
Abstract
Huntington's disease (HD) is a progressive, inherited neurodegenerative condition that imposes a profound, multidimensional burden on individuals with HD and their families. This qualitative study explored the physical, emotional, socioeconomic, and intergenerational impact of HD across six European countries, drawing on interviews with individuals diagnosed with HD and family caregivers. Findings reveal that HD disrupts daily functioning, employment, relationships, and long-term planning. Cognitive and psychiatric symptoms were particularly burdensome, driving declines in quality of life (QoL) and emotional well-being. Caregivers reported extensive physical, financial, and psychological strain, with many assuming care responsibilities from a young age or eventually caring for multiple relatives. These burdens frequently spanned generations, with participants describing how HD shaped their upbringing, reproductive choices, and expectations for future caregiving.
Despite some optimism regarding future research, participants expressed concern that therapeutic advances would not arrive in time to benefit them, reinforcing the urgency for non-pharmacological support. There was strong support for more accessible, consistent, and family-centred care models that integrate clinical services with psychosocial and financial supports. Participants emphasized the importance of early diagnosis, proactive care planning, and coordinated support networks to mitigate caregiver burden and improve long-term outcomes.
These findings underscore the need for healthcare systems and policies to move beyond symptom management and address HD as a multigenerational, systemic challenge which needs to be met with a holistic model of care responsive to the evolving needs of both patients and caregivers.
Keywords
Introduction
Huntington's disease (HD) is a progressive, autosomal dominant neurodegenerative disorder characterized by behavioral changes, psychiatric symptoms, cognitive decline and motor dysfunction. 1 It is caused by an expansion of cytosine-adenine-guanine (CAG) repeats in the HTT gene, resulting in a mutant huntingtin protein that impairs neuronal function.2,3 HD has varying prevalence across populations, affecting approximately 5.65 people per 100,000 in Europe and 3.9 per 100,000 globally.3,4 Onset typically occurs between ages 30 and 50, with symptoms worsening over time.1,5 While HD is typically characterized by adult-onset of symptoms, a rare pediatric-onset form can occur before the age of 18 and is often marked by more rapid progression, and intensity of symptoms.1,6 Despite significant advances in understanding HD pathology, effective disease-modifying treatments remain unavailable, and current management focuses primarily on symptom relief. 7
As an autosomal dominant disorder, HD arises when an individual inherits an expanded CAG trinucleotide repeat (≥36 repeats) in the HTT gene from either parent. The mutation is fully penetrant at ≥40 repeats, meaning all individuals with this expansion will eventually develop the disease. 8 Their children have a 50% chance of inheriting the mutation, contributing to a substantial intergenerational burden. Although individuals with 27 to 35 CAG repeats do not develop HD themselves, they may transmit an expanded allele to their children due to repeat instability. 1 Given its hereditary nature, HD often imposes a significant burden across at least two to three generations due to genetic transmission, caregiving responsibilities, and emotional strain. 9 Intergenerational burden of HD is multifaceted, affecting families emotionally, socially, and economically. 10 Research has shown that HD caregivers experience significantly greater stress than caregivers of patients with dementia, averaging 2 points higher on the Zarit Burden Interview scale.11,12 This heightened burden likely reflects the prolonged course of HD and the cognitive disturbances that complicate caregiving, often leading caregivers to neglect their own needs in order to prioritize affected family members, thereby compromising their quality of life (QoL).11–13 Studies have shown that caregiving burden not only increases as HD progresses, but is also associated with elevated psychological burden among family caregivers, including higher self-reported depression and reduced cognitive capacity, challenging earlier assumptions that caregiver burden stabilizes or adapts over time.14,15
The economic burden of HD—including medical costs, reduced productivity, and out-of-pocket expenditures—is considerable. In 2024, annual costs per patient ranged from $40,000–$215,000 (USD) in Europe, $1915–$7132 (USD) in Asia, and $2542–$90,515 (USD) in the Americas. 16 As the disease progresses, families encounter significant financial challenges, such as the need for early retirement, reduced work hours, and the costs associated with hiring professional caregivers.17,18
Recent work has acknowledged geographical and cultural influences on burden, alongside unique challenges created by variations in national healthcare systems.19–21 Cross-national differences in public coverage and familial caregiving expectations shape both the economic and emotional impact of HD, with cultural norms further influencing how this burden is experienced. 22 Yet, these insights often remain fragmented, and the broader intergenerational consequences are frequently overlooked. Research commonly isolates emotional, economic, or social dimensions without examining how these intersect across generations for individuals with HD and their caregivers.23–26 Oliveira et al. (2022) underscore the emergence of illness-related legacies within HD families, calling for family-centered care that accounts for these dynamics. 27 However, this remains underexplored from a holistic, multi-generational, and cross-national perspective.
To address these gaps, this study examined the physical, emotional, intergenerational, socioeconomic, and QoL burden of HD from the perspectives of individuals diagnosed with HD and family members who assume significant caregiving responsibilities for those with HD.
HD shares many of the structural and lived challenges observed across other rare and progressive neurodegenerative diseases, including Alzheimer's disease, Parkinson's, other dementias, and amyotrophic lateral sclerosis. Across these conditions, disease progression is accompanied by substantial emotional strain, long-term caregiving demands, financial hardship, and profound disruptions to family life, often extending beyond the affected individual to caregivers and future generations.28–31 As such, insights derived from the HD experience, such as those found in this study, also offer broader relevance for understanding the holistic burden of rare neurodegenerative diseases more generally.
Methods
This qualitative study examined the burden of HD from the perspectives of individuals with early or moderate manifest HD and family caregivers in six European countries: Denmark (DK), France (FR), Germany (DE), Italy (IT), Spain (SP), and the United Kingdom (UK). Caregiving was defined as the provision of unpaid essential support necessary to maintain the health and well-being of individuals with HD.
Clinical sites were not involved in recruitment, and no interventional procedures were used. This study was reviewed by an independent review board, which assessed the protocol and determined that it met applicable ethical standards. Ethics approval was not sought in each individual country, as all data were collected anonymously, no personal were processed, no interventions were conducted, and analyses were performed exclusively on aggregated, non-identifiable data.
Participants were recruited by local patient organisations (POs) using existing networks, advertisements, and direct outreach. These organisations served as key stakeholders in the conduct of the study, supporting participant recruitment and providing input on the development of interview guides; as such, members of the participating POs were not included as interview participants. Potential participants were screened using standardized eligibility guides and provided with study information and the opportunity to ask questions prior to consent. Eligible participants completed electronic informed consent and sociodemographic and clinical questionnaires before interviews were scheduled, with confidentiality supported through participant-selected names and preferred interview modality. Further detail regarding the recruitment process can be found in the Supplemental Materials. Eligible individuals with HD were 18 years of age or older with a confirmed diagnosis by an HD specialist. Eligible caregivers were 18 years of age or older, provided at least ten hours per week of unpaid care to someone with manifest HD, and did not have a diagnosis of manifest HD themselves. While all individuals in this group were caregivers to a family member with HD, they are not necessarily related to the individuals in the HD group interviewed in this study. The two groups were recruited independently.
Recruitment aimed to acquire geographic diversity and balance across the two participant groups. Participants were compensated according to fair market value in the respective countries where the study was conducted. Interviews were conducted between December 2022 and August 2023.
