
Abstract
Introduction
Medical treatments have limited long-term effect in task-specific dystonia. Whilst evidence supports the use of rehabilitation, no randomised controlled trials have been undertaken. This small-scale study determined the feasibility of implementing and evaluating a mixed sensory–motor task-specific dystonia rehabilitative programme.
Methods
Participants with writer’s or musician’s dystonia were recruited from a movement disorder and hand therapy clinic. Feasibility measures were recruitment rate, retention, session attendance, adherence to exercises. Self-report measures at 0, 3 and 6 months included: Arm Dystonia Disability Scale (ADDS), Tubiana and Chamagne Scale (TCS), Brief Illness Perception Questionnaire (BIPQ), Health Status (EQ-5D 5L), Clinical Global Impression Scale (CGI). Task performance was video-recorded at baseline and 6 months. At 6 months, interviews explored participant experiences of the intervention.
Results
Fifteen patients were recruited over 6 months (rate 2.5/month, musician’s dystonia = 8, writer’s dystonia = 7). Complete data sets were collected for twelve people(80%). The programme comprised a maximum six sessions plus daily home exercises. Nine completed the home programme at ≥75%. No adverse events were reported. Effect sizes at 3 and 6 months, respectively, were ADDS 3-month = 0.28, 6-month = 0.23; TCS 3-month = 0.13, 6-month = 0.53; BIPQ 3-month = 0.38, 6-month = 0.71; EQ-5D-5L 3-month = 0.34, 6-month = 0.59; video analysis at 6 months = 0.78. Eleven (92%) improved on the CGI. Interviews supported acceptability of the intervention.
Conclusions
This intervention was feasible to deliver with high retention, adherence and acceptability. Improvements occurred across measures. This informs the development of future randomised controlled trials.
Introduction
Task-specific dystonia (TSD) is a subtype of dystonia in which an abnormal posture occurs during the performance of a specific, usually highly skilled task, such as playing a musical instrument (musicians’ dystonia, MD) or writing (writers’ dystonia, WD). It can be very disabling, especially for professional musicians, with up to 62% of affected patients unable to continue their performance careers. 1 The pathophysiology and aetiology of TSD is not completely understood. It is thought likely to be related to sensorimotor system alterations potentially caused by interaction between the continued repetitive practice of a highly skilled movement in the face of imposed intrinsic (e.g. fatigue or injury) or extrinsic (alterations in technique or mechanical demands) changes. Correspondingly, there is experimental evidence for both motor and sensory dysfunction (such as altered inhibition within motor cortical areas and alterations in the delineation of the sensory homunculus representing the affected part) 2 as well as a wider cognitive context that includes an abnormal attentional focus during performance, anxiety and perfectionism. 2
Existing medical treatments such as oral medications (e.g. trihexyphenidyl) and botulinum toxin injections are limited in their long-term efficacy. 3 There is an increasing interest in using specific rehabilitative techniques which include: sensory re-education,4–8 sensory motor retuning,9–13 mirror therapy 14 and slow-down exercise treatment. 15 However, randomised controlled trials (RCTs) of these interventions have not yet been undertaken.
Given that there is pathophysiological evidence for mixed sensorimotor dysfunction in TSD, our hypothesis is that a mixed sensory–motor rehabilitation approach would be effective in improving function. There is need for a full-scale blinded RCT to investigate the efficacy of such an intervention in improving the function and quality of life of persons with TSD. However, beforehand a feasibility study is warranted to ensure the operational components are appropriate. Thus, we had two main aims. The first aim was to assess the feasibility (patient acceptability and adherence) of providing a mixed (supervised and home-based programme) of sensory–motor rehabilitative activities currently offered as “usual care” in an outpatient hand therapy practice. The second aim was to evaluate operational elements of the trial design related to participant recruitment, retention and suitability of the assessment process and outcome measures. To achieve these aims this study had several objectives (Table 1).
Study objectives.

Methods
This was a small-scale, single-group feasibility study. The intervention was delivered as part of routine clinical practice, at an outpatient hand therapy clinic, and the assessments were approved by the local ethics committee (North West London Research Ethics Committee 1. Ref: 11/LO/0307) and carried out at a specialist neurological hospital. Informed written consent was obtained from all participants. Figure 1 provides an overview of the study design and participant pathway.

Study design.
