
Abstract
BACKGROUND:
Very low birth weight (VLBW) infants must achieve several maturational milestones to be discharged home from the NICU.
OBJECTIVE:
Describe the timing of maturational milestones in VLBW infants and the impact of clinical variables and milestone achievement on postmenstrual age (PMA) at discharge.
METHODS:
For VLBW infants without severe lung disease discharged home from a level IV NICU, we assessed PMA at the achievement of thermoregulation, cardiorespiratory stability, feeding, and discharge.
RESULTS:
In 400 infants (median GA 28.4 weeks), lower birth weight, white race, and having multiple comorbidities of prematurity predicted later discharge PMA. The most common milestone sequence was CPAP discontinuation, caffeine discontinuation, thermoregulation, apnea resolution, and full oral feeds. PMA at apnea resolution and full oral feeds correlated highly with discharge PMA.
CONCLUSIONS:
In a single-center VLBW cohort, comorbidities of prematurity impacted the timing of NICU discharge through delay in oral feeding and cardiorespiratory stability.
Introduction
Premature infants require respiratory and nutritional support and continuous monitoring in a Neonatal Intensive Care Unit (NICU) until near or beyond term corrected age. Length of NICU stay for very low birth weight infants (VLBW, < 1500 grams) inversely correlates with gestational age (GA) due to immaturity of multiple organ systems, and in some cases due to organ damage that impacts milestone achievement. A greater understanding of variables that impact physiologic stability and maturation could lead to strategies to facilitate earlier discharge home for some VLBW infants [1].
Milestones generally considered necessary for discharge home from the NICU include the ability to thermoregulate without an incubator, breathe without pressure support and without significant apnea, and eat by mouth without a nasogastric tube. Recent studies have demonstrated that earlier weaning from an incubator is feasible and safe but may not substantially impact the timing of NICU discharge [2, 3]. Major factors influencing the duration of NICU stay include lung disease and apnea [4–6]. In our prior work on apnea, we found that the number and duration of oxygen desaturation and bradycardia events at 32 weeks PMA predicts prolonged stay in the NICU [7]. Finally, full oral feeding requires both respiratory stability and neurologic maturity, and VLBW infants often require prolonged tube feeding even after reaching other maturational milestones [8–10]. Some infants may be discharged home with medications or equipment to support breathing and feeding, which requires significant caretaker education and outpatient support [11–13].
In this study, we analyzed the achievement of five maturational milestones that typical VLBW infants achieve as they approach term PMA: transition off continuous positive airway pressure (CPAP), discontinuation of caffeine therapy, thermoregulation out of an incubator, resolution of significant apnea of prematurity, and full oral feeding. We specifically excluded infants with severe bronchopulmonary dysplasia to focus on infants with more typical milestone acquisition, but did not exclude infants who ultimately went home on medications or equipment, including tube feedings. The goal of this study is to determine variables associated with prolonged NICU stay and describe the typical sequence of achieving milestones required for discharge in order to identify infants for whom advanced planning for post-discharge supportive therapies might lead to earlier and safe discharge home.
Methods
Study design
We conducted this retrospective study with approval from the Institutional Review Board with a waiver of consent. The inclusion criteria were birth weight < 1500 grams, GA < 33 weeks, admission to the NICU at the University of Virginia (UVA) from 2012–2017, and discharge home. We excluded infants if they had major chromosomal or congenital anomalies, were transferred to UVA beyond 32 weeks PMA, or required high-level respiratory support beyond 36 weeks PMA, defined as requiring mechanical ventilation, Non-invasive positive pressure ventilation, or CPAP. We collected clinical and demographic data from the electronic medical record (Epic, Verona, WI) and a NICU database (NeoData, Isoprime, Chicago, IL).