Study materials included screening forms, electronic informed consent, sociodemographic and clinical questionnaires, and semi-structured interview guides. The guides were informed by existing literature, reviewed by a patient advocate, and refined through pilot testing. The study was approved by an ethical institutional review board, in accordance with local law. Interviews were conducted in participants’ local languages by trained interviewers via videoconference or telephone. Each interview lasted approximately sixty minutes and followed a semi-structured format.
Transcripts were translated into English, de-identified, and analyzed by adopting a thematic content analysis approach in ATLAS.ti (v22), using a pre-specified qualitative analysis plan which included thematic and conceptual coding of content for initial coding dictionary development. A coding framework was developed and refined iteratively using a constant-comparative method. Themes were identified through both deductive and inductive approaches. Descriptive statistics were calculated using SAS to summarize participant characteristics. Additional methodological details are provided in the Supplementary Materials.
Results
Individuals with HD
A total of 19 individuals with early or moderate manifest HD participated in the study. Insights were drawn from survey data on symptoms and clinical features, and semi-structured interviews. Detailed participant characteristics for the individuals with HD are presented in Table 1 and representative quotes are provided in Table 2.
Characteristic and demographic data of study participants with manifest HD.
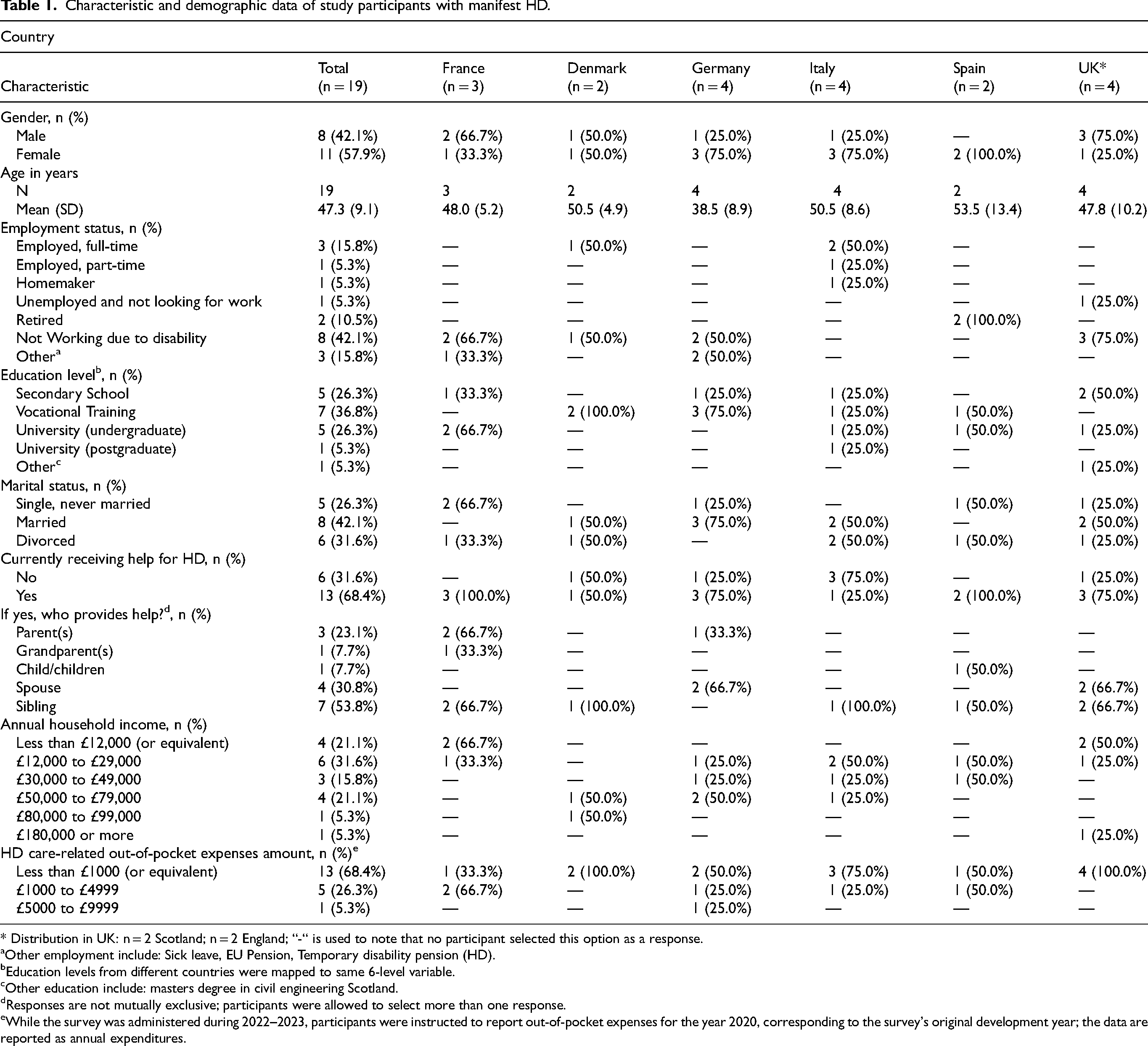
* Distribution in UK: n = 2 Scotland; n = 2 England; “-“ is used to note that no participant selected this option as a response.
Other employment include: Sick leave, EU Pension, Temporary disability pension (HD).
Education levels from different countries were mapped to same 6-level variable.
Other education include: masters degree in civil engineering Scotland.
Responses are not mutually exclusive; participants were allowed to select more than one response.
While the survey was administered during 2022–2023, participants were instructed to report out-of-pocket expenses for the year 2020, corresponding to the survey's original development year; the data are reported as annual expenditures.
Key findings and themes expressed by individuals with HD.
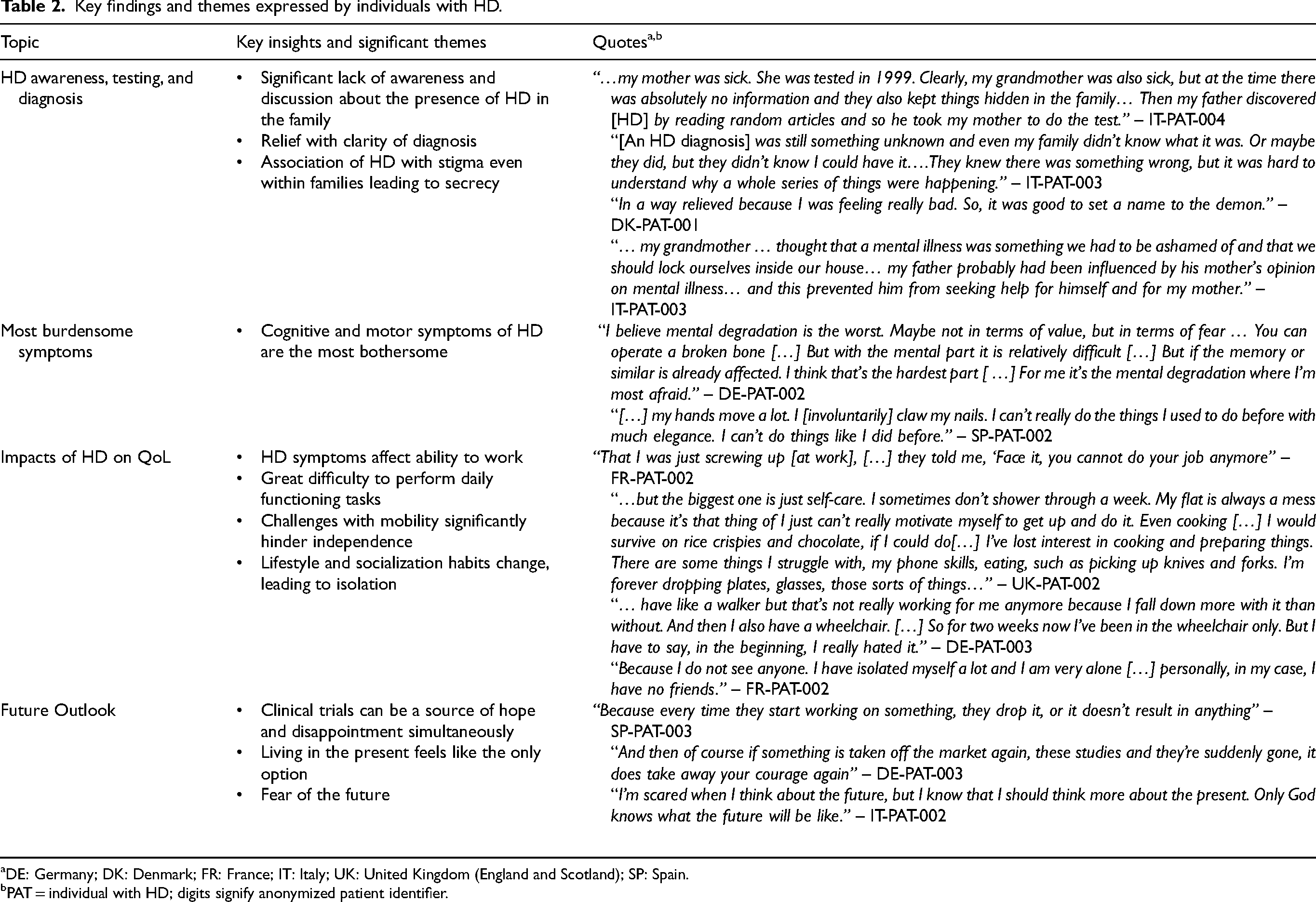
DE: Germany; DK: Denmark; FR: France; IT: Italy; UK: United Kingdom (England and Scotland); SP: Spain.
