
Abstract
Introduction
Exercises are widely used and recommended for peripheral joint and hand osteoarthritis (OA); however, the evidence on which specific exercise regimen is most effective is unclear.
Methods
A pilot randomized controlled trial was conducted to compare the effect of specific first carpometacarpal (CMC) joint stabilizing exercises and general exercise on function, pain and strength. Thirty-nine participants with OA of the first CMC joint were recruited and randomly assigned into one of two exercise groups. Exercises were taught as a home programme then reviewed and only progressed as tolerated. The participant and assessing physiotherapist were blinded. Primary outcome was the Disabilities of the Arm, Shoulder and Hand (DASH) Questionnaire at three and six months. Pinch and grip strength, pain scores at rest and during pinch and abductor pollicis longus (APL) moment were secondary measures.
Results
Twenty-two patients completed follow-up at six months. At baseline the general exercise group had significantly stronger pinch and APL moments but was not different in any other measures. The improvement (reduction) of DASH scores at three and six months was not significantly different between the two groups; however, the general exercise group had a greater reduction in DASH score from baseline to three months (13 points P = 0.001).
The outcomes were not affected (P > 0.05) by any variables except APL moment at baseline. Increased APL moment at baseline was associated with an improved outcome in both groups (P = 0.01).
Conclusions
While this pilot study was inadequately powered the results can be used to plan a future large-scale trial.
Introduction
Osteoarthritis (OA) of the first carpometacarpal (CMC) joint of the thumb is one of the most common forms of arthritis affecting up to 22% of the population. 1 There are many conservative treatments for OA CMC joint in widespread use with little evidence supporting them. 2 Given the prevalence of this condition, it is imperative that we examine these treatments to determine their effectiveness.
Exercise is widely used and recommended for peripheral joint 3 and hand 4 OA but the evidence for the choice of exercise regimen is not clear. One randomized controlled trial looking at the difference between two different regimens of splintage and exercise for OA CMC joint 5 showed improvements in terms of pain, pinch strength and function with both regimens. Stamm 6 showed significant improvements in grip and function with exercise and joint protection advice. Rogers and Wilder, 7 using exercise for OA of the hand, reported modest improvements in grip and pinch, but no changes in function or pain.
Taylor 8 suggested a regimen of exercises specifically designed for the CMC joint that strengthen abductor pollicis longus (APL). It is suggested that this muscle is critical to maintaining stability at the CMC joint.9–12 Taylor 8 proposed that the exercises will improve the joints’ dynamic stability (i.e. ability to prevent shearing forces or subluxation with function). There is currently no clinical evidence to support the use of these specific exercises.
This pilot study aims to test a protocol comparing the effect of CMC joint stabilizing exercises with general strengthening exercises on function, pain and strength at three and six months. Secondary aims were (i) to assess whether the results of the exercise programme are influenced by strength of APL, pinch grip, age, sex or grade of OA; (ii) to determine the effect size in function measured by DASH to inform sample size calculations for a larger scale study; and (iii) to test the feasibility of conducting a larger scale trial.
Method
A pilot randomized controlled trial was designed to compare the effects of two different types of exercise regimen on symptoms of OA of the CMC joint. An unrelated (different) participant design was used as it would not be possible for participants to undertake both types of exercise without significant order effects.
Ethical approval was granted by the Derbyshire Local Research Ethics Committee (LREC REF: 0310/749(S)).
Recruitment
All patients referred to the Pulvertaft Hand Centre, Derby, between March 2004 and January 2007 with a clinical diagnosis of first CMC joint OA that had been confirmed radiologically13, 14 were eligible for the study. Although Taylor 8 proposed that the specific exercises should be used with early arthritis as those with advanced changes may be unable to perform them, there is no evidence to support this concept and exercise is traditionally used in all patients with OA regardless of disease severity. All grades of OA 15 were therefore included in the pilot study, with a view to analysing in a full sample if all grades tolerated or benefited from exercise. Participants were considered for inclusion irrespective of any other intervention that they were undertaking such as joint injection or splinting. Splints were given with education but no exercise prescription as this represented current practice at the time. Exclusion criteria were suspected or confirmed inflammatory joint disease, coexisting hand conditions and inability to cooperate with the exercise regimens. This covered a wide spectrum from unable to attend appointments, unwilling or unable to do exercises due to home circumstances, health issues, poor memory: a decision being made by the patient and referring doctor together.