Participants
The study recruited consecutively eligible participants over a 6-month period, from a movement disorder clinic at the National Hospital for Neurology and Neurosurgery and a private hand therapy clinic, London Hand Therapy. Participants were eligible for inclusion if they were: aged ≥18 years of age, with a diagnosis of TSD affecting writing or musical performance made independently by two neurologists specialising in movement disorders (MJE, AS, AM, IP) and symptoms causing sufficient impairment for the patient to request treatment. Exclusion criteria were the presence of another neurological (e.g. peripheral neuropathy) or musculoskeletal condition that could impair hand function, ongoing treatment with botulinum toxin injections into any muscles of the affected upper limb and the receipt of hand therapy or physiotherapy in the last 12 months. Of those who met the inclusion and exclusion criteria, all accepted to participate in the study apart from three people who were declined by the research team due to funding limitations.
Intervention: sensory–motor rehabilitation therapy
The intervention was designed so that it could be implemented in publicly funded clinical practice and included a self-directed home exercise program framed within clinical therapist encounters. For this feasibility study a specialist hand therapist with more than 18 years of experience treating TSD (KB) carried out the mixed sensory–motor rehabilitative therapy. The intervention combined four previously published specific treatment approaches to TSD and five generic hand therapy treatments. A summary of treatment approaches can be seen in Table 2. The treatment sessions were standardised, apart from minor changes such as accommodating positions to make them more comfortable, and notes were taken at each treatment session for all individuals.
Summary of treatment approaches.

The intention was for participants to receive a maximum of six therapy sessions over a 6-month period: initial appointment (60 min), first follow-up appointment 1 month after initial appointment (60 min) and then each further follow-up appointment at six weekly intervals (30 min each). Participants were requested to undertake a home exercise programme which was integral to this rehabilitation programme. They were asked to complete a daily log by hand or electronically. The recommended amount of each exercise was indicated on the written home exercise log and patients were asked to accurately record the time they spent undertaking the exercises.
Feasibility outcomes
Feasibility measures were recruitment rate over the 6-month period, retention, attendance at therapy sessions and adherence to the home exercise programme (quantified using the patient-reported daily log). There is no guidance regarding the minimum intensity and frequency of rehabilitation required to gain an effect; however, from a theoretical perspective it is more likely that an effect will be gained if adherence levels are high. With this in mind, together with clinical experience and feedback from patients as to what was a “reasonable” rate of adherence, we decided a priori that acceptable adherence was attendance at ≥75% therapy sessions and completion of ≥75% or more of prescribed home exercises. Adverse events were to be recorded in the clinical notes by the clinician and/or in the home exercise log by the patient. Participants were asked their opinion of the effectiveness of individual therapy components on a three-point Likert scale (anchored with effective and not effective).
Clinical outcomes
The following standardised and validated patient-reported questionnaires were collected at baseline, 3 and 6 months into the intervention:
(1) (2) (3) (4) (5)
At baseline and 6 months a standardised video recording was undertaken to capture a clinician-rated assessment of change. Musicians were asked to play a piece that exacerbated their dystonia for 2 min and a mezzo forte legato scale of two octaves 15 times at a speed of eight notes per second (metronome paced). For the free playing the tempo was defined at the baseline assessment and the piece was repeated at the same tempo at 6 months. Participants with writing dystonia were video-recorded writing a standard sentence 10 times, writing five lines of interconnected ‘l’ with 10 letters per line. Two neurologists (MJE, LR) blinded to the treatment session rated videos according to the following scale: no impairment (1), mild impairment (2), moderate impairment (3), severe impairment (4). Scores were generated for both the predetermined sequence (interconnected ‘l’ or scale) and the free task production (writing sentence or piece).
Qualitative interviews
All participants were invited to undertake a brief semi-structured interview to ask them about their experience of engaging in the hand therapy intervention and home exercise programme. These brief, audio-recorded interviews were undertaken by the primary researcher (KB). They were transcribed verbatim, coded and thematically analysed.
Data analysis
This was a feasibility study, and hence inferential statistical analysis and hypothesis testing of the outcome measures is not appropriate and thus was not undertaken. 35 Both the patient characteristics and change in outcomes were investigated using descriptive statistics and the calculation of effect sizes (between baseline and 3 months; and baseline and 6 months) according to Cohen’s d. 36 An effect size (ES) of 0.8 is considered large, an effect size of 0.5 is considered medium and effect size of 0.2 is small. 37 Statistical analysis was run using SPSS (version 24).