PAT = individual with HD; digits signify anonymized patient identifier.
Family member diagnosis serves as a turning point in HD awareness
Most individuals with HD first became aware of the disease following the diagnosis of a family member (n = 17/19, 89%). Several individuals described a broad sense of confusion within their families caused by the disease, particularly because of a lack of understanding about HD, its implications and the behaviours of affected relatives. This uncertainty often made their early experiences more difficult. For some, an HD diagnosis, even incidental, brought clarity to past family dynamics.
Some participants also described a general lack of accessible information about HD and genetic testing at the time they first encountered the symptoms (n = 4/19, 21%). Over a third of participants reported pursuing genetic testing following another family member's diagnosis, while a similar proportion sought testing after noticing symptoms themselves. Upon receiving their diagnosis, several participants recalled feelings of shock, sadness, or depression, and some required psychological support or medication. Other individuals described experiencing acceptance, or even relief, upon receiving clarity about their condition.
Amidst diverse symptoms associated with HD, cognitive impairment emerges as a common driver in decline of QoL
Cognitive challenges emerged as the most frequently cited and burdensome symptoms, with difficulty concentrating (n = 13/19, 68%) and memory lapses (n = 8/19, 42%) highlighted early in the disease journey. Organizational difficulties and trouble following instructions were also commonly reported. These impairments significantly affected daily functioning, from completing household tasks to maintaining employment.
Physical and motor symptoms were also prevalent (n = 16/19, 84%), including fatigue, balance and coordination problems, speech delays, and sleep disturbances. These issues impaired mobility, increased dependence on others for self-care, and interfered with leisure participation. Many individuals used physiotherapy, speech therapy, or sleep medications in response. During interviews, the interviewer and accompanying family members of participants with HD observed motor and speech-related symptoms, including delayed speech and involuntary jaw movements, that were not consistently self-reported in pre-interview clinical forms, indicating the presence of non-awareness. Psychological health was also adversely affected in most participants (n = 16/19, 84%), with frequent reports of anxiety, depression, and stress. Participants linked these symptoms to strained social interactions and noted frequent embarrassment or withdrawal from public settings due to fears of stigma or misunderstanding. Over one-third required psychotherapy or psychotropic medication to manage these symptoms.
Cumulatively, these symptoms had a profound impact on QoL. Over three-quarters of participants (n = 15/19, 79%) described reduced ability to manage daily tasks such as cooking, shopping, and personal hygiene. Nearly all participants (n = 18/19, 95%) reported HD-related disruptions to their occupational or educational activities. Several were forced to leave employment due to symptom progression, while others experienced reduced productivity and prolonged task completion. In some cases, participants reported increased financial strain resulting from reduced household income.
Individuals with HD report a mix of optimism and doubt towards the future
Over half of participants (n = 13/19, 68%) expressed optimism about the future of HD research, despite recognizing that advancements may not benefit them personally within their lifetime. In contrast, some voiced skepticism, citing failed clinical trials and limited therapeutic progress. While uncertainty and fear about their own future were common, most participants conveyed hope that future generations would benefit from meaningful advances in HD treatment
Caregivers of individuals with HD
23 family caregivers of individuals with HD participated in this study. Detailed participant characteristics and representative quotes acquired during the interview process can be found in Tables 3 and 4, respectively.
Characteristic and demographic data of study participants that are familial caregivers of individuals diagnosed with manifest HD.
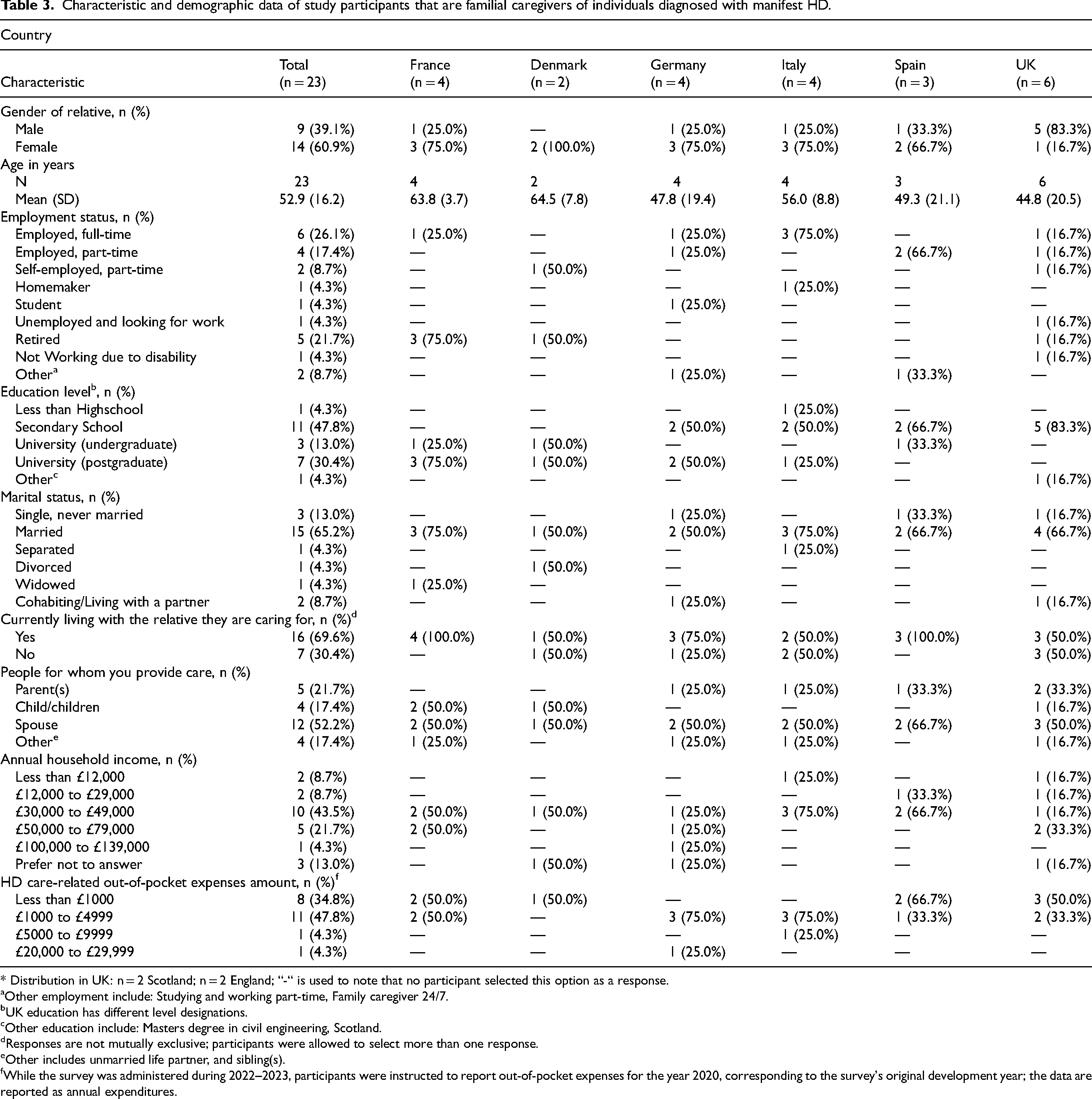
* Distribution in UK: n = 2 Scotland; n = 2 England; “-“ is used to note that no participant selected this option as a response.