Definitions
Dates and PMA of maturational milestones were abstracted from the medical record and determined using the following guidelines and definitions:
CPAP discontinuation: the first day an infant did not require any duration of CPAP, excluding a transient need for CPAP or higher level respiratory support after a procedure. Decisions about CPAP discontinuation were made at the discretion of the care team with the general unit guideline to consider transitioning off CPAP at 30–32 weeks PMA to either nasal cannula or room air. For infants never on CPAP, we used the birth date and gestational age as the date and PMA to achieve this milestone. Caffeine discontinuation: the last date of a caffeine dose, including doses given within a week of caffeine discontinuation due to recurrent events. The unit guideline recommends caffeine for all infants with significant apnea and, since 2015, to prophylactically initiate caffeine therapy for all infants < 32 weeks’ gestation. Caffeine is discontinued once an infant weans off of respiratory support that provides positive end-expiratory pressure and no longer has significant apnea events requiring stimulation. For infants who never received caffeine, we used GA as the PMA for this milestone, and for those discharged on caffeine we used discharge PMA. Thermoregulation: the first day the infant no longer required an external heat source, excluding a transient need for heat after a procedure. The unit guideline recommends weaning the incubator temperature gradually once the infant weighs > 1500g and transitioning to a bassinet or crib once the infant’s temperature is stable in a 26°C incubator. Apnea resolution: the date an infant completed an event-free “countdown” following either caffeine discontinuation (including a 5-day washout period) or the last documented event requiring intervention, whichever came later. An event requiring intervention included any apnea, bradycardia, desaturation (ABD) of any duration, or combination that required tactile stimulation, repositioning, supplemental oxygen, or bag-mask ventilation. Our unit’s recommended apnea countdown period was eight days [14] until 2015, and seven days thereafter. For infants who never received caffeine and never had documented ABD events, we used the gestational age as the PMA of apnea resolution. Full oral feeding: the first date on goal feed volume the infant did not require any tube feedings. The unit guideline is to offer oral feeding beyond 32 weeks PMA once an infant is off CPAP and showing readiness. Nurses increase oral feedings and remove the enteric tube once an infant consistently takes at least 75%of the volume prescribed. We typically prescribes a goal feeding volume of 150 ml/kg/day. In the years of this study, our unit did not have a home nasogastric feeding program. Infants who were not making progress with oral feeds but were otherwise ready for discharge were considered for surgical gastrostomy tube placement if parents favored this option.
Statistics
The median (25th, 75th percentile) or number (%) was calculated to describe variables unless otherwise indicated. We compared the demographic and clinical characteristics, including the Score for Neonatal Acute Physiology with Perinatal Extension 2 (SNAPPE-2) [15], for infants discharged before versus after 40 weeks PMA using Fisher’s test for categorical variables and Mann-Whitney U tests for continuous variables with non-normal distributions. We used multivariable linear regression to test the association of clinical variables with PMA at discharge. The model included demographic and clinical variables as predictors. We calculated Spearman correlation coefficients for PMA at each milestone and PMA at discharge. We assessed statistical significance using a two-tailed p-value < 0.05 and performed statistics using GraphPad Prism version 8.0.0 for Windows (GraphPad Software, San Diego, CA) and R version 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Cohort characteristics
During the years of analysis (2012–2017), 650 VLBW infants were admitted to the UVA NICU. We excluded 58 infants who died, 126 infants on high-level respiratory support at 36 weeks PMA, 10 with major congenital anomalies, and 56 who were transferred to outside facilities before NICU discharge. Table 1 shows the characteristics of the 400 infants meeting inclusion criteria, grouped by whether they went home before or after their due date. Infants with PMA≥40 weeks at discharge had lower GA and BW, higher SNAPPE-II scores, and more comorbidities of prematurity than infants discharged before 40 weeks PMA (Table 1, p < 0.05). SNAPPE-II scores were missing in 77 infants for whom data from the first 12 hours after birth were unavailable due to transfer from an outside hospital. We developed a multivariable linear regression model using birth weight, multiple gestation, sex, antenatal steroids, race, year, and a count of comorbidity diagnoses as predictors. Lower BW, white race, and an increasing number of comorbidities (sepsis, NEC, severe IVH, or BPD) were linearly associated with increasing PMA at discharge (p < 0.01). We used BW and not GA as a predictor in the model since these two variables were highly correlated (r = 0.78).