Results
Over the 6-month recruitment period 15 patients met the inclusion criteria and were recruited, eight with MD and seven with WD.
Feasibility outcomes
The mean recruitment rate was 2.5 per month. In terms of retention, 12 (80%) of the recruited subjects completed the study. Table 3 provides a summary of the sample's demographic and diagnostic characteristics. Two patients dropped out of the study due to a lack of motivation (one before the commencement of the therapy and another after two therapy sessions as they stated that they did not want to complete the home exercise programme). A third patient stopped the study after 10 weeks due to developing a shoulder tendinopathy on the non-dystonic side, this was not related to the intervention or participation in the trial. For those completing the study, there was a 97% attendance rate at therapy sessions. Of the 72 therapy sessions offered (12 subjects with the possibility of six sessions each), only two sessions were not attended due to significant personal events (family funeral, patient in labour). Nine of the 12 participants completed the home exercise programme at ≥75% (all writing dystonia patients, four (57%) with MD). Two of the 12 (16.67%) reported finding the home exercise programme too arduous and too intense to complete (one from each patient group). No adverse events were reported.
Clinical characteristics for recruited participants (n = 12).
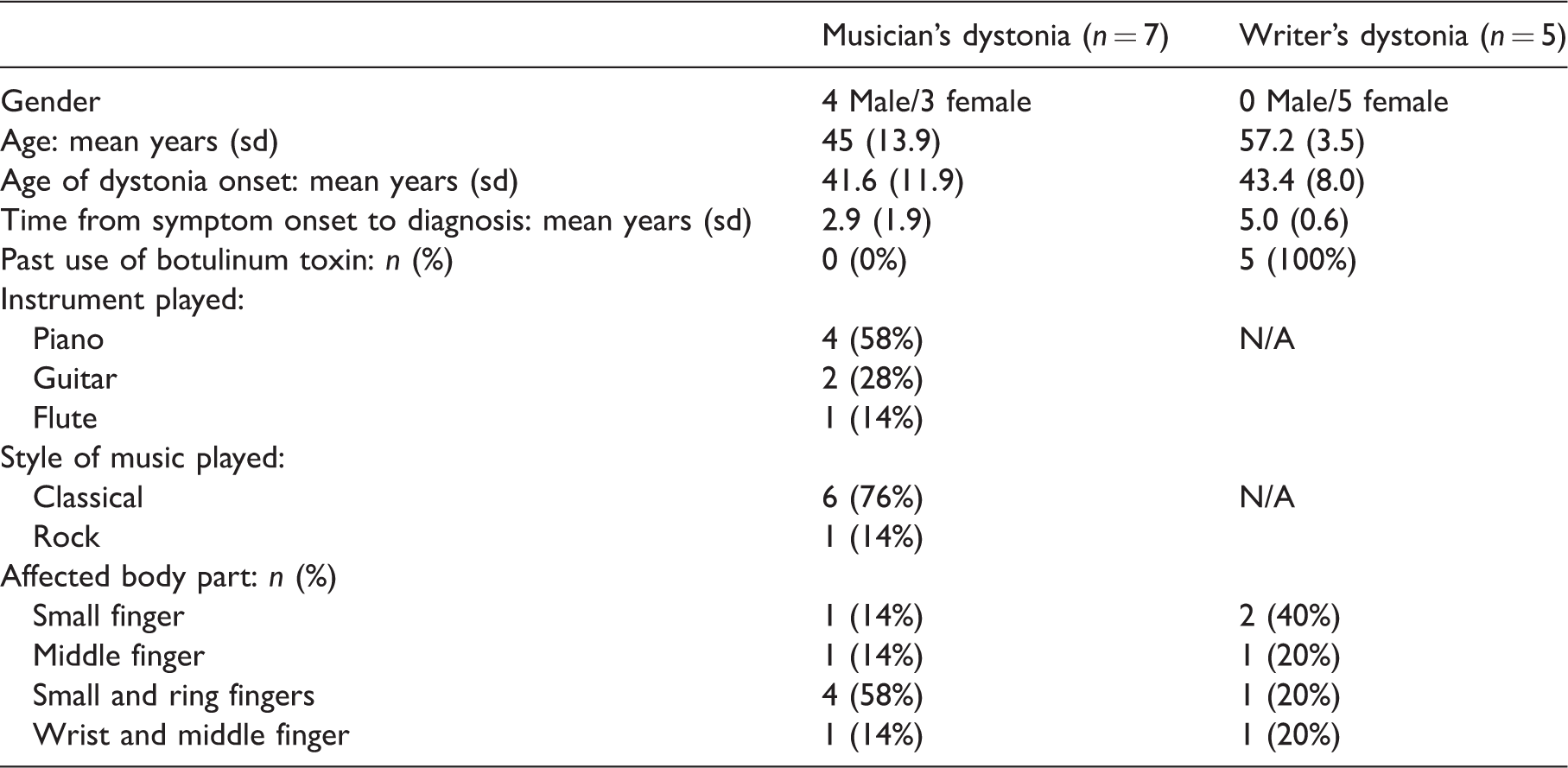
N/A: not applicable.