Other employment include: Studying and working part-time, Family caregiver 24/7.
UK education has different level designations.
Other education include: Masters degree in civil engineering, Scotland.
Responses are not mutually exclusive; participants were allowed to select more than one response.
Other includes unmarried life partner, and sibling(s).
While the survey was administered during 2022–2023, participants were instructed to report out-of-pocket expenses for the year 2020, corresponding to the survey's original development year; the data are reported as annual expenditures.
Key findings and themes expressed by caregivers of individuals with HD.
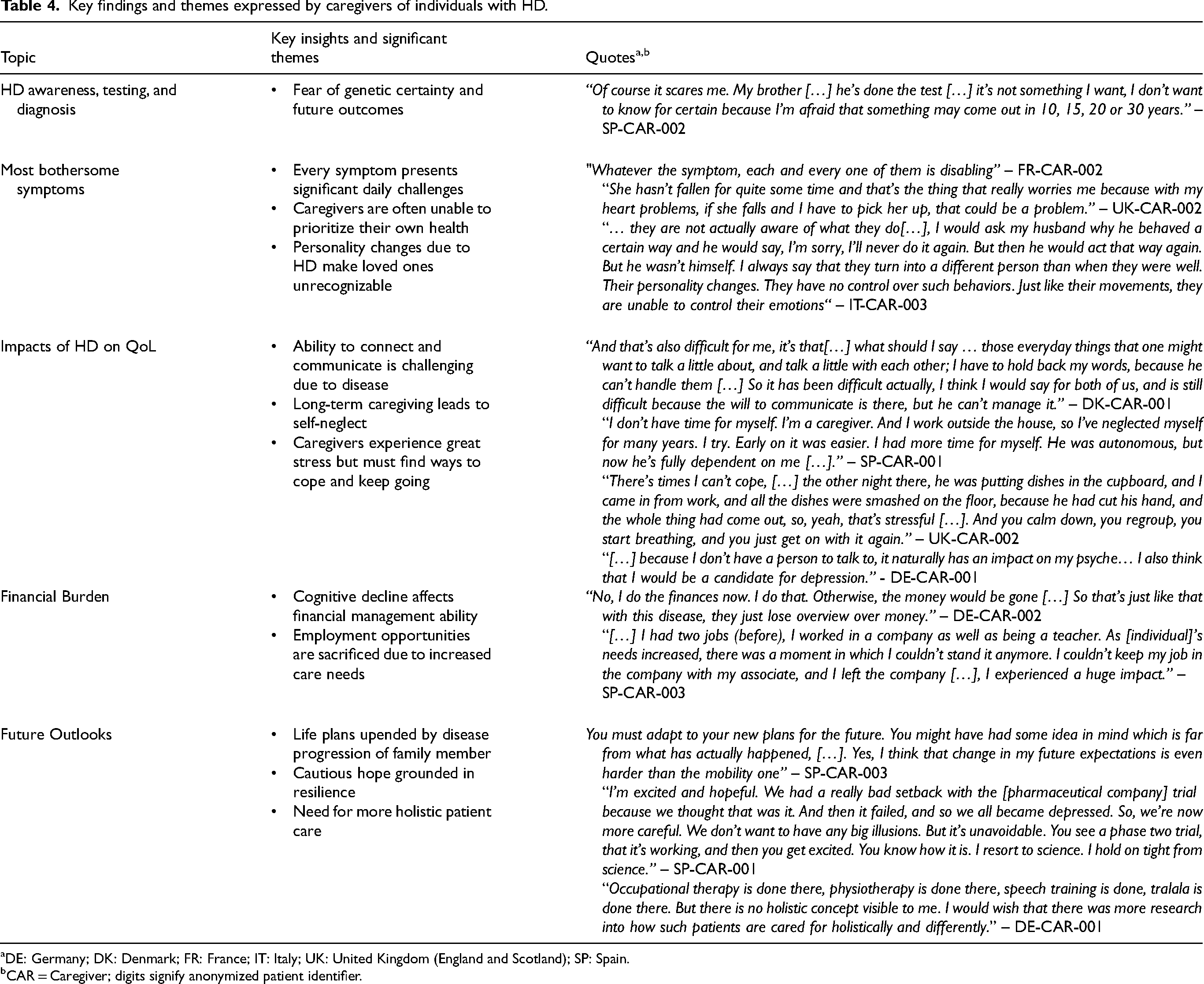
DE: Germany; DK: Denmark; FR: France; IT: Italy; UK: United Kingdom (England and Scotland); SP: Spain.
CAR = Caregiver; digits signify anonymized patient identifier.
Caregiving for individuals with HD is a multi-generational, time-intensive, and often uncompensated burden
Most caregivers provided support to a spouse (n = 12), parent (n = 5), child (n = 4), or sibling (n = 4). The time dedicated to caregiving ranged from 10 to over 40 h per week. Caregivers reported providing varying amounts of care per week, with 11 providing 10–19 h, 3 providing 30–39 h, and 9 providing more than 40 h on average. All caregiving was reported to be unpaid.
Testing for HD among biologically related caregivers of individuals with HD is accompanied by anxiety
All biologically related caregivers in this study (n = 11/11, 100%) first learned about HD when their family member was diagnosed or disclosed the diagnosis. Among the caregivers, 6/23 underwent predictive genetic testing for HD, with most expressing anxiety related to a potential positive result. Two participants confirmed they were gene carriers, while the other four were not. A biological family member who opted against testing cited fear of receiving a positive result and anxiety about future symptom onset. Most caregivers (n = 16/23, 70%) did not pursue HD testing due to a perceived lack of personal risk, a view that was consistent with the fact that many caregivers were not biologically related to the individual with HD (n = 12/23, 52%).
