
Abstract
Patients with breast or prostate cancer have a high chance of developing bone metastasis, which is associated with many skeletal-related events. The development of novel bone metastasis treatments is lagging behind due to the lack of reliable models. We aimed to develop a humanized bone metastasis model comprising vital human bone discs and human metastatic cancer cells (bone metastasis discs), which were subsequently cultured ex vivo or subcutaneously implanted into nude mice. Ex vivo culture experiments confirmed that cells within the bone metastasis discs remained metabolically active, while the presence of metastatic cancer cells could be monitored using bioluminescence. Although histological analyses confirmed the presence of relevant bone cells in the human bone tissue, no apparent formation of metastatic lesions was detected over the 2-week ex vivo culture period. In contrast, subcutaneously implanted bone metastasis discs demonstrated clear metastatic lesion formation, with osteolytic characteristics, that progressed from 3 to 6 weeks after implantation for both breast and prostate cancer bone metastasis discs. Histologically, healthy bone tissue with bone marrow compartments as well as anastomosis was observed. Cisplatin treatment of ex vivo cultured bone metastasis discs significantly decreased the bioluminescent signal from (prostate) cancer cells, while no effects of cisplatin treatment were observed for in vivo implanted bone metastasis discs. Our data provide a proof of concept for an ex vivo/in vivo bone metastasis model with vital human bone and human metastatic cancer cells but require further fine-tuning to improve robustness, relevance, and quantification methods. Future research could potentially use these models for the evaluation of novel bone metastasis treatments, accelerating their potential clinical application.
Impact Statement
Bone metastasis remains a major clinical challenge in breast and prostate cancer, in part due to the lack of physiologically relevant human-based experimental models for therapy development. This study presents a proof-of-concept humanized bone metastasis platform that integrates vital human bone tissue with human metastatic cancer cells in both ex vivo and in vivo settings. By demonstrating sustained tissue viability, tumor cell monitoring, and clinically relevant osteolytic lesion formation in vivo, this work advances current bone metastasis modeling beyond conventional animal and in vitro systems. Although further optimization is required, this dual ex vivo/in vivo approach provides a promising foundation for more predictive preclinical testing of bone-targeted anticancer therapies, with potential to accelerate translation toward clinical application.
Introduction
Breast and prostate cancers spread in approximately 60% and 80% of patients to form bone metastasis.1,2 Once such a bone metastatic lesion is diagnosed, 5-year survival rates for patients rapidly drop down to approximately 10%, 3 and patients may experience painful skeletal-related events (e.g., bone fractures). 1 Current treatment of bone metastasis encompasses a multimodal approach, wherein chemotherapy, radiation, osteoclast-targeted therapy, and possible resection of the metastatic lesion are combined.4,5 However, as evident from the low survival rates, these treatments are not sufficient, and new therapies are needed. Examples of these new therapies are bifunctional bone grafts, immunotherapy, or therapies targeting specific parts of the bone metastasis vicious cycle. 6 These new treatments have largely been evaluated in in vitro models based on cancer cell lines or simplistic subcutaneous cancer models in mice.7–15 However, to expedite clinical use of these treatments, evaluation of these treatments in bone metastasis animal models is needed. 16
Currently, most traditional bone metastasis animal models are not utilized for evaluation of novel treatments, but they are designed for unraveling key events of the bone metastasis process. The general concept of these models is to inject cancer cells, either from cell lines or xenografts from human biopsies, orthotopically, intracardially, via caudal vessels, or intraosseously in an attempt to establish bone metastasis. However, all of these injection methods are accompanied by various drawbacks such as technical difficulties, metastasis to other organs, and low bone metastatic take rates. 17 Currently, the most convenient method entails intraosseous injection, as it results in the highest bone metastatic lesion take rate, 17 but this stalls at ∼85% depending on the cancer cell type. 18 Other drawbacks related to these traditional bone metastasis models are the structural and molecular differences between animal and human bone 19 and severe animal suffering as animals might experience impaired mobility.18,20
To improve traditional bone metastasis in vivo models, ongoing research has recently shifted toward the use of implanted vital human bone as a site for cancer cells to form bone metastatic lesions.21–32 This approach presents several advantages, since it humanizes the bone (micro)environment in an animal model, decreases animal suffering as it is not their own skeletal system that is being affected, and reduces the number of animals required if multiple bone explants per animal are implanted. To this end, various sources of human bone have been explored, such as human fetal bone, 33 rib bone after lung cancer removal,25,27,29–31 or bone from discarded femoral heads after hip replacement surgery.22–24,26,28,32,34 From those options, bone from femoral heads is considered most favorable as this source (i) involves the least ethical restrictions, (ii) is likely to be free of cancer cells, and (iii) functioned as load-bearing bone that is known to exhibit superior osteogenic responses. 35 Notably, similar drawbacks as reported for the traditional bone metastasis models, for example, metastasis to other organs24–27,29 or low bone metastatic take rates,23,28 still persist in these bone metastasis in vivo models. Other limitations for these bone metastasis models are (i) the decreased reproducibility, as bone is often morselized instead of cut to standard size,22,23,25,28–32 (ii) the lack of quantification of metastatic lesion progression during experimental procedures, and (iii) failure to demonstrate the localization of the metastasis in the human bone explants. Besides in vivo implantation of human bone,21–32 ex vivo organ cultures34,36–39 can also be explored for the assessment of metastatic lesion formation and progression.
We herein focus on overcoming these aforementioned drawbacks by the development of a fully humanized and standardized bone metastasis model comprising vital human bone tissue and human metastatic cancer cells. To achieve this aim, we sourced human femoral heads, which we processed into trabecular bone discs with a central defect to serve as the location for metastatic cancer cell seeding. This “forced metastasis” method has proven to be successful in previous work,22,34 but a consistent 100% metastatic lesion take rate has not yet been achieved. Attempting to overcome this limitation, we increased metastatic cancer cell seeding numbers from 0.01 (34) to 0.25 million per bone disc. Bone discs were then either used for ex vivo organ culture or subcutaneous implantation in nude mice and followed up for analysis of bone metastatic lesion formation and progression with nondestructive (e.g., metabolic activity, bioluminescence, and cytokine secretion) and destructive (histology and immunohistochemistry) techniques. In addition, we tested in both models the efficacy of systemic chemotherapy treatment with the model chemotherapeutic drug cisplatin4,40 by its supplementation to the culture medium or intravenous injection.
Material and Methods
General cell culture
Breast cancer cells (MDA-MB-231, ATCC), prostate cancer cells (PC3; kindly provided by the Department of Urology, Radboudumc, The Netherlands), and prostate cancer cells transfected with luciferase (PC3_LUC; kindly provided by the Department of Urology, Radboudumc, The Netherlands) were maintained in a log phase in basic medium (BM; αMEM without ascorbic acid (A14090, Gibco) supplemented with 10% fetal bovine serum (FBS, Gibco) and 1% penicillin–streptomycin (P/S, Gibco)) in standard conditions (a humidified atmosphere with 5% CO2 at 37°C).
