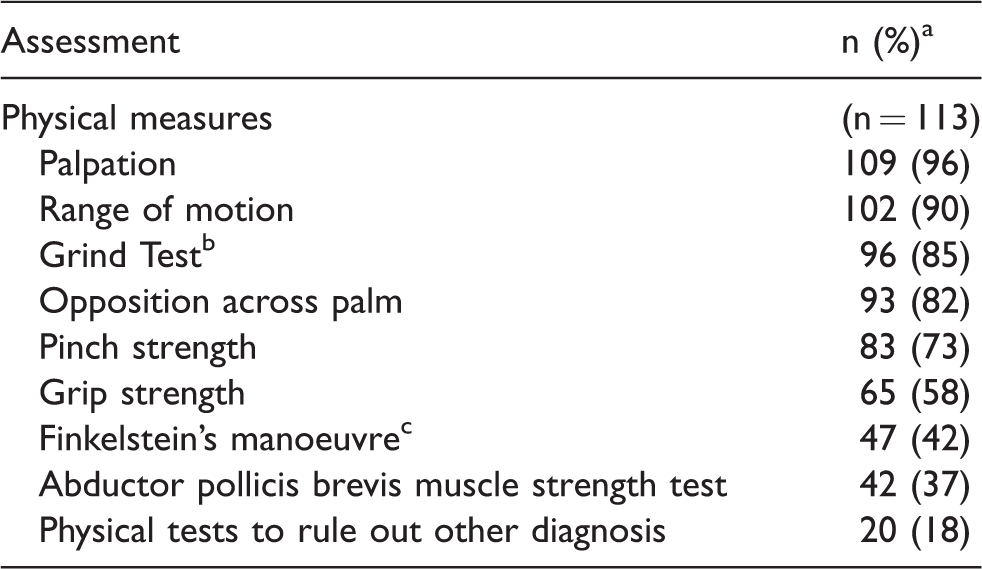
aRespondents were able to choose more than one option
bPerformed by grasping the thumb phalanx and exerting axial compression while rotating the thumb CMC joint. 15
cPerformed by grasping the thumb and abducting the hand ulnar ward. 29
Sixty-five per cent of respondents would use some form of questionnaire in their initial assessment (n = 80). The most common self-report questionnaires administered were the Disabilities of Arm, Shoulder Hand (DASH) (n = 30, 384%) and the Patient-Related Wrist and Hand Evaluation (PRWHE) (n = 19, 24%). Eighty per cent of respondents chose to assess pain using the numerical pain rating scale (NRS) or visual analogue scale (VAS).
Treatment
The most common treatment approaches for the clinical case scenario were orthoses prescription (n = 96, 92%), pain education (n = 81, 78%), heat (n = 78, 75%), exercise therapy (n = 77, 74%) and massage with topical NSAID (n = 55, 53%). All participants chose a combination of treatments rather than a single therapy. Specific details for orthoses prescription, pain education and exercise therapy are described in Table 2.
Most common treatment approaches.
