
Abstract
Introduction
Upper extremity injuries are common, and often treated by occupational therapists. The need to evaluate the effectiveness of occupational therapy interventions to guide practice is pertinent. This systematic review and meta-analysis investigate the effectiveness of occupational therapy-led computer-aided interventions among adults with conditions of the hand, wrist, and forearm.
Methods
A systematic literature search of five databases was undertaken for randomized studies examining occupational therapy-led computer-aided interventions for the treatment of hand, wrist, and forearm conditions. The primary outcome was function, with secondary outcomes of pain, grip and pinch strength. The quality of the included studies was independently assessed using the Cochrane Risk of Bias V2 tool. Meta-analyses were completed.
Results
Three randomized controlled trials were included with 176 participants. One study reported on app use on a tablet and two studies reported on computer gaming. Participants had a variety of hand and wrist diagnoses, treated both conservatively and operatively. There is limited evidence demonstrating that computer-based interventions are as effective as other occupational therapy-led interventions in improving function, pain, grip and pinch strength post-intervention, including small effect size following meta-analysis: grip strength (Fixed Effects Model, SMD 0.13, 95% CI 2.63; –2.36, I2 = 0%) and pinch strength (Fixed Effects Model, SMD –0.12, 95% CI 1.25; -1.50, I2 = 11%).
Conclusions
Limited evidence was found to support the use of computer-aided interventions for adults with a hand, wrist or forearm injury. Further high-quality research is recommended inclusive of a broader range of technologies and a broader range of clinical and patient-reported outcome measures.
Introduction
Hand and upper extremity injuries are a common occurrence, 1 affecting all age groups. According to the National Centre for Health Statistics in America, 26% of injury-related emergency department presentations nationwide were in relation to the hand and upper extremity. 2 Conditions and injuries of the hand can have serious consequences, affecting a person’s ability to function and carry out daily activities including self-care, work, and leisure activities, and may lead to mood disorders and trauma-related stress.3–5 Occupational therapists are key healthcare professionals in the provision of care to people with an upper limb condition with studies demonstrating the effectiveness of occupational therapy for those with chronic hand conditions, 6 after hand injury, 7 and after hand surgery. 8 To improve patient outcomes, occupational therapists draw on a diverse range of intervention types to achieve patient goals, including exercise programmes, 9 splinting and orthosis provision, 10 occupation-based intervention, 11 joint protection programmes, 12 and more recently technology and computer-aided interventions.
A serial, cross-sectional analysis of United States of America nationally representative data from the National Health and Nutrition Examination Survey (NHANES) found the prevalence of computer use among adults increased from 29% to 50% between 2003 and 2016 and from 15% to 53% for those aged 65 years and over. 13 Reduced uptake of technology use among older adults has been a focus of attention in recent years, however, a recent Canadian study found internet use increased from 32% to 68% among those aged 65 and older between 2007 and 2016. 14 The use of technology in healthcare settings has grown in recent years and has been proven as an effective method of delivering healthcare rehabilitation to populations including stroke, Parkinson’s disease, chronic pain, and musculoskeletal conditions.15–17 Video gaming has been used to provide a distraction for those with chronic and acute pain18,19 and as a means of providing health education. 20 In a systematic review including 38 randomized controlled trials investigating the role of video gaming in improving health-related outcomes for a variety of physical and psychological conditions, the authors found there is potential for video games to improve health outcomes including psychological therapy outcomes, physical therapy outcomes, and health education outcomes. 21