Bone disc preparation and culture
The local medical ethics review committee was consulted for the experimental use of left-over femoral heads after hip replacement surgery (Radboudumc, The Netherlands); ethical approval for the anonymous use as reported herein was not required (only gender and age were to be reported; Supplementary Table S1). Obtained femoral heads were stored at 4°C until further processing (max. 16 h) to prepare bone discs (Fig. 1A). With an 8 mm diameter trephine drill (MF Dental), bone cylinders were harvested. These cylinders were cut to the intended size with a circular table diamond saw (Struers), removing the cortical bone layer, which resulted in the final bone discs (8 mm diameter, 4 mm height; Fig. 1A). 34 With a stationary bench drill (H260 104 023, Komet Dental), a central defect was drilled (2.2 mm diameter and 3 mm depth) to facilitate metastatic cancer cell loading. During all cutting and drilling procedures, the samples were gently rinsed with sterile PBS (Gibco) to dissipate generated heat. Discs were stored in BM + an extra 1% P/S for 1.5 h before inverting the discs on a petri dish to desiccate the central defect from media and placing the discs into a 24-well plate. For metastatic cancer cell seeding, various conditions were explored in pilot experiments to find the most appropriate method that would result in grafting the highest number of cancer cells without residual cancer cells growing on the tissue culture plastic or in the PBS washing step (Supplementary Table S2). Ultimately, the most appropriate condition was 0.25 million cancer cells (either MDA-MB-231, PC3, or PC3_LUC) concentrated in 10 µL of cell culture medium, which was then carefully pipetted into the central defect of a bone disc. For all bone discs, BM was carefully added via the walls of the well until the bone disc was just submerged; subsequently, bone discs were cultured for 24 h in standard conditions. Thereafter, bone discs were washed by picking up the bone discs with forceps and submersing them three times in fresh PBS after which they were placed into a fresh 24-well plate. Bone discs were then either continued for ex vivo culture supplemented with 2 mL BM per well and refreshed every ∼3 days (Fig. 1B) or implanted subcutaneously in nude mice for in vivo studies (Fig. 1C). An overview of experimental conditions can be found in the supplementary files (Supplementary Table S3).
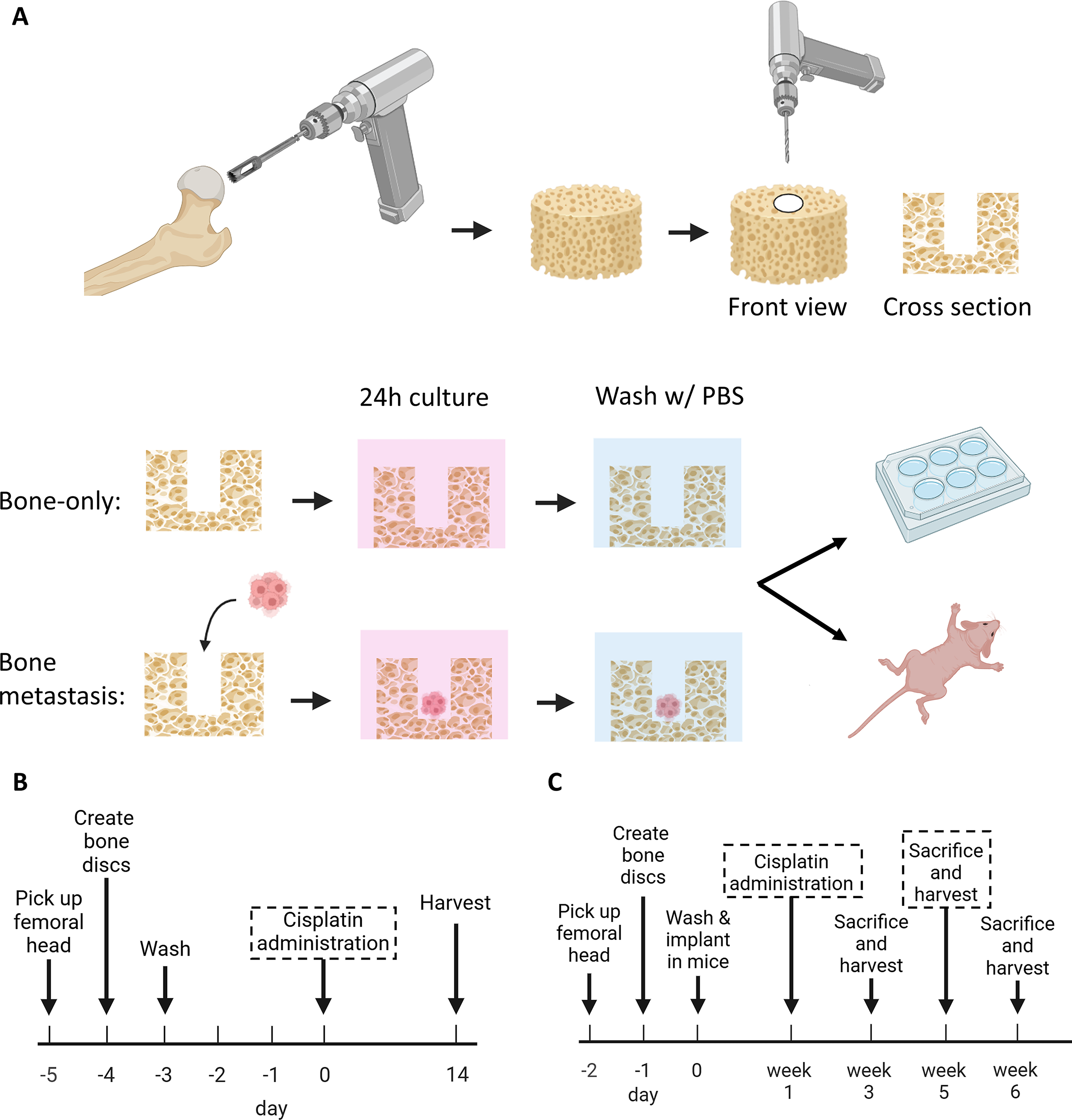
Schematic representation of bone disc preparation and subsequent experimental procedures to establish a human bone metastasis model.
Ex vivo bone disc experimental procedures
Systemic cisplatin administration
Cisplatin (AK Scientific) was dissolved in αMEM and subsequently diluted to attain final concentrations of 25, 50, or 100 µM. Bone discs (n = 3) were exposed to cisplatin for a 24-h treatment period at day 0.
Metabolic activity measurements
Metabolic activity of cells within bone discs (n = 3) was measured at days −3, 1, 4, 7, 10, and 14 with an AlamarBlue assay (Thermo Fisher Scientific), according to manufacturer’s instructions. In short, a 10% AlamarBlue solution in BM was prepared and supplemented to the bone discs, which were placed in a new well plate. After 4 h of incubation, 200 µL of supernatant was transferred to a black 96-well plate for measuring fluorescent intensities with an excitation of 560/30 nm and emission of 620/40 nm with a plate reader (BioTek Synergy HTX Multi-Mode Reader). All metabolic values were corrected for background, and values of each bone disc were related to baseline values at day −3. Lastly, bone discs were washed with PBS and supplemented with fresh media for continuation of ex vivo culture.
Ex vivo bioluminescence intensity measurements
Luciferin (IVISBrite™ D-Luciferin potassium, Perkin-Elmer) was dissolved in PBS (30 mg/mL) to prepare a working solution of 150 µg/mL luciferin in BM. On days −3, 0, 1, 4, 7, 10, and 14, bone discs (n = 3) were placed in a black 24-well plate with a forceps, and 1 mL of working solution was supplemented to each bone disc for an incubation duration of 15 min. Bioluminescence intensity was then measured with an optical imager (MILabs) with an exposure time of 1 min, iris setting of f/2.8, preamp value of 2X, binning of 2 × 2, and open emission filter. A photographic reference image was taken with the same iris and preamp value and a 200 ms exposure time. With accompanying software (MILabs), bioluminescence intensities were acquired per area of bone disc (e−/s/sr/mm2). All bioluminescence intensities of each bone disc were related to baseline values at day −3. Bone discs were then washed with PBS and supplemented with fresh BM for continuation of ex vivo culture.