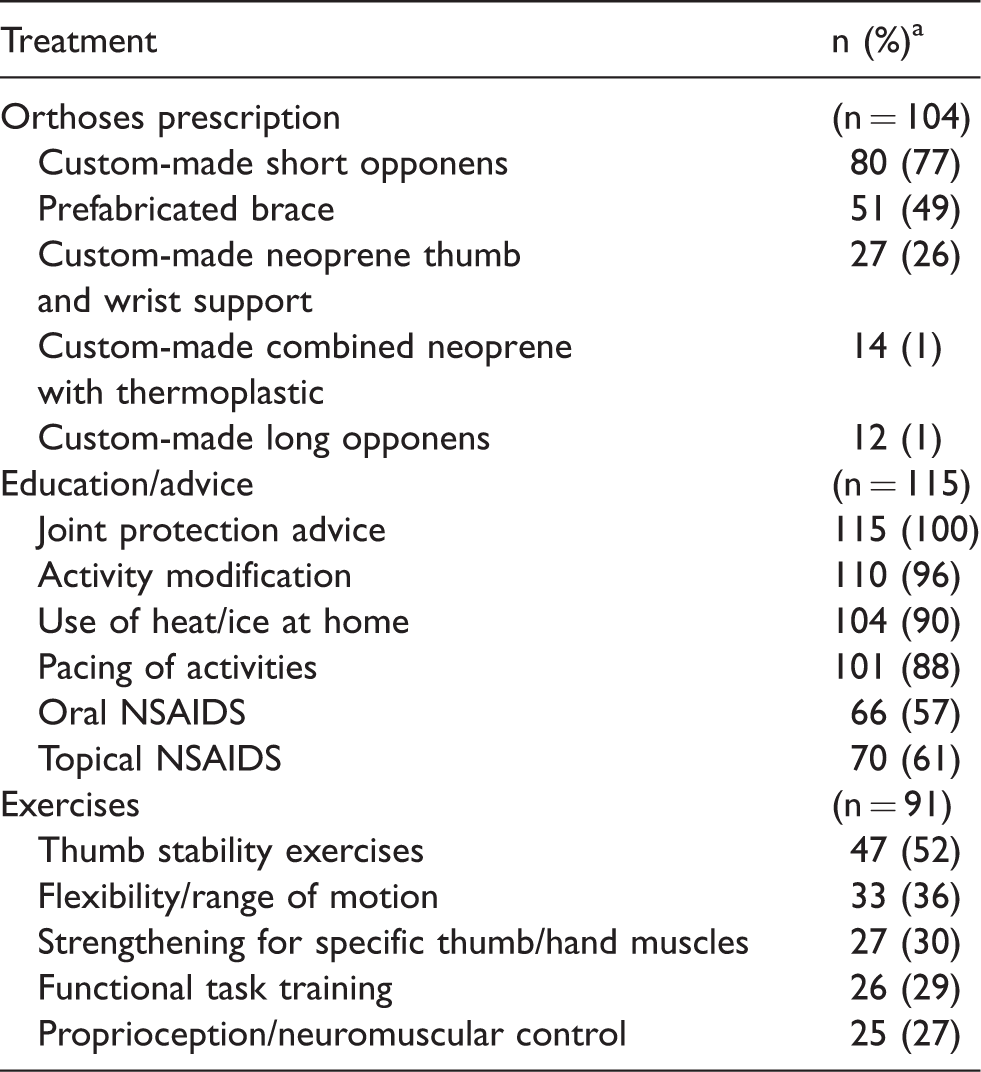
NSAIDS: nonsteroidal antiinflammatory drugs.
aRespondents were able to choose more than one option.
The most common approach for orthosis prescription was a custom-made short opponens (Table 2). The reported dosage for the orthosis varied across participants. The most commonly reported dosage was ‘only during aggravating activities or at-risk activities’, regardless of the type of splint.
All participants would offer education and advice regarding OA disease as part of their treatment (Table 2). All respondents would offer advice regarding joint protection, and almost all participants would offer education and advice regarding activity modification (n = 115, 100%), the use of heat/ice at home (n = 104, 90%) and the pacing of activities (n = 101, 88%).
About half of the participants would give thumb stability exercises for the patient in the clinical case scenario (n = 47, 52%) (Table 2). Other types of exercises included flexibility or range of motion exercises (n = 33, 36%), strengthening for specific thumb or hand muscles (n = 27, 30%), functional task training (n = 26, 29%) and proprioception or neuromuscular control exercises (n = 25, 27%). The main choice for delivery of exercises was through written advice (n = 68, 76%), followed by verbal advice (n = 59, 66%) and supervision of exercises in the clinic (n = 51, 57%). About half of the participants agreed that the exercises ‘must be pain-free’ (n = 34, 38%), whereas 27% (n = 24) felt that it was ‘okay to have very mild pain’.