Computer-aided interventions are diverse and include the use of gaming and applications on tablets, touchscreens, and smartphones. This diversity lends itself to the use of stimulating and interesting programmes and has the potential of being more widely accessible, not only in clinics and hospitals but in homes. From a clinician’s perspective, computer-aided interventions offer the opportunity for ‘real time’ grading of exercises and activities, data analysis, interesting content, and improving function.15,22,23 Adherence to therapy programmes has long been problematic in healthcare with low adherence associated with poorer functional outcomes24–26 and disuse, stiffness and disability in those with a hand condition. 25 Home exercise programmes provided by clinicians such as occupational therapists, physiotherapists, and surgeons, have been proven to be effective in the rehabilitation of upper limb conditions.27–30 However, studies have reported that up to 65% of patients are not adhering to their prescribed upper extremity home exercise programme.31,32 Whilst these programmes are typically paper-based, there is a growing body of evidence reporting the benefits and acceptability of computer use to help increase adherence. 33 Alongside adherence, the potential for improved function and accessibility to treatment has been reported in the literature. A randomized controlled trial demonstrated that a tablet application ‘ReHand’ improved functional outcomes in participants post carpal tunnel release at 4 weeks. 34 In a recent cross-sectional cohort study participants’ use of a smartphone app to complete an exercise programme and to access information about their condition was assessed using the Mobile Application Rating Scale (MARS) questionnaire. 35 The authors found the Hand Therapy app was perceived as ‘above average’, with a score of 3.5 overall out of five, and mean scores found to be above average for the subsets of engagement, aesthetics, functionality, and subjective quality of the app on the MARS questionnaire. In a two-arm trial of two occupational therapy interventions on hand disability among people with early diffuse cutaneous systemic sclerosis, participants in a home-based ‘App Alone’ group improved equally to the ‘intensive group’ of in-person occupational therapy at 18 weeks. 36 Whilst the use of technology in treating a variety of conditions such as stroke and Parkinson’s Disease is reported to improve patient outcomes and as a mechanism for providing health education, few have investigated its role in injuries and conditions of the upper limb, particularly within occupational therapy literature. Computer and smartphone use is prevalent across all age groups, and are relatively inexpensive devices that can be made available in clinics or used in the delivery of home hand therapy programmes. Given the prevalence of upper limb conditions and the need to provide evidenced based diverse interventions, the purpose of this review is to locate and synthesise current available evidence regarding the effectiveness of occupational therapy led computer-aided interventions for adults with a condition or injury of the hand, wrist, or forearm in relation to function, pain, and strength outcomes.
Methods
The review protocol was registered on PROSPERO (CRD42022371593). There were no deviations from the pre-registered protocol. This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2015 statement37,38 (Supplementary Material 1). The methodology for the review was informed by the Cochrane Handbook for Systematic Reviews of Interventions. 39
Search strategy
Searches were carried out in CINAHL, Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE (OVID), EMBASE, and PubMed in November 2022. No restriction on the studies’ publication date was applied and databases were searched from the date of inception. MeSH terms and associated keywords were used covering the topics of hand, wrist, forearm, occupational therapy, hand therapy, computer, tablet, and application use. The reference lists of all eligible studies were hand-searched for further relevant studies. A search strategy example is provided in Supplementary Material 2.
Inclusion criteria
Population
Studies involving adults (18 years of age or more) with a hand, wrist, or forearm condition or injury, for example, fractures, tendon injury, nerve injury, and carpal tunnel syndrome were included in this review. The condition or injury had to impact primary or secondary outcomes (described below) to be included in this review.
Intervention
Interventions provided by an occupational therapist using computer-aided interventions. Computer-aided interventions include computer-based exercise programs, gaming, video, or applications such as those found on smartphones or computer tablets.
Comparator
Usual care or another active intervention was compared to occupational therapy computer-aided intervention within this review.
Outcomes
The primary outcome was functional ability post occupational therapy intervention, measured using a validated scale, such as the Disabilities of the Arm, Shoulder and Hand (DASH). 40 Secondary outcomes include pain and grip and pinch strength utilising outcome tools such as the Visual Analogue Scale 41 and Jamar dynamometer (J. A. Corporation, New Jersey, USA).
Study Design
All randomized controlled trials (RCTs), quasi-RCTs, controlled before and after studies, and interrupted time series (ITS) designs were included.