Quantification of matrix metalloproteinase-9
Supernatants of bone disc (n = 3) cultures were collected at days 0, 4, 7, 10, and 14, and centrifuged at 300 g for 3 min to sediment bone debris. Then, 1 mL of bone debris-free supernatant was frozen at −70°C until further use. Matrix metalloproteinase-9 (MMP-9) concentrations in supernatants were measured with an enzyme-linked immunosorbent assay (Biotechne, R&D Systems) according to the manufacturer’s instructions. In short, plates were coated with capture antibody, subsequently blocked with bovine serum albumin (Biotechne, R&D systems), after which 100 μL of undiluted supernatant or standard was added. Thereafter, detection antibody, subsequent streptavidin-horseradish peroxidase, substrate solution, and stop solution were added. Absorbance was read at 450 and 540 nm (for correction) with a plate reader.
In vivo procedures
Animal operation procedures
Bone discs seeded with metastatic cancer cells were transported to the animal facility after overnight culture and implanted subcutaneously into nude mice (Mus Musculus, BALB/cAnN-Foxn1nu/nu/Rj//Janvier, at least 6 weeks old) in accordance with ethical approval document AVD10300202216051 (Centrale Commissie Dierproeven). A total of four bone discs per animal were implanted, two on each side of the vertebral column, with the central defect facing the skin. Female and male animals were used for metastatic breast cancer discs and prostate cancer discs, respectively. At 24–48 h prior to surgery, animals ingested analgesia (RIMADYL) via drinking water, and all animals received a subcutaneous injection of carprofen (RIMADYL) 0–4 h before surgery. For implantation of bone discs, animals were anesthetized with inhalation of isoflurane (Isoflutek). A single subcutaneous incision was made centrally on the back of the animals, and four subcutaneous pockets were made using tunneling, followed by placement of one bone disc per pocket. The incision was then closed with sutures. For the first experiment, to determine sustained bone viability and bone metastasis progression, a total of 6 mice were used (1 male and 1 female with bone-only discs, 2 females with breast cancer bone metastasis discs, and 2 males with prostate cancer bone metastasis discs). For the second experiment, to determine bone metastasis progression after cisplatin treatment, a total of 4 mice were used (4 males with prostate cancer bone metastasis discs).
Animal treatment
After surgery, mice were fed with booster food for 7 days, checked closely for discomfort, and weighed daily for 10 days. Subsequently, mice were weighed and checked two times per week. Skin wounds on top of bone discs were treated with honey ointment (Vetramil). At the indicated time points, animals were sacrificed by CO2 suffocation.
In vivo bioluminescence intensity measurements
Fresh luciferin solutions were prepared prior to each bioluminescence intensity measurement. For this, 30 mg of luciferin was dissolved in 2 mL of DPBS (w/o Mg2+ and Ca2+; Gibco). Per animal, 10 µL of luciferin solution/g body weight was injected subcutaneously into the neck folds. After 5 min of waiting, animals were sedated by isoflurane inhalation. Animals were then placed into the optical imager, positioning the bone discs optimally, and then bioluminescence intensity was measured with an exposure time of 1 min, iris setting of f/4.0, preamp value of 4X, binning of 4 × 4, and open emission filter. A photographic reference image was taken with the same iris and preamp value and a 200 ms exposure time. With accompanying software, bioluminescence intensity measurements were acquired per area of bone disc (e−/s/sr/mm2). All bioluminescence intensities of each bone disc were related to baseline values at week 1.
Cisplatin administration
Cisplatin was dissolved in physiological solution (0.9% sodium chloride, Fresenius Kabi) at 1.2 mg/mL and subsequently filtered with a 0.2 µm filter to sterilize the solution. At week 1, immediately after bioluminescence intensity measurements, half of the animals (n = 2) received intravenous (i.v.) injections of cisplatin (4 mg/kg body weight) or placebo (physiological solution) via their tail veins.
µCT scanning of bone discs
Formalin-fixated bone discs were scanned using a GE Phoenix NanoTom M nano-CT scanner equipped with a diamond-tungsten target and a 12-bit gray scale resolution detector (General Electric). The scans were performed at an effective voxel size of 4.9 µm. The X-ray source parameters were set to an acceleration voltage of 60 kV and a beam current of 170 µA, with an exposure time of 500 ms. A total of 1000 images were acquired over a full 360 rotation° with a rotation step of 0.5°. A 0.2 mm aluminum filter was applied during the scanning process. During image reconstruction, beam hardening correction and Gaussian filtering were performed using GE Phoenix datos|x2 software. 3D voxel-rendered models were created using CT-Vox V3.0 software (Bruker MicroCT NV).
Histological procedures
Fixation, decalcification, and embedding of bone discs
After fixation in buffered formalin (for 24 h), bone discs were decalcified in decalcifying solution composed of 10% ethylenediaminetetraacetic acid (Sigma-Aldrich) with a pH of 7.2–7.4 for an average of 3 weeks. Before further processing, bone discs were visualized with X-ray imaging (Planmeca) to verify successful decalcification. Next, bone discs were dehydrated in series of ethanol and embedded into paraffin (Paraplast, Leica) by cutting the bone discs perpendicularly through the central defect and placing the bone discs with the cutting edge down into the paraffin mold. Finally, 5 µm histological sections were cut with a microtome (Leica RM2165).
Hematoxylin and eosin staining
Histological sections of bone discs were stained with hematoxylin and eosin (H&E). In short, histological sections were stained with hematoxylin (Delafield method) for 8 min, rinsed in running tap water for 10 min, and dehydrated through various ethanol gradients, after which they were stained with yellowish eosin (0.3% in 96% ethanol, Merck) for 2 min. Sections were then cleared in xylene (Klinipath), mounted with DPX mounting medium (Sigma-Aldrich), covered with glass coverslips, and dried overnight in a fume hood before imaging with a digital slide scanner (PANNORAMIC 1000 slide digitalization system [3DHISTECH]) and evaluated in CaseViewer (Histech).
Tartrate-resistant acid phosphate staining
For evaluation of tartrate-resistant acid phosphate (TRAP) activity as a marker for osteoclasts, 41 histological sections were deparaffinized with xylene and rehydrated in a series of ethanol and incubated with 0.2 M Tris(hydroxymethyl)aminomethane (Serva)/MgCl2 (Sigma) buffer (pH 9) at 37°C for 1 h. After a short rinse with MilliQ, sections were incubated in acid phosphate medium at 37°C for 30–120 min until control samples started to show red color. After a rinse with tap water, sections were dehydrated quickly in a graded ethanol series, cleared with xylene, mounted with DPX mounting medium, covered with glass coverslips, and dried overnight in a fume hood before imaging with a digital slide scanner and evaluated in CaseViewer. Acid phosphate medium consisted of 100 mg Napthol AS-BI phosphate (Serva) dissolved in 10 mL N,N-Dimethylformamide (Serva), to which 50 mL Veronal buffer (prepared with 1.9 g of sodium-acetate (Merck) and 2.9 g of sodium-barbiturate (Merck) dissolved in 100 mL MilliQ) was applied. Thereafter, 2 g of MgCl2 (Sigma) was dissolved in this solution, where after 16 mL pararosaniline solution (equal parts pararosaniline, prepared with 1 g pararosaniline (Merck) dissolved in 20 mL MilliQ and 12 N HCl (Merck), gently heated while stirring, cooled, and filtered) and freshly prepared 4% sodium-nitrite (Merck) were added. An additional 130 mL MilliQ and 1.52 g of potassium sodium tartrate (Boom) were added, sequentially, pH was adjusted to 5.0, and finally the solution was filtered before use.