Attitudes and beliefs
Perceived benefit of exercise for base of thumb OA
Fifty-two per cent of respondents totally or largely disagreed that ‘a standard set of exercises is sufficient for every patient with chronic thumb pain’ (Figure 1). Forty-nine per cent of respondents agreed to some extent that ‘strengthening the muscles around the thumb stops the thumb problem from getting worse’ (Figure 1). Thirty-eight per cent of respondents agreed to some extent, and thirty-four percent of respondents totally or largely agreed that ‘hand therapists should prescribe strengthening exercises targeted at the thumb/hand muscles to every patient with chronic thumb pain’ (Figure 1).

Attitudes and belief statements of physiotherapists and occupational therapists with expertise in the field of hand therapy (Part 1).
The majority of respondents totally or largely disagreed or disagreed to some extent (51% and 25%, respectively) that ‘exercise works just as well for everybody, regardless of the amount of pain they have’ (51% and 25%, respectively) (Figure 1). Survey respondents agreed that exercises become less effective for patients with increasing radiographic severity, with 64% totally or largely agreeing towards exercise for mild thumb osteoarthritis, 45% for moderate thumb osteoarthritis and 8% for severe thumb osteoarthritis, including the STT joint (Figure 1).
There was a low level of agreement reached on the statement ‘hand therapists should prescribe general whole body exercise, for example, yoga or swimming, for every patient with chronic thumb pain’ with the results almost evenly distributed among levels of disagreement and agreement (Figure 1). Forty-one per cent of respondents also totally or largely disagreed with the statement that ‘increasing overall activities of the whole body stops the thumb problem from getting worse’ (Figure 1).
Patient and therapist roles
Over half of respondents (56%) totally/largely agreed with the statement that ‘how well a patient complies with their exercise program determines of effective it will be’ (Figure 2). The majority (84%) of respondents agreed that ‘it is the patient’s responsibility to continue doing their exercise program’ (Figure 2).
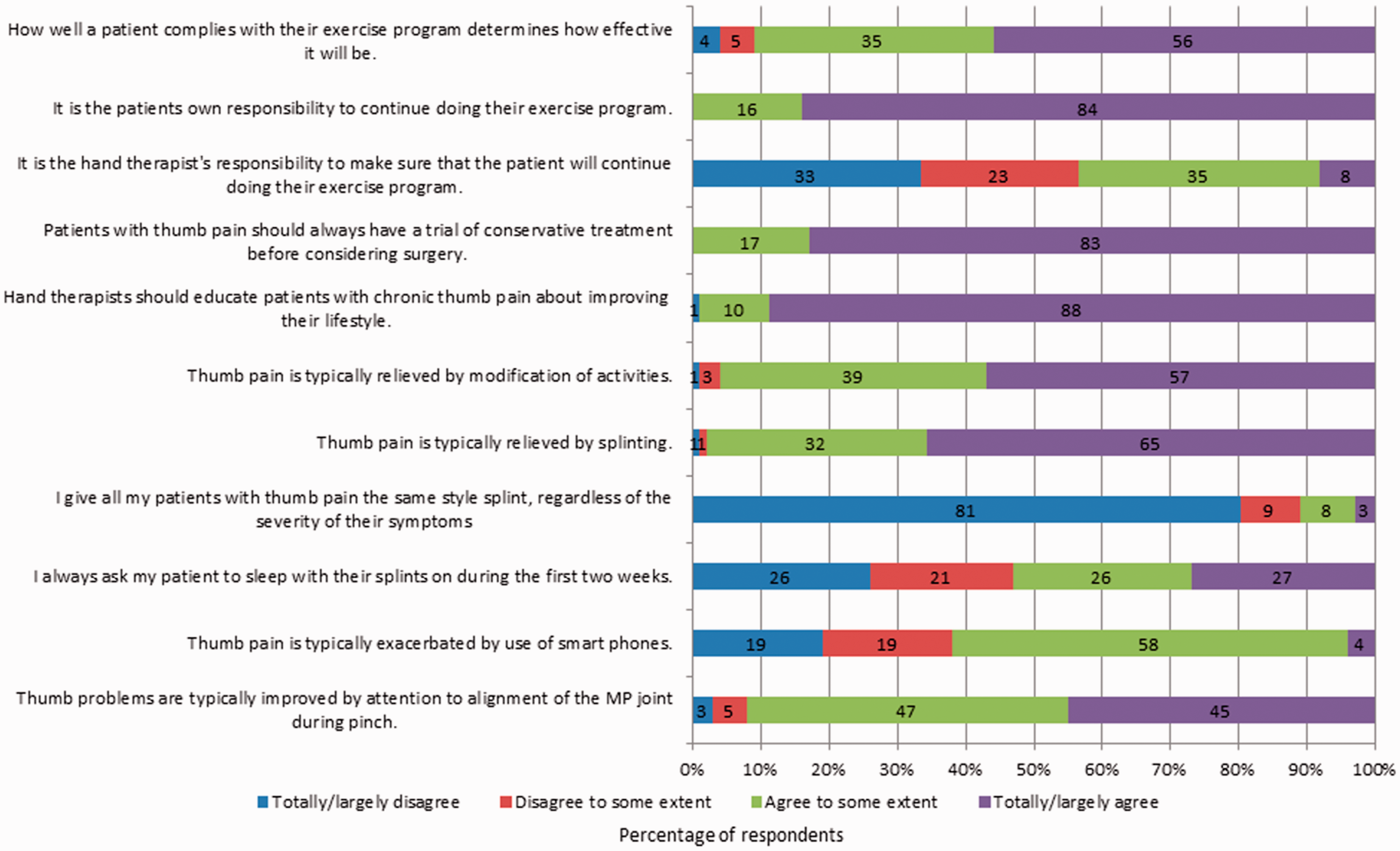
Attitudes and belief statements of physiotherapists and occupational therapists with expertise in the field of hand therapy (Part 2).
Perceived benefit of education/advice
A substantial proportion of respondents agreed that ‘patients with thumb pain should always have a trial of conservative treatment before considering surgery’ (83%) and that ‘hand therapists should educate patients with chronic thumb pain about improving their lifestyle’ (88%) (Figure 2). Thirty-nine per cent and fifty-seven per cent of respondents agreed to some extent and totally or largely agreed with the statement that ‘thumb pain is typically relieved by modification of activities’ (Figure 2).
