
Abstract
Gastroparesis (GP), defined as delayed gastric emptying (GE) without mechanical obstruction, is an underdiagnosed non-motor symptom of Parkinson's disease (PD) that may affect levodopa pharmacokinetics and contribute to motor fluctuations. In PD, GP pathophysiology involves Lewy pathology in the enteric nervous system, neurohormonal dysregulation, gut microbiota alterations, and adverse effects of medications, including levodopa. Disruption of the gut-brain axis further exacerbates gastrointestinal dysmotility, leading to malnutrition, reduced quality of life, and increased hospitalization rates. Clinically, GP delays GE, resulting in erratic levodopa absorption and unpredictable ON/OFF responses. Diagnosis is challenging due to symptom overlap with other gastrointestinal disorders and the lack of validated scales specific to GP in PD. Gastric scintigraphy remains the reference method for assessing GE, although its use is limited by methodological variability and interference from ongoing PD treatments.
This review critically examines the epidemiology, pathophysiology, and clinical consequences of GP in PD, and highlights its bidirectional relationship with levodopa pharmacokinetics, particularly its contribution to motor fluctuations. We discuss current pharmacological management strategies, with a focus on the efficacy and safety profile of domperidone. Finally, we propose the hypothesis that the future integration of digestive biomarkers and longitudinal clinical data could contribute to a more individualized treatment approach.
Keywords
Introduction
Parkinson's disease (PD) is a complex, heterogeneous, and progressive neurodegenerative disorder, classically characterized by motor symptoms such as resting tremor, rigidity, and bradykinesia. 1 Non-motor symptoms (NMS) are also a prominent component of PD and have received growing attention in recent years.2–6 Among them, gastrointestinal (GI) manifestations are widespread and disabling, affecting the entire digestive tract yet remaining underrecognized.
These symptoms can manifest as early as the prodromal phase, 7 several years or even decades before diagnosis, 8 and can progress over the course of the disease.9–11 Common GI manifestations include dental and periodontal disease, sialorrhea, dysphagia, gastroesophageal reflux, gastroparesis, and lower GI issues such as constipation or fecal incontinence.2,12–15
Despite their clinical burden, GI symptoms are often underreported and underestimated by patients and overlooked by clinicians.2,16–18 However, they significantly impair quality of life19–23 and are associated with weight loss, malnutrition,24,25 aspiration pneumonia, and increased hospitalization and mortality.3,4,26
Gastroparesis (GP), defined as delayed gastric emptying (GE) without mechanical obstruction, manifests through non-specific symptoms such as nausea, vomiting, early satiety, abdominal pain, and bloating.27,28 Beyond reducing quality of life, GP has critical therapeutic implications in PD. Although GP is, by definition, symptomatic, delayed GE itself may occur without symptoms. By impairing the absorption of antiparkinsonian medications and other drugs,12,29–31 both GP and delayed GE may reduce treatment efficacy and contribute to motor fluctuations (e.g. delayed-ON or no-ON responses).
To date, no specific guidelines exist for diagnosing or managing GP in PD. However, its identification and management may serve two critical goals: (i) improving patients’ quality of life through symptom control, and (ii) enhancing the efficacy of oral antiparkinsonian drugs, particularly at the motor fluctuation (MF) stage.
This review will examine (i) the prevalence, pathophysiology, therapeutic implications, and diagnostic strategies related to GP in PD; (ii) the bidirectional relationship between GP and dopaminergic treatment response; and (iii) pharmacological management options for GP in PD.
Gastroparesis in Parkinson's disease
Epidemiology
The exact prevalence of GP in PD is challenging to establish due to diagnostic variability, though studies have consistently confirmed its presence.32–36 Delayed GE is reported in 70–100% of patients,37,38 with up to 90% showing delayed GE for solids and approximately 40% for liquids. 39 Delayed GE may remain clinically silent or manifest through non-specific GI symptoms such as nausea, early satiety, bloating, postprandial discomfort, or abdominal pain.
GP may occur at any stage of PD. Although it tends to be more frequent and symptomatic in advanced stages,1,34,39,40 no consistent association with disease duration has been demonstrated. 39
Pathophysiology
The pathophysiology of GP in PD is multifactorial, involving impaired neurohormonal control of GE 41 and preprandial dysrhythmias affecting the baseline electrical rhythm,42,43 resulting in dysmotility. Dopamine plays a central inhibitory role in gastric motility, primarily through D2-receptor–mediated suppression of acetylcholine release in enteric cholinergic neurons, thereby reducing antral contractility and slowing GE. 44 In PD, dopaminergic dysfunction further disrupts autonomic and vagal pathways involved in the regulation of gastric motility, contributing to impaired GE. 45
This multifactorial impairment is driven by several pathophysiological mechanisms, including:
Degeneration of dopaminergic neurons in the central and enteric nervous systems (ENS), along with Lewy bodies spreading within the brainstem, vagus nerve, and gut, according to Braak's hypothesis32,40,46–49; Altered parasympathetic tone50,51 and dysfunction of cholinergic anti-inflammatory signaling, linked to gastric muscle inflammation and macrophage infiltration
52
; Lower levels of ghrelin, a pro-motility neuropeptide secreted during fasting53–55; Altered gut microbiota,
7
potentially affected by dopaminergic drugs, slowing transit and reducing levodopa bioavailability56–58; Medication-induced effects by some drugs,38,59–62 including antiparkinsonian agents that may directly impair GE through various mechanisms.63,64
Therapeutic implications
In PD, the GI tract plays a key role in the transit, metabolism, and absorption of drugs, particularly levodopa, the cornerstone of antiparkinsonian therapy. Levodopa is a hydrophilic dopamine precursor with a short half-life, mainly absorbed in the duodenum and proximal jejunum. 65 It is rapidly metabolized by aromatic L-amino acid decarboxylase (AADC) and catechol-O-methyltransferase (COMT). To enhance its bioavailability and limit peripheral adverse effects, levodopa is routinely co-administered with AADC inhibitors and often with COMT inhibitors to prolong its action. 66
Levodopa's intestinal uptake relies on active transport, competing with dietary amino acids.67,68 While not absorbed in the stomach, 69 delayed GE can impair its timely delivery to the absorption sites.