Procedure
All participants were given information about the study, and informed consent was obtained by the investigator (BD). Participants were randomly allocated on a 1:1 basis using a sealed envelope method into one of the two exercise groups. Both hands of patients with bilateral symptoms were treated by the allocated method. The random allocation sequence was generated and assigned by a research assistant who had no part in treatment or assessment. The investigator who was blinded to the exercise group allocation then completed the baseline assessment. The participants were taught their exercise regimen (Appendix A) and given standardized advice from the designated unblinded therapist (NY). They were seen at approximately one, three and seven weeks for review and exercises were progressed if they could be performed correctly and sustained with no increase in pain. Participants were then re-assessed at three and six months after randomization. The investigator remained blinded to the treatment group until after the study concluded.
Outcomes
The primary outcome measure was Disabilities of the Arm, Shoulder and Hand Questionnaire (DASH). It is designed to quantify disability and symptom experience (0 being no disability/symptoms to a maximum score of 100). The DASH has good construct validity, is responsive to change and has good test-retest reliability. 16
Secondary objective assessments were also chosen as they were considered to be appropriate, valid, reliable and easy to carry out:
Pinch strength in kilograms measured by the Jamar pinch gauge according to a standard protocol17, 18
Visual analogue scale (VAS) for current pain level taken at rest and during pinch 19
APL moment in Newton metres using a piece of equipment designed for this study (APL moment is the product of the force exerted at the thumb tip and moment arm which is the length of the thumb measured in metres). As the specific exercise regimen was intended to recruit and strengthen APL it was felt having some measure of its strength would help to explore the effect of the exercise regimen. It is important to note however that this equipment has not been studied for validity or reliability (Appendix B).
The primary and secondary outcomes were measured at randomization and repeated at three and six months after randomization. Participants were asked whether they had received any other treatments.
The following data were collected at initial assessment: age, sex, hand dominance, side affected, grade of OA according to the Eaton Littler classification (Appendix C), 15 and any other interventions received.
Sample size
At the planning stage of this study, papers investigating physiotherapy interventions for OA in this joint were not identified. Literature evaluating detectable differences for OA was scarce. 20 It was therefore decided to carry out a pilot study and from the data collected perform a sample size calculation, which would be more accurate than one based on assumptions.
Blinding
It was not possible to blind the treating therapist; however, the investigator and participants were blinded to the allocated exercise group to minimize any experimenter bias. The same physiotherapist (NY) treated all participants and the lead investigator (BD) performed all assessments.
Statistical methods
Statistical analyses were conducted using SPSS v17 (SPSS(UK) Ltd, Woking, UK). The distribution of continuous variables was tested using the Shapiro–Wilk test and their histograms. The skewed variables were reported using the median (Interquartile range [IQR]), otherwise they were reported using mean (±standard deviations). The statistical analysis was done based on people randomized and not on thumbs as independence of thumbs of bilateral participants could not be assumed. The outcome measures for bilateral participants were averaged across thumbs for the same person. The complete data-set per outcome was used.
The comparison of the continuous variables between the general and the specific exercise group at baseline was done using the Mann-Whitney U and the independent t-test. The Fisher's exact test was used for checking the association between sex, splint use, severity of OA, steroid injection prior to study and the groups. The changes in DASH scores were tested using the General Linear Model for repeated measures. Changes in pinch strength, VAS at rest and during pinch, and APL moment during six months period were tested using the Friedman test. The paired comparison of the skewed variables between two time points was done using the Wilcoxon test. The changes in DASH scores at three and six months compared with baseline were compared between the two exercise groups using the independent t-test.
Results
Figure 1 shows the study recruitment and follow-up. One bilateral patient was excluded having completed the study as he had been mistakenly entered on the database as randomized into a different exercise group for each thumb and the intervention he received could not be verified from the data collection forms.
Study recruitment and follow-up
Both groups were comparable with regard to age, sex and affected hand being dominant, grade of OA, splint use, steroid injection given prior to the study or number of appointments attended (Table 1). In order to compare the effects of the specific versus general exercise regimen, only complete data for participants retained at the assessment point of three and six months were used.