Cohort characteristics, grouped by discharge at < or≥40 weeks PMA. Categorical variables are shown as n (%) and continuous variables as median [25th, 75th %ile]. (*p < 0.05)
Cohort characteristics, grouped by discharge at < or≥40 weeks PMA. Categorical variables are shown as n (%) and continuous variables as median [25th, 75th %ile]. (*p < 0.05)
Figure 1 shows the distributions of PMA at the achievement of each milestone. The milestone PMA did not change significantly over the years studied, 2012–2017. On average, infants weaned off CPAP first, followed shortly thereafter by caffeine discontinuation. Weaning from an incubator occurred next, followed by apnea resolution and full oral feeding. Median PMA at these milestones was 32.5, 33.7, 34.6, 36.3, and 36.3, respectively. Twelve infants (3%) were never treated with CPAP or higher respiratory support and 22 (6%) never received caffeine.
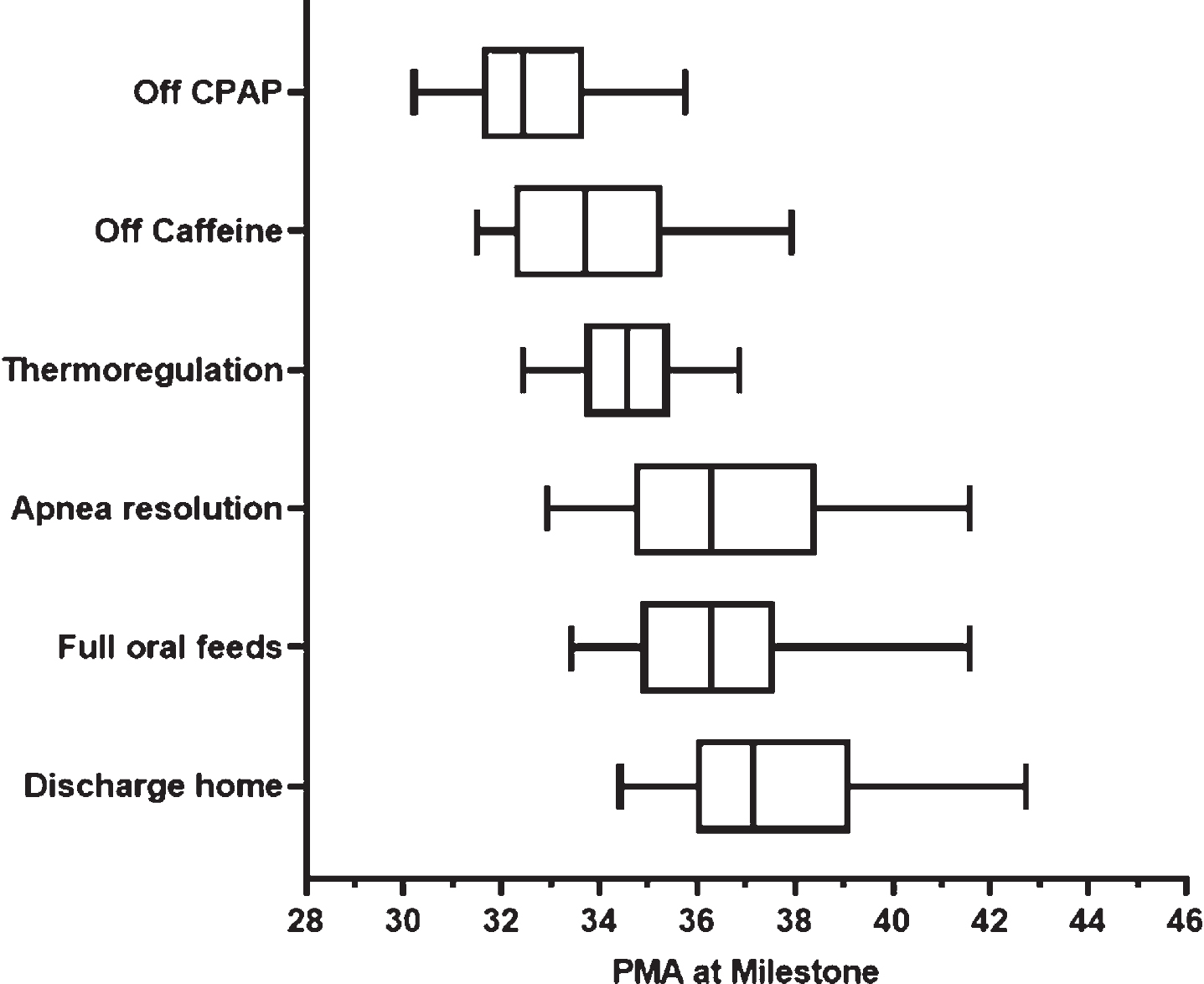
Milestone PMA. For 400 VLBW infants not requiring high-level respiratory support at 36 weeks PMA, the time of achieving milestones is shown. The boxes represent the first and third quartiles with a line at the median, and the whiskers represent the 5th and 95th percentiles.
Caffeine discontinuation occurred, on average, ten days after the transition off CPAP. The timing of these two milestones varied widely, from 10 days before to 44 days after, reflecting variability in practice and individual patient factors. For 54%of infants, the final milestone achieved prior to discharge was resolution of apnea. For