Contin et al. demonstrated that postprandial intake, compared with fasting, delays levodopa absorption, prolongs time to maximum concentration (Tmax), reduces motor response duration, and decreases the area under the curve (AUC) by 24%.70,71 Therefore, patients are advised to take levodopa on an empty stomach, ideally 30 to 60 min before meals or 1 to 2 h afterwards, and to limit protein intake at the evening meal. 72
Optimizing levodopa pharmacokinetics is essential for improving efficacy, reducing doses, and preventing both motor (e.g. OFF periods, unpredictable ON/OFF fluctuations, dyskinesias) and non-motor complications (e.g. mood and neuropsychiatric fluctuations). Moreover, continuous dopaminergic stimulation helps to avoid the pulsatile effects that sensitize nigrostriatal and mesocorticolimbic pathways, which contribute to dyskinesias and impulse control disorders, respectively. 73
Since GE strongly influences levodopa absorption, managing GP could significantly improve treatment outcomes. In early PD, improving GE may stabilize levodopa levels and delay dose escalation. In advanced PD, treating GP may reduce delayed or unpredictable ON responses and mitigate OFF periods. A better understanding and management of this GI dysfunction is essential for optimizing motor and NMS control throughout disease progression.
Diagnostic strategies
GP symptoms are non-specific and may mimic structural disorders such as peptic ulcers, partial gastric or small bowel obstructions, gastric cancer, or pancreatobiliary diseases. 74 In a study of 146 patients with GP of various etiologies (idiopathic 36%, diabetic 29%, post-surgical 13%, and PD-related 7.5%), the most common symptoms were nausea (92%), vomiting (84%), bloating (75%), early satiety (60%), and abdominal pain (46%), consistent with other findings.75,76
In PD, GP symptoms may overlap with GI adverse effects of dopaminergic treatments or NMS. While GP can often be suspected based on clinical history, Chaudhuri et al. reported that up to 62% of NMS in PD go unreported, due to embarrassment or lack of awareness, with GI symptoms underreported in 43.5% of cases. 16 This highlights the need for proactive screening and patient education.
Standardized clinical assessment and screening
To date, no validated, reproducible scale exists specifically for diagnosing GP in PD. However, standardized symptom assessment remains crucial for clinical monitoring and research consistency.63,77
The Non-Motor Symptom Questionnaire (NMSQuest) screens for various PD-related NMS, including GI symptoms (e.g. sialorrhea, ageusia, dysphagia, reflux, nausea, vomiting, constipation, and fecal incontinence). 78 Although validated in PD and correlated with Hoehn and Yahr stage, 79 it does not quantify symptom severity or diagnose GP.
The Gastrointestinal Dysfunction Scale for Parkinson's Disease (GIDS-PD) was developed to quantify GI dysfunction in PD, but still requires validation for routine clinical use, 80 and like the NMSQuest, it is not specific to GP.
The Gastric Cardinal Symptom Index (GCSI) is based on a self-assessment of nine symptoms over two weeks, scored from 0 to 5. It yields a global severity score by averaging the results of three subscales. While specific to GP and commonly used in trials,81–85 it has not yet been validated for PD. Importantly, the GCSI is not a diagnostic tool, as it reflects symptom severity and treatment response rather than delayed GE, and it does not include abdominal pain, despite this being a frequent symptom in GP. 86
Ultimately, symptom-based tools have limitations in their diagnostic capabilities. In a cohort of 572 patients with scintigraphy-confirmed GP, Balan et al. found that clinical suspicion had only a 29% positive predictive value. 87 Singh et al. further showed that symptoms of rapid GE may mimic those of delayed GE, underlining the limits of symptom-only approaches. 88
Challenges in objectively diagnosing gastroparesis in Parkinson's disease
While clinical evaluation and symptom scales may suggest GP, definitive diagnosis requires objective evidence of delayed GE without mechanical obstruction. 89
Gastric scintigraphy using a standardized solid meal remains the gold standard for the assessment of GE. According to recent international guidelines, 4-h protocols provide the highest diagnostic accuracy and reliability, whereas shorter protocols, particularly two-hour measurements, are associated with a higher risk of misclassification.90–92 In PD, however, the application of this reference method presents specific challenges. Strict adherence to 4-h protocols often requires withholding dopaminergic medication before and throughout the examination, which is frequently not feasible due to motor fluctuations, discomfort, and increased immobility. Early resumption of dopaminergic treatment is often necessary and typically requires water intake, a well-recognized source of bias in GE measurements. In addition, methodological variability (meal type, fasting duration, posture, acquisition settings) and clinical heterogeneity (disease stage, medication status) further limit reproducibility. As a result, studies report heterogeneous findings, ranging from delayed to normal or even accelerated GE, possibly related to the maintenance of dopaminergic treatment during testing, which for ethical and clinical reasons is rarely interrupted. 93
13C-labeled gastric emptying breath tests represent a recognized, non-invasive alternative to scintigraphy for the assessment of GE.90,91 These tests may show greater delays, as highlighted by Knudsen's meta-analysis. 93 However, their interpretation relies on several physiological processes beyond gastric emptying itself, including intestinal absorption and hepatic metabolism, which may be altered in PD. Additionally, small intestinal bacterial overgrowth (SIBO) can further distort test results and lead to an overestimation of GE delay.