Caregivers identified cognitive, psychological, and movement-related symptoms as the most disruptive and burdensome aspects of HD
Many caregivers described cognitive changes—such as difficulty with concentration (n = 20/23, 87%), task planning, and following instructions (both n = 19/23, 83%)—as particularly noticeable and disruptive in the individuals they cared for. Psychological symptoms, including irritability, depression, anger, and impulsivity, were also frequently cited as highly impactful. Movement and speech difficulties were widely reported, often significantly impairing daily functioning. Caregivers reported that individuals with HD were often unaware of their behavioral, emotional, and motor symptoms, frequently failing to recognize or recall their actions and experiencing marked personality changes and loss of behavioral control, which caregivers described as particularly challenging to manage. Safety concerns were commonly raised, particularly around falls related to chorea and balance issues.
When asked which symptoms were most burdensome for them as caregivers, responses varied, but cognitive and movement-related challenges were consistently emphasized. Collectively, participants highlighted the inherent complexity of caregiving in HD, noting that the diverse and disabling symptom burden posed substantial emotional and practical challenges.
Caregiving takes an emotional toll that can substantially diminish QoL
Caregivers of individuals with HD reported wide-ranging impacts on their QoL, with particular emphasis on psychological well-being (n = 20/23, 87%). Many described feeling chronically stressed, anxious, discouraged, or emotionally depleted. Participants used phrasing such as “psychologically drained,” “sad or depressed,” and “frustrated” to characterize the emotional toll of caregiving. Several participants described bearing the full weight of caregiving without emotional support or someone to confide in, leading some to seek help through antidepressants, therapy, or other mental health services.
A recurring theme was the impact of caregiving on daily life functioning (n = 19/23, 83%), with many describing routines organized almost entirely around caregiving responsibilities. The burden of managing household tasks alongside care duties was frequently noted. Neglect of self-care was common, with participants reporting fatigue and diminished sleep quality as caregiving demands intensified.
Several caregivers described how their lives had been substantially altered – one stopped fostering children, while others assumed full responsibility for the HD individual's personal and social life. Some remained near their parents’ homes to provide continuous support, and a few relied on friends or extended family to manage day-to-day tasks. Participants noted that social constraints—such as the need to plan outings in advance, avoid spontaneity, or avoid alcohol consumption in case of emergencies—were common, but generally not seen as the primary source of caregiver burden.
Caregivers often make professional sacrifices that affect their financial standing
More than half of caregivers (n = 13/23, 57%) identified spending more than £1000 (or equivalent) per year for out-of-pocket expenses attributed to their care for family members with HD, with two reporting more than £5000 (or equivalent) annually. Transportation to medical appointments, medication, and formal care for the individuals with HD were the most frequently cited expenses. Due to the provision of care for individuals with HD, several caregivers had to leave their jobs, reduce their working hours, or take on fewer professional responsibilities.
The outlook for caregivers is marked by uncertainty but hope for the future
Many caregivers described the emotional toll of adjusting life expectations and aspirations in response to caregiving demands (n = 18/23, 78%). Uncertainty around disease progression led some to delay or forgo personal goals, such as international travel or relocation, with several highlighting the difficulty of future planning due to the unpredictable needs of the individual with HD.
When reflecting on HD research, most caregivers expressed cautious optimism (n = 17/23, 74%). While hopeful for therapeutic advances, many acknowledged that such progress may not alter the disease course for their loved ones. One caregiver emphasized the need for greater access to non-pharmacological interventions and called for more holistic, person-centered care. Others reported finding emotional support through shared experiences with fellow caregivers, which helped reduce feelings of isolation and strengthened their sense of community.
Generational and familial burden
Familial burden of HD is significant
Nearly all individuals with HD (n = 18/19, 95%) and most caregivers (n = 16/23, 70%) reported strained personal relationships, including conflict with siblings and emotional volatility with partners. Some individuals with HD attributed their divorce to the challenges of HD (n = 2/19, 11%). Some individuals described the emotional toll on children who regularly witnessed arguments or tension at home, often stemming from HD-related behavioral changes in a parent. Discussions about future care planning were often sensitive. While some participants had begun considering long-term arrangements, others felt it was premature or avoided the topic due to discomfort or fear of burdening family members. Representative quotes illustrating family dynamics and the intergenerational impact of HD are provided in Table 5.
Key findings and themes expressed by caregivers and individuals with HD addressing generational burden.
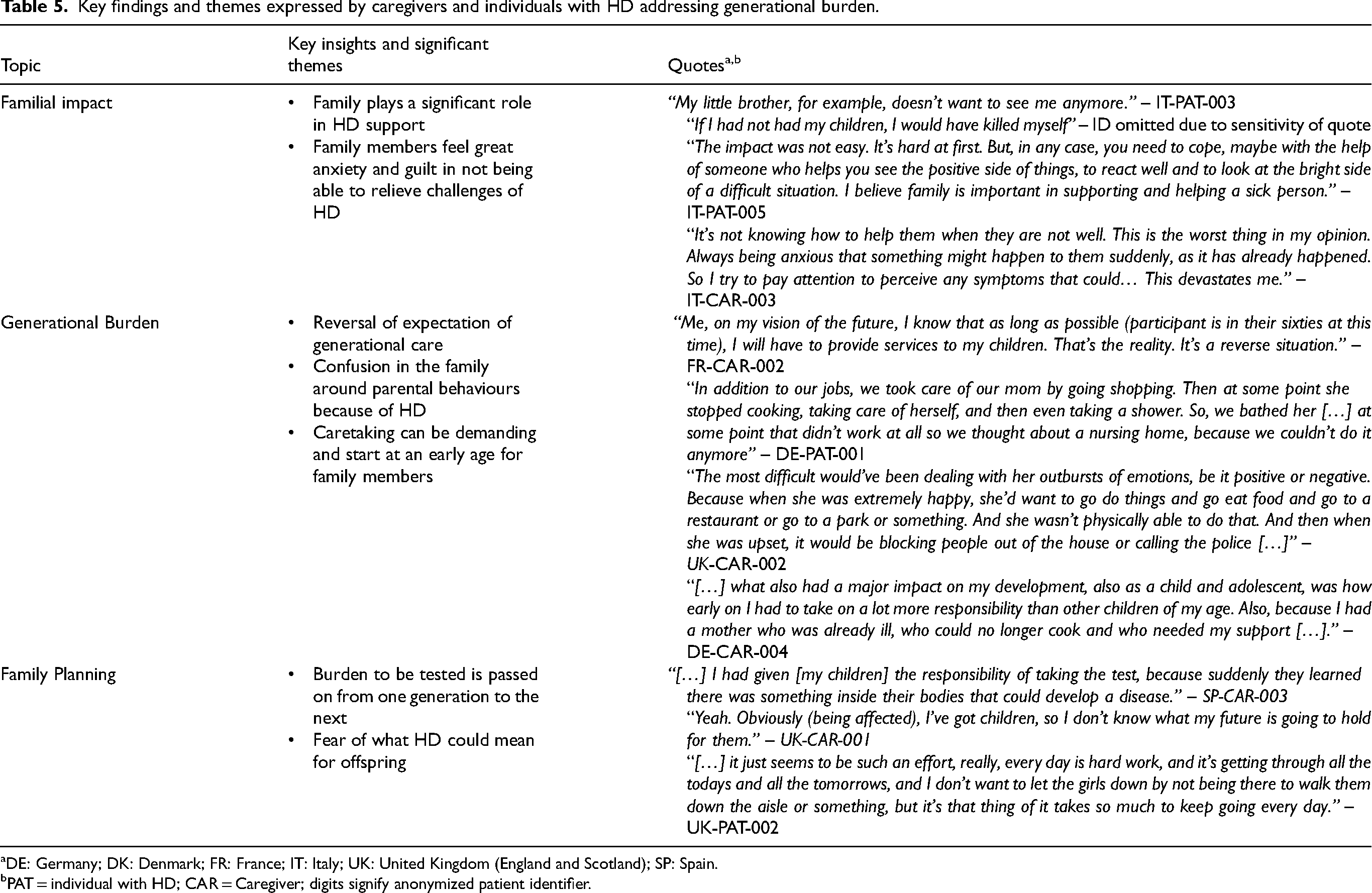
DE: Germany; DK: Denmark; FR: France; IT: Italy; UK: United Kingdom (England and Scotland); SP: Spain.