most infants, this occurred after caffeine discontinuation followed by a 5-day caffeine washout period, and then a 7-8 day “countdown” period without ABDs requiring intervention. Sixteen infants (4%) were discharged home on caffeine and an apnea monitor due to the emergence of significant ABD spells after one or more attempts at caffeine discontinuation. Of note, 43 infants had a late ABD event documented within a week of discharge, and only ten of these infants had a home apnea monitor prescribed. A review of clinician notes indicated that many late events were attributed to feeding issues and gastroesophageal reflux, and some occurred following stressors such as vaccines, eye exams, or inguinal hernia repair.
Table 2 shows that full oral feeding was the final milestone achieved for 37%of the cohort, and these infants had higher median gestational age and birth weight than those with apnea resolution as the final milestone. Fourteen infants were discharged on tube feeds (1 nasogastric and 13 gastrostomy tubes). Thermoregulation was the final milestone achieved for 10%. These infants had lower discharge PMA and were less likely to have required CPAP or caffeine.
Characteristics of infants, grouped by the last achieved milestone
Lower GA correlated with increasing PMA at all milestones, with the exception of thermoregulation. (Fig. 2) Discharge often occurred before term corrected age (< 37 weeks PMA) for infants born at 29–32 weeks GA but more often occurred at or beyond term corrected age for infants born < 29 weeks GA.