Other modalities, such as radiopaque markers, MRI, the Wireless Motility Capsule (WMC), electrogastrography, or gastric biopsies, may provide complementary physiological information but are not validated diagnostic methods and rely on a lower level of evidence (Table 1). MRI studies have reported reduced gastric contraction amplitude without significant impairment of global motility, 94 whereas antral contractility assessed by scintigraphy appears unchanged in mild-to-moderate PD. 32 WMC studies suggest a more generalized slowing of GI transit rather than isolated GE delay. 95
Diagnostic methods for gastroparesis.

Overall, GE assessment in PD remains complex, as it often requires balancing methodological rigor with clinical feasibility in a population characterized by motor fluctuations and limited tolerance to prolonged dopaminergic withdrawal. Although scintigraphy is the gold standard, its reliability depends on strict standardization, which may be difficult to achieve in this specific population. Limitations include patient mobility during prolonged fasting, interference with dopaminergic treatment, and difficulty suspending medications.
In this context, the evaluation of GE in PD often requires a balance between methodological rigor and clinical feasibility. While guideline-recommended protocols remain the benchmark, practical adaptations may be necessary to ensure tolerability and patient safety and tolerability in routine clinical practice. When early resumption of dopaminergic treatment is unavoidable, the use of dispersible or non-oral formulations of levodopa may theoretically limit fluid intake and reduce measurement-related bias; however, this approach has not been formally validated and results should therefore be interpreted with caution.
Bidirectional relationship between gastroparesis and motor fluctuations
Natural history of motor fluctuations
Levodopa remains the standard for motor symptom control in PD, offering strong benefits, especially during the initial “honeymoon” phase.96–101 Over time, however, the effect of each dose diminishes, leading to motor fluctuations (MF). 102
Two mechanisms explain this shift: (i) presynaptic neuron loss reduces dopamine storage, increasing reliance on frequent dosing; and (ii) postsynaptic changes from pulsatile stimulation sensitize motor (nigrostriatal) and non-motor (mesocorticolimbic) pathways, contributing to dyskinesias and impulse control disorders.
These mechanisms underlie the dual nature of the clinical response to levodopa: a short-duration effect persisting in late stages, and a long-duration effect that progressively declines over time.103–106 As PD progresses, the therapeutic window progressively narrows: the interval between the minimum threshold needed to relieve OFF symptoms and the upper threshold that induces dyskinesias becomes increasingly reduced, sometimes to the point of near disappearance, resulting in a continuous alternation between OFF periods and ON states with disabling dyskinesias.107–109
MF can appear within 5–6 months of treatment initiation,110,111 and affect over half of patients within three years, 112 marking disease progression. 113
These fluctuations can manifest in various forms (Figure 1, inspired by Chaudhuri et al.
300
)
114
:
Wearing-off: the medication's effects fade before the next dose. ON-OFF phenomena: alternation between periods of good motor control (ON) and poor control or motor block (OFF). Delayed ON: a delayed clinical drug response to a given dose. No ON or suboptimal ON: reduced or absent response to a given dose.