Data pertains to all participants who completed the study.
Clinical outcome measures
Table 4 summarises the outcome measure results, at each time point, for the 12 participants who completed the study. The effect sizes demonstrated that there were small improvements from baseline in the patient-reported ADDS at the two assessment points. There were small-to-medium patient-reported improvements in the Tubiana Champagne Questionnaire, the BIPQ and perceived health status (EQ-5D 5L score); with scores on each of these measures continuing to improve over the timeline of the study. The clinician-rated video analysis showed moderate improvements over time with sensory–motor rehabilitation therapy.
Changes in clinical outcomes at baseline, 3 and 6 months (n = 12).

NA = Not assessed.
aScale only completed by musicians.
Qualitative interviews
All 12 participants who completed the study engaged in the interviews. The techniques reported by participants to be effective, neutral or not effective are shown in Figure 2. Patients affected by MD found the following treatments effective: sensory motor retuning (86%), slow-down exercise therapy (71%) and mirror therapy, shoulder range of motion and hand-strengthening exercises (43% each). Patients affected by WD found the following treatments effective: hand-strengthening exercises (80%) and sensory–motor retuning, shoulder range of motion and slow-down exercise therapy (60% each). None of the participants reported either soft tissue massage or ultrasound therapy to be effective.
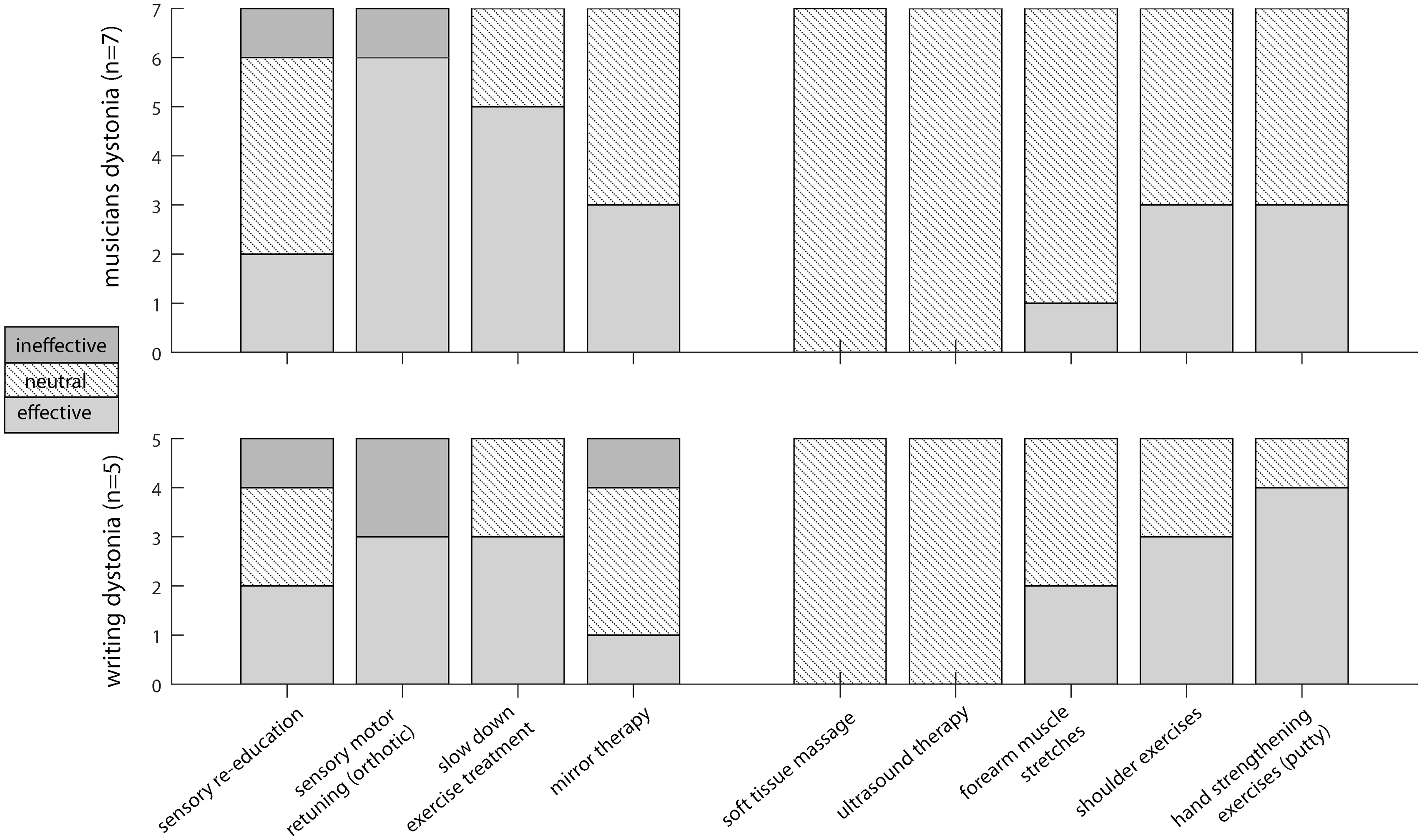
Effectiveness of specific therapy techniques (participant reported).
Three main themes were identified: (i) The impact of dystonia, (ii) individuals respond differently to different treatment techniques and (iii) changes require persistence and can take time (Table 5).
Overview of qualitative results.
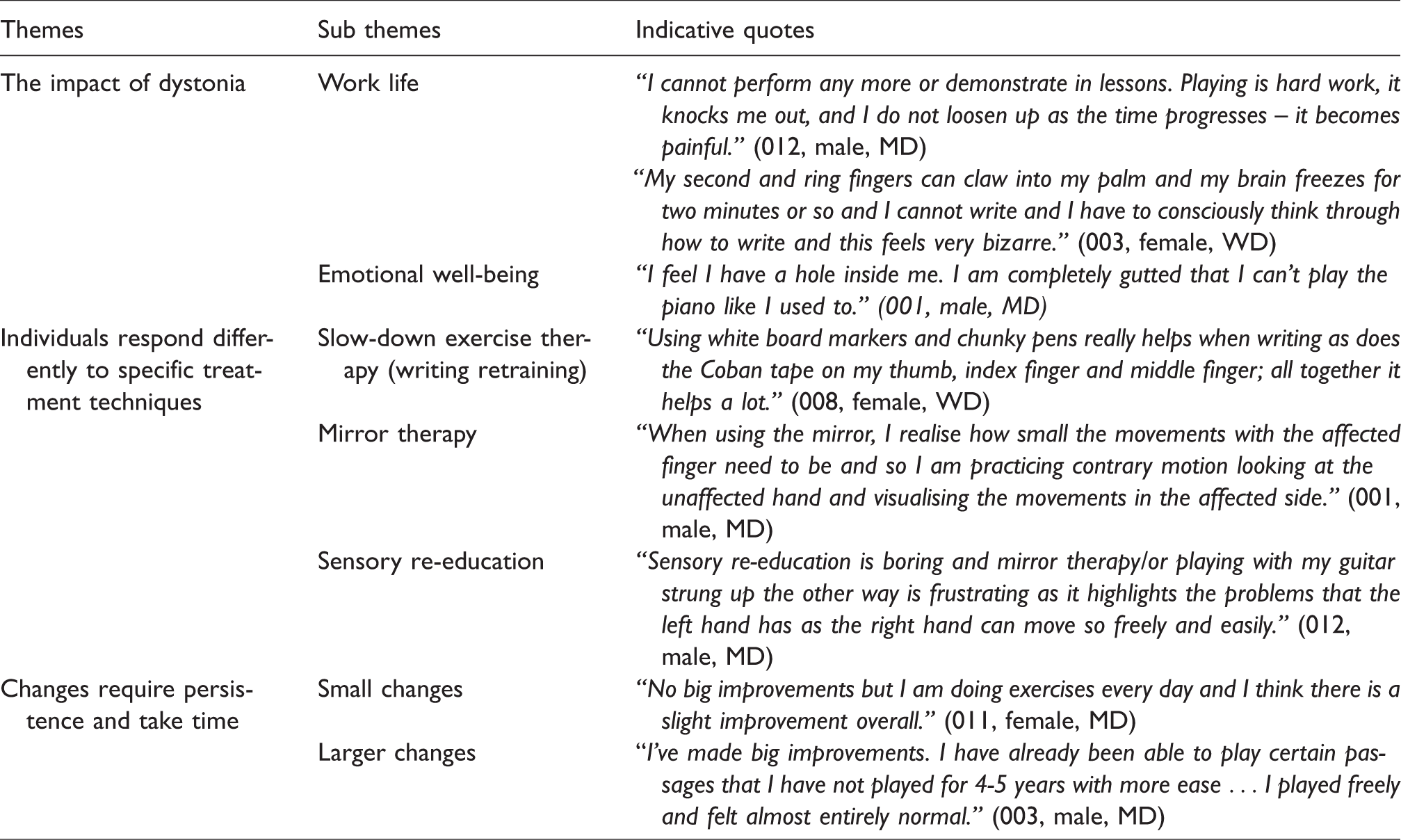
Theme 1: the impact of dystonia
