
Abstract
This review evaluated transdisciplinary empirical research on wearable health technologies using the input-mechanism-output model and addressed a major concern relating to the invasiveness of wearables. The dataset consisted of 250 published papers that investigated wearables for health-related purposes. Papers focused on technological inputs and health output factors, de-emphasizing theoretical mechanisms that could effectively translate the former into the latter. The lack of transdisciplinary research in the field is limiting both identification of effectiveness and evidence of beneficial health outcomes, with a considerable divide between technologists and public health researchers. Privacy concerns relate to increasing trends in collecting data for mental health and physical health, with the latter escalating exponentially. Invasiveness of wearables has increased over time in terms of collected signals and the derived health information, monitoring both users and their social and physical environments. We conclude with reflections for conceptual development, commercial application and policy regulation.
Introduction
Wearable technologies are poised to surge ahead in popularity due to a combination of innovativeness and functionality, particularly in the continuous monitoring of health-related parameters (Casselman et al., 2017). We define wearable health technologies as body-attached or body-implanted smart devices capable of tracking physiological signals for health-related purposes. These mobile health (mHealth) wearable devices promise support for elderly care, chronic disease management, clinical decision-making, as well as promotion of healthy and energetic lifestyles (Dunn et al., 2018). Living up to their potential will likely result in the radical transformation of certain healthcare areas, particularly coinciding with the rise of self-care.
The burden of care is being transferred onto patients as a result of demographic and environmental trends such as aging populations in developed countries due to increased life expectancies (Crimmins & Zhang, 2019), the burgeoning of youth populations in the Global South facing an inadequate health infrastructure (Fatusi & Hindin, 2010), the onset of lifestyle diseases with global urbanization (Goryakin et al., 2017), and health issues emerging from the onset of climate change (Austin et al., 2019). Coupled with an emphasis on pre-emptive lifestyle modifications, wearable health technologies, as part of a broader mHealth array including mobile apps (Chib & Lin, 2018), will enable self-care among individuals.
However, despite the increasing trend of nudging individuals toward self-care, mHealth apps have failed to provide patients with adequate empowerment features (Brew-Sam & Chib, 2019). Similarly, the evidence of wearables as a positive tool for health promotion remains inconclusive, impeding the realization of potential benefits. The purpose of this review is to evaluate the existing literature on health-related wearables, with the aim to inform future research and policy.
Literature review
Definition of wearable health technologies
The term “wearables” has acquired a particular connotation in the contemporary digital world. A widely used definition proposed by Wright and Keith (2014) delineates wearable technologies as “electronics and computers that are integrated into clothing and other accessories that can be worn comfortably on the body.” Wearables, however, no longer merely signify items that can be worn on the body, but are also associated with implanted smart devices (Sandvik, 2020) and the capability to communicate autonomously and process information on the go (Park et al., 2014). While the health-related functions of wearables are increasingly being recognized, the formal definition of wearable health technologies is yet to be established.
We adopt a broad view of wearable health technologies, summarizing three main features: being attached to or implanted within the body of the user (Sandvik, 2020); providing a continuous way of gathering physiological signals requiring none or little interaction from the user (Rodríguez et al., 2017); aiding beneficiaries for tracking and protecting health (Sandvik, 2020). These features of wearable health technologies (henceforth wearables, noting definition) are used as criteria to establish boundaries for the current review, and also to distinguish them from other technologies, such as mobile phone applications (Brew-Sam, 2020) and assisted living technologies (Blackman et al., 2016).
Empirical research on wearables has gained traction as these devices become popular. Recent reviews analyzed studies focused on their development (De Zambotti et al., 2019; King et al., 2017), their effectiveness in health interventions (Brickwood et al., 2019; Chang et al., 2018), and their ability to assess or predict health conditions (Burnham et al., 2018; Elgendi & Menon, 2019). Among extant reviews, there is more focus on the development of wearable technology and the accompanying health outcomes, but a considerable gap lies in theoretical explanations of human behavior regarding wearables.
Transdisciplinary integration of wearables research remains a challenge, one which we intend to address through synthesizing the existing knowledge of the development, use, and effectiveness of wearables across disciplines.
Transdisciplinary framework: inputs, mechanisms, outputs
The input-mechanism-output (I-M-O) framework (Chib et al., 2015) can be used to synthesize transdisciplinary contributions to wearables research. The existing literature on wearables comes from many disciplines—specifically, engineering, social science, and health science (Williams et al., 2020). Numerous papers stem from engineering science, with focus on technological development of wearable devices and related algorithms (King et al., 2017); we term these as input features. Studies in public health and medical science investigate wearables as a tool for health promotion (Gordt et al., 2018), both for individuals and healthcare institutions; we identify these as outputs. Social science research links these disparate disciplines by investigating human adoption and usage behavior in using wearables to improve health outcomes (Schueller et al., 2017), in other words, the mechanisms that explain the relationship between technological inputs and health outputs. However, multidisciplinary integration in research of wearables across these three main domains remains a challenge (Williams et al., 2020). This is a gap that the I-M-O model can fill, as it encompasses the major disciplines across both hard and soft sciences.
The I-M-O model has been used to organize the state of research on other health technologies. In particular, scholars have found application of the I-M-O model useful for categorizing previous studies and outlining research gaps (Brew-Sam, 2020), and for highlighting the lack of scope and coverage in extant literature (Hoque & Sorwar, 2017). Similarly, social scientists have attempted to connect technological designers’ perspectives with users’ perspectives, adoption motivations, and eventual behavior (Huang & Ren, 2020), suggesting greater cohesiveness and explanatory power through such means.
In context of this review, inputs refer to the design features of wearable devices, such as technological design, user engagement strategies in design, and user acceptance factors that guide design. These include, for example, factors such as battery life, design appeal, or technical functionality (Maher et al., 2017; Rosales et al., 2017)
Mechanisms refer to the theoretical explanations applied to understanding human factors in related contexts, specifically how and why people adopt wearables, understanding their usage patterns, and how wearables can drive attitudinal and behavioral changes. For example, the Technology Acceptance Model has been applied to understand adoption and usage patterns of wearables (Niknejad et al., 2020). A meta-analysis by Prestwich et al. (2014) of 190 health behavior interventions reported that the Health Belief Model, Social Cognitive Theory, Theory of Planned Behavior, and the Transtheoretical Model were among the common theories applied in health behavior interventions. However, only 56% of the reviewed studies reported using a theoretical frame, and amongst these papers, the majority bore weak associations between the reported theory and the outcomes of the interventions (Prestwich et al., 2014). Of particular significance for this review, mHealth research has been found lacking in the application of communication theories to improve user engagement and persuasiveness of interventions (Vandelanotte et al., 2016). This review fills the gap in the current assessment of the use of theory in wearables research.