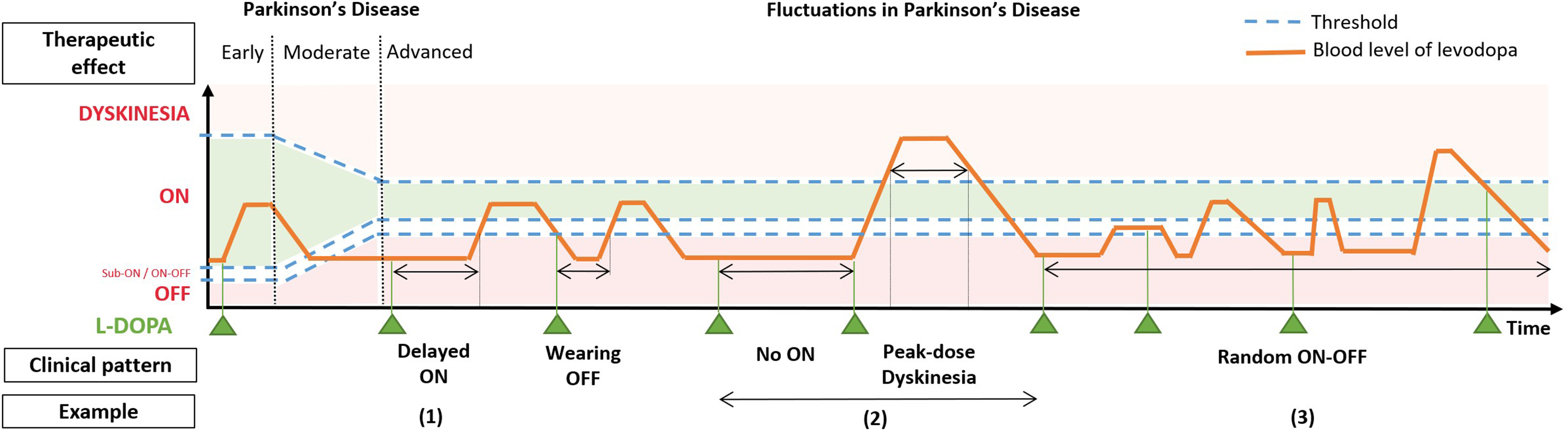
Levodopa-related motor fluctuations in PD. Inspired by Chaudhuri et al.300
OFF periods lengthen and become disabling. 115 Delayed ON episodes may last twice as long as wearing-off episodes and significantly increase total OFF time, 116 worsening quality of life.117,118
Managing MF grows more difficult with disease progression due to the narrowing therapeutic window. Initial approaches include dose fractionation to smooth fluctuations, 119 but advanced stages often require second-line therapies for continuous dopaminergic delivery, including: apomorphine pumps, levodopa-carbidopa intestinal gel pumps, deep brain stimulation (DBS) of the subthalamic nuclei or, more recently, subcutaneous foslevodopa-foscarbidopa pumps.120–122 These treatments, however, may not be suitable for all patients and are contraindicated in some cases.
Gastroparesis and motor fluctuations
Studies have shown that delayed GE in PD correlates with more advanced disease, including higher Hoehn and Yahr stages, greater Unified Parkinson's Disease Rating Scale (UPDRS) scores, and motor complications such as delayed ON, wearing-off, ON-OFF fluctuations, rigidity, and tremor.32–34,39,123–127 These associations support a potential link between GP and both motor symptoms and NMS.
Impact of gastroparesis on levodopa absorption
A study in 31 PD patients showed that delayed GE correlates with altered levodopa pharmacokinetics, suggesting its role in delayed-ON episodes. 128 Prolonged gastric retention impairs small-intestinal absorption and reduces bioavailability.33,40,124,128–135 In the stomach, levodopa may be prematurely converted into dopamine by AADC, which is not absorbed and may further delay GE, creating a vicious cycle. Additionally, gastric food retention, especially proteins, interferes with levodopa transporters, further reducing absorption and increasing the risk of suboptimal or absent ON responses.12,60,72
Impact of levodopa on gastroparesis
In a scintigraphy study of 51 PD patients, 42% of those with motor fluctuations had delayed GE, which was associated with higher doses of AADC inhibitors. 136 Bestetti et al. proposed that levodopa may delay GE by increasing gastric dopamine, which inhibits motility via dopaminergic receptors in the stomach and enteric neurons.136–138 In contrast, dopamine antagonists show prokinetic effects.139–142
Levodopa has been shown to slow GE in both young and elderly healthy subjects after single or repeated doses.37,143–147 This effect also appears in patients with GP, where those on levodopa have slower GE than untreated individuals.32,148,149
In PD, when a dose seems ineffective due to delayed GE, patients may take an extra dose. If both are released suddenly, it may trigger peak-dose dyskinesias. Thus, irregular GE alters levodopa pharmacokinetics and may lead to erratic motor responses, exacerbated by levodopa's own inhibitory effects on GE.50,119,132
Pharmacological treatments for gastroparesis in Parkinson's disease
In PD, treating GP aims to (i) alleviate GI symptoms that affect quality of life, and (ii) enhance the absorption of oral dopaminergic drugs. Enhancing GI transit may increase treatment efficacy, favor more continuous dopaminergic stimulation, and reduce the risk of sensitization-related motor and behavioral complications.
A stepwise strategy is proposed: first, identify and avoid medications that delay GE; second, introduce prokinetics when needed, with attention to safety.
PD patients are often elderly and have multiple comorbidities, leading to frequent use of prescribed and over-the-counter drugs. 150 A meta-analysis by Bhagavathula et al. found that 40% of PD patients are polymedicated (5–9 drugs) and 18% over-polymedicated (≥10 drugs), increasing risks of adverse effects, drug interactions, and non-adherence. Other studies link higher medication counts with more hospitalizations.151–153
Before prescribing prokinetics or modifying antiparkinsonian therapy, deprescribing drugs that impair GE should be considered. 154
Medications contributing to gastroparesis in Parkinson's disease
According to studies, medications are a frequent cause of GP, and were the second-most common reason for GP in 2009, after diabetes. 155 Medications were the third-most common influencing factor for GP in 2022, accounting for 11.8% of cases. 156
Several drug classes are known to delay GE, including anticholinergics, beta-adrenergic agonists, glucagon-like peptide-1 (GLP-1), somatostatin analogs, opioids, antacids, and tricyclic antidepressants.64,157,158
While all potentially impairing medications should be reviewed, this section focuses on four drug classes commonly used in PD care.