Splinting for base of thumb OA
Sixty-five per cent of respondents totally or largely agreed with the statement, ‘Thumb pain is typically relieved by splinting’ (Figure 2). A great majority (81%) of respondents totally or largely disagreed with the statement, ‘I give all my patients with thumb pain the same style splint, regardless of the severity of their symptoms’ (Figure 2). There was a wide range of agreement and disagreement with the statement ‘I always ask my patients to sleep with their splints on during the first two weeks’ (Figure 2).
Discussion
To our knowledge, this is the first survey to describe the attitudes, beliefs and common practices of occupational therapists and physiotherapists with expertise in the field of hand therapy with regard to the management of base of thumb OA in Australia. The findings reveal that although there is consistency around general physical assessment and treatments for base of thumb OA, the specifics of exercise and orthosis prescription are variable. Overall, the attitudes and beliefs statements were evaluated as expected for base of thumb OA management.
Diagnosis of base of thumb OA is made on a combination of signs and symptoms. It is assumed when there are pain and tenderness at the base of thumb as well as joint enlargement and deformity on physical examination. 14 The commonly reported assessment tools used by clinicians in the survey were palpation, range of motion, grind test and strength measures. The grind test has been suggested to diagnose base of thumb OA but has only moderate validity for confirming or excluding the diagnosis (specificity 80%, sensitivity 53%) 15 Apart from the grind test, none of the other commonly used assessment measures have been subjected to psychometric testing in the diagnosis for base of thumb OA. Base of thumb osteoarthritis can also be screened with the adduction test (specificity 93%, sensitivity 94%) and extension test (specificity 95%, sensitivity 94%); however, these were not included as options in our survey. 16 These two tests are more specific and sensitive compared to the grind test. 16
There is limited evidence from high-quality trials and, consequently, a lack of clinical practice guidelines specifically for the treatment of base of thumb OA. Instead, recommendations focus on hand OA in general.8,17,18 The guideline for hand OA published by the Italian Society for Rheumatology recommends a combination of joint protection and hand exercises. However, this recommendation was based only on expert opinion. 18 None of the recommendations made by the American College of Rheumatology (ACR) guidelines published in 2012 were classified as strong due to limited research and only small to moderate treatment effect sizes (20). Conditional recommendations were made for instructions on joint protection, assistive devices, use of thermal modalities and orthoses (20).