Outputs refer to the outcomes arising from the usage of wearables, such as the effects of wearables on individual health in terms of behavioral and physiological measures and the improved efficiency of healthcare organizations. This would include factors such as changes in individuals’ physical activity or BMI (Pourzanjani et al., 2016; Shuger et al., 2011), or changes in the way organizations collect electronic health records (Dinh-Le et al., 2019). Refer to Figure 1 for an outline of the I-M-O framework applied in this review.

I-M-O framework for review of health-related wearables.
The I-M-O model thus maps interdisciplinary fields and the roles each discipline plays, from engineers to social scientists to public health researchers. Social scientists can play an important linking role in the integration of this transdisciplinary field, contributing insights on psycho-social mechanisms of human behavior based on theory. For a holistic overview of current research on wearables, and the role that social scientists can play in advancing knowledge on wearable health, we pose our first research question.
RQ 1: What is the status of current empirical research on health-related wearables in terms of (a) technological development (input factors), (b) the mechanisms of adoption and usage, and (c) impact and effectiveness (output factors)?
Increasing invasiveness of wearable health technologies
As the integration of sensors renders wearables increasingly sophisticated (Businesswire, 2020), privacy challenges are the most frequently mentioned issues in the wearable technology industry (World Economic Forum, 2020). Rapidly advancing technological development of wearables allows providers to create a more personalized experience (Kemper, 2019). However, as extremely detailed and highly personal (medical) information is being collected, consumers are worried about the vendor’s potential opportunistic behaviors relating to their private information (Banerjee et al., 2018). Technology providers that fail to balance the personalization–privacy paradox risk alienating customers in their efforts.
Besides industry concerns, the importance of privacy issues has also been addressed in academic literature. Empirical evidence shows that privacy concerns have a negative impact on consumers’ use of wearables (Marakhimov & Joo, 2017). Invasiveness, as a characteristic of information technology perceived by users, refers to the potential for privacy invasion posed by the manner in which personal health data is gathered, processed, and used (Paschal et al., 2009). A study on people with diabetes suggested that invasiveness is a barrier to self-monitoring (Wagner et al., 2005).
Privacy concerns in both commercial and academic domains require an investigation of the invasiveness of wearables. From the perspective of the I-M-O framework, consumers’ privacy concern as a predictor of users’ adoption of wearables (Mechanism) is impacted by invasiveness as a technology design issue (Input). It is important to explore whether the research on invasiveness has responded to privacy concerns. Thus, we pose our second research question.
RQ 2: How has research on the invasiveness of wearables evolved in response to consumers’ privacy concerns?
Method
This review analyzed research papers investigating wearable technologies for health-related purposes. The intent was to provide a systematic update of developments within this emergent mHealth subfield, and not to present an exhaustive summary of all studies involving wearables. We chose Web of Science (SSCI) and PsycINFO as the literature databases. These two databases were most frequently used for reviews in communication research (Borg et al., 2019).
The process of data extraction and analysis was adapted from the Cochrane collaboration systematic review methodology (Higgins & Thomas, 2019), which includes defining the research question, developing inclusion and exclusion criteria, conducting high sensitivity search, using a standardized form for data extraction, and considering meta-analysis when appropriate, else presenting a narrative assessment. This paper follows a similar process as Cochrane reviews, with two notable distinctions.
First, unlike Cochrane reviews that focus on a narrow research question, this review addresses a broader topic of wearables research across multiple disciplines. Although this approach does sacrifice depth for breadth, researchers and practitioners frequently express a need for a broad overview to identify areas of interest and specify how their work complements the greater body of wearables research.
Second, Cochrane reviews adopt a strict methodology for quantitative evaluation of studies, recommending that data selection and extraction be carried out by two coders independently. However, this review emphasizes a descriptive analysis of the literature, so we employed a simplified version of the Cochrane methodology. Specifically, one co-author first conducted literature selection and coding, and any problems encountered were forwarded to two other co-authors. To guide this study effectively, we derived explicit criteria from our previous work (Chib & Lin, 2018; Chib et al., 2015) on mHealth reviews. In order to avoid bias and error, the selected material was checked by a second co-author, similar to methods applied by Zhang, Calabrese et al. (2018).
Selection of dataset
All authors agreed on the research questions and search keywords, meeting at each stage to make decisions on inclusion/exclusion criteria. We used a combination of Medical Subject Headings (MeSH) and selected free terms for scientific publications of health-related wearables. Fuzzy matching queries applied in Web of Science and PsycINFO on 27 August 2019 were (wearable* OR fitness tracker* (MeSH) OR activity tracker* (MeSH)) AND (health* (MeSH)). Search results across databases were combined into 1056 papers. Precise criteria were applied to this initial dataset acquisition.
Inclusion criteria required peer-reviewed journal articles to be written in English language, have available full texts, and comprise original empirical evidence of wearable technologies. Duplicates (n = 47), incomplete records (n = 46), book sections (n = 9) and dissertations (n = 4) were excluded, bringing the total down to 950. Next, screening of titles, keywords and abstracts led to the removal of irrelevant articles (n = 368), along with conceptual articles (n = 100), study protocols (n = 30), and literature reviews (n = 93) due to the absence of empirical evidence. A set of empirical studies (n = 109) were removed as wearables were merely used as a measurement tool for research instead of studying the device itself. Figure 2 illustrates the process of deriving this dataset. The final dataset comprised 250 articles published between 2010 and 2019.