Anticholinergic medications
Anticholinergic drugs (e.g., trihexyphenidyl, tropatepine, biperiden) are still widely used in PD, especially for tremor control. In some Asia-Pacific countries, their prescription rates surpass those of dopamine agonists and follow levodopa, with reported usage ranging from 24% to 40% in studies from New Zealand, Japan, and India. 159 These agents restore dopaminergic-cholinergic balance by blocking central muscarinic receptors, particularly in the striatum. 160 However, their benefits are limited by adverse effects, especially in older adults, where discontinuation may improve motor symptoms and reduce fall risk. 161
Beyond PD-specific agents, many commonly used drugs, such as some antidepressants, antihistamines, and urinary antispasmodics, also have anticholinergic properties.162–165
PD patients with psychiatric or neurological comorbidities, or older adults, are more likely to be exposed to anticholinergic medications.163,166 The cumulative effect of these drugs, referred to as the “anticholinergic burden”, can lead to significant adverse effects, particularly in older patients, in whom such drugs are often considered inappropriate.166–169 Peripheral effects include classic atropine-like symptoms: urinary retention, worsening of glaucoma, constipation, dry mouth and skin, thirst, hyperthermia, mydriasis, and tachycardia. Central effects may manifest as confusion, memory impairment, reduced attention, or delirium, particularly in individuals with cognitive vulnerabilities.170,171 To assess and minimize these risks, tools such as the Anticholinergic Cognitive Burden (ACB) scale and the Anticholinergic Risk Scale (ARS) are commonly used in psychiatry, geriatrics, and neurology.163,172–174
From a GI perspective, anticholinergics inhibit acetylcholine at M3 receptors, reducing gastric contractility, particularly in the antrum, and delaying GE.12,63 They may also lower levodopa bioavailability, thereby compromising treatment efficacy, especially in advanced PD. 175
GABA Analogs
Gabapentin and pregabalin, structural analogs of gamma-aminobutyric acid (GABA), are often used in PD to treat neuropathic pain and restless leg syndrome. Although they reduce neuronal excitability centrally, they may also affect gastrointestinal function. By inhibiting P/Q-type calcium channels and decreasing acetylcholine release, they could impair parasympathetic tone and contribute to delayed GE.176,177
Opioids
Opioids such as morphine, oxycodone, hydrocodone, fentanyl, and antidiarrheals like loperamide delay GE by binding to μ-opioid receptors in the ENS. This inhibits acetylcholine release, increases pyloric tone, and slows gastrointestinal transit.178–181
In a 2019 study, 19.3% of 223 patients with delayed GE were on long-term opioids; they showed more severe symptoms and higher hospitalization rates than non-users. 182 Another study in 583 patients with gastroparesis found that 41% used opioids, with worse gastric dysfunction scores, more hospitalizations, and greater use of antiemetics compared to non-users. 183
Constipation, a common opioid adverse effect, was also frequent in both studies and is particularly relevant in PD, where GI motility is already compromised.
Glucagon-like peptide-1 receptor agonists
GLP-1 receptor agonists (e.g. exenatide, liraglutide, semaglutide, lixisenatide) are increasingly prescribed for type 2 diabetes and obesity. These agents are well known to delay GE through central and peripheral mechanisms and may therefore contribute to or exacerbate GP.184,185
Although not used as treatments for PD symptoms, GLP-1 receptor agonists may be prescribed in PD patients with metabolic comorbidities. At the same time, emerging experimental and clinical data suggest potential neuroprotective effects in PD. Notably, the LIXIPARK trial recently reported a slowing of motor disability progression with lixisenatide in early PD. However, further studies are needed to confirm these findings.186–192
In PD patients with suspected or confirmed GP, the potential impact of GLP-1 receptor agonists on gastric motility should therefore be weighed against their possible neurological benefits.
Prokinetic treatments
Currently, no clear guidelines exist for managing GP in PD, and no therapeutic indications are formally validated. Prokinetic agents may help by enhancing and coordinating GI contractions, thereby promoting intraluminal transit. A network meta-analysis by Ingrosso et al., which included 29 randomized controlled trials (RCTs) and 3772 patients, found that only dopaminergic antagonists significantly outperformed the placebo for symptom relief in the general population. 193 While most reviews focus on diabetic GP,194–197 this section specifically addresses therapeutic strategies evaluated in PD.
Dopaminergic antagonists
Dopamine plays a central role in both the central nervous system and ENS, 198 particularly in GI motility. Activation of D2 and D3 receptors in the area postrema and nucleus of the solitary tract contributes to the emetic response.199,200 In the gut, D2 receptor activation inhibits acetylcholine release, lowers sphincter tone, disrupts antral-duodenal coordination, and delays GE. 201 Blocking these receptors restores acetylcholine release and improves antral contractions.
Dopaminergic antagonists such as metoclopramide202,203 and domperidone193,204 block D2 receptors, providing both antiemetic and prokinetic effects. Their efficacy in GP is supported by several randomized trials and cohort studies, including those reviewed by Ingrosso et al.. 193 Despite their Anatomical Therapeutic Chemical (ATC) classification as prokinetic agents, their use in PD is limited due to safety concerns and adverse effects.