Exclusion criteria
Studies were excluded if the population reported on was less than 18 years of age; if participants had a hand condition specific to complex medical complaints, for example, cerebrovascular accident (CVA); where the primary presentation was not concerning the hand, wrist, or forearm; studies targeting the shoulder or elbow and not the distal upper limb; where the primary treating clinician providing intervention is not an occupational therapist; and technologies which are not typically readily accessible within homes and clinics, such as virtual reality and robotics. Observational studies were excluded as well as experimental studies that did not randomize participants to intervention and control groups.
Study selection and data extraction
References generated from the search were exported to Endnote software, where duplicates were removed. Two authors (MS and AMM) independently screened all studies by title and abstract for eligibility. Eight studies were selected by the reviewers as meeting inclusion criteria and underwent full text review. Conflict regarding eligibility arose for two of the articles and a third author (KR) was consulted. A final decision was made by the third author following discussion with all three authors. Figure 1 details the process of identifying studies. Prisma flow diagram.
Data were extracted from included studies by one reviewer (MS). A second author (AMM) independently checked 20% of the data extracted and confirmed accuracy and appropriateness. The information extracted included authors, year of publication, country, setting, study sample size, study design, outcome measures, and period of follow-up. Data were entered into a prepared Microsoft Excel document. The information extracted included authors, year of publication, country, setting, study sample size, study design, outcome measures, and period of follow-up. RevMan V.5.4.1 software was used to analyse the data for the meta-analysis. For the primary outcome of function, meta-analysis could not be completed. For continuous data, mean differences with 95% CIs were reported or standardised mean difference (SMD) and 95% CI were calculated where different methods of measurement were used. Heterogeneity was explored across the included studies by examining the participants' details, the content and duration of interventions, outcomes, and duration of follow-up. Heterogeneity was further explored visually, by inspecting the forest plots and the associated Chi 2 and I2 statistics. The I2 statistic was interpreted using a guide by Deeks and colleagues, 42 as strict cut-offs are no longer recommended.
Quality assessment
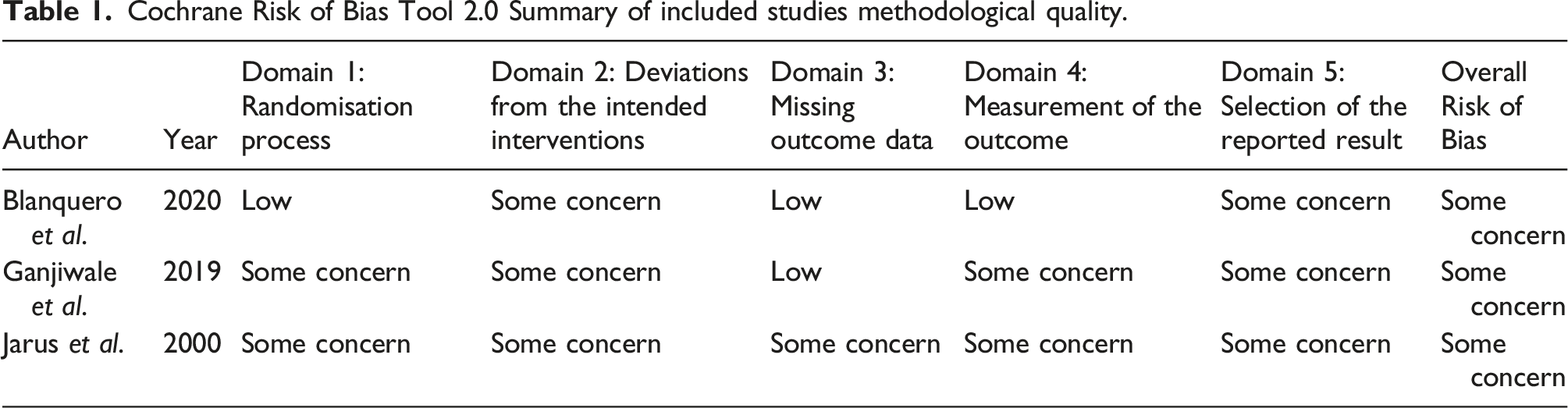
Cochrane Risk of Bias Tool 2.0 Summary of included studies methodological quality.