Baseline data according to exercise group
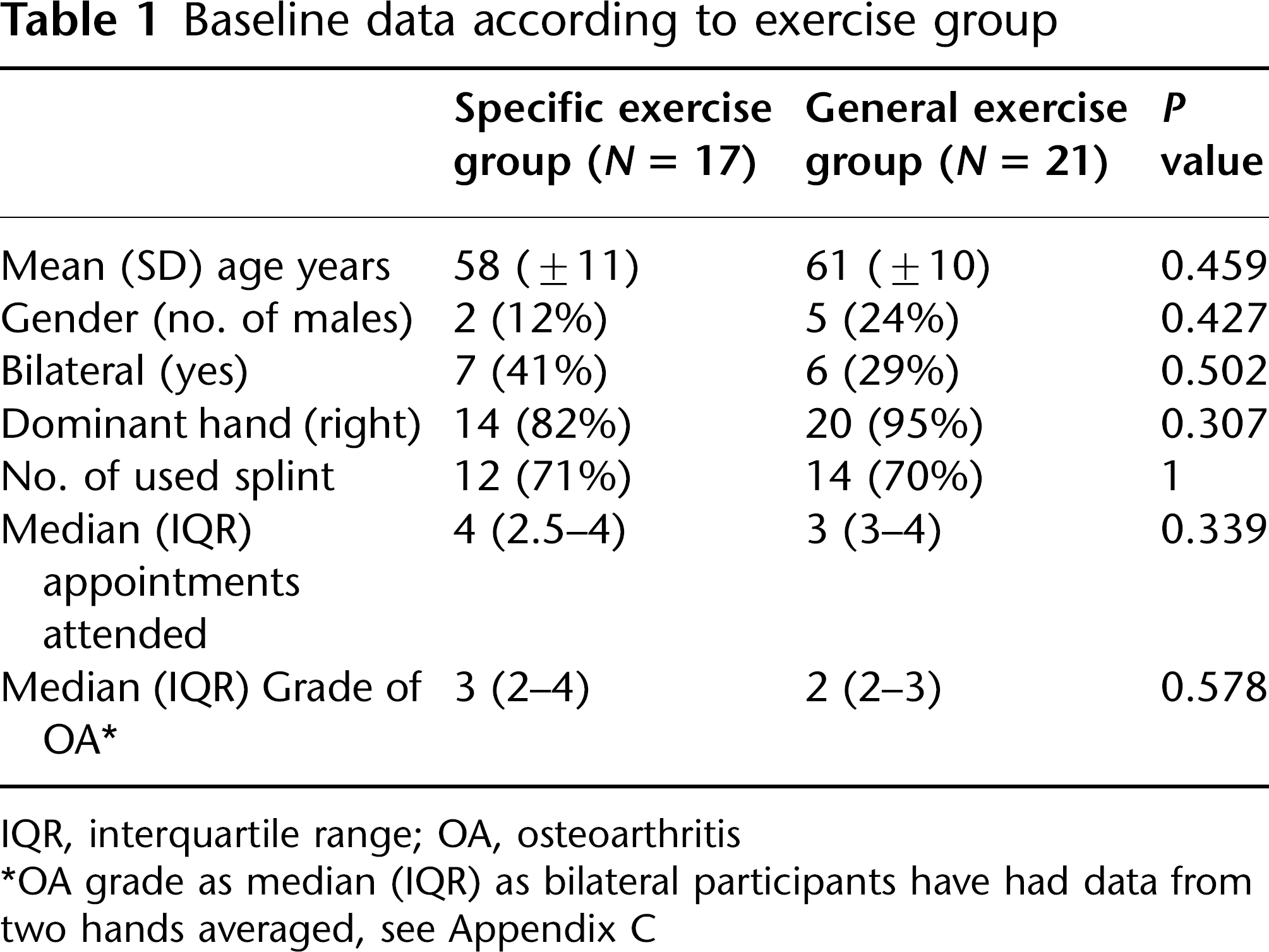
IQR, interquartile range; OA, osteoarthritis
OA grade as median (IQR) as bilateral participants have had data from two hands averaged, see Appendix C
Sixteen patients (41%) did not complete the six-month follow-up; reasons for non-attendance are known for six participants (Figure 1). These 16 participants had significantly higher baseline resting and pinch pain scores than those who attended at six months (Table 2). There were no other differences between this group and those who attended for follow up.