Metoclopramide
Metoclopramide, widely used in diabetic GP, crosses the blood-brain barrier and poses a high risk of neurological adverse effects. Its central antidopaminergic action can cause dyskinesia, akathisia, and drug-induced parkinsonism.205,206 In 2009, the FDA issued a black box warning limiting use to 12 weeks. 207 In PD, metoclopramide worsens symptoms 208 and is considered inappropriate according to the Beers criteria. 209 In 2011, the Movement Disorder Society confirmed that it presents an unacceptable risk in PD and recommended domperidone as a safer alternative. 210
Domperidone
Domperidone, unlike metoclopramide, has limited blood-brain barrier penetration and a lower risk of neurological side effects. 211 It is widely used to treat GI symptoms in GP, 212 particularly in PD, where it is often co-prescribed with levodopa, entacapone, or continuous apomorphine infusion to improve tolerance. 213
At doses of 30–80 mg/day over extended periods, several studies have shown it improves GE and relieves symptoms such as nausea, vomiting, and bloating.137,204,214,215 One RCT also demonstrated increased levodopa bioavailability with domperidone. 216
However, its use is controversial due to the cardiac risks associated with it. Case-control studies and meta-analyses have linked domperidone to QTc prolongation, ventricular arrhythmia, and sudden cardiac death, especially in patients over 60 and at doses >30 mg/day.217–219 High-dose studies in PD orthostatic hypotension confirm a dose-dependent cardiac risk.220,221 As of June 2025, data extracted from VigiBase, the WHO pharmacovigilance database, using the Standardized MedDRA Queries (SMQ) narrow term “Cardiac Arrhythmia” identified 1106 cases, including 41 (3.7%) with fatal outcomes. These concerns led to regulatory limits of 30 mg/day in Europe and Canada,222–224 and the FDA has not approved domperidone, except through expanded access programs.137,225
Nevertheless, other studies using higher doses (up to 120 mg/day) reported benefits with low cardiovascular risk under proper monitoring.226,227
Risk increases with co-prescription of QT-prolonging drugs (e.g. ondansetron, quetiapine, escitalopram, commonly used in PD) and in patients with hypokalemia or cardiac comorbidities.212,228–233 Other adverse effects, including hyperprolactinemia, fatigue, weight loss, and restless leg syndrome, must also be considered.
Despite safety concerns, domperidone remains a common choice for PD among neurologists, mainly due to the lack of safer alternatives. It is particularly used to improve the tolerability of antiparkinsonian drugs, often leading to use beyond official guidelines. 234 Careful cardiovascular evaluation, including ECG and clinical risk scores,235–237 may help ensure safer use, 238 though specific validation in PD-related GP is still needed.
Motilin receptor agonists
Motilin receptor agonists, including the macrolides erythromycin and azithromycin, stimulate antral and gastric contractions, improving GE and small bowel motility in GP. However, this effect has not been clearly demonstrated in PD.239–243
However, these agents are not suitable for long-term use due to drug interactions (notably with erythromycin), risk of QT prolongation,244,245 and tachyphylaxis linked to motilin receptor down-regulation. 246 A meta-analysis of randomized trials by Almalki and Guo found no increased risk of cardiovascular events or mortality with azithromycin, but emphasized the limitations of observational studies in establishing causality and the need for further data to assess macrolide cardiotoxicity. 247
In PD, Nakatsuka et al. showed a 1.7-fold increase in the plasma concentration of cabergoline, a dopaminergic agonist, when used in combination with clarithromycin, another macrolide. 248
A 2018 randomized, double-blind Phase II trial evaluated camicinal (GSK962040), a motilin receptor agonist, versus placebo in PD. Over 7–9 days, camicinal accelerated levodopa absorption (shorter Tmax), reduced daily OFF time (−2.31 h/day), increased ON time (+1.88 h/day), and improved total MDS-UPDRS scores with good tolerability, suggesting camicinal may enhance motor response in PD patients with GP. 249
5-HT4 agonists
Early 5-HT4 receptor agonists, such as cisapride 250 and tegaserod, 251 showed prokinetic efficacy but were withdrawn due to serious cardiovascular adverse events related to QT prolongation, hERG channel inhibition and affinity for 5-HT1/5-HT2 receptors.252–254
In contrast, newer-generation 5-HT4 receptor agonists have been developed with greater receptor selectivity and minimal off-target cardiac effects. Agents such as mosapride and prucalopride, primarily prescribed for constipation, have shown benefits in small PD cohorts, including faster GE, longer ON periods, and improved UPDRS II and III scores.255–258
Velusetrag, a highly selective 5-HT4 receptor agonist, 259 has demonstrated efficacy in idiopathic and diabetic GP260,261 and, in a mouse model of PD, improved gastrointestinal motility, reduced gut inflammation, and restored microbial dysbiosis. 262 These preclinical data support further evaluation of velusetrag in PD-related GI dysfunction.