Dealing with missing data
Study data were not available regarding functional outcomes in one paper and the authors were contacted. 44 No response was received.
Results
Summary of included studies characteristics.
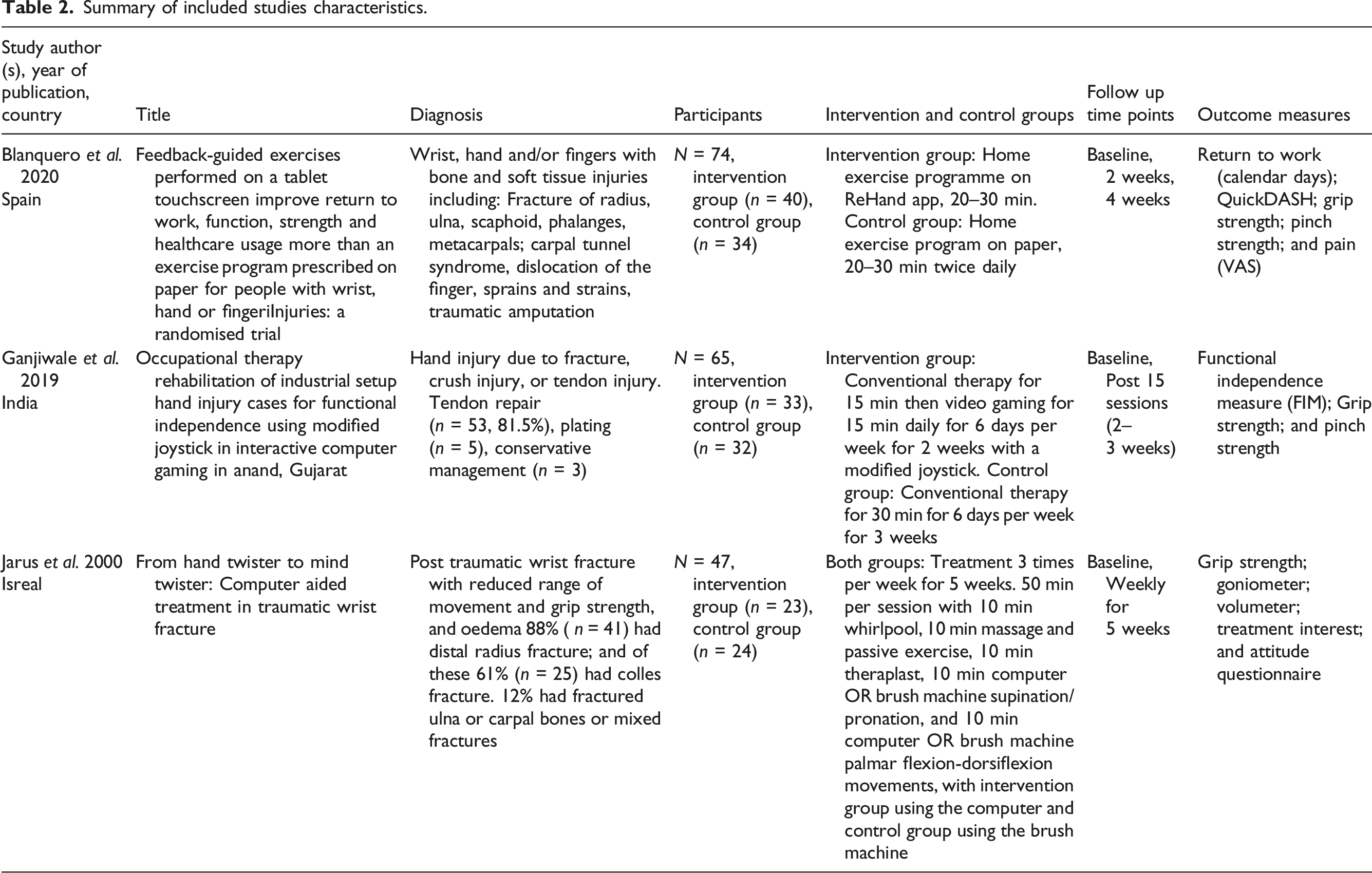
In relation to intervention type, one study reported on app use on a touchscreen tablet, 45 whilst the remaining two studies reported on computer gaming using a modified joystick. Intervention length varied from 2 weeks to 6 weeks across the three studies. Time spent on computer-based interventions was 15 min up to 30 min. One study 45 reported on the intervention group exclusively completing an individualised home exercise programme on a tablet app for the entire 20 to 30-min session compared to a control group completing paper-based activities; whilst the two other studies describe 15 to 20 min computer-based activities in addition to other modalities including whirlpool, Theraplast, massage, or passive movements over a session of 30 min 44 and 50 min. 46 Only one of the intervention programmes reported on was completed by the participants in their homes using a ReHand app. 45
Risk of bias findings
All studies received an overall rating of ‘Some Concern’ of risk of bias when assessed using the Cochrane Risk of Bias Tool 2.0. One study 46 was assessed as having ‘some concern’ of risk of bias across all five domains; similar to the Ganjiwale et al. 44 trial rated as ‘some concern’ of risk of bias in five domains. In contrast, Blanquero et al. 45 trial was deemed to have a ‘low risk’ of bias across three of the domains: the randomization process, missing outcome data, and measurement of the outcome.
Functional outcomes
Across the included studies, two of three evaluated function as an outcome44,45 using standardised outcome tools: the QuickDASH 40 and the Functional Independence Measure (FIM). 47 Blanquero et al. report a greater short-term improvement of functional ability as measured by the QuickDASH when assessed at week two (MD-12, 95%CI –22; –3). At week four the mean difference favoured the intervention group however did not clearly show the effect was beneficial (MD –11, 95% CI –25; 3). Ganjiwale et al. compared an intervention group receiving conventional occupational therapy and video gaming using a modified joystick to conventional occupational therapy alone. Findings suggest both groups were comparable regarding functional independence as measured by the Functional Independence Measure (FIM). Meta-analysis was not possible as data on the FIM was not available and was not received having contacted the authors. Overall, one study showed short-term significant differences in function, with two studies demonstrating no long-term difference in function.