Baseline pain median (IQR) and DASH score mean (SD): patients who completed six-month assessment versus Did Not Attend (DNA) assessment
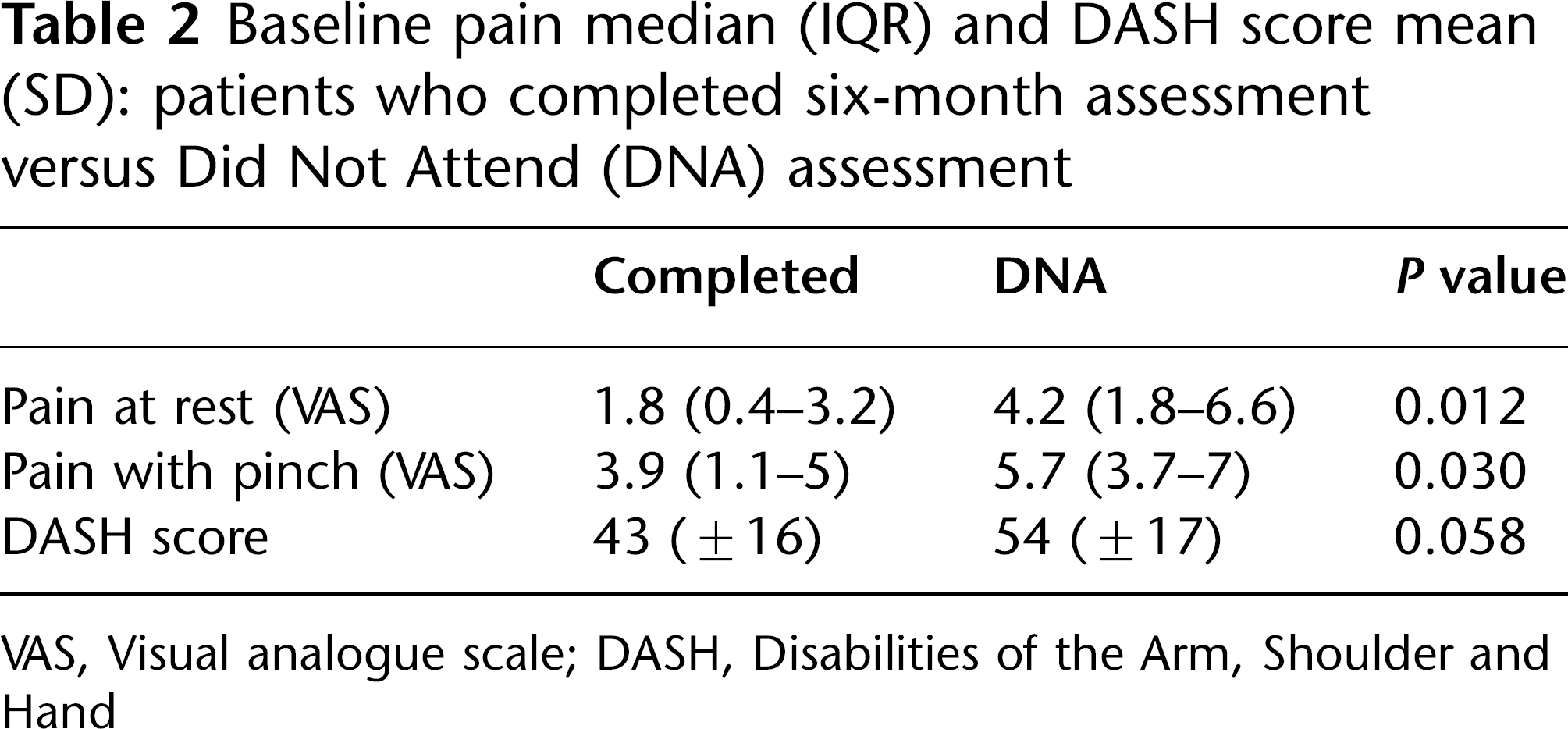
VAS, Visual analogue scale; DASH, Disabilities of the Arm, Shoulder and Hand
Both groups showed small reductions in DASH scores at three and six months but there were no significant differences between the two exercise groups at either three or six months (Table 3). Within each group only the general exercise group reduced DASH score significantly from baseline and only at three months (13 points P = 0.001) (Table 4).