H2 receptor antagonists
Nizatidine (NZT), a selective H2-receptor antagonist initially used for the treatment of peptic ulcer disease, differs from other agents in its class by exhibiting prokinetic properties in both animals and humans.263–265 Beyond inhibiting acid secretion, NZT enhances gastric motility, making it a potential option for treating reflux symptoms associated with GP. 263
This effect is thought to result from increased acetylcholine activity, mediated by non-competitive inhibition of myenteric acetylcholinesterase. 266 Elevated acetylcholine levels stimulate gastric contractions267,268 and promote ghrelin secretion, which may further enhance motility through hypothalamic pathways.269,270
In a three-month open-label study of 20 PD patients, NZT (150 mg twice daily) improved GE and motor symptoms. The treatment was well tolerated, with no reported adverse effects, though clinical details were limited. 271
Motilitone
Motilitone (DA-9701) is a traditional herbal medicine derived from Pharbitidis semen and Corydalis tuber. It has demonstrated clinical efficacy similar to itopride in functional dyspepsia. 272
Motilitone acts via multiple mechanisms, functioning as a 5-HT4, 5-HT1A, and α2-adrenergic receptor agonist, and as a D2 receptor antagonist. Its 5-HT4 agonism and D2 antagonism likely contribute to improved GE. 273
In PD, a double-blind non-inferiority trial by Shin et al. compared motilitone (30 mg) to domperidone (10 mg), both taken three times daily, 30 min before meals, for four weeks in 40 patients. GE assessed by MRI before and after treatment, improved significantly in the motilitone group, although between-group differences at 120 min were not significant. GE changes did not correlate with levodopa dose, disease duration, or UPDRS III or IV. Levodopa plasma levels increased with motilitone, but not significantly. 273
In a phase IV multicenter, double-blind, placebo-controlled trial including 144 PD patients, Choi et al. reported that 30 mg/day of motilitone improved GI symptom-related quality of life (assessed by the Nepean dyspepsia index) after 4 weeks, and reduced overall GI symptom severity after 12 weeks. Importantly, no worsening in motor symptoms was observed, based on UPDRS III, Hoehn and Yahr, and K-PDQ-39 scores. 274
Other therapeutic approaches for gastroparesis in Parkinson's disease
In PD-related GP, oral levodopa in dispersible or liquid forms may slightly reduce Tmax by passing more easily through the pylorus,275–277 whereas extended-release formulations remain more dependent on GE. 278
Non-pharmacological strategies are valuable adjuncts. Dietary modifications, such as small-particle, low-fat, low-fiber meals and physical activity, may alleviate symptoms. However, restrictive diets require caution to avoid malnutrition and constipation.233,279–283
If symptoms persist, non-oral antiparkinsonian therapies may be considered,12,29 such as transdermal dopamine agonists, sublingual or subcutaneous apomorphine,12,284 inhaled levodopa, and newer subcutaneous or intrajejunal levodopa formulations.121,122,285 These strategies bypass the GE but are generally considered second-line due to the complexity of their implementation and the daily management challenges they pose for patients.
Deep brain stimulation may reduce the need for oral medications, though its impact on GI symptoms remains unclear.286,287
Other interventions such as botulinum toxin injection, gastric per-oral endoscopic myotomy, and pyloroplasty are being explored, but evidence in PD remains limited.288–292 Gastric electrical stimulation has demonstrated symptomatic efficacy in refractory GP, particularly in reducing nausea and vomiting, despite inconclusive evidence of a consistent effect on GE293,294; however, it has not been specifically evaluated in patients with PD, and its role in PD-related GP therefore remains uncertain. Vagus nerve stimulation and acupuncture have not shown consistent benefits. 295
Identifying and treating contributing factors such as Helicobacter pylori, small intestinal bacterial overgrowth, or hiatal hernia remains essential for optimal management.127,296
Lastly, proton-pump inhibitors (PPIs) are frequently prescribed in patients with GP, particularly in diabetic GP. However, international consensus statements indicate that PPIs have no demonstrated efficacy on GP itself and should be reserved for the treatment of coexisting gastroesophageal reflux disease rather than gastric motility disorders.297,298 In patients with PD, who are often older and polymedicated, any potential benefit on reflux symptoms should be weighed against known risks of long-term PPI use, including infectious complications, micronutrient deficiencies, gut microbiota alterations, and potential drug–drug interactions. When prescribed, the indication and duration of PPI therapy should therefore be clearly justified and regularly re-evaluated.
Conclusion
In PD, diagnosing and managing GP remains challenging due to the absence of validated diagnostic tools and disease-specific guidelines. The lack of dedicated studies limits our understanding of the complex interactions between PD, its treatments, and GP. Although their co-occurrence is well recognized, longitudinal research is needed to clarify causal relationships. The pathophysiological models of Braak and Per Borghammer suggest early ENS involvement in some PD subtypes, supporting the development of personalized diagnostic and monitoring approaches.
These findings refine the concept of a disrupted gut–brain axis in PD, where bidirectional communication between the GI tract and the central nervous system plays a central role in disease expression and progression. 186 In this context, the gut microbiota may influence both GI motility and the pharmacological response to dopaminergic therapy, 299 offering new therapeutic targets.
A major clinical concern is the impact of delayed GE on levodopa absorption. Delayed GE may cause erratic uptake and contribute to motor complications. Improving GE could stabilize plasma drug levels, reduce fluctuations, and improve quality of life.
At early disease stages, optimizing GE may enhance levodopa response and delay postsynaptic sensitization involved in dyskinesias and impulse control disorders. In advanced PD, GP management could reduce the need for dose escalation and complex regimens, improving adherence and reducing complications.