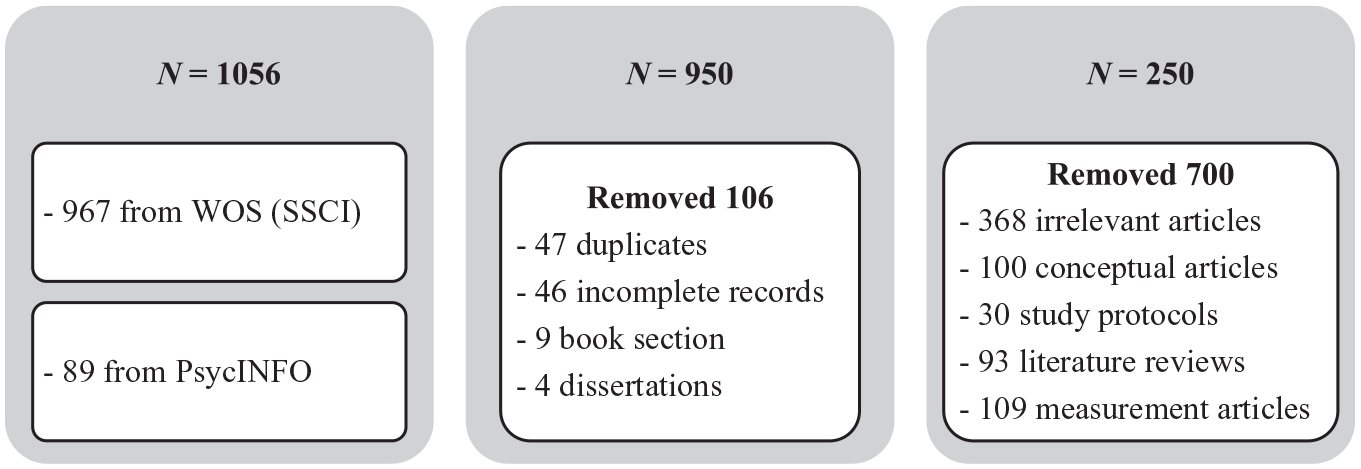
Steps taken towards the selection and formation of final dataset (N = 250).
Data extraction and analysis
For every paper in the dataset, information was extracted using a standardized form including fields for descriptions of the wearable device used in the study, descriptions of study methods, and factors relating to the I-M-O framework. One co-author first used the form to extract information from the articles and a second co-author double-checked the results. All authors met regularly to analyze selected articles and synthesize the findings to derive the themes answering the research questions posed. Statistical pooling of results for meta-analysis was not possible due to extensive heterogeneity of study methods and results.
Findings
Descriptive overview of dataset
Types of sensors used
Wearable devices can provide useful information and services for different health aspects. We classified body-mounted bio-sensors into three categories according to the type of health information they collected: (1) physical, (2) psychological, and (3) social. First, physical activity tracking utilizes tools such as accelerometers to monitor body motion signals, and further derives physical activity information such as step counts and activity intensity. Second, psychological indicators are derived from respiration, electrodermal activity, and signals produced by the electrocardiogram, to monitor mental health states. Sensors for social interaction, such as augmented reality glasses, cameras, and acoustic sensors, are designed to monitor interactions between individuals and their environment through the gathering of external visual, audio, or video information. A summary of the sensors used and information collected is shown in Table 1.
Types of wearable sensors and information collected in dataset (N = 250).
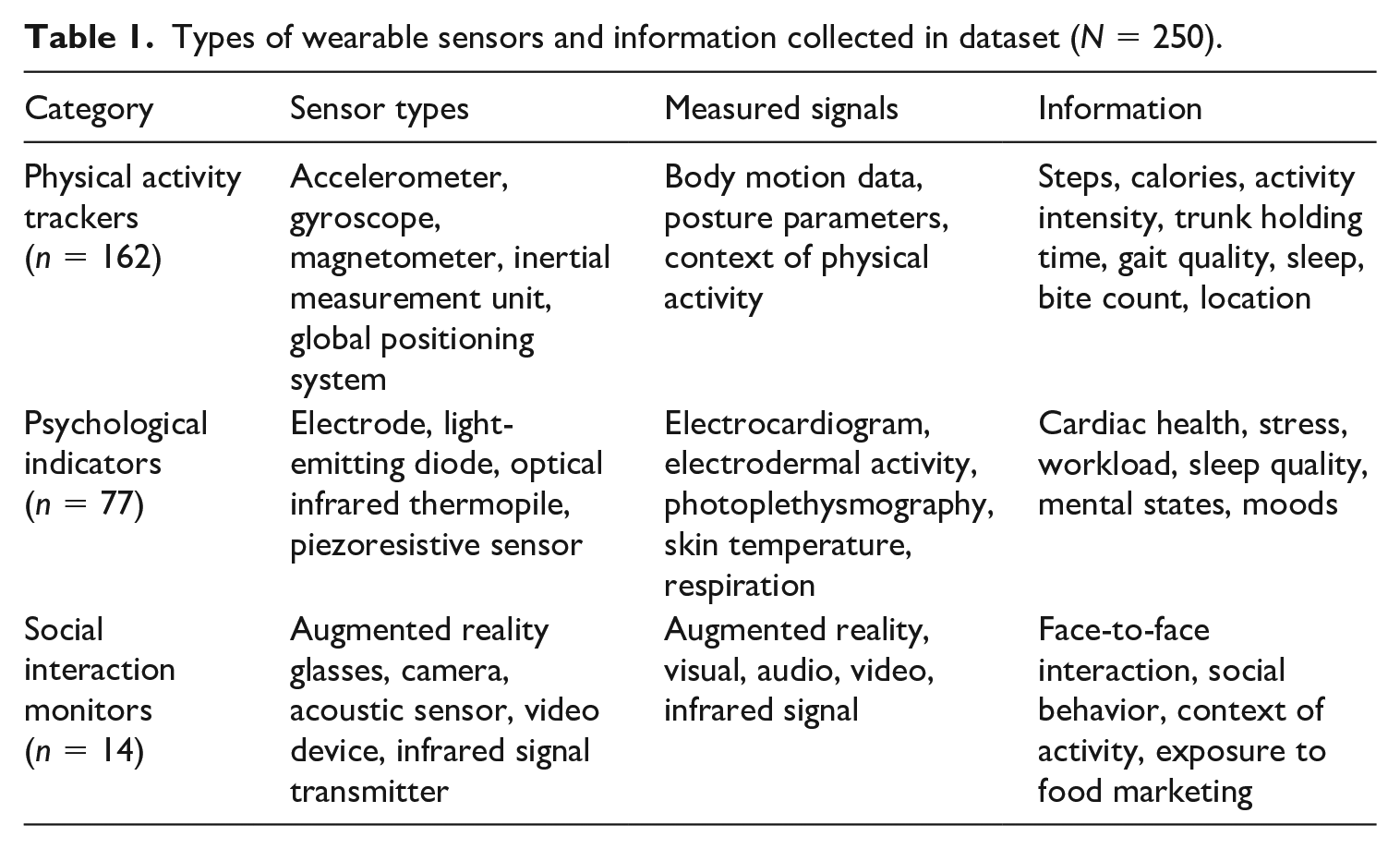
We note that some papers (n = 64) employing multi-sensor arrays relate to more than one category. Researchers more frequently used physical activity sensors (n = 162) and psychological indicator sensors (n = 77). Sensors monitoring social interaction were seldom studied (n = 14). These relative proportions reflect the level of maturation in the field, with wearables studies prioritizing physiological measurement over social interaction.