Immunohistochemical staining
For luciferase and cytokeratin 18 (CK18) immunohistochemical staining, histological sections of bone discs were deparaffinized with xylene, and peroxidases were blocked with hydrogen peroxide (Merck). Sections were then hydrated in a graded series of ethanol and air-dried. With a liquid-repellent slide marker pen (DAKO), a circle around the mounted bone discs was drawn to limit the spreading of applied liquids. Sections were then treated with formaldehyde to ensure adequate adhesion, rinsed with PBS, and for antigen retrieval either treated with 0.075% trypsin (Fluka) at 37°C for 15 min for luciferase immunohistochemical staining and with a citrate buffer (pH 6) at 70°C for 10 min and 0.075% trypsin at 37°C for 5 min for CK18 immunohistochemical staining, and rinsed with PBS again. Subsequently, sections were preincubated with 10% normal donkey serum (NDS, Millipore) in PBS to reduce nonspecific binding. Polyclonal firefly luciferase antibody (ThermoFisher, PA5-32209, 1:400 dilution in 2% NDS) or polyclonal CK18 antibody (ThermoFisher, PA5-143130, 1:400 dilution in 2% NDS) was then incubated overnight. Thereafter, for luciferase immunohistochemical staining, sections were rinsed with PBS, incubated with the second antibody (donkey anti-rabbit with biotin, Jackson, 711-065-152, 1:500 dilution) for 1 h, followed by avidin–biotin complex (ABC, ThermoScientific) staining for 45 min. With DAP, the signal was then visualized, and sections were counterstained with hematoxylin (Mayer’s method). After rinsing, sections were mounted with DPX mounting medium, covered with glass coverslips, and dried overnight in a fume hood before imaging with a digital slide scanner and evaluation in CaseViewer. For CK18 immunohistochemical staining after the overnight incubation of the first antibody, the sections were rinsed with PBS, incubated with the second antibody (donkey anti-goat AF594, ThermoFisher, A-11058, 1:200 dilution) for 1 h, and counterstained with 4′,6-diamidino-2-phenylindole. After rinsing, sections were mounted with DPX mounting medium, covered with glass coverslips, and dried overnight in a fume hood before imaging (Zeiss Axio Imager Z2 fluorescence microscope at 10x magnification).
Statistical analyses
Data are expressed as mean ± standard deviation. Statistical analyses were performed using Prism software (GraphPad, version 10), except for the bioluminescence data of the cisplatin-treated and ex vivo cultured bone discs, which were performed in R (version 4.4.1). Ex vivo bone metastasis progression data of metabolic activity, bioluminescence intensity, and MMP-9 concentration were statistically analyzed with independent Student’s t tests at each time point comparing bone-only with bone metastasis discs. Metabolic activity data on the therapeutic efficacy of cisplatin exposure to ex vivo bone discs were statistically analyzed with a two-way analysis of variance (ANOVA), followed by a Tukey posthoc multiple comparisons test. Bioluminescence intensity data on therapeutic efficacy of cisplatin exposure were grouped (days 0–1 and days 4–14) and analyzed by a multilevel regression model that accounted for the clustering of measurements in 12 bone metastasis discs. In this model, time (in two groups: days 0–1 and days 4–14) and treatment (4 sizes, with 0 µm as reference group) were the independent variables. From this regression model, 95% confidence intervals were presented. Pooled bioluminescence intensity data of bone discs of cisplatin- or placebo-treated mice were statistically analyzed with an independent Student’s t test between placebo- and cisplatin-treated groups. For all statistical analyses, a p value of <0.05 was considered significant.
Results and Discussion
Initial assessment of bone discs
Bone discs with a central defect were prepared from discarded human femoral heads following total hip replacement surgery. Immediately after drilling procedures, debris visible to the naked eye was not detected (Fig. 2A). The central defect functioned as a mini-well, applicable for metastatic cancer cell seeding in higher seeding numbers than used previously in ex vivo human bone cultures.22,34,36,37,42 Even though prostate cancer cells were seeded into the defect, most bioluminescence signals originating from luciferase-expressing prostate cancer cells were observed across the entire top surface of the bone discs 24 h after cell seeding (Fig. 2B), showing substantial variation in cell spreading (data now shown). Histological assessment of these initial bone discs showed empty central defects for bone-only discs (Fig. 2C) and the presence of rounded and loosely connected prostate cancer metastatic cancer cells in the defect for bone metastasis discs (Fig. 2D, red inset). Bone debris was observed at the base of the central defect and along the peripheral edges in both types of discs, attributable to the drilling procedure. Furthermore, bone discs had an apparent healthy bone morphology, in line with bone morphology of aging patients,43–45 showing bone trabeculae where most lacunae were filled with nucleated osteocytes and adipose-rich bone marrow (Fig. 2D, green inset).

Initial histological appearance of cancer cells in bone discs after 24 h ex vivo culture.
Determination of bone viability and tracking prostate cancer metastatic lesion progression during ex vivo bone disc culture
A general consensus of best practice to evaluate bone health and metastatic cancer progression in ex vivo cultured bone explants combined with cancer cells has not yet been reached, due to the sparse amount of current literature focused on this type of bone metastasis model.34,36–39 Thus, various methods to determine bone viability and track metastatic lesion progression over a 2-week culture period were explored and assessed for suitability herein. Cancer-cell-free bone-only discs and bone metastasis discs (seeded with PC3_LUC cells) were cultured for 2 weeks, based on previously reported time periods for statically cultured viable bone tissue. 46 First, a noninvasive AlamarBlue assay was explored to determine gross metabolic activity. Remarkably, absolute metabolic activity values on day −3 showed no significant difference between the bone-only and bone metastasis discs (Fig. 3A), despite the seeding of 0.25 million metastatic cancer cells. Over time, relative metabolic activity values remained comparable between bone-only and bone metastasis discs (p > 0.05). At day 14, average relative metabolic activity values of bone discs remained at ∼218%, indicating metabolically active bone for the entire culture period. Given the similarity in metabolic activity read-outs for bone-only and bone metastasis discs, these results led to the conclusion that relative metabolic activity values are not suitable for tracking metastatic lesion progression but are useful for measuring overall metabolic activity of ex vivo cultured bone discs to confirm the viability of the bone discs.

Assessment of ex vivo bone metastasis progression.
Secondly, noninvasive bioluminescence signals were recorded over time. The bioluminescence signal consistently originated from the top of the bone disc, and not from the interior of the central defect (Fig. 3C) into which metastatic cancer cells were seeded. Quantified bioluminescence intensities showed abundant bioluminescence intensity for bone metastasis discs versus negligible intensity for bone-only on day −3 (Fig. 3D; p < 0.0001). This outcome was as expected as only the metastatic cancer cells expressed luciferase for catalyzing the conversion of luciferin into the light-emitting oxyluciferin. During the 2-week ex vivo culture period, bone-only discs showed a negligible bioluminescence intensities, while bone metastasis discs showed an initial increase at day 1, followed by a decrease thereafter until day 14 (Fig. 3E). This decrease over time suggests a decrease in the number of metastatic cancer cells but could also be caused by cancer cells penetrating into the marrow compartment of the bone discs. Importantly, a total loss of bioluminescence signal was observed when bone metastasis discs were flipped prior to recording (Supplementary Fig. S1A, B). In this case, the bioluminescence signal needs to pass through the entire bone disc, and due to the anisotropic and complex composition of cancellous bone, the signal is easily scattered. 47 This could cause a reduction in bioluminescence intensity, thereby limiting the reliability of tracking metastatic lesion progression. Nevertheless, measuring relative bioluminescence intensities could be a suitable method to determine metastatic cancer cell quantities during ex vivo culture, as this method is noninvasive, allowing multiple measurements over time, which contrasts earlier studies only confirming presence of cancer cells on a single time point during culture.34,37
Thirdly, MMP-9 concentrations in supernatant were measured as a biomarker for metastatic cancer cell activity.34,48–53 Remarkably, MMP-9 concentrations on day 0 were significantly higher for bone-only discs compared with bone metastasis discs (Fig. 3F; p < 0.05). A possible explanation for this result might be the interference of intrinsic MMP-9 secretion by cells present within the bone disc (e.g., from the bone or marrow compartment)54,55 or a delay in osteolytic activity of metastatic cancer cells seeded into the bone disc. During prolonged ex vivo culture, bone-only and bone metastasis discs showed similar relative concentrations of MMP-9 secreted into the culture medium (Fig. 3G). Due to the absence of sustained differences in MMP-9 levels between bone-only and bone metastasis discs over time, MMP-9 quantification was not considered a reliable indicator of metastatic lesion progression in this ex vivo model.