However, current clinical trials remain limited by small sample sizes, short durations, and inconsistent assessments. Among pharmacological options, domperidone is the most studied prokinetic in PD, but its use requires caution due to dose-dependent cardiac risks, particularly at doses above current recommendations. Nevertheless, these risks must be carefully weighed against the potential benefits of improving gastroparesis and associated gastrointestinal symptoms. However, a prokinetic should only be prescribed after first considering the discontinuation of treatments that may delay GE.
Future GP management in PD should rely on a personalized approach integrating clinical and digestive biomarkers with real-world data. This strategy may refine diagnosis, improve pharmacokinetic predictability, alleviate GI symptoms, and reduce motor complications, reinforcing the need for comprehensive, individualized care (Figure 2).
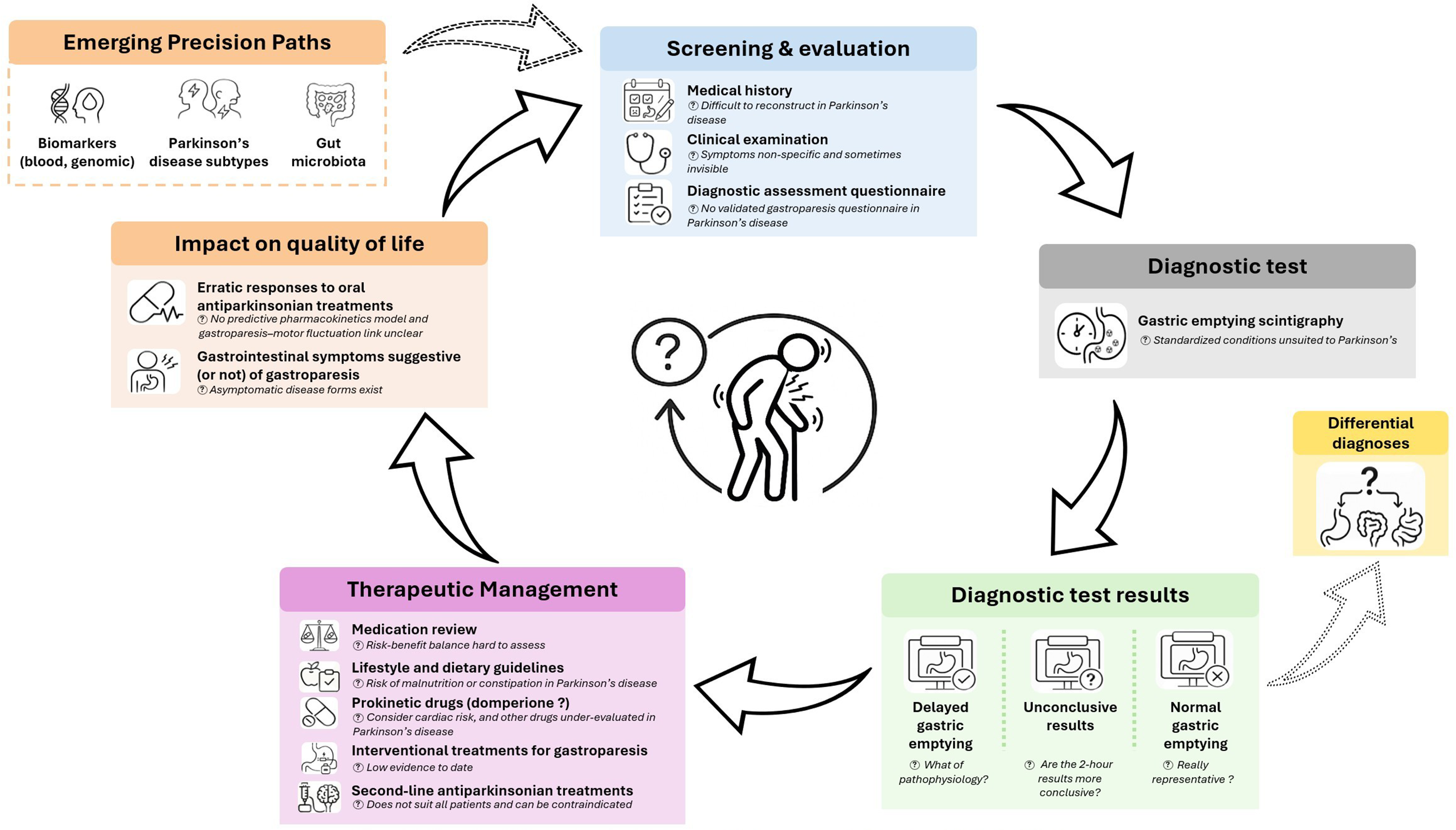
Precision medicine cycle in Parkinson’s gastroparesis: an equation with multiple unknowns.
Footnotes
Acknowledgments
The authors would like to thank all colleagues and collaborators who contributed to the development of this review through their insightful comments and support.
Ethical considerations
Not applicable. This article is a narrative review and does not report original studies involving human participants, human data, or human tissue.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
Q.D. and V.M. drafted the manuscript. Q.D. also designed and produced all figures. M.-B.V.-R. and M.B. contributed to the conceptual framework, critical review, and revision of the manuscript. J.F. and E.T. participated in the review design and provided critical feedback. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Not applicable. No datasets were generated or analyzed during the preparation of this narrative review. Any supporting material can be made available by the corresponding author upon reasonable request.