Sensors were seamlessly integrated into devices worn on the body, like wristbands, clothing, insoles and belts, to continuously monitor health information in an unobtrusive manner. Some papers studied wearables mounted on more than one body part (n = 37), while some did not specify the mounting location (n = 54). Sensors monitoring physical activity and psychological indicators were predominantly wrist-mounted, while sensors monitoring social interaction were mostly hung around the neck. The latter received the lowest ratings (Fang & Chang, 2016). Some users felt odd wearing them, suggesting that implementation of social interaction trackers might face the challenge of low acceptability.
Target audiences
Study samples used in the review dataset comprised two broad categories: the general healthy populace, with the purpose of health maintenance or improvement; or patients, with the purpose of coping with diagnosed diseases. Around 23% of the 250 studies used patient samples, while 77% studied healthy population groups. These disproportionate numbers indicate the current emphasis on using wearables in health management, and a need for more empirical studies on disease management. In similar vein, 241 studies investigated the use of wearables at the individual consumer level, while only nine papers addressed their use by healthcare organizations. This suggests that even though wearables are commercially prevalent, their formal adoption by healthcare providers remains limited. At this juncture, we can speculate that this is due to lack of substantive evidence of beneficial health effects and privacy of medical records required by legislation of healthcare providers.
Amongst healthy population study samples, approximately two-fifths specifically studied employees and the elderly (see Figure 3 for distribution of the review sample). The specific focus on these two target groups indicate how researchers perceive a need to emphasize health promotion amongst working adults and older adults and envision the use of wearables as a means of motivation for self-care.
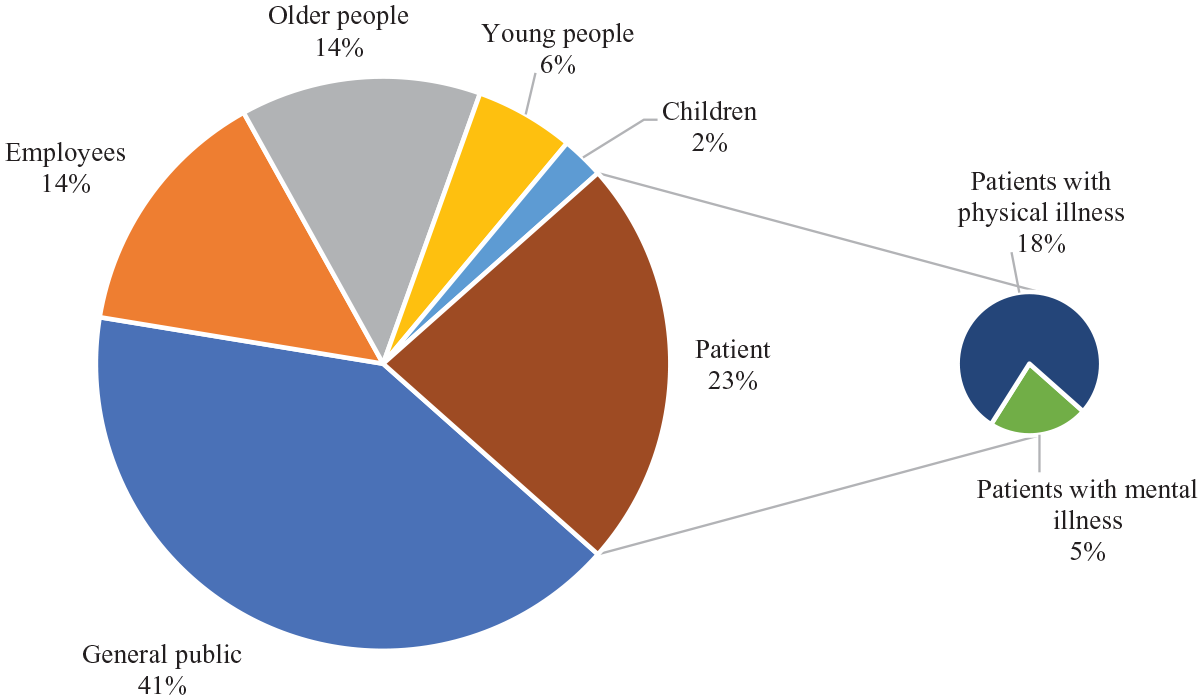
Distribution of study samples in dataset.
Current status in the I-M-O framework (RQ1)
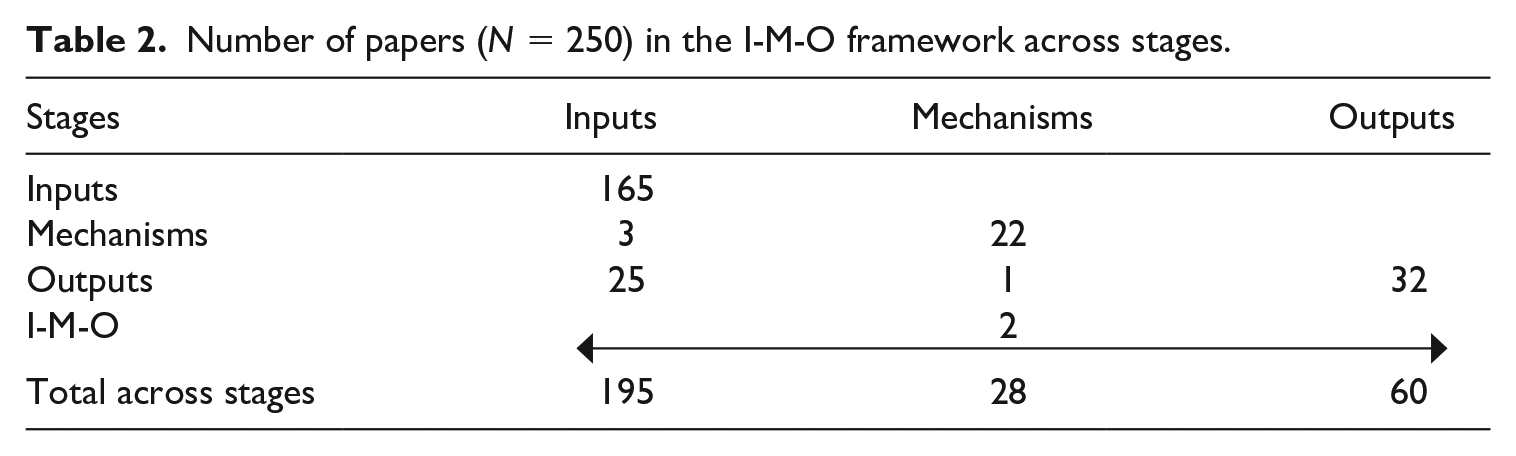
The first research question inquired about the status of current empirical research on health-related wearables in terms of the I-M-O framework. The aim was to synthesize transdisciplinary research on wearables, so as to provide a holistic overview of available empirical data and identify research gaps (see Figure 4, Table 2, and Table 3). Analysis of the dataset revealed that the present scientific emphasis is on technology development rather than on health outcomes, with explanatory frameworks comparatively de-emphasized. Specifically, a total of 195 papers addressed input factors including technological design (n = 112), user acceptance (n = 59), and engagement strategy (n = 24). Second, 60 papers addressed output factors, specifically individual (n = 57) and organizational (n = 3) health outcomes. Lastly, 28 papers addressed mechanisms explaining adoption (n = 17), post-adoption use (n = 7), and prediction of health behavior change (n = 5), with one paper addressing both adoption and post-adoption mechanisms.