Lastly, to evaluate bone morphology, bone cellular characteristics, and localize cancer cells, bone discs were destructively analyzed using histology. To this end, bone-only discs (Fig. 4A) and bone metastasis discs (Fig. 4B) were fixated at the end of the 2-week ex vivo culture period, decalcified, paraffin-embedded, sectioned, and stained with H&E. Cross-sections of the bone discs made perpendicularly through the central defect (Fig. 4A, B, top left image) showed the presence of remaining bone debris in the central defect for both the bone-only and bone metastasis discs. Osteocytes and bone marrow were still present after 2 weeks (Fig. 4A, B, green inset), similar to previously reported results of ex vivo human or animal bone cultures.38,39,46,56–59 Osteoclast presence was not investigated, as the rapid reduction of osteoclastic activity in ex vivo human bone cultures was recently reported. 59 In bone metastasis discs, loosely connected cells with a spherical morphology were still present in the central defect (Fig. 4B, left red inset), which were confirmed to be metastatic cancer cells by positive luciferase immunohistochemical staining (Fig. 4B; right red inset). Quantification of this luciferase-positive staining was hampered by false-positive staining of the edges of bone trabeculae. Compared with the initial presence of metastatic cancer cells (Fig. 2D), an apparent decrease in metastatic cancer cells was observed after 2 weeks of ex vivo culture (Fig. 4B), suggesting that metastatic cancer cells were lost during prolonged ex vivo culture. This decrease may be attributed to cell death, migration out of the bone disc, or technical issues related to procedure of histological processing (e.g., too loose connection with the bone disc; Supplementary Fig. S1C). While the initial bone metastasis discs histologically showed presence of metastatic cancer cells on top of the bone discs (Supplementary Fig. S1D), corroborating bioluminescence signal recordings at the same moment, no luciferase-positive immunohistochemical staining was observed on top of the bone metastasis discs after 2 weeks of ex vivo culture (data not shown). Lastly, no signs of metastatic cancer cell invasion into the bone marrow compartment were observed, which contrasts the clinical manifestation of bone metastasis.60,61 Histological assessments allowed for a more thorough qualitative analysis of the bone discs but appears insufficiently reliable as luciferase-positive staining did not correspond to bioluminescence signal localization, and false-positive staining hampered quantification of metastatic lesion areas.

Histological analysis of ex vivo cultured bone discs. After 14 days of ex vivo culture, bone-only discs
Ex vivo bone metastasis model demonstrates limited sensitivity to cisplatin treatment
During ex vivo culture, bone-only and bone metastasis discs (seeded with PC3_LUC cells) were exposed to various concentrations (0–100 µM) of the model chemotherapeutic drug cisplatin4,40 for a 24-h treatment period. Effects of cisplatin exposure were assessed with relative metabolic activity values, bioluminescence intensity measurements, and (immuno)histological evaluations. At day 14, a cisplatin dose-dependent decrease in relative metabolic activity was observed for both bone-only discs and bone metastasis discs (Fig. 5A), suggesting effects of cisplatin on the viability of metastatic cancer cells as well as cells intrinsically present within the bone and marrow compartments of the bone discs. Remarkably, relative metabolic activity values did not drop down below ∼62% for the bone metastasis discs treated with 100 µM cisplatin, demonstrating a lower susceptibility to cisplatin than 2D cocultures of bone metastatic cancer cells combined with human bone marrow stromal cells, as these cultures were previously shown to be completely eradicated at this concentration of cisplatin. 62
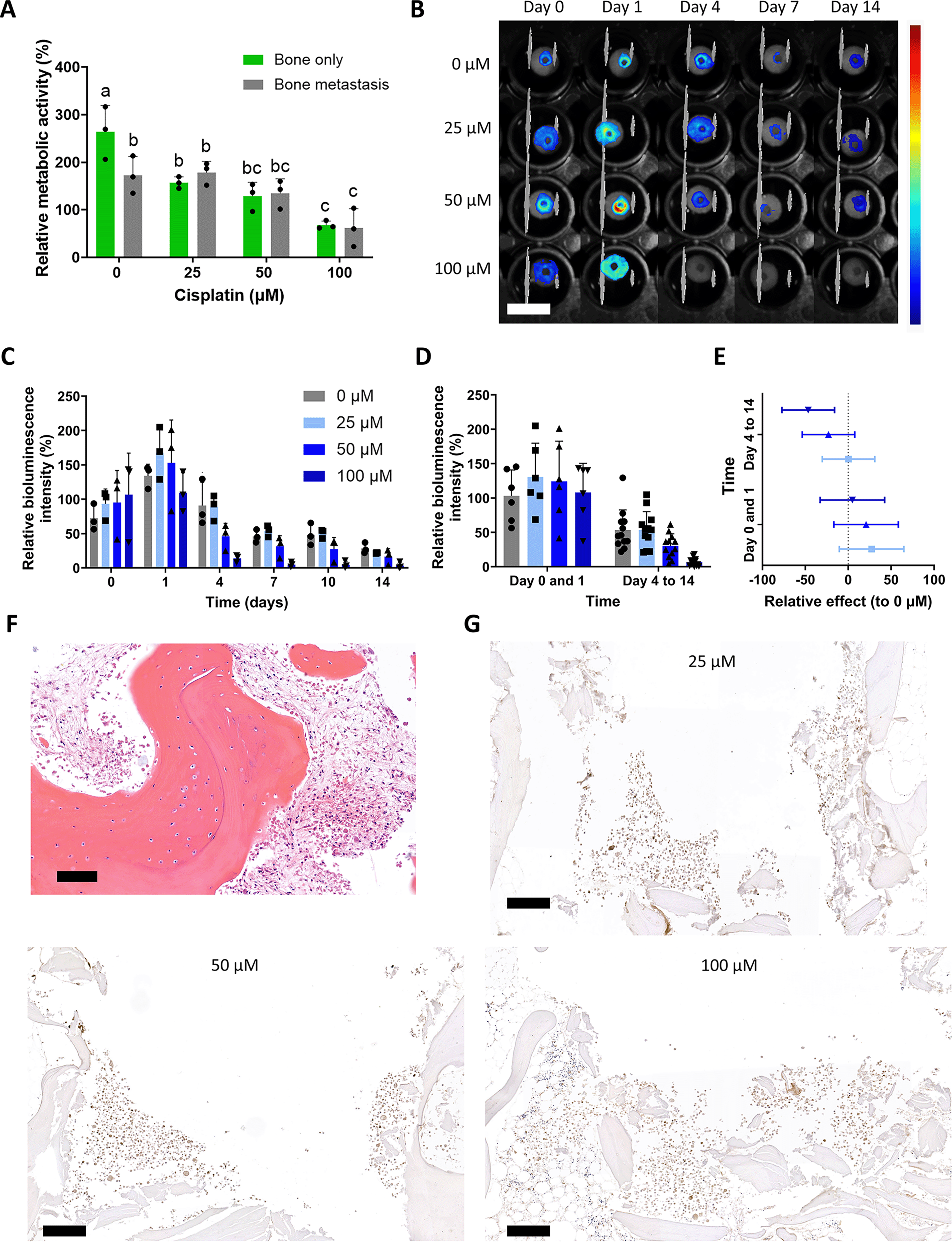
Therapeutic efficacy of cisplatin supplementation to ex vivo bone disc cultures.