PAT = individual with HD; CAR = Caregiver; digits signify anonymized patient identifier.
Intergenerational exposure to HD
The intergenerational burden of HD was evident across both individuals with HD and caregivers. On average, individuals with HD reported having 2.6 family members exhibiting symptoms and 1.4 with a confirmed genetic diagnosis. Most (n = 17/19, 89%) reflected on growing up with affected relatives, often assuming caregiving responsibilities during childhood. The intensity of care ranged from occasional assistance to over 40 h per week. Participants described emotionally difficult upbringings shaped by secrecy, early role reversals, social isolation, and limited emotional support. In several cases, silence about the disease, sometimes passed down from grandparents, deepened feelings of confusion and fear. Many reported struggling to balance their own developmental needs with caregiving responsibilities, particularly as symptoms progressed and institutional care became necessary. This transition was often accompanied by guilt and emotional strain.
Caregivers similarly reported extensive family histories of HD, with an average of 2.3 relatives diagnosed by genetic testing and 1.8 exhibiting symptoms. Nearly half (n = 11/23, 48%) had additional family members with HD beyond those they directly supported. For those raised by symptomatic parents or grandparents, early caregiving was described as distressing due to mood instability, communication challenges, and lack of support. In contrast, caregivers exposed to HD later in life often recognized early symptoms only in hindsight and described their experiences more neutrally.
Preparing the next generation for HD care
Participants across both groups expressed concern about future caregiving, particularly about who would assume responsibilities once they were no longer able. There was a common but often implied expectation that younger generations, typically adult children or grandchildren, would take on this role, underscoring the long-term emotional and logistical demands HD places on families across generations.
Many caregivers and individuals with HD described efforts to discuss HD with their children, typically initiated when children reached a certain age, began asking questions, or encountered the topic independently. While some noted potential benefits, including increased awareness, informed reproductive choices, and stronger family bonds, others described reactions of fear, avoidance, or denial. Despite these challenges, a few participants recalled positive intergenerational experiences, such as observing a healthy parent serve as a dedicated caregiver, offering a model of resilience, compassion, and hope.
Hereditary nature of HD is an important consideration in family planning
Among participants with HD, most were parents (n = 12/19, 63%), nearly all of whom conceived naturally. One reported using in vitro fertilization (IVF), and none had adopted children. When asked about genetic testing, most indicated that their children had not been tested. Several participants reflected on how HD influenced their family planning—some delayed or reconsidered having children due to the diagnosis, while others chose to proceed despite initial hesitation. A number of individuals had children before knowing their HD status and believed that earlier awareness might have changed their decisions.
Experiences of growing up with HD in the family also shaped participants’ perspectives on parenthood. Some described emotional hardship during childhood that led them to question whether they wanted to bring children into a similar situation. Others expressed uncertainty but acknowledged that these experiences would likely influence future reproductive decisions.
Family caregivers expressed similar reflections. Most were parents (n = 18/23, 78%), with one reporting adopting. Although caregivers in this study were not diagnosed with HD, 61% stated their children had undergone genetic testing. Most caregivers (52%) were spouses of individuals with HD, which may explain the high testing rates among their offspring. A few caregivers encouraged their children to explore alternatives to biological reproduction in the absence of genetic testing. One noted her children had chosen to delay testing until adulthood, citing the lack of available treatments. Another expressed concern about her daughter's decision to become pregnant without first confirming her genetic status.
Discussion
This study is among the first to examine the multidimensional burden of HD across multiple European countries, incorporating the lived experiences of individuals with HD and family caregivers. The findings reveal a complex interplay between symptomatic, emotional, and socioeconomic stressors that collectively diminish QoL and impact familial relationships. Critically, the results highlight the intergenerational nature of HD burden, across and within generations, capturing the evolving challenges faced by individuals who grow up in HD-affected families, assume caregiving responsibilities, and may later develop the disease themselves. These insights underscore the need for care models and health policies that address the long-term, cross-generational impact of HD on families.
HD's multifaceted burden affects the entire family
HD progression imposes a substantial and evolving burden on individuals with a diagnosis, those at risk, and caregivers, extending well beyond the affected individual. As the disease advances, caregivers experience increasing emotional, psychological, and practical strain driven by progressive motor, cognitive, and behavioral symptoms. 15 This burden is evident even in pre-manifest HD and is further compounded by economic impacts, including reduced employment, productivity loss, and out-of-pocket costs.14,18 Prior studies contextualize the individual experiences described here within a broader pattern of psychiatric and functional burden across the HD disease spectrum. Longitudinal data from prodromal HD populations demonstrate that psychiatric symptoms, including depression, anxiety, irritability, and apathy, often emerge years before motor onset and persist or worsen over time, contributing to early functional impairment and reduced QoL. 32 Consistent with previous research, our findings confirm that HD manifests through a wide array of symptoms, eliciting both physical and emotional distress.18,25,33,34 Although cognitive impairment emerged as the most cited symptomatic burden among individuals with HD and caregivers, there was notable variation in symptom impact across participants. These differences align with recent work demonstrating the heterogeneous phenotypic expression of HD and support the notion that individuals with HD may benefit from personalised care plans to accommodate their specific needs. 35 The cumulative impact of HD symptoms undermines autonomy, mental health, and future planning. While both groups acknowledge the presence and burden of symptoms, caregivers were more likely to notice symptoms that individuals with HD did not recognize, highlighting issues of non-awareness. The lack of awareness of these symptoms elevate caregiver burden through increased physical demand, elevated social isolation, dependence, and tension related to patient care.36,37 It also sheds light on discrepancies sometimes observed between severity of symptoms experienced by individuals with HD compared to family caregivers who observe these symptoms.
Individuals with HD commonly reported difficulty with daily tasks, disrupted careers, financial strain, and strained family dynamics. While most households reported relatively modest out-of-pocket costs (<£1000 [or equivalent] per year), a subset experienced higher expenses that represented a considerable share of household income, particularly among lower-income groups. Given that caregiving responsibilities are typically assumed by family members, caregiver participants consistently experienced similar challenges across the same domains, underscoring the holistic burden of the disease. 34
Caregiving imposes significant financial strain, with consequences extending beyond the household to broader societal productivity. Nearly half of respondents (47.8%) reported spending £1000–£4999 (or equivalent) annually on HD care, which represents ∼3–17% of income for the most common household bracket (£30,000–£49,000 [or equivalent], 43.5% of respondents), but may account for up to 42% of income among those earning less than £29,000 (or equivalent) annually. Caregiving responsibilities often compel individuals to reduce working hours, forgo career advancement, or exit the workforce entirely. In a study by Lai et al. (2012), over one-third of caregivers reported depleting savings, giving up necessities, or being unable to afford basic extras due to caregiving expenses. 9 These adjustments lead to substantial opportunity costs and in turn, diminished economic contributions. These findings underscore the critical need for policies that mitigate the economic toll of informal caregiving. Overall, individuals with HD and caregivers reported highly overlapping symptom experiences, particularly with respect to social withdrawal and disrupted relationships, substantial psychological and emotional distress, and marked impairments in daily functioning, including self-care, mobility, and routine household activities.