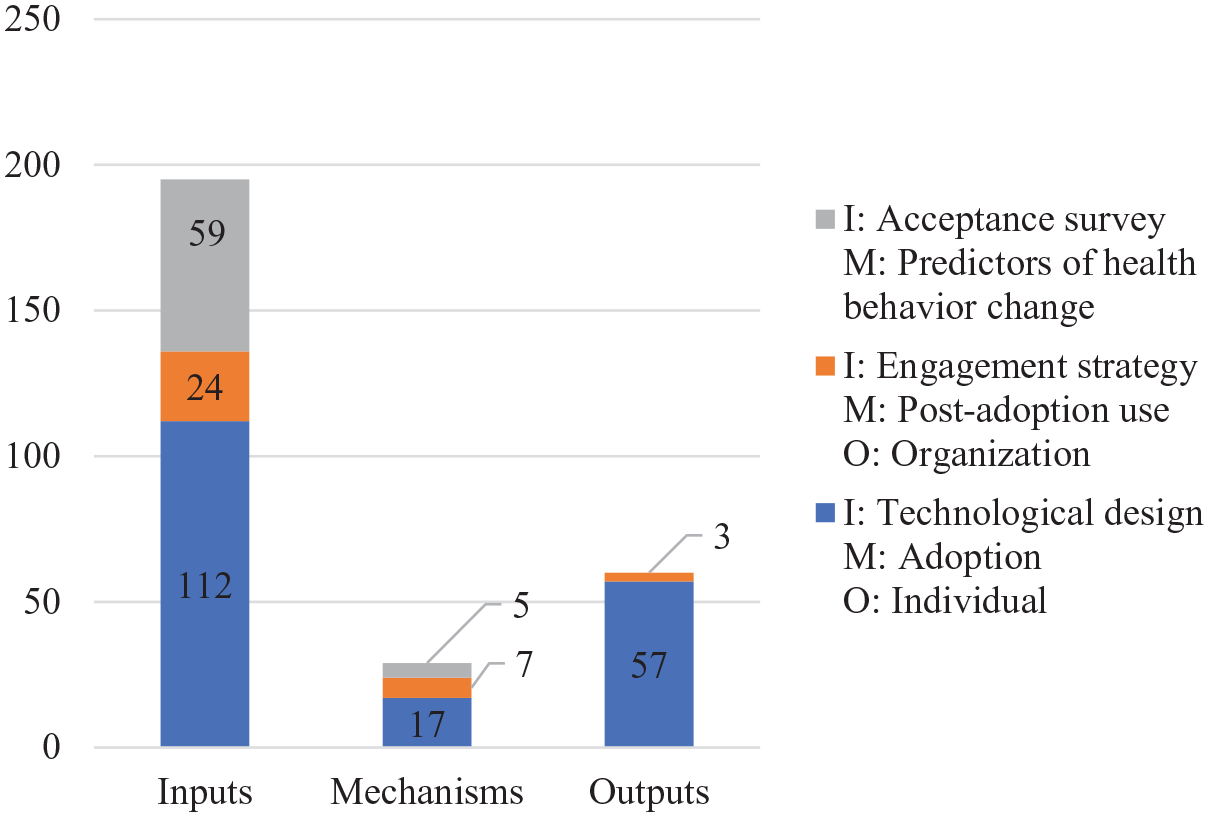
Papers (N = 250) sorted into I-M-O categories.
Number of papers (N = 250) in the I-M-O framework across stages.
Number of papers (N = 250) in the I-M-O framework across themes.

Note: Figures in bold indicate the key statistics that will be explained in-text.
Multi-stage papers
These numbers are overlapping and not cumulative, because 29 papers contained two stages of the framework—either I-O (n = 25), or I-M (n = 3), or M-O (n = 1)—and two papers addressed all three stages of the I-M-O framework (see Table 2 and Table 3 for details).
Only 12% (31/250) of the dataset comprised multi-stage papers, much less than the proportion in the mHealth App field (42%, 36/85) (Chib & Lin, 2018), indicating that sophistication of research design in this sub-field is hampered by the lack of interdisciplinary integration. This is indicative of an emergent phase of a sub-field.
I-M-O papers (n = 2)
Two papers examined the entire I-M-O pathway—both linked engagement strategies to predictors of health behavior changes, then to individual outcomes. Jang and Kim (2019) used feedback of different formats and values to motivate daily step change, applying the concept of a perceived companion for health attitude and behavior change. Factors derived from Social Cognition Theory were studied to explore the link between social incentives to motivate physical activity (Ratz et al., 2019). However, seeing how less than 1% (2/250) of the dataset covered all three stages, there is an evident lack of studies that apply theory to explain how and why required inputs can lead to desired outputs.
I-M papers (n = 3) and M-O papers (n = 1)
Three papers studied the link between inputs and mechanisms; for example, researchers applied the extended Technology Acceptance Model to explain users’ preference for screen shapes (Kim, 2016) and the feasibility of an early warning cardiac monitoring system (Lin et al., 2018). One paper studied the link between mechanisms and outputs, using the extended Technology Acceptance Model to explain continued tracker use and consequent individual health outcomes (Lunney et al., 2016). While this is a good start in using theory to increase the rigor of studies on wearables, the apparent lack of papers that examined the role of theorized mechanisms points to the necessity for more theory-informed research.