Relative bioluminescence intensities showed a dose- and time-dependent decrease in response to cisplatin exposure (Fig. 5B&C). Using pooled data (days 0–1, and days 4–14; Fig. 5D) to strengthen statistical power, we performed a multilevel regression model with time and cisplatin as the two independent variables, and 0 µM as control group. From this, the 95% confidence intervals showed a significant effect for the 100 µM cisplatin-treated samples for days 4–14 (Fig. 5E). This observed anticancer effect for only this high cisplatin concentration is in line with previous literature on ex vivo cultured human bone with cancer cells treated with chemotherapeutics. 37
Remarkably, the cellular characteristics of the bone showed no apparent alterations upon exposure to 100 µM of cisplatin (Fig. 5F) based on similarities in osteocytes and bone marrow cellularity compared with untreated bone-only discs. Lastly, immunohistochemical staining of luciferase showed qualitatively similar numbers of cancer cells in central defects for all concentrations of cisplatin (Fig. 5G), which was comparable with the cancer cell presence in untreated controls (Fig. 4B).
In general, culturing human bone discs seeded with metastatic cancer cells ex vivo appears to have potential as a bone metastasis model, but numerous improvements should still be implemented to enhance their clinical relevance. For example, the current characterizations yielded inconsistent results, and no clear dose-dependent differences in the anticancer efficacy of cisplatin were observed. Possibly, the robustness of the model can be improved by (i) increasing the number of replicates 63 ; (ii) further fine-tuning of the various analytical techniques used, for example, by optimizing AlamarBlue or luciferin working solution incubation times; or (iii) improving immunochemical staining procedures. Moreover, the ex vivo culture of human bone discs might be improved by optimizing culture conditions. For example, the inclusion of FBS in culture media for ex vivo culture of bone is debated, as FBS could potentially disrupt the streaming potentials in the lacuna-canalicular network, 35 but FBS has also been reported to be essential for maintaining bone cell viability. 38 Furthermore, we decided to culture bone discs without osteogenic supplements, as this procedure was shown to negatively affect osteocytes.64,65 Conversely, these osteogenic supplements might be favorable for osteoblasts. However, no consensus exists to date on the optimal culture medium composition, which necessitates further research on this aspect. 35 Furthermore, mechanical stimulation is frequently applied for ex vivo bone cultures to trigger appropriate osteocyte function,46,66 which is claimed to be essential for new bone formation. 66 Mechanical stimulation has also been associated with increased bone mineral density, 57 more pronounced anisotropic microstructures, 67 and increased osteoblast activity. 58 In addition, effective perfusion of the whole bone tissue can be achieved by implementing fluid flow, which could lead to prolongation of successful culture periods, as it could improve nutrient delivery and waste removal.35,68 Despite a potential role of immune cells in the bone metastasis cascade, 69 adding immune cells to this ex vivo model would be complicated; importantly, the bone marrow compartment already contains a large variation of immune cells (i.e., both from the innate and adaptive immune system). Lastly, culturing the bone tissue under low-oxygen (hypoxic) conditions could be considered, as this resembles the bone and cancer microenvironment more closely.38,70 All these factors could potentially contribute to the quality of the bone metastasis ex vivo model but would require more technical setups and knowledge, hence decreasing model feasibility.
Subcutaneous implantation of bone discs results in integration with the host and preservation of bone morphology and viability
In vivo subcutaneous implantation of viable bovine bone tissue was recently shown to maintain tissue viability, as it became integrated via anastomosis (i.e., connection with the host vasculature). 21 Consequently, we subcutaneously implanted human bone-only discs and bone metastasis discs (here with PC3 or MDA-MB-231 cancer cells) into immunodeficient mice. To this end, a single cutaneous incision was made, after which four subcutaneous pockets were created dorsally via blunt dissection in which bone discs were placed (Supplementary Fig. S2A). During the entire implantation period of 3 or 6 weeks, bone discs remained at the site of implantation (Supplementary Fig. S2B), and animals increased in weight (Supplementary Fig. S2C) without showing major adverse effects.
Histological analyses were performed at week 3 (Fig. 6) and week 6 (Fig. 7) to determine bone viability. Bone-only discs (Figs. 6A and 7A), bone metastasis discs with breast cancer cells (Figs. 6B and 7B), and bone metastasis discs with prostate cancer cells (Figs. 6C and 7C) all showed large variations in bone density, bone debris at the bottom of the central defect and occasionally at the edges of the disc, and the presence of mice skin on top of the discs (indicated with black arrows). In Figures 6 and 7, the green insets show the presence of nucleated osteocytes, high cellularity of bone marrow, and blood vessels of various sized diameters in various locations within the bone discs filled with erythrocytes (indicated with black arrow heads), which corroborates earlier work.22,23,25,26,28,32,34,71 Occasionally, osteoblasts (indicated with blue arrow heads) were observed lining the trabeculae, suggesting bone formation, confirming earlier work.22,24,34 Furthermore, TRAP staining demonstrated the presence of localized osteoclastic activity at week 3 (Supplementary Fig. S3B) and week 6 (Supplementary Fig. S3C), which seemed to colocalize with the bone debris at the edges of the bone discs and at the bottom of the bone defect. Remarkably, TRAP staining was not observed in the bone discs prior to implantation (Supplementary Fig. S3A). This discrepancy suggests that osteoclasts arise from the host24,72 and position themselves in the vicinity of bone debris. Relevant bony cell types and erythrocyte-filled blood vessels were found in all subcutaneously implanted bone discs, independent of the type of cancer cell seeded, suggesting viable and well-integrated bone disc implants.