A recent systematic review by Spaans in 2015 reported that there were only a few high-quality studies which evaluated conservative treatment for base of thumb OA. 12 The authors concluded that orthoses were shown to reduce pain without any effect on function, strength or dexterity. 12 There is no high-level evidence to support the use of analgesics and patient education in joint protection for persons with base of thumb OA. 12
Orthosis prescription was the most commonly reported treatment for the base of thumb OA clinical case scenario. The rationale behind the orthosis is that it provides external support to the CMC joint avoiding subluxation of the joint and compensatory movements as well as preserving the first joint space.19,20 Splinting was shown to reduce the amount of subluxation in those with grades 1 and 2 base of thumb OA. However, those with more advanced OA (grades 3 and 4) did now show any reduction of subluxation. 11
Although there is some evidence that orthoses effectively reduce pain in persons with base of thumb OA,21,22 the optimal dosage remains controversial. This is reflected in our results with no agreement regarding the duration of orthosis wear. There is also limited evidence on the optimal type of orthosis suitable for CMC OA. Sillem et al. 23 compared the effectiveness of two different orthoses – a custom-made thermoplastic CMC orthosis and a prefabricated orthosis. The authors found no statistically significant differences in hand function, grip strength and pinch strength. 23
Although a prefabricated orthosis has been shown to be preferred by patients, 23 the majority of survey respondents would choose to make a custom short opponens orthosis (77%). A recent study by de Almeida et al. 24 surveyed physiotherapists, occupational therapists and physicians (rheumatologists) about the choice of orthoses for a patient with base of thumb OA, where respondents indicated their preference based on 25 photographs of orthoses models. Among the 275 respondents of the survey, there was no consensus regarding orthosis prescription with variations in the number of joints immobilised and a preference for rigid materials involving the wrist, CMC and MCP joints. 24
Although there is a lack of evidence to support improvements in hand function, orthosis prescription is a widely accepted component of treatment and may improve pain. The lack of robust evidence makes it difficult to discern the optimal type and duration of wear of the orthosis for base of thumb OA because of high potential for bias in current studies as highlighted in a systematic review. 25
The majority of clinicians reported that they would prescribe hand exercises for the patient, but there was no agreement regarding the specific type of hand exercises. Hand exercises aim to maximise the pain-free functional range of motion, increase functional strength for pinching and grasping tasks, maintain joint stability and avoid development of fixed deformities. 26 A systematic review which assessed the effectiveness of orthoses, the effectiveness of exercise and a combination of both, concluded that there is a large variety in designs in orthosis prescription and exercise programmes. 25 Therapists were reluctant to recommend the performance of exercises through pain, probably due to the fear of causing further damage to the joint. Further high-quality research should assess the harms and benefits of exercising in the presence of pain and which pain limits are acceptable. The results from single trials showed that hand exercises might reduce pain and increase ROM, whereas a combination of an orthosis and exercise will reduce pain and stiffness as well as improve function. 25 It is shown that an orthosis reduces hand pain. However, there is limited evidence to support a combination of an orthosis and exercise in hand OA. 25
This study revealed some uncertainty regarding the perceived benefit of exercise for base of thumb osteoarthritis, especially with increasing radiographic severity. There was little agreement reached on the benefits of whole-body exercise to improve chronic thumb pain in those with thumb base OA. This notion is also demonstrated in a previous survey used to assess the management of knee OA by physiotherapists in the United Kingdom. 13 However, there is no direct correlation between radiographic severity and pain intensity. 27
Over half of the survey respondents largely or totally agreed that how well a patient adheres with their exercise programme determines how effective it will be, and there was a firm belief that exercise adherence was the patient’s responsibility and not the therapist’s. This may reflect a paternalistic approach adopted towards exercise and base of thumb OA.