Mean (SD) reduction of DASH scores at three and six months from baseline compared between two groups
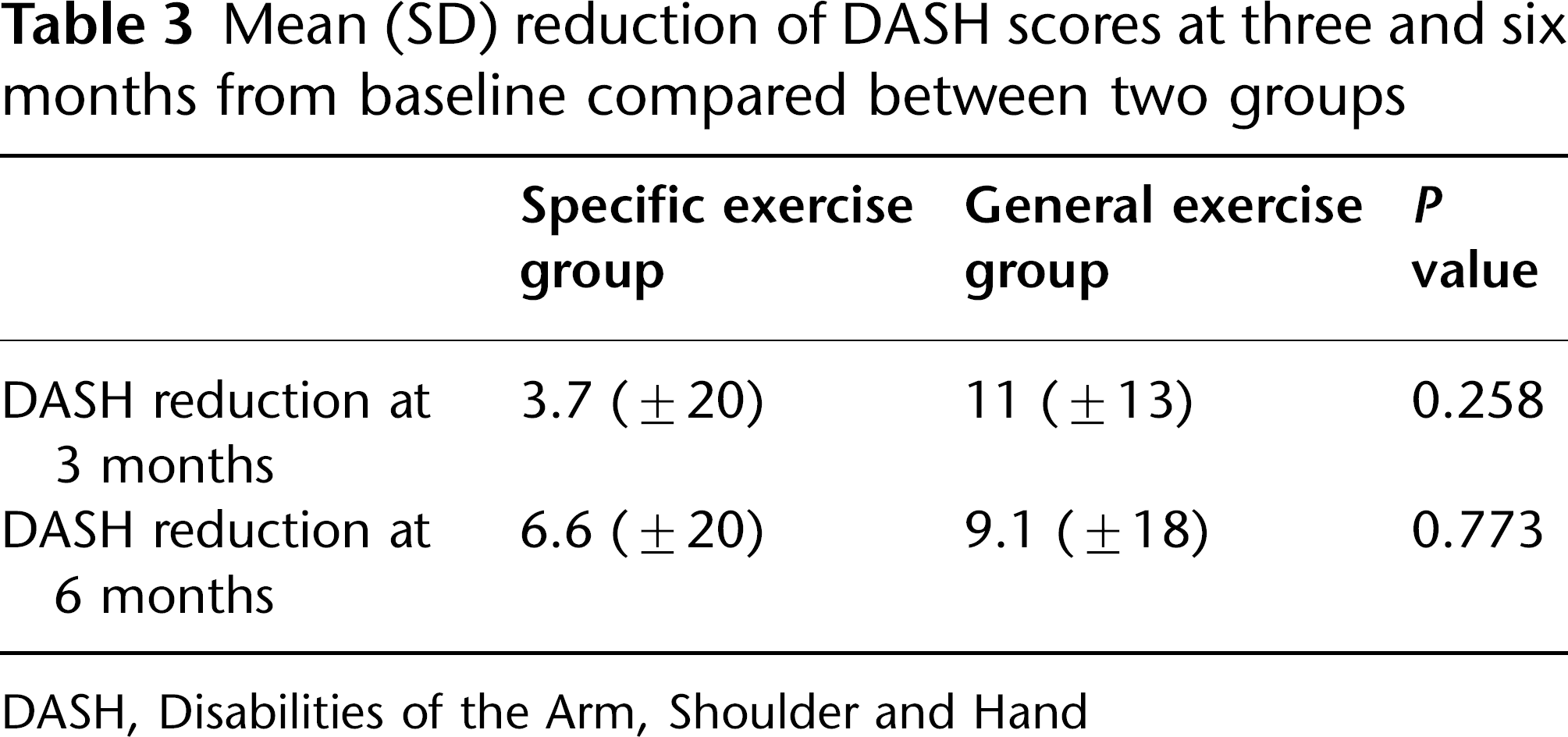
DASH, Disabilities of the Arm, Shoulder and Hand
Pinch strength (kg) and APL moment (Nm) median (IQR) and DASH mean (sd)
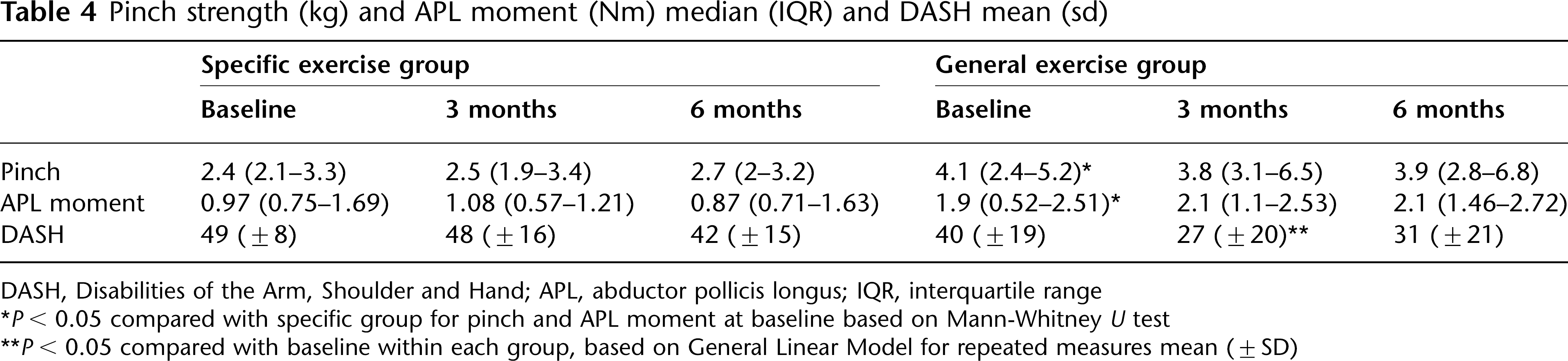
DASH, Disabilities of the Arm, Shoulder and Hand; APL, abductor pollicis longus; IQR, interquartile range
P < 0.05 compared with specific group for pinch and APL moment at baseline based on Mann-Whitney U test
P < 0.05 compared with baseline within each group, based on General Linear Model for repeated measures mean (±SD)
Participants in either exercise groups who reduced their DASH score by 12.7 points or more at six months were categorized as having clinically ‘improved’. 16 There was no difference between the two exercise groups for percentage of patients improved (specific = 18%, general = 24%, P = 0.709). All the baseline variables were analysed to see if any could predict outcome. Only the APL moment (Nm) at entry showed a significant (P = 0.01) difference between those who had improved 2.2 (1.7–2.7) and those who had not 1.1 (0.7–1.8). The use of a splint did not affect improvement or deterioration of DASH scores (P = 0.727). The majority of patients in both groups used a splint at baseline.
At baseline the general group had significantly stronger pinch and APL moment than the specific group. The general group had a small reduction and the specific group a small increase in their pinch strength over six months (Table 4). APL moment improved in the general group and reduced in the specific group but none of these changes were significant over six months.
The specific group did not improve their pain score at rest or with pinch over six months. The general group showed significant improvement in resting pain score (P = 0.019) and pain with pinch (P = 0.033) (Table 5).
Median VAS Scores (IQR)

VAS, visual analogue scale; IQR, interquartile range
Significant difference from baseline based on Wilcoxon test
Discussion
As a pilot study the results need to be read with caution due to small sample size. A sample size calculation carried out using the pilot study data (Appendix D) with adjustment for the 41% attrition rate that was observed in this study, showed 164 participants should be recruited in total. This pilot study is underpowered and therefore at risk of Type II error. The results of this pilot study suggest that we need to question the usefulness of the specific exercise regimen as it was used in this study. Taylor 8 hypothesized that the specific regimen to strengthen APL would increase stability at the CMC joint which would increase functional ability (DASH score). This did not occur in the specific exercise group; however, the general group demonstrated a statistically and clinically 21 significant improvement at three months (P < 0.05) of 13 points reduction (in DASH score). There was no significant change in APL moment in either group, but there was a trend towards increase in APL moment in the general group, who also showed a significant reduction in pain (resting and pinch); so it may be that stability of the CMC joint did improve with general exercise.