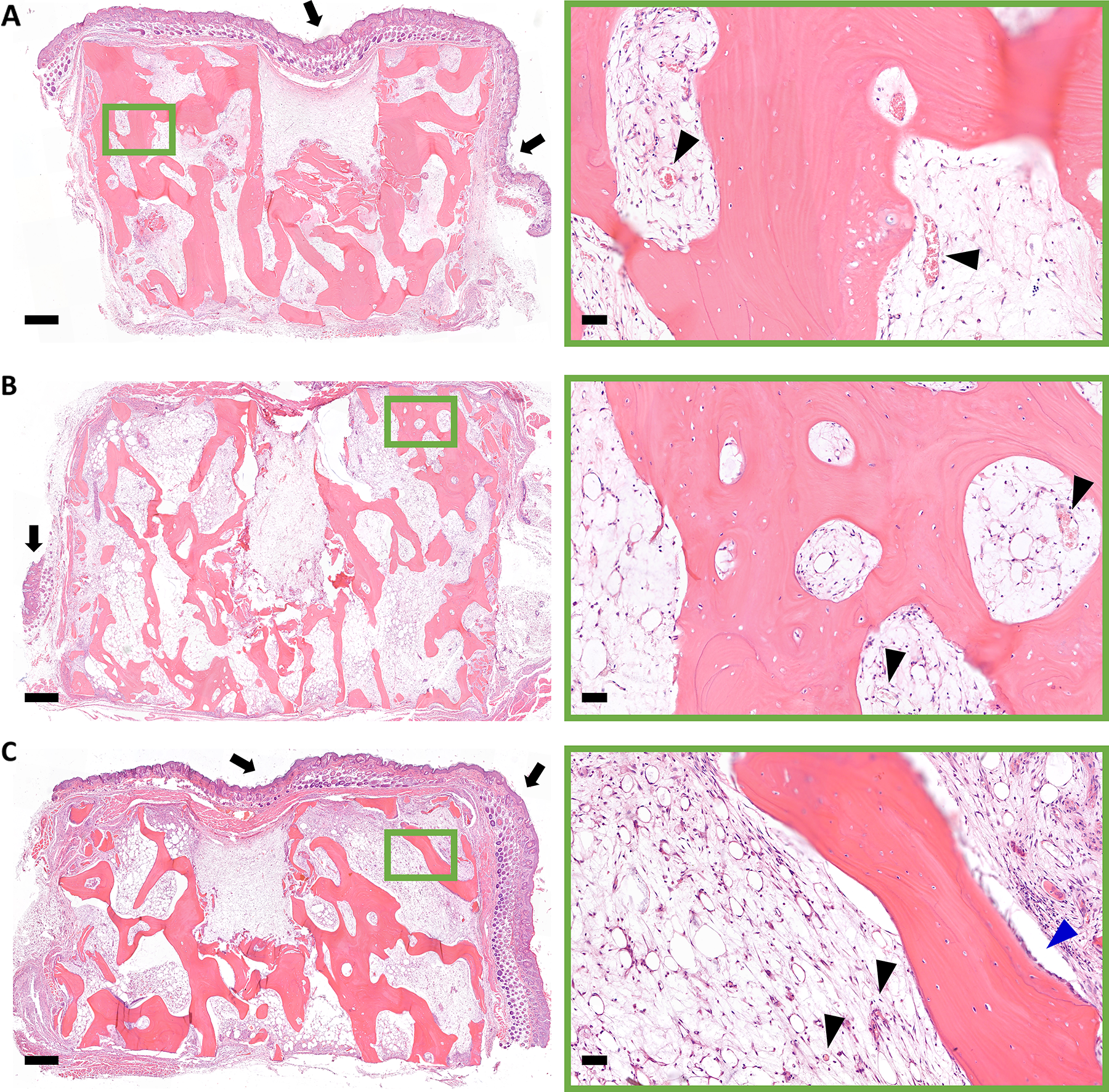
Histological appearance of bone discs retrieved after 3 weeks of subcutaneous implantation in nude mice. Overview images of bone-only
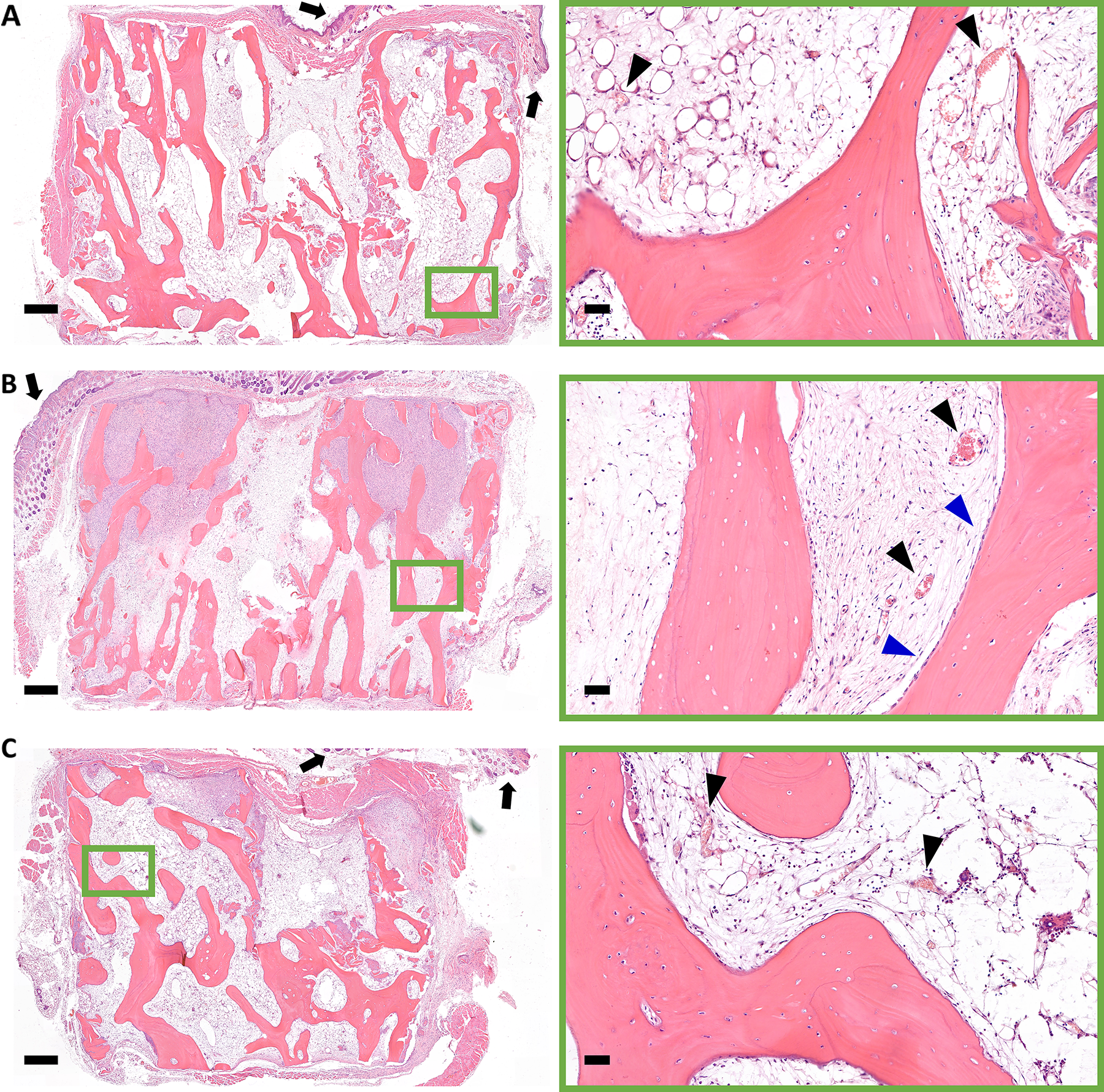
Histological appearance of bone discs retrieved after 6 weeks of subcutaneous implantation in nude mice. Overview images of bone-only
Formation of osteolytic bone metastatic lesions in subcutaneously implanted human bone
To investigate the presence of bone metastatic lesions, we next attempted to identify cancer cells using (immuno)histochemistry. Other tissues of the nude mice were not scrutinized for the presence of metastasis, as it was previously shown that models of forced metastasis or via intraosseous injection of either PC3 or MDA-MB-231 cells did not show metastasis to other organs.22,24,25,33,34 We first focused on the central defect (indicated with an asterisk) to find cancer cells, since this was the original site where cancer cells were seeded. Surprisingly, we did not find any cancer cells located within this defect region. Instead, we observed areas of high cellularity with large and irregular nuclei in the intertrabecular spaces near the top of discs next to the central defects (Fig. 8A&C, indicated with black arrows). These areas of high cellularity were identified as cancer cells invading the bone marrow, similar to other cancer cells in the bone microenvironment in earlier preclinical and clinical studies.24,25,28,30,32,33,60,61,73 For breast cancer bone metastasis discs retrieved at week 3, such tumor stroma were not observed, but at week 6, the tumor stroma occupied a large portion of the intertrabecular space in 4/4 bone metastasis discs (Fig. 8A). This metastatic lesion take rate of 100% is higher than the 80% previously reported for bone implanted subcutaneously together with MDA-MB-231 cells. 34 Interestingly, TRAP activity was predominantly observed near the trabeculae surrounded by the tumor stroma (Fig. 8B), suggesting an osteolytic lesion similar to previous work reporting on breast cancer cells invading (engineered constructs of) bone.23,24,29,74 For prostate cancer bone metastasis discs, small tumor stroma areas were detected for 2/4 bone metastasis discs retrieved at week 3, and slightly larger tumor stroma areas for 3/4 bone metastasis discs retrieved at week 6 (Fig. 8C), resulting in a metastatic lesion take rate of 75%. Using CK18 immunohistochemistry, we confirmed that PC3 cells constituted these tumor stroma areas, as CK18 is a cancer marker for cancers with epithelial origin26,29,38,75 suitable for application in the bone microenvironment25,76 and successfully used previously to identify PC3 cells. 71 Similar to bone metastasis discs with breast cancer cells, high levels of TRAP activity were observed in the vicinity of trabeculae surrounded by these tumor stroma areas, suggesting an osteolytic type of metastatic lesion. This is in line with previous reports of PC3 invading (engineered constructs of) bone.25,27,33,71,77,78 Consequently, our bone metastasis model with subcutaneous implantation of human bone demonstrates potential as a relevant in vivo bone metastasis model, as it presents i) a high metastatic lesion take rate for both cancer cell types, ii) cancer cell invasion into the intertrabecular space similar to clinical results,60,61 and iii) osteolytic activity similar to various clinical cases of bone metastasis for patients suffering from breast or prostate cancer. 79

Bone metastasis progression in bone metastasis discs subcutaneously implanted in nude mice.