Grip and pinch strength outcomes
Grip strength was measured across all three studies. Ganjiwale et al. reported results between intervention and control groups were comparable regarding grip strength using a Jamar hand dynamometer (J. A. Preston Corporation, New Jersey, USA). Jarus et al. completed a randomized controlled trial with an intervention group receiving treatment with a computer using a computer game “Revenge of Doh” (Taito Corporation, Tokyo, Japan) and a control group received treatment with a brush machine alongside conventional therapeutic approaches for both groups. Results show significant improvement in grip strength for participants in both intervention and control groups, with no significant differences between groups. Overall, two studies reported no difference in strength with one study reporting better strength in the intervention group. Meta-analyses demonstrated non-significant findings between groups in relation to grip strength (Fixed Effects Model, SMD 0.13, 95% CI 2.63; -2.36, I2 = 0%) post-intervention (Figure 2). Grip strength post-intervention.
Pinch strength outcomes
Pinch strength was measured across two studies.44,45 Meta-analyses demonstrated improvement in pinch strength (Fixed Effects Model, SMD –0.12, 95% CI 1.25; –1.50, I2 = 11%) post-intervention (Figure 3). Pinch strength post-intervention.
Pain outcomes
Blanquero et al. was the only included study to assess pain as an outcome. Using a visual analogue scale of 0–10 cm, mean estimates favoured the intervention group at week two and week four.
Other reported outcomes
Other benefits reported by Blanquero et al. include participants in the intervention group returning to work sooner and demonstrating a reduction in healthcare usage. Jarus et al. reported on the range of motion and level of oedema, with significant improvement in both intervention and control groups [48]. The authors utilised a Treatment Interest visual analogue scale to assess participants’ interest in their prescribed treatment. The computer-aided group showed significantly more interest in treatment than did the brush machine group.