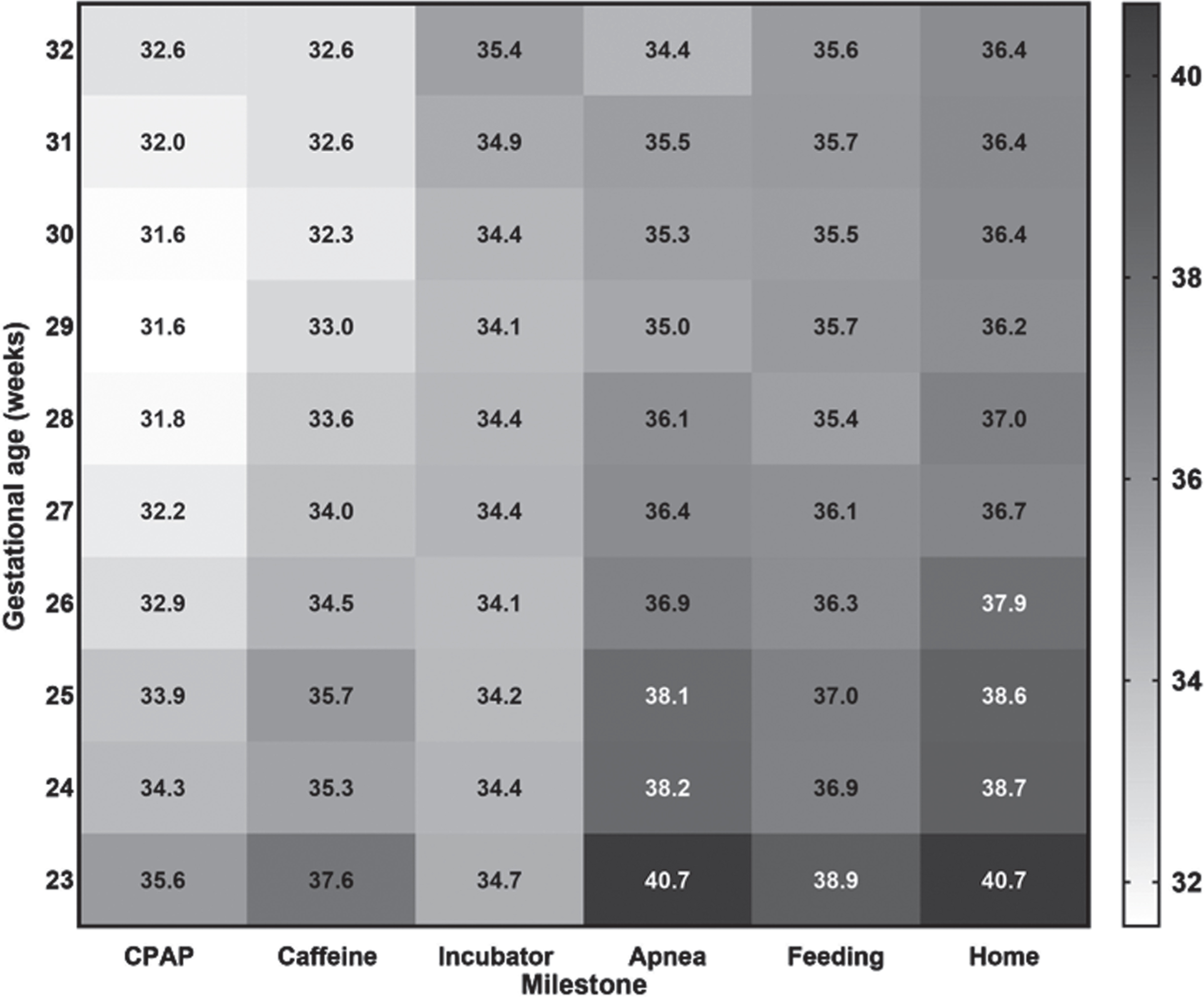
Impact of GA on PMA at milestone achievement. Heat map showing median PMA at the achievement of each milestone, including discharge home (columns) based on gestational age in weeks (rows). The color gradient depicts increasing PMA with darker shading.
For 90%of infants, the achievement of full oral feeding and finishing an apnea countdown were the final milestones before discharge. Figure 3 shows PMA at achieving the feeding milestone plotted as a function of the timing of apnea resolution, demonstrating that most infants achieved these two milestones around the same PMA. We reviewed 88 infants’ records with a gap of more than two weeks between reaching full oral feedings and completing an apnea countdown, 47 with feeding occurring first, and 41 with ABD resolution first. In the latter category, the majority of infants (22/41) were born at GA > 29 weeks, had resolution of apnea at a relatively early PMA (mean 35 weeks), and were discharged at a typical PMA (mean 38 weeks). Reasons for delayed oral feeding achievement included surgical gastrointestinal issues, anatomic issues, and respiratory issues. Ten infants with a > 14-day gap between the apnea and feeding milestones had no medical reason documented, and clinician notes described poor oral feeding skills.