Clinically, osteolytic lesions are determined by X-ray or CT scans. 1 As such, we used µCT imaging for preliminary investigations, scanning one bone disc per experimental group (Supplementary Fig. S4). However, substantial variability in bone density, which was also evident in the histological sections, limited the utility of µCT in this context and precluded further qualitative or quantitative assessments. If bone density would have varied less between the various samples and if a larger sample number was investigated, then a more in-depth analysis could have possibly been made. 68 It further needs to be emphasized that the priority for this work was to establish metastatic lesions in the human bone, for which it has been postulated that osteoporotic bone is likely more susceptible.80,81
Bioluminescence enables tracking of metastatic lesion progression and treatment effects
By exposing the central defect in the bone metastasis discs to the skin side, we were able to utilize bioluminescence for tracking cancer cells in prostate cancer bone metastasis discs (using PC3_LUC cells) to monitor and quantify metastatic lesion progression or effects of systemic cisplatin treatment during experimental procedures. To this end, prostate cancer bone metastasis discs were subcutaneously implanted into 4 mice and left for acclimatization for 1 week, when bioluminescence intensity was measured as the starting point. Thereafter, mice were randomized into either the control (placebo i.v. injection; 2 mice with each 4 bone metastasis discs) or systemic cisplatin treatment (cisplatin i.v. injection; 2 mice with each 4 bone metastasis discs) group. Bioluminescence intensities were measured once per week until sacrifice at week 5, after which bone discs were retrieved and histologically processed.
Recordings of bioluminescence intensity showed apparent signal from predominantly the central region of the bone metastasis discs (Fig. 9A). Repetitive recordings of bioluminescence intensity over the 5-week implantation period showed relative constant and similar intensities for both groups (Fig. 9B). Pooling the data from all time points did not reveal a significant difference between cisplatin-treated and control groups (Fig. 9C).

Cisplatin administration and bioluminescent monitoring of prostate cancer bone metastasis discs implanted subcutaneously in nude mice.
Bioluminescent intensities for the control bone metastasis discs did not increase, which might be explained by a lack of cancer cell growth as observed using histological evaluations after 5 weeks of implantation in in vivo experiment #2 as compared with in vivo experiment #1. Here, cancer cells could only be observed in 3/8 (37.5%) control bone metastasis discs and 2/8 (25%) cisplatin-treated bone metastasis discs, and tumor stroma invading the intertrabecular space (indicated with black arrows) were much smaller (Fig. 9D; control bone metastasis disc corresponding with the ∼220% bioluminescent intensity data point at week 5) as observed in experiment #1 (Fig. 8C). Bioluminescent intensities might have been higher if lesions in experiment #2 had reached similar dimensions as in experiment #1.
As each animal experiment was performed with bone discs from a different donor, the interexperiment variability, such as the varying bone density 82 and age, might have caused the inconsistencies in metastatic lesion progression. Thus, the results as observed here should be confirmed with future experiments with bone from similar human donors, especially because the sample size in this study is relatively small. For these future experiments, other factors could also be included in the study design. For example, osteoporotic bone is generally considered a more favorable environment for cancer cells, 39 as well as female-associated hormones in the bone microenvironment. 83 To improve this study aspect, the choice of human donors could be standardized to a larger extent, for example, by requesting more information from the donors, which however was not allowed using the current ethical approval. To circumvent donor variability, other researchers have explored tissue-engineered bone constructs,77,78,84 which however required longer experimentation times to grow bone and addition of various other components (e.g., cells and growth factors), which decreased the practical feasibility of the model. Therefore, more research is needed to find a balance between interexperiment variability and feasibility of implanting human bone subcutaneously into immunodeficient mice for modeling bone metastasis.
In addition, it would be of interest to explore the preparation of bone metastasis discs with other cancer cell types. For example, lung cancer cells as this cancer type is the most prevalent to cause bone metastasis after breast and prostate cancer. 85 Furthermore, the model opens up opportunities for personal medicine as cancer cells from patient biopsies can potentially be used for preparing bone metastasis discs. 86
Conclusion
Human bone discs seeded with metastatic cancer cells were either cultured ex vivo or implanted subcutaneously in immunodeficient mice. Ex vivo culture of bone metastasis discs demonstrated the viability of cells in bone for up to 2 weeks, but cancer cell presence decreased over time as observed using bioluminescent intensity measurements as well as with histological evaluations. In contrast, subcutaneous implantation of bone metastasis discs demonstrated (i) bone viability, (ii) integration via connection to the host vasculature, and (iii) progressive growth of osteolytic lesions similar to clinical bone metastasis. However, both methods require further research to render the model more clinically relevant and reliable, especially an increase in sample size is needed to make these proof-of-concept results more robust. If such progress can be achieved in the future, ex vivo culture and in vivo implantation of bone metastasis discs hold strong potential for evaluation of novel treatment options to accelerate their potential clinical use for bone metastasis patients.
Authors’ Contributions
C.-A.E.S., M.D., S.C.G.L., and J.J.J.P.v.d.B. contributed to the conception and design of the study. C.-A.E.S. and J.J.J.P.v.d.B. performed experiments, collected and analyzed data, and drafted the manuscript. R.v.R., N.W.M.v.D., and V.M.J.I.C. contributed to experimental work, data acquisition, and technical support. E.M.B. contributed to statistical analysis and data interpretation. M.D., S.C.G.L., and J.J.J.P.v.d.B. contributed to data interpretation and critical revision of the manuscript. J.J.J.P.v.d.B. conceived and supervised the study. All authors reviewed and approved the final manuscript.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Nederlandse Organisatie voor Wetenschappelijk Onderzoek (NWO) under project number 17835.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.