Discussion
This systematic review aimed to locate, describe, and analyse the current evidence regarding the effectiveness of occupational therapy-led computer-aided interventions for adults with a condition or injury of the hand, wrist, or forearm. Following a comprehensive search of five databases, only three articles met the inclusion criteria. Across the three trials, one evaluated the use of an application on a touchscreen tablet and two evaluated a computer-based intervention using a modified joystick with forearm, wrist, hand, and fingers targeted movements to complete games. Participants’ ages ranged from 18 to 80 years and represented both males (58%) and females (42%). Regarding the primary outcome of function, two studies evaluated function as an outcome with one study showing a short-term significant difference in function, while both showed no significant long-term difference in function. Two of the studies demonstrated no difference in grip strength between groups whilst one study showed significantly better strength in the intervention group. Two studies measured pinch strength and meta-analysis revealed improvement for intervention groups. Mean estimates favoured the intervention group regarding pain reduction, however confidence intervals were too imprecise to indicate a truly beneficial effect. Despite non-conclusive findings, intervention and control groups had similar outcomes. Thus, the current review has added to the knowledge base that computer-based interventions have the potential to be as effective for this population as other occupational therapy-led interventions or as part of a multi-modal approach.
It is important in light of these findings to consider barriers and facilitators associated with the use of computer-aided interventions. Treatment adherence is identified as being of concern throughout an intervention, where patients can lose motivation when treatments become monotonous over time. 48 Patient non-adherence to treatment programmes is directly related to poorer functional outcomes and can limit treatment benefits, with the meta-analysis by DiMatteo et al. 49 reporting recovery as trebled in patients who adhere to treatment recommendations when compared to those who do not. One included study in the current review assessed treatment interest and reported participants had a significantly greater interest in the computer-based intervention than standard treatment, 46 this increased interest may support treatment adherence. In a recent systematic review 50 exploring interventions to aid therapy adherence in people with an upper limb condition, the use of audio-visual technology (DVD and videotape) and smartphone applications were found to be used increasingly with this population. Of the three included studies in this review, one is from the year 2000, 46 however two of the studies are recent, from 2019 44 and 2020. 45 This may indicate this is a growing area of investigation and the type of technology being used and reported on may be richer and broader in the coming years. The recent development of an online version of the Strengthening and Stretching for Rheumatoid Arthritis of the Hand program, mySARAH, 51 a tailored, progressive 12-weeks exercise program for people with hand problems due to rheumatoid arthritis is one example of the use of computers and handheld devices in delivering therapeutic interventions, with initial evaluation indicating mySARAH as feasible, acceptable, and beneficial to participants. 52 Computer-based interventions have the potential to offer diversity and stimulation to patients, in an accessible format, to increase adherence, and psychological and physical therapy outcomes.20,21,52
Controlled studies on the use of common gaming platforms such as Nintendo Switch® and Leap® were not found for the target population of this systematic review, despite their potential alongside conventional occupational therapy approaches in other health conditions. The use of technologies such as the Nintendo Switch® and virtual reality-based upper extremity training in the post-stroke population have been shown to improve functional and strength outcomes 53 and led to high satisfaction and compliance rates 54 when combined with conventional therapy.54,55 The use of an occupationally embedded computer-based intervention for persons with traumatic brain injury elicited significantly more upper limb range of motion versus rote exercise. 56 Gaming consoles such as Nintendo Switch® and Leap® are relatively inexpensive and programmes involving their use could be implemented in a person’s own home. Methodologically robust studies evaluating a wider variety of gaming consoles and virtual reality intervention in people with an upper limb condition could add to the evidence base regarding gaming and occupational therapy practice.