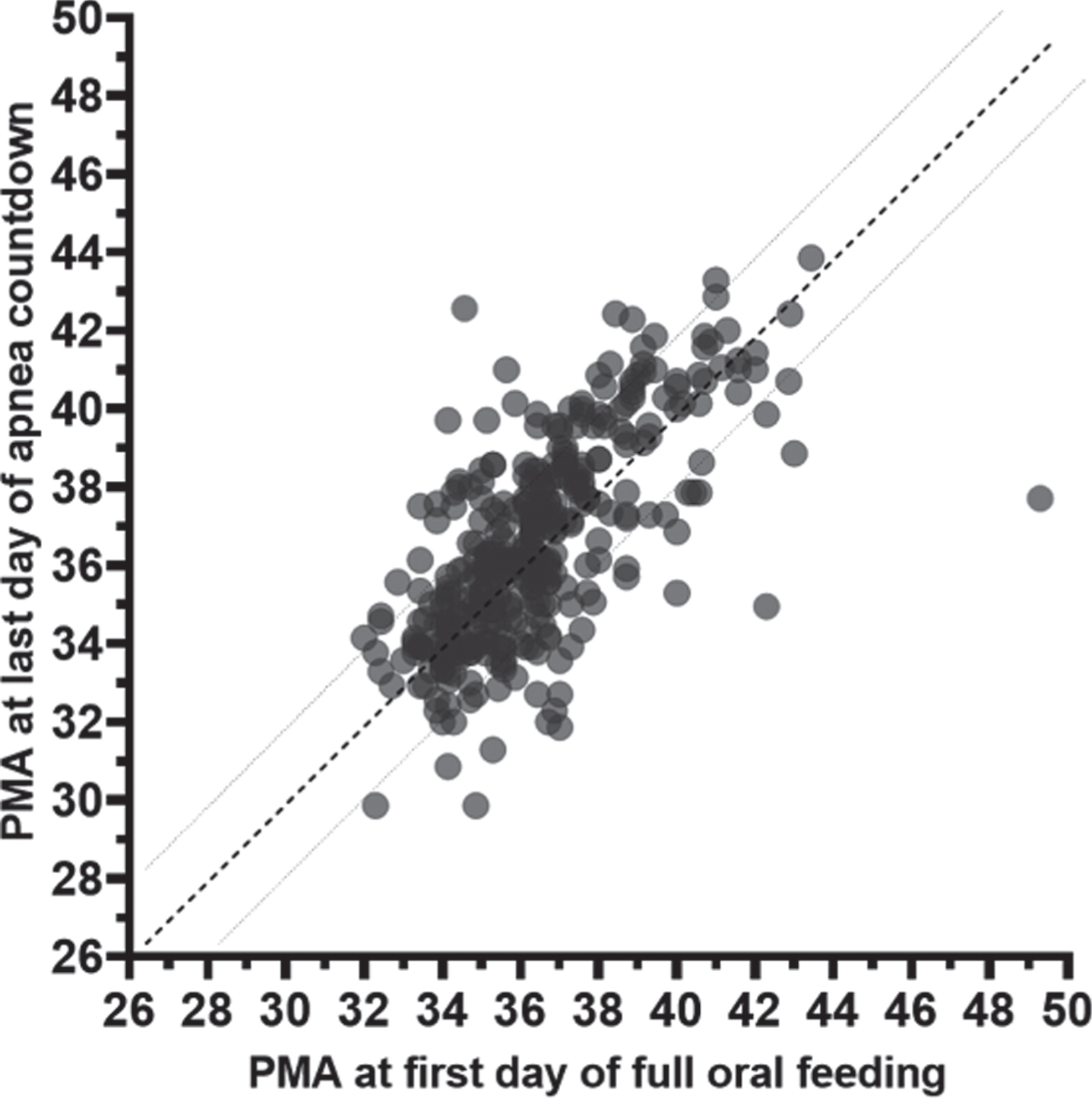
PMA at apnea resolution as a function of PMA at full oral feeding. The dashed line represents the line of unity with slope = 1, and the dotted lines represent a 2-week gap between the two milestones on either side.