One strength of our survey was the web-based design which allowed it to be distributed with little cost to a large population of hand therapists. Also, we were able to specifically target members of the Australian Hand Therapy Association, who have extensive training in the area of treatment of hand conditions. All members are required to have practised as a qualified physiotherapist or occupational therapist for a minimum of three years and have a minimum of 3600 hours of clinical experience in the field of hand therapy within the last five years, as well as other qualifications. 28
The main limitation of this study was the poor response rate. This is typical of many survey studies and may be partly explained by the length of the survey, the lack of an adequate reward for completion of the survey and that there was a competing survey related to base of thumb OA distributed contemporaneously. The poor response rate may also affect the generalisability of our study if the responses of those who completed the study differed systematically from those who did not answer the survey.
Also, the use of a single case scenario might limit our capacity to reflect true clinical practice, as the presentation of each patient with base of thumb OA may vary resulting in some differences in assessment and treatment. This may be better revealed by a mixed methods survey involving interviews. Finally, due to the diversity in the open-ended questions, we were unable to analyse these responses. We may have different findings if we had analysed the open-ended questions.
In general, the attitudes and beliefs statements were rated by the survey participants according to the current evidence for base of thumb OA management. However, some controversial statements had unexpected ratings, and the main issues were generalising the patient management, the uncertainty of effectiveness of exercises for severe thumb OA and the notion that it was entirely up to the patient or therapist to be responsible for the continuation of the patient’s exercise programme. For example, eighty-four per cent of respondents largely or totally agreed that ‘It is the patient’s own responsibility to continue doing their exercise program’.
The survey results also provided insight into the common practices for the assessment and treatment of base of thumb OA. The participants agreed on the main categories of assessment (palpation, range of motion, grind test and strength measures) and treatment (orthosis prescription, exercises and joint protection). Joint protection had unanimous agreement even in subcategories. However, there was no consensus regarding the type and dose of orthosis and exercises. We believe that this finding reflects the lack of specific evidence-based recommendations for orthosis prescription and exercises in the management of base of thumb OA.
Conclusion
This survey demonstrates some consistency among hand therapists in Australia in their general treatment for base of thumb OA. There are variations in practice with regard to specific types of exercise and orthosis prescription. This may be due to lack of standardised models of care for this disease. Further high-quality randomised controlled trials and meta-analysis are needed to establish the scientific evidence for base of thumb OA management. This will be the first step to enable the translation from evidence to clinical practice.
Footnotes
Acknowledgements
We would like to thank the Australian Hand Therapy Association (AHTA) for distributing the survey and the members who responded.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an NHMRC program grant (1091302). DJH is supported by an NHMRC Practitioner Fellowship. KLB and PH are supported by NHMRC Research Fellowships (1058440 and 1102905). MAH is funded by the National Institute for Health Research (NIHR) School for Primary Care Research. The funders did not influence the study design or the writing of this article. The views expressed in this publication are those of the authors and not necessarily those of the NHMRC, NHS, the NIHR or the Department of Health.
Informed consent
Online consent was obtained from participants for their anonymized data to be published in this article.
Ethical approval
The study was approved by the University of Sydney Human Resources and Ethics Committee (ref: 2015/802).
Guarantor
DJH.
Contributorship
VD, KLB, LAD, JPE, PWH, MAH, DJH, RJ, DK, YM, BV, AW, and SRR contributed to study conception and design. VD drafted the first version of the manuscript. All authors revised the manuscript critically for important intellectual content and read and approved the final version. All authors agree to be accountable for all aspects of the work.