Of the four papers that linked mechanisms with either inputs or outputs, two investigated the I-M link between technological design and adoption (Kim, 2016; Lin et al., 2018); one, the I-M link between engagement strategy and post-adoption (Shin & Biocca, 2017); and one, the M-O link between post-adoption use mechanism and individual health outcomes (Lunney et al., 2016). The difference in numbers between I-M and M-O papers shows that scholars currently emphasize theory-driven inputs over health outputs.
I-O papers (n = 25)
Only two of 112 technological design studies investigated health outcomes, which indicates that the effectiveness of most technological designs in terms of health impact is unknown. These studies investigated feasibility of stress classifiers (Winslow et al., 2016) and trunk inclination alarms (Yan et al., 2018) while measuring stress and posture scores respectively. In contrast, studies on engagement strategies are mostly linked to health outcomes (20/24). Social incentives (e.g., Ellingson et al., 2019), financial incentives, (e.g., Chokshi et al., 2018) and feedback on user performance (e.g., Fukuoka et al., 2018) were among the common engagement strategies employed to yield outputs. The stark difference in these proportions suggests that currently user-centric designs, as compared to techno-centric designs, more closely relate to health outcomes.
Single-stage papers and highlighted themes
Amongst the papers that covered only a single stage of the I-M-O framework, technological design (n = 108) and acceptance (n = 54) were the most frequently studied themes. When summed with the multi-stage papers, the same two themes were emphasized: technological design (n = 112) and acceptance (n = 59). The emphasis on early developmental input factors of technological design and acceptance of wearables indicate that the field is still in infancy. In contrast with previous reviews on mHealth use in developing countries (Chib et al., 2015) and mHealth apps (Chib & Lin, 2018), we found that with wearables, technological design was more broadly studied. This is likely because wearables are a combination of hardware and software; prior studies on mHealth focused more on software input factors such as user interface and usage, instead of the many different types of hardware designs that are of current interest.
The third most studied theme was individual health outcomes (n = 57). Organizational health outcomes (n = 3) were examined far less in comparison, indicating that the research on the uptake of wearables in healthcare systems is limited. Wearables might still be viewed as predominantly a consumer-level technology. There needs to be more evidence of positive outcomes to pave the way for introduction of wearables into healthcare systems settings.
While papers addressing mechanisms were the least amongst the three categories, the majority (15/28) focused on adoption. However, we also noted a shift towards post-adoption phases, and resultant behavioral changes, which is a positive sign of development in the field. For the complete details of all 250 reviewed papers, please see the table in Online Appendix A.
Invasiveness of wearables (RQ2)
The second research question asked: How has research on the invasiveness of wearables evolved in response to consumers’ privacy concerns? Papers that studied technological designs (n = 112) were analyzed to explore the trend of wearables’ invasiveness. We plotted two timelines to reflect the evolution of wearables for physical health (n = 92, see Figure 5), and for mental health (n = 20, see Figure 6), with details relating to the type of signals and information collected. Overall, the number of studies investigating wearable designs increased in recent years for both physical and mental health. The former thrust increased exponentially from one paper in 2011 to 30 papers in 2018, and 19 papers in 2019 (up until August). However, papers studying technological design for mental health purpose increased marginally from one paper in 2010 to five papers in 2018, and three papers up until August 2019. We argue that the difference in the rates of increase is likely due to disparity between the types of signals collected by wearable technologies, and the types of information produced from those signals.
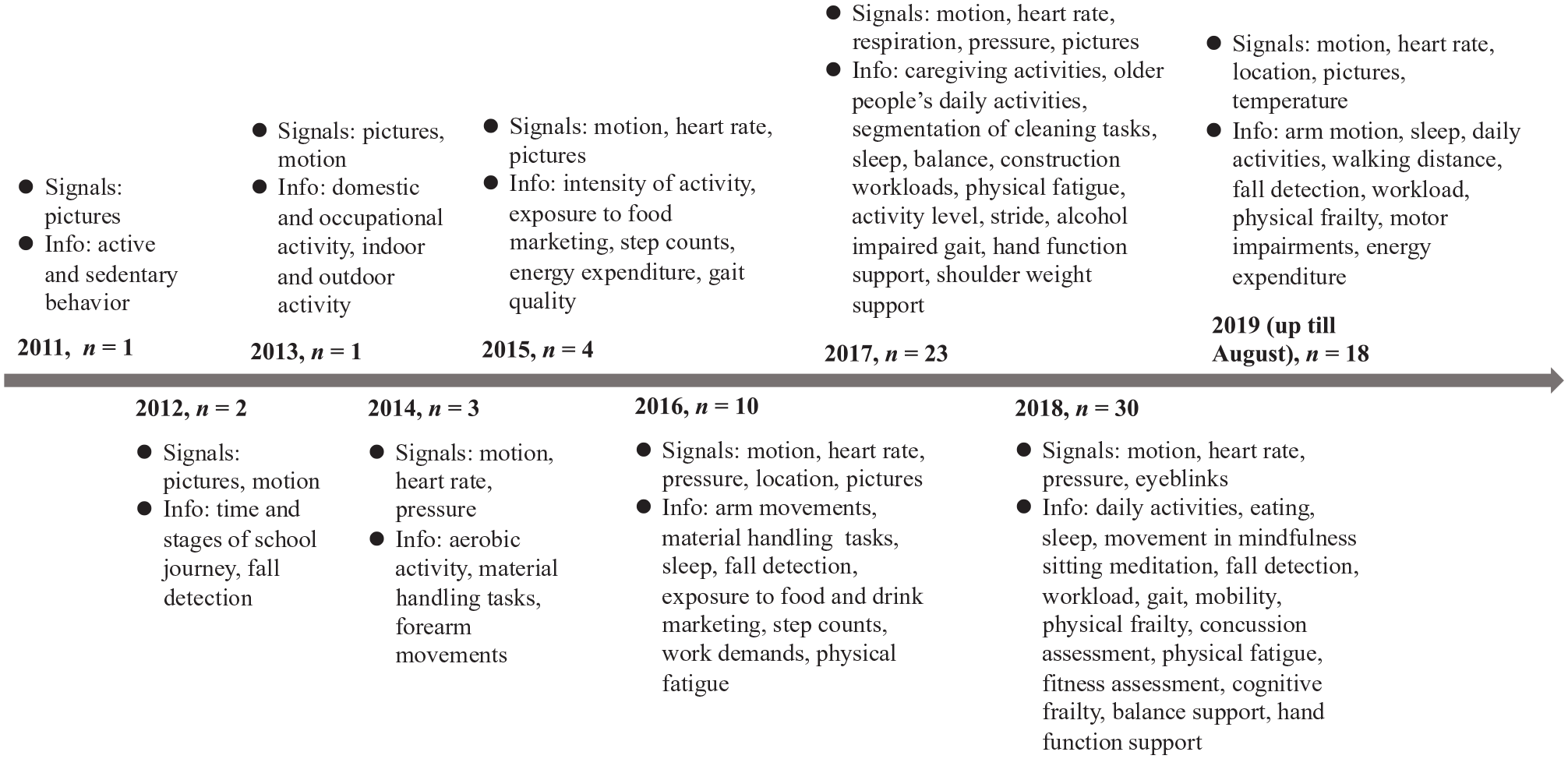
Timeline of wearables for physical health (n = 92).