All the participants described the negative impact of dystonia on their lives, which resonates with the findings of other qualitative work. 38 In particular, the participants described the specific physical impairments they experienced which impacted upon their ability to carry out tasks and professional activities. This marked impact on people’s emotional well-being was striking but is not surprising given that these symptoms typically reach their peak at the high point of the musicians’ professional career and can render them unable to play and indeed at times never able to return to their profession. This impact on emotional well-being is in line with the findings of other studies, which demonstrate a tendency towards perfectionism and anxiety in musicians developing focal dystonia. 39 Interestingly, subjects with WD often see the condition as “inconvenient” rather than career-threatening, likely because difficulties with writing can be compensated for more easily in employment compared to difficulties with playing a musical instrument for a professional musician.
Theme 2: Individuals respond differently to different techniques
People’s perception of their response to specific treatment techniques varied. This variation in response differed over the timeline of the study. For example, some participants initially found the exercises frustrating and with little improvement in their function, but reported noticing marked improvements over time.
Several participants commented that these rehabilitative treatment approaches were preferable to medical interventions such as Botulinum toxin: “I had three sessions of Botox but I found it made my hand weak and not functional, I couldn’t do buttons up or hold a key or write at all and therefore I have not had any more. I’m now using a Bic biro with a lot of Coban tape to build it up and it really helps the feeling of freedom and ease of writing – my hand still sometimes gets tense and I need to shake it out but my forearm does not get tense now.” (010, female, WD)
Theme 3: Changes require persistence and take time