Of the 47 infants with > 14 days from reaching full oral feeds to apnea resolution, 18 (38%) had documentation of suspected gastroesophageal reflux or emesis temporally associated with ABD events requiring intervention. An additional 12 infants had prolonged caffeine therapy, seven due to chronic lung disease, and five due to a surgical procedure late in the NICU stay. Six infants of relatively late GA (> 30 weeks) achieved full oral feeds quickly and spent extra time in the NICU for the apnea countdown. One infant developed late apnea with a rhinovirus infection. Finally, ten infants continued to have apnea spells requiring intervention after reaching full oral feedings, without other variables identified.
Table 3 shows Spearman correlation coefficients for PMA at milestone achievement and PMA at discharge, with incubator weaning correlating the least and full oral feeds and apnea resolution correlating the most with discharge PMA.
Spearman’s correlation coefficients testing the linear association between the PMA at each milestone achieved and the PMA at discharge
In this single-center cohort of VLBW infants, the typical sequence of achievement of maturational milestones was weaning off CPAP, caffeine discontinuation, ability to thermoregulate out of an incubator, resolution of significant apnea, and achieving full oral feeding. Variables associated with higher PMA at NICU discharge included lower birth weight, white race, and having multiple comorbidities diagnosed during the NICU course.
We limited our analysis to infants without severe BPD (those not requiring CPAP or higher respiratory support at 36 weeks PMA) since lung disease has a major impact on milestone acquisition [16, 17]. Our unit guideline recommends waiting until an infant transitions off CPAP to discontinue caffeine and initiate oral feeding, whereas other units might discontinue caffeine sooner or allow bottle feeding for infants on CPAP [18–20]. Prolonging caffeine therapy for infants with BPD [21] may explain the racial disparity we found in discharge PMA, since infants of Caucasian race tend to have more severe lung disease and therefore later discontinuation of caffeine in our unit [22]. We also found that infants requiring home oxygen were discharged at a higher PMA. This may be due in part to prolonged requirement for nasogastric tube feeding in infants with more significant lung disease, or due to additional time required for arranging home equipment and caregiver training.
Timing of apnea resolution had the greatest correlation with NICU length of stay, as others have described [10, 23]. Multiple variables affect the maturation of respiratory control and completion of an “apnea countdown”, including gestational age (24), timing of caffeine discontinuation [25, 26], duration of apnea-free monitoring, and deciding what constitutes as a significant cardiorespiratory event warranting additional inpatient observation. In a recent report, implementation of an explicit guideline for nurses to document clinically significant ABD events resulted in more accurate reporting but did not shorten the length of stay [26]. Our unit guideline, in the years of this review, included a five-day caffeine “washout,” followed by a 7-8 day apnea countdown for VLBW infants [14]. Recent data suggest that infants of higher gestational age might safely be discharged following a shorter observation period of 5 spell-free days [4].