Despite a growing uptake of technology use among older adults, an age divide in the use of technology is reported, with lower usage among older adults compared to other age groups. This is attributed to factors including sociodemographic differences in exposure to technology, motivation, skills needed to use the Internet, and age-related onset of health problems. 14 Another barrier to the use of technology in healthcare is the lack of access and associated costs for some technologies. Therapists’ awareness of barriers and facilitators to the use of technology in practice is pertinent when implementing computer-aided interventions. The Technology Acceptance Model (TAM) and subsequent consolidated versions of the TAM in the Unified Theory of the Acceptance and Use of Technology (UTAUT) may assist therapists in understanding the processes underlying the acceptance of technology, to predict the behaviour of use and provide a theoretical explanation for the successful implementation of technology with patients.57,58 The UTAUT model describes seven primary factors that influence an individual's use of technology: (1) performance expectancy; (2) effort expectancy; (3) social influence; (4) facilitating conditions; (5) hedonic motivation; (6) price value; and (7) habit. 58 They found age, gender, and experience impacted some of these relationships. 58 It is advantageous for occupational therapists to be aware of such factors, including the barriers and facilitators in the implementation of computer-aided interventions to ensure correct and effective application.
Limitations were noted across the three included studies. Limitations in Blanquero et al. 45 study included non-assessment of adherence to the exercise programs, in addition to the study reporting on a wide variety of condition types, reducing clarity regarding the intervention effect for specific hand, wrist, or forearm conditions. Limitations noted in the Ganjiwale et al.’s 44 study include the intervention group being reported as having sessions across a 2-week period, compared to a 3-week period for the control group. This could have implications for the outcomes as there was a significant difference in the length of treatment time between groups. Jarus et al. 46 did not assess function or occupational performance, nor adherence to the programs described.
Given the prevalence of upper limb conditions and the need to evaluate and effectively report on occupational therapy interventions, it is important to continue to expand the evidence base through high-quality, methodologically robust, trials. This review was limited by the sparsity of randomized trials and the methodological quality of the studies included in this review. Within the current review, it was noted that not all studies assessed all outcomes primary and secondary, for example, function. Furthermore, in one of the studies that did assess function, the outcomes were not fully reported on, with a lack of data availability to draw conclusions or complete meta-analysis. 44 The Template for Intervention Description and Replication (TIDieR) 59 is an extension of item five of the CONSORT 2010 statement 60 and item 11 of the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2013 statement, and its use can help improve the completeness of reporting and the replicability of interventions reported on. 61 This, alongside utilisation of appropriate outcome measures, encompassing Core Outcome Measures in Effectiveness Trials (COMET) standardised outcome sets, is key to adding quality and value to future studies. A review of virtual reality and gaming consoles which have demonstrated positive findings for other populations with upper limb dysfunction, such as CVA, could add to the occupational therapy evidence base for those with a hand condition. Further research priorities include the need for robust trials evaluating occupational therapy-led computer-aided interventions reported in line with appropriate reporting guidelines.
Conclusion
Computer-aided interventions in occupational therapy practice for those with a hand, wrist, or forearm condition require further investigation. Generally, this review supports the premise that occupational therapy-led computer-based interventions using touchscreen and video games have promising yet limited evidence to support their effectiveness in terms of improvements in function, pain, grip, and pinch strength when compared to conventional occupational therapy approaches. Gaming may be utilised to complement hand therapy rehabilitation programmes where appropriate, alongside other evidence-based approaches.
Supplemental Material
Supplemental Material - Effectiveness of occupational therapy-led computer-aided interventions on function among adults with conditions of the hand, wrist, and forearm: A systematic literature review and meta-analysis
Supplemental Material for Effectiveness of occupational therapy-led computer-aided interventions on function among adults with conditions of the hand, wrist, and forearm: A systematic literature review and meta-analysis by Margo Sheerin, Ann-Marie Morrissey, Rose Galvin, Damien Ryan, Leonora Carey, and Katie Robinson in Hand Therapy
Footnotes
Acknowledgements
The authors thank the following people: The authors who kindly responded to requests for data or information, Annette O’Driscoll for her guidance on occupational therapy practice for conditions of the upper limb, and Shirley Reale for her support throughout completion of this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.