Many of the participants reported that the changes in symptoms and function took time and required patience and persistence, and could sometimes be demoralising. For some the changes were small, whilst others noted larger improvements.
TSD is a complex condition that affects individuals in a variety of ways: emotionally, physically and in specific task performance such as writing or playing a musical instrument. Use of a variety of individual techniques in combination seems to assist most people, but this requires time and commitment from patients to actively engage in the rehabilitation process.
Discussion
Here we have reported data from a feasibility study of a specific sensory–motor rehabilitation therapy programme for people with TSD affecting writing and musical performance. This intervention was feasible to deliver with high retention, adherence and acceptability to patients. Improvements occurred across measures and were typically larger at the 6-month compared to 3-month assessment, which lends support to an on-going therapeutic effect of hand therapy over time.
All patients who met the inclusion criteria and were invited to take part in the study agreed to do so. Perhaps the high acceptance rate was partially due to the hand therapy being funded by a grant and thus not incurring private patient fees. There are a range of published treatment approaches typically delivered alone in a high-intensity experimental setting that are arguably difficult to translate into routine clinical practice. The sensory–motor rehabilitation therapy programme we employed in this study is one we have used in routine clinical practice for many years, and is specifically designed to incorporate a range of previously described hand therapy techniques using a small number of face-to-face treatment sessions and a home exercise programme. The results of this feasibility study demonstrated that this intervention is acceptable to most participants. Adherence to attendance at the face-to-face therapy sessions and to the home exercise programme was above our 75% threshold in 75% of the participants. There were no adverse events reported related to the intervention.