However, caregivers consistently described a profound and ongoing sense of loss as they witnessed the gradual cognitive and psychological decline of their loved ones. Indeed, the emotional weight of caregiving is often compounded by anticipatory grief and the strain of shifting family roles, such as a spouse becoming a fulltime caregiver, or a child stepping into an adult role prematurely.9,16,38 Many family caregivers are not formally trained to manage the emotional or functional demands of caregiving, including complex tasks such as administering feeding tubes or urinary catheters, supporting mobility, or responding to emotional outbursts. 39 Existing research underscores the importance of integrating family caregivers as active partners in care teams. Facilitating mutual knowledge exchange and establishing clearly defined roles tailored to individual capacity may improve both care coordination and overall quality of care. 40 As many caregivers are compelled to prioritise the needs of individuals with HD over their own well-being, they may themselves suffer from the broader medical burden should their health begin to deteriorate. Comprehensive support systems that address emotional, psychological, and physical challenges faced by caregivers are essential to safeguarding their health and ensuring that their lives are not relegated to a secondary status in the context of caregiving.
Participants also described HD as a multigenerational experience, often initiated by the diagnosis of a parent, grandparent, or other family member. This reflects findings that HD frequently shapes family dynamics well before the emergence of clinical symptoms in younger generations.27,41 In this study, several participants retrospectively identified long-term behavioural changes in family members that were only understood in the context of a subsequent HD diagnosis. Recognizing HD related symptoms at an earlier stage may help mitigate misunderstandings and interpersonal strain within families, underscoring how diagnostic delays can affect not only clinical outcomes but also family relationships. 42 Early diagnosis may also influence family planning decisions, as both individuals with HD and their caregivers expressed concerns about the implications for their children. Some participants reflected that receiving an earlier diagnosis might have influenced their reproductive or life decisions. The generational impact of HD extends beyond the inheritance of caregiving responsibilities; it also encompasses the emotional and psychological weight of genetic testing, and, for some, the difficult decision to forgo having biological children altogether.
Thus, the burden associated with HD is multifaceted, spanning multiple domains of everyday life, and holistic, as it extends beyond the diagnosed individual to impact their familial caregiving network, often in similarly disruptive and deeply challenging ways.
While the individual living with HD, represented at the centre, is directly affected across multiple areas of life, their caregivers, including parents, spouses, siblings, and future generations, experience similar burdens. This parallel impact across emotional, social, financial, and physical health domains highlights HD as both a multifaceted and holistic burden.
A comprehensive approach to HD care must consider caregivers needs
The findings from this study reinforce the need for a holistic, family-centred model of care that acknowledges HD's profound impact on both individuals and their families. HD is a systemic and generational disruptor that affects emotional well-being, socioeconomic resilience, and family functioning.19,34,43 Beyond personal consequences, HD imposes broader societal costs, including lost productivity, disrupted education, and increased reliance on informal and formal care systems.16,44
Caregivers frequently reported neglecting their own health, often experiencing physical and psychological deterioration that, in some cases, left them in need of care themselves. This aligns with existing literature describing a feedback loop in which chronic stress and prolonged deferral of self-care contribute to significant health complications for caregivers.12,39
Although disease-modifying therapies for HD remain unavailable, international treatment guidelines outline standardized, symptom-targeted approaches that may meaningfully reduce patient and caregiver burden.21,45 These include pharmacologic management of chorea using VMAT2 inhibitors such as tetrabenazine or deutetrabenazine, treatment of psychiatric symptoms with antidepressants (eg. SSRIs), mood stabilizers, or atypical antipsychotics, and structured access to physiotherapy, occupational therapy, and speech and language therapy to support mobility, daily functioning, and communication.21,45,46 While some participants accessed therapy, antidepressants, or mental health services, such efforts were typically reactive, underscoring a lack of proactive, accessible psychological support.
The caregiving experience is further complicated by the progressive shrinking of social networks. Both groups described withdrawing from friendships, intimate relationships, community life, and even support groups due to the stigma surrounding HD and the unpredictability of disease-related behaviours. These patterns reflect a broader emotional burden that extends beyond practical care and requires ongoing psychological support, anticipatory education, and access to coordinated care pathways.
Current healthcare systems, often structured around acute episodic care, are poorly equipped to address the evolving, long-term needs of families affected by HD. A proactive, multidisciplinary model could help mitigate these challenges by enabling earlier intervention, strengthening caregiver resilience, and maintaining patient function. Such a model requires an interdisciplinary team—tailored to context and patient needs—which may include, but is not limited to, neurologists, psychologists, psychiatrists, genetic counsellors, palliative care specialists, care coordinators, and rehabilitation professionals. Crucially, it must also integrate family-centred supports such as respite services and caregiver training.
Centralized ‘one-stop-shop’ models, adapted from frameworks used in memory clinics, intracranial hypertension programs, and oncology, offer a promising foundation for delivering such integrated care.47–49 Crucially, these models must recognize the dynamic, intergenerational nature of HD caregiving. In many cases, care initially provided by a spouse is later assumed by adult children, who often care for both the affected parent and the aging caregiver while simultaneously managing their own risk of developing the disease or living with the knowledge that they carry the mutation and will eventually become ill. 39
Ultimately, the burden of HD is multidimensional, evolving over time and affecting entire familial networks in similarly disruptive ways. A care model that anticipates and addresses these intertwined challenges is essential to delivering compassionate, coordinated, and sustainable care. 48
Early detection and intervention can empower families to make informed decisions
Evidence from pediatric HD demonstrates that early-onset disease is often marked by severe neuropsychiatric, cognitive, and behavioral disturbances that impose substantial emotional and caregiving demands with additional burden attributed to early affected parents. 50 Although not the focus of the present study, findings in adolescents and young adults suggest that psychiatric burden may emerge prior to clinical diagnosis in individuals carrying the HTT expansion, with potential implications for intergenerational burden when emerging symptoms coincide with caregiving responsibilities for affected parents. 51 Early diagnosis provides a critical window for timely support for individuals with HD and their caregivers. It enables informed decisions about genetic testing and family planning. It also facilitates early access to counselling, reproductive services, caregiver training, and community-based supports; measures which have shown to improve outcomes and reduce caregiver burden. 52 These findings highlight the importance of timely recognition and structured diagnosis, not only for individuals but for the entire family unit. Beyond symptom management, early diagnosis supports future planning, emotional preparedness, and continuity of care.