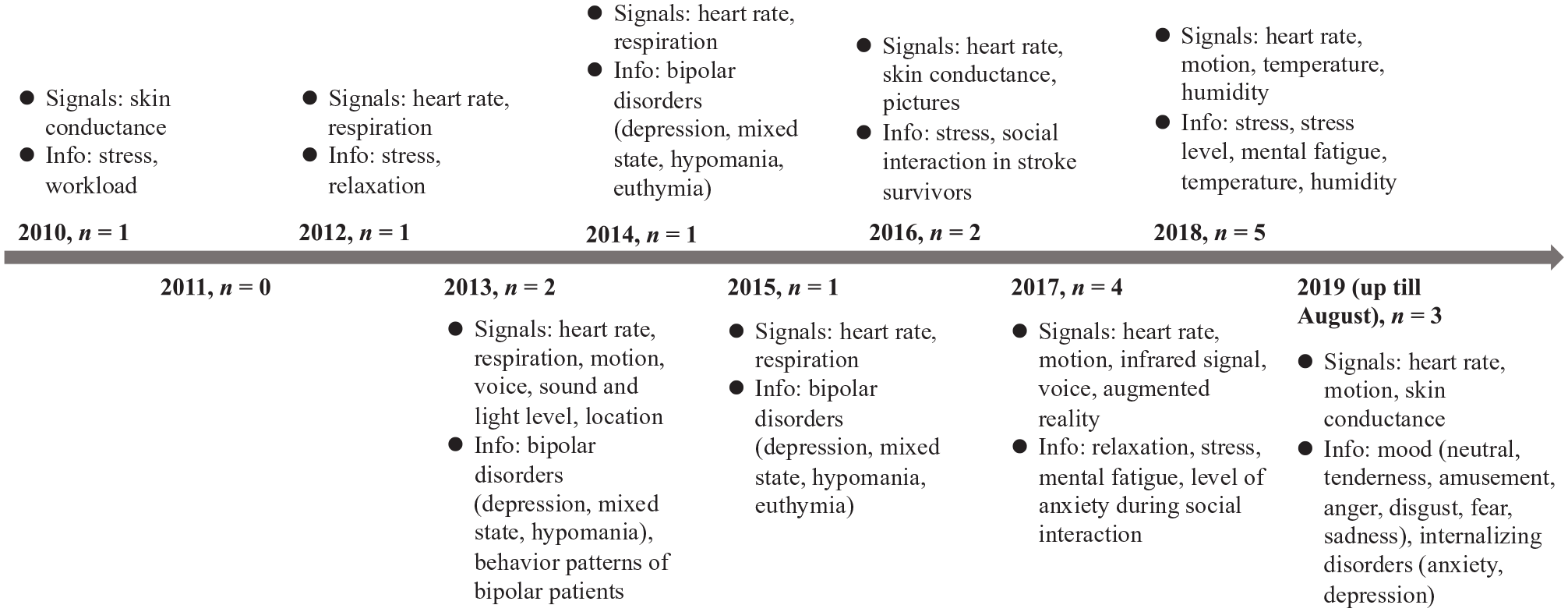
Timeline of wearables for mental health (n = 20).
In physical health papers, physiological signals yield information or make predictions for physical health. A complex transitional process is involved in mental health measures—physiological signals need to be converted into psychological information to predict mental states. Currently, the translation between physiological signals to mental health is less advanced in the study of wearables.
Generally, the timelines highlight two key points in relation to the invasiveness of wearables: (1) sensor signals are increasing in quantity due to integration of sophisticated hardware, and (2) collected health information exhibits increasing sophistication of purpose and level of detail due to complex software algorithms.
Signals
For both physical and mental health studies, wearable devices not only measured physical signals such as an individual’s health indicators and behaviors, they also measured ecological signals such as an individual’s interaction with natural and social environments.
Physical health
In the early stages, signals for physical health mainly utilized time-stamped pictures gathered by cameras (Kelly et al., 2011). Other signals such as motion (Ferrari et al., 2012), heart rate (Reiss & Stricker, 2014), pressure (Kim & Nussbaum, 2014), location (Cowburn et al., 2016), respiration (Lee, Seto et al., 2017), eyeblinks (Horiuchi et al., 2018), and temperature (Lui & Menon, 2019) were gradually introduced over the years. The timeline (Figure 5) shows that both physical and ecological signals were collected from the beginning, and both types of signals increased as devices integrated the collection of more signals over time.
Mental health
In the early stages, skin conductance (Setz et al., 2010) was utilized in mental health studies; then signals such as heart rate and respiration (Choi et al., 2012); motion, voice, location, sound and light level (Mohiuddin et al., 2013); infrared signals (Masumoto et al., 2017); augmented reality (Keshav et al., 2017); and humidity and temperature (Austad et al., 2018) were added. The timeline (Figure 6) shows that physical signals were utilized more in earlier years; ecological signals were subsequently added. As with physical health, studies on mental health are applying the use of wearables that integrate both types of signals, and the signals collected are simultaneously increasing.
Common signals collected to measure both physical and mental health included heart rate, motion, temperature, respiration, and location. However, physical health studies also used signals such as pictures, pressure, and eyeblinks; while mental health studies utilized skin conductance, voice, augmented reality, infrared, and signals about sound and light levels. From the distinctiveness of signals, we noticed that signals uniquely used for physical health were external body indicators such as pressure and eyeblinks, while signals uniquely used for mental health were internal body signals (e.g., skin conductance), and ecological signals reflecting social interactions (e.g., voice, augmented reality, infrared). Ecological signals reflecting natural environments were employed differently, with physical health studies utilizing pictures; and mental health studies, signals about sound and light levels.