Specific exercise aims to increase strength and activity in APL to reduce shear and pain at the CMC joint. A small but not significant reduction in APL moment was observed during the study suggesting that improved stability was not achieved. However the test used for APL moment tested power and we were unable to test stabilizing action. Validating a method to test CMC joint dynamic stability would help in understanding the impact of different types of exercise on this joint.
The specific exercise regimen was designed using research that has established the activity of APL in a variety of positions and activities.9,14,22 However, it has not been established whether the exercises are effective in activating and strengthening APL. These studies were done in the normal population and activity of APL may be different in patients with OA. Level one exercise in Taylor's regimen involves moving the CMC joint and this is contradictory to the dynamic stability concept 23 which proposes that initially the joint needing to improve stability should be statically controlled while movement occurs at the joints in close proximity. This would suggest that the CMC joint should be actively held still while controlled selective movement is produced at the other joints of the thumb.
Pinch strength was not significantly improved in either group, suggesting the exercise carried out was of insufficient intensity. Participants were instructed to do 10 repetitions of each exercise 3–4 times a day which would generally be considered adequate in clinical practice, this was recommended by Taylor 8 for her regimen and was used successfully along with splintage to increase pinch strength by Wajon and Ada. 5 In this pilot study compliance was not formally assessed; it was encouraged by giving written information, one to one teaching of the exercises and regular follow-up. It was noted by the treating therapist that participants found it hard to carry out the specific exercises which may have affected compliance. In planning any future study attention would need to be given to ways of monitoring compliance to evaluate whether sufficient exercise was carried out to achieve the desired effect. Measures to enhance compliance with exercise and reduce loss to follow up are needed, e.g. exercise diaries, goal setting around functional problems and problem solving any barriers to exercise and attending appointments at each attendance. Other studies on exercise in this group have also encountered problems with attendance, losing more participants the longer the follow-up period extends, e.g. 15% (6) by six weeks 5 and 39% (30) participants by 32 weeks, 7 this loss to follow up needs to be taken into account in sample size calculations.
It is interesting to note that those who did not attend follow up were those with higher pain scores and lower DASH scores, but not a particular stage of disease. We do not know if this was because they all found exercise unhelpful. One participant who withdrew certainly expressed this view. Treatment diaries detailing intensity and frequency of exercise, symptom response and problems encountered would provide a patient perspective on the effect of exercise, aid analysis of the effect of exercise and assist in educating the participant to exercise safely.
Studies looking at timing of exercise intervention with regard to other modalities, e.g. splinting, joint protection and task modification and in relation to stage of disease would be helpful. The majority of participants in this study already had splints. Clinical experience and research shows exercise will be better tolerated by a mildly symptomatic joint and benefits gained are more likely to be maximized by joint protection and task modification techniques. 24 This pilot trial mirrored current clinical physiotherapy practice; it did not control for other interventions making it hard to be certain changes seen were due to exercise alone. Trials with an optimal package of care plus or minus exercise would control for the other variables while not denying participants standard treatment.
This study recruited both hands in participants with bilateral thumb CMC joint OA, which meant data for a given person had to be averaged as it could not be assumed each thumb was an independent case. A better approach would be to recruit a single hand per participant. Finally as it is impossible to blind the therapist giving the exercise intervention, training should be given regarding using a consistent attitude and approach to avoid bias towards a particular form of treatment.
Conclusions
This pilot study indicated that in this sample specific exercise was not superior to general exercise, neither did it improve function or pain, nor increase APL or pinch strength. General exercise did seem to improve function, pain and also demonstrated a trend of improvement in APL strength. Increased APL moment was related to improved functional outcome. The general group had significantly higher APL moments at entry than the specific group.
The findings of this pilot study cannot be used to guide any general recommendations regarding the specific exercise regimen for clinical practice; however, they do raise questions about the widespread use of a regimen of exercises that lacks any clinical evidence to support its use. Further research should look at exercise from several different aspects:
Optimal timing with regard to disease stage, in relation to other conservative treatments and in relation to symptom severity.