Cautious optimism of the future underscored by need for better support
The results of this study align with a growing consensus that HD care must extend beyond symptom management. Although several promising candidates are in clinical trials, no therapies that affect the underlying cause of disease have been approved to date, underscoring the need to improve care coordination, caregiver support, and long-term planning. Integrated multidisciplinary models—comprising neurologists, psychiatrists, social workers, physiotherapists, and genetic counsellors—have shown benefits in other neurodegenerative conditions, such as Alzheimer's disease, Parkinson's disease, and multiple sclerosis, and are increasingly recommended for HD.29,48,53 Participants strongly supported more accessible, consistent, and holistic care pathways. These models should be culturally sensitive and publicly funded to reduce disparities in care delivery.25,54
Participants in both groups were in agreement, and felt that ongoing research is unlikely to advance quickly enough to benefit them within their lifetime, reflecting the challenges of HD drug development. 55 This shared sentiment underscores the need for continued innovation recognizing the emotional toll on those awaiting advances. Despite this, participants expressed optimism about emerging tools that could improve quality of life. Digital health solutions such as telemedicine, online support groups, and symptom tracking apps have shown promise, particularly in underserved geographies. 56 However, addressing HD disease management and burden requires more than clinical breakthroughs; it calls for a reimagining of how healthcare systems respond to chronic, inherited, and stigmatised conditions, and a commitment to compassionate, equitable care.
Strengths and limitations of this study
This study employed purposive, qualitative thematic content analysis to develop a conceptual understanding of the holistic burden of HD. A key strength was the inclusion of participants from six culturally diverse European countries, enriching the dataset with varied perspectives. Collaboration with patient organisations further enhanced the study by fostering engagement with individuals directly affected by HD. Patient organisations also contributed to the development of the study and interview materials, helping ensure that the research approach and discussion topics reflected priorities relevant to the HD community.
However, certain limitations should be considered. Participants were likely more informed or engaged, often recruited through advocacy groups, which may introduce selection bias and limit generalizability. Additionally, individuals with severe psychiatric manifestations of HD or those unable to meaningfully participate in an interview were not included in the study. As a result, experiences associated with more advanced disease stages or severe neuropsychiatric symptoms may be underrepresented. This may also limit insight into the experiences of caregivers supporting individuals with the highest levels of functional impairment, where caregiving demands and psychosocial burden may be particularly substantial. The semi-structured interview design allowed participants to raise issues most salient to their lived experience; however, it also constrained the ability to consistently explore the extent to which decisions such as foregoing parenthood were directly attributable to HD, highlighting an area for future focused inquiry. In addition, almost all participants from the patient and caregiver groups were not related, constraining insights into caregiving dynamics. The absence of clinical data on disease severity limited interpretation across disease stages. Despite providing rich, in-depth accounts of the lived experiences of individuals with HD and family caregivers, this study is based on a relatively small sample size (N = 42). As such, the findings should be interpreted as qualitative and largely anecdotal rather than as quantitative. While this does not diminish the validity or importance of the experiences described, it does limit the extent to which the findings can be extrapolated to the broader HD population. While international representation added diversity, the small sample size per country precluded meaningful cross-country comparisons and limited conclusions on specific national healthcare system support frameworks. As such, findings should not be interpreted as representative of individual country-level healthcare performance, given the limited number of interviews conducted within each country. Nevertheless, the consistency of themes observed across countries suggests shared and potentially universal caregiving experiences. Future studies with larger, country-specific samples and targeted evaluation of healthcare and social support systems would be valuable to further explore these relationships. Suicidality, a recognized feature of HD, was infrequently reported in this study, which may reflect the interview context rather than true absence. As interviews relied on spontaneous disclosure rather than direct questioning, experiences related to suicidal thoughts may be underrepresented. This underscores the importance of future research designed to more fully explore suicidality and its implications for individuals with HD and their families.
Future research should examine the impact of HD diagnoses across generations and over time to better understand how the disease's evolving demands shape caregiver responsibilities, impose intergenerational economic consequences, and contribute to the overall burden. Such studies would also provide insights into how the manifestations and effects of HD shift across generations.
Supplemental Material
sj-docx-1-hun-10.1177_18796397261443133 - Supplemental material for The holistic burden of Huntington's disease: A qualitative study of multigenerational impact on individuals and family caregivers across Europe
Supplemental material, sj-docx-1-hun-10.1177_18796397261443133 for The holistic burden of Huntington's disease: A qualitative study of multigenerational impact on individuals and family caregivers across Europe by Charlie Albert Smith, Savita Bakhshi Anand, Astri Arnesen, Cecilia Jimenez-Moreno, Charles Patrick Khoury, Helen Luck, Joshua Trivlidis, Doorsa Tarazi, Mai-Lise Nguyen, Anna Kotzeva, Kunal Samanta and Carla Dias Barbosa in Journal of Huntington's Disease
Footnotes
Acknowledgements
The authors would like to thank all of the individuals with HD and family members of individuals with HD who gave up their time to participate in this study. We are also grateful to the patient organisation leads and partners for their valuable contributions to this important study, particularly for their commitment over the course of this project and its efforts to highlight a less-researched aspect of HD. These organisations include: European Huntington Association, Huntington Disease Association of England & Wales, Scottish Huntington's Association, Asociación Corea de Huntington Española, Fondazione Lega Italiana Ricerca Huntington, Association Huntington France, Landsforeningen Huntington Sygdom, and Deutsche Huntington-Hilfe e.V. We also acknowledge the foundational contributions of former project colleagues, Umang Ondhia and Mar Ferrero of Roche, who were essential for the creation and publication of this research, respectively. The study was funded by F Hoffmann-La Roche Ltd, Basel, Switzerland in accordance with Good Publication Practice (GPP) 2022 guidelines (![]() ) and was conducted in collaboration with Shift Health and Evidera. Shift Health and Evidera were employed under contract by F. Hoffmann-La Roche Ltd for the purposes of this work to manage an independent and credible study and to gather unbiased viewpoints.
) and was conducted in collaboration with Shift Health and Evidera. Shift Health and Evidera were employed under contract by F. Hoffmann-La Roche Ltd for the purposes of this work to manage an independent and credible study and to gather unbiased viewpoints.
Consent to participate
Participants provided both electronic and oral consent to take part in this study.
Consent for publication
Participants provided both electronic and oral consent to publish information gathered for this study.
Author contributions
This study was funded by F. Hoffmann-La Roche Ltd. F. Hoffmann-La Roche Ltd defined the overall concepts, scope, and details of the study, provided funding, and reviewed and approved technical documents. Shift Health, a health research and strategy consulting firm, was responsible for overall project management, secondary data analysis, data interpretation, and manuscript drafting. Evidera, a research organization specializing in patient-centered outcomes and health economics, developed technical documents supporting the research, including the protocol, training materials, documents describing the analytic approach, and the study report. Evidera also conducted and analyzed interviews and reported the study results. Local patient advocacy groups collaborated with Evidera to identify, screen, and schedule eligible participants for interviews. The Huntington's Disease Expert Advisory Group provided input into the research design and reviewed technical documents.
All authors contributed to the interpretation of findings, critically revised the manuscript for important intellectual content, and approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CAS was an employee of Evidera and later an employee of F. Hoffmann-La Roche and stockholder of F. Hoffmann-La Roche AG at the time of this research
SBA and CDB are employees of Evidera (a business unit of PPD, part of Thermo Fisher Scientific), which received funds from F Hoffmann-La Roche to conduct the study.
AA has received consulting fees from F Hoffmann-La Roche.
CJM was an employee of Evidera (a business unit of PPD, part of Thermo Fisher Scientific), which received funds from F Hoffmann-La Roche to conduct the study.
CPK, HL, JT, DT are employees of Shift Health which consults with organisations across the health and life sciences sector, including F Hoffmann-La Roche. CK, HL, JT and DT were employed under contract with F Hoffmann-La Roche for the purposes of this study. MLN, AK and KS are current employees of and shareholders in F Hoffmann-La Roche
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.