We identified several infants who ultimately went home on caffeine after having apnea during their countdown period, but stayed in the NICU for up to a week longer than anticipated. Predicting prolonged NICU stay might allow identification of infants, such as those at risk for apnea resolution at a later PMA, for whom advanced planning for post-discharge medications and support could lead to earlier, safe discharge. We previously found that the duration of desaturation spells at 32 weeks PMA predicted discharge at > 40 weeks PMA [7] and speculate that some of these infants might benefit from prolonged caffeine therapy. In a pilot randomized trial, caffeine beyond NICU discharge reduced intermittent hypoxemia events [21, 27] and this is the subject of an ongoing larger randomized clinical trial (ICAFF RCT, ClinicalTrials.gov NCT03321734). Additionally, a trial of post-discharge caffeine for moderately preterm 29–33 w GA infants is underway, with length of NICU stay as the primary outcome (MoCHA RCT, ClinicalTrials.gov NCT0334072).
The PMA at achieving thermoregulation varied little, suggesting that maintaining temperature out of an incubator depends on neurologic maturation, and morbidities such as lung disease have less impact. Several clinical trials found weaning infants from the incubator at a lower weight to be safe without an adverse effect on weight gain, but that this practice may not significantly shorten length of stay [2, 28]. We found that only 10%of infants achieved all other milestones before thermoregulation, therefore PMA or weight at incubator discontinuation had little impact on NICU length of stay in our cohort.
For many infants in our review, the ability to take all feedings by mouth came last and therefore determined discharge timing. Most infants achieved the feeding and breathing without apnea milestones within two weeks of each other. Infants who achieved apnea resolution at least two weeks earlier than full oral feeding had higher gestational age and fewer comorbidities. However, those who achieved full oral feeding after term corrected age suffered more adverse events, such as sepsis or NEC, than those who fed by mouth earlier [9]. For the 42 infants in our cohort with a long gap between achieving all other milestones and full oral feeding, arranging tube feeds at home might have significantly shortened the NICU stay. Our center recently instituted a home nasogastric tube feeding program for preterm infants who are otherwise stable for discharge, with daily contact with families to ensure weight gain and ease the transition to the home environment. Early results after a year of the program showed that this might reduce NICU length of stay by about a week for select patients [12].
Several limitations of our analysis deserve consideration. First, we did not include infants back-transported to referring NICUs, many of whom were less critically ill in their initial NICU course and may have achieved milestones earlier. Second, the significant variability in clinical practices in our unit, despite guidelines, limits our ability to separate physiologic maturation from practice variation in the analysis of the timing of milestone achievements. Third, we were not able to account for complex sociodemographic variables that could impact discharge readiness. Finally, our findings may not directly translate to other NICUs with different practices, patient demographics, and rates of preterm morbidities such as chronic lung disease and necrotizing enterocolitis, which have a significant impact on NICU length of stay [1].
Conclusion
Infants born extremely preterm require prolonged NICU stay for supportive technologies and specialized care as they mature. In our study of 400 VLBW infants without severe lung disease, most infants followed a similar sequence of achieving maturational milestones. Lower birth weight, white race, and the number of morbidities experienced during the NICU course predicted later discharge PMA. Persistent apnea and the need for tube feeding contributed to an extended length of stay, with comorbidities and degree of prematurity as covariates. Efforts to facilitate earlier safe discharge home from the NICU, including caffeine therapy and nasogastric tube feeding at home, might not only shorten the hospital stay for some infants but also improve other outcomes by facilitating earlier family-centered care.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethics statement
This study was performed in accordance with the Declaration of Helsinki. The UVA Internal Review Board for Health Sciences Research approved the study with a waiver of informed consent (protocol # 12008).
Availability of data and materials
Our data are available to readers upon request.
Funding
K23 HD097254 (PI: B. Sullivan); R01 HD072071 (PI: K. Fairchild)
Author contributions
BS designed the study, performed statistical analyses, and wrote the first draft of the manuscript; KF made a substantial contribution to the conception and design of the study and editing the manuscript; CS and SA collected the data from the medical records, performed statistical analyses, and produced the figures; RS contributed to the interpretation of the results and editing of the manuscript. All authors approved the final version to be published.
Footnotes
Acknowledgments
None.