The type of exercise (range of motion, stability or strength) with indications and contraindications for each type. Developing and validating an exercise prescription pathway, general exercises may be more appropriate for a patient presenting with joint stiffness, muscle shortening and weakness, stability for normal range but abnormal movement patterns.
Understanding whether the specific exercise regimen does strengthen APL in the presence of OA pathology.
Assessment of the dynamic stability of the first CMC joint.
Footnotes
Acknowledgements
Audrey Parks, Mary Bradley and Melanie Arundell for their support. Steve Attfield for his assistance in making the APL device. Apostolos Fakis for his statistical work and Simon Mockett who sadly passed away before this project was complete, for his endless and untiring support for this project.
Exercise regimens
Frequency: 3–4 times per day. All exercises are performed resting on the little finger side of the hand with the wrist extended back slightly.
APL tester
This was manufactured specifically for this study. It consists of a metal base plate covered with a thin layer of foam and a metal moveable bar upon which the patients press (using the APL muscle) this forces the bar onto another metal plate containing a load cell transducer. This transducer connects to a digital display unit reading force in Newtons (Figures 2 and 3). The equipment is adjustable for right and left hands. To improve reliability the equipment was used in a standardized position with one investigator taking the measurement (BD).
APL testing equipment showing digital display APL testing equipment showing test position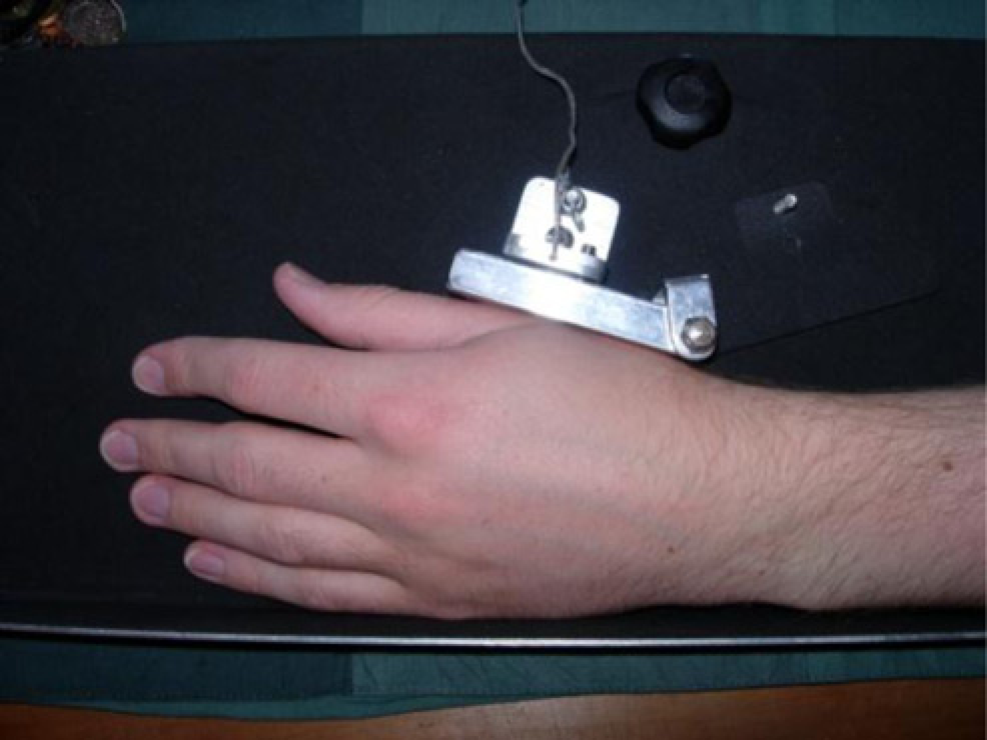

Eaton and Littler classification system for grading OA 15
Sample size calculation
The power calculation could be based on the common standard deviation of changes of DASH scores from baseline to six months from this study (18.9) and the minimum important difference of 12.7 points 16 between the two groups. Assuming power of 90% and significance level of 5% then 96 participants should be recruited in total. Adjusting the sample size for 41% attrition rate at six months that was observed in this study then 164 participants should be recruited in total.
Frequency: 3–4 times per day. All exercises are performed resting on the little finger side of the hand with the wrist extended back slightly.