One difficulty with designing treatment studies in patients with TSD is the lack of specific measures to assess symptom severity. 1 In this study we used a range of patient-reported and clinician-rated objective outcome measures. Of these, the most promising outcome measures in this study with respect to effect size were the patient-reported CGI and the clinician-rated video. At the end of the treatment, 50% of participants (2 WD, 4 MD) reported a good outcome (self-rating of much improved or very much improved), with a large ES on the CGI. A slight tailing off from perceived benefit was noted at 6 months in comparison to 3 months on the CGI. This suggests that either the patient reported CGI or the clinician-rated video of performance may be useful primary outcome measures in this patient group, with the BIPQ and health state as secondary outcome measures. These results demonstrate that in a future powered trial (alpha 0.05, 80% power), a sample size of 36 would be required if the primary outcome was the patient-reported CGI (6 month mean 3.08, 3 month mean 2.58, SD 0.51); 54 for the clinician-rated video score (6 month mean 1.89, baseline mean 2.50, SD 0.78); or 66 for the patient reported BIPQ.
When interviewed, all patients reported that dystonia had a negative impact on their lives emotionally and in work and functional activities. The treatments that individuals found useful were dependent on the person with many preferring therapeutic approaches rather than medical interventions. MD patients reported that sensory–motor retuning and slow-down exercise therapy were the two most effective treatments followed equally by mirror therapy, shoulder active range of motion exercises and hand-strengthening exercises. Hand-strengthening exercises were reported as being the most effective treatment in the WD group with sensory motor retuning, shoulder range of motion exercises and slow-down exercise therapy all equally being reported as effective. Time and persistence was required to note changes with some only having small and others having larger improvements.
While this feasibility study was not designed to assess the efficacy of this intervention, these results do provide supportive evidence of a positive treatment outcome in some patients across a range of outcomes. Uniquely compared to previous studies in this area we adopted a mixed rehabilitative approach, combining several specific and general therapies based on individual assessment and response. This approach is supported both by the patient-reported Likert scales evaluating effectiveness of specific therapy techniques and the qualitative interview data; participants typically found more than one therapeutic approach to be beneficial. We believe that it is reasonable to propose that in a future clinical trial this mixed rehabilitative approach be used, rather than selecting a single approach for all patients.
Study limitations
Ideally in establishing feasibility of a future RCT, we would have included a control condition, to determine the willingness of patients to be randomised, and likely retention rates for this group. Also, our sample size was small and we relied on self-report to assess compliance with the home exercise program. The hand therapy intervention was implemented by a single therapist and whilst this meant that the treatments were standardised this could be viewed as a limitation due to possible bias and lack of generalisability. As the hand therapy intervention was funded by a grant, the acceptance rate may have been artificially high. This may have also had an impact on participants being more motivated to attend the therapy sessions and complete the home exercise programme and log. The follow-up was limited to 6 months; ideally, longer-term follow-up of these patients would be of interest, as the treatment timeframe for this condition is considerable and often management of the symptoms is the focus rather than cure. Finally, in addition to asking people about their experience of engaging in the hand therapy intervention and home exercise programme, it would have also been helpful to seek their views, and the views of the clinical researchers, about the study processes and design features (such as acceptability of the recruitment procedures and outcome measures) to inform the design of a future RCT. 40
Conclusions
This intervention was feasible to deliver with high retention, adherence and acceptability. Improvements occurred across measures and were typically larger at the 6-month compared to the 3-month assessment, which lends support to an ongoing therapeutic effect of hand therapy over time. The findings provide data to help support the design and development of a future controlled trial for rehabilitation in TSD.
Footnotes
Acknowledgements
The authors thank Lucia Ricciardi for being involved in rating the videos.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The British Association of Hand Therapy and James Tudor Foundation enabled by the Dystonia Society UK assisted with part funding for this project. Anna Sadnicka is funded by a Guarantors of Brain Clinical Fellowship Award.
Ethical approval
Ethics approval was gained from University College London, NHS Foundation Trust, The National Hospital for Neurology and Neurosurgery (Reference 11/LO/0307). This study has therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed consent
All persons gave their informed written consent prior to inclusion in the study. Details that might disclose the identity of the subjects in the study have been omitted.
Guarantor
KB.
Contributorship
KB and MJE researched literature and conceived the study. KB, AS and MJE were involved in protocol development, gaining ethical approval and patient recruitment. KB, AS, A-M M, IP were involved in data collection. KB was involved in implementing the intervention. KB, JF and AS were involved in data analysis. KB wrote the first draft of the manuscript and MJE, AS, JF and JM amended this draft. All authors reviewed and edited the manuscript and approved the final version of the manuscript.