Information
We noted that information collected about physical health and mental health was increasingly sophisticated in terms of range and depth. We define range as the variety of information signals collected and their use for a wide variety of purposes, while depth comprises the detail and precision of the signal.
Physical health
A wide range of information on physical activity was used to monitor various human activities, both private and professional across human lifespans. To list some examples, daily physical activity levels of school-aged children (Kelly et al., 2012) and adults (Doherty et al., 2013) were measured to promote active lifestyles. The manual tasks of blue-collared populations were recognized to prevent work-related musculoskeletal disorders (Kim & Nussbaum, 2014; Liu & Chan, 2017). Sleep of adolescents was assessed to monitor their health (De Zambotti et al., 2016). Older people’s daily activities were assessed to support home-based care (Liu et al., 2017). Feeding gestures were detected to prevent obesity (Zhang, Stogin et al., 2018). Movement in mindfulness meditation was detected to facilitate training (Rodriguez et al., 2018). Environmental information such as indoor or outdoor settings (Doherty et al., 2013), and exposure to food marketing (Barr et al., 2015), were collected to better design health behavior interventions.
In terms of depth, we noted that over time, more fine-grained information was obtained through enhanced analytical sophistication of signals. Initially, the information extracted captured discrete dichotomous information, but progressed to continuous measurements. Activities progressed from merely being identified as occurring (or not) to being able to judge the type and the quality of the specific physical activity. For example, activity was merely differentiated from sedentary behavior (Kelly et al., 2011), then became more explicitly defined as aerobic and anaerobic activity (Reiss & Stricker, 2014), followed by categorization of light, moderate, and vigorous activity (Ferguson et al., 2015). Gradually, continuous quantification of activity was achieved, enabling the calculation of the amount of energy expenditure (Ferguson et al., 2015), assessment of physical fatigue (Maman et al., 2017), and workload (Hwang & Lee, 2017).
Mental health
The depth of mental state analysis increased in sophistication over time. In earlier years, studies conducted binary classifications of mental states, i.e., stress vs. workload (Setz et al., 2010) or stress vs. relaxation (Choi et al., 2012). Subsequently, continuous stress levels could be calculated as algorithms via multi-factor analysis so that mental states could be measured more precisely (Betti et al., 2018).
In earlier years, stress was distinguished from the normal mental state (Setz et al., 2010), before a spate of studies investigated specific mental health issues. To determine strategies for promoting mental health, changes in behavioral patterns were monitored and found to be associated with changes in bipolar patients’ moods (Mohiuddin et al., 2013). Later, four types of bipolar disorders (depression, mixed state, hypomania, euthymia) were differentiated (Lanata et al., 2015). Recent studies take a more praxis-driven angle. Three mental states (fatigued, stressed, relaxed) of car drivers were distinguished to develop an intelligent safety alert system (Lee, Chong et al., 2017). The effect of environmental temperature and humidity on workers’ stress was evaluated (Austad et al., 2018). Seven types of moods (neutral, tenderness, amusement, anger, disgust, fear, sadness) were measured to detect negative emotions that could lead to social isolation in older adults (Martínez-Rodrigo et al., 2019). Wearables were also used to screen children for internalizing disorders like anxiety and depression (McGinnis et al., 2019).
In sum, the invasiveness of wearables increased for both physical and mental health. Wearables collected physiological signals and environmental signals, which both increased in quantity over time with the integration of hardware. In terms of derived information, more detailed attributes that reflect distinct dimensions of activity were explored over time as sophisticated measurement was achieved through advanced software and algorithms. This information was used for increasingly sophisticated purposes, from measurement to prediction and prevention of health issues.
Discussion
This review was conducted to determine the status of the current empirical research on wearables based on the I-M-O framework and examine trends in the invasiveness of wearable technologies. We consider the research, practical, and policy implications of the review.
Research perspectives
The findings reinforce our view that more sophisticated conceptual research is needed to translate the techno-optimism of wearables into tangible health benefits. Conceptual mechanisms are crucial to achieve the development of worthwhile inputs and efficacious outputs, yet consistent with prior I-M-O reviews (Chib & Lin, 2018; Chib et al., 2015), trends in this review show that research on emerging technology tends to focus on inputs and outputs and de-emphasize theoretical explanations. We find that the current emphasis is on input factors (n = 195) such as technological design and acceptance of wearables, which reflects the emergent nature of the sub-field. There is need for more empirical evidence of effectiveness on health outputs, as evaluation comprises only a quarter of studies.
Due to the multi-disciplinary nature of wearable devices, researchers have been calling for a transdisciplinary approach to realize their full potential (Kumar et al., 2013; Park et al., 2014). Social scientists should aim to understand consumer and patient behavior to uncover the link between different types of inputs and outputs through more inter-disciplinary collaborations. However, our review showed that inter-disciplinary multi-stage papers (13%, n = 31) were much less than single-stage studies, with the diminished role of the social scientist posing a risk to the advancement of wearable health technologies.
Applied perspectives
Scalability and sustainability are fundamental concerns in healthcare. Consumer adoption of wearables is increasing, suggesting the scalability of health initiatives involving wearables; however, such use is low and rarely sustained beyond several months (Fisch et al., 2016). One possible reason might be the lack of integration of wearables within a broader health ecosystem, with technology developers focusing on individual consumers rather than health institutions. First, the overwhelming emphasis of research has been at the individual consumer level, with a gap in the uptake of wearables in health organizations and for disease management. Second, healthy population samples (77%) were much more studied as compared to patient samples (23%). While physicians agree that wearables can improve patient monitoring and physician–patient communication (Loos & Davidson, 2016), more research needs to be conducted to investigate the challenges for uptake of wearables at the health organizational level. Third, one consequence of the focus on consumer-level technologies is that wearables research prioritizes technological hardware design much more than observed in prior reviews on mHealth (Chib et al., 2015) and mHealth apps (Chib & Lin, 2018), which focused more on software input factors like user interface and usage. Consequently, there is greater emphasis on technology adoption than on evaluation of health benefits. There is perhaps a need for commercial enterprises to consider self-care within an integrated program in conjunction with health institutions as a complement to traditional healthcare, rather than solely as a substitute consumer intervention.
Policy perspectives
We found that the invasiveness of wearables increased in terms of collected signals and derived health information. While sensor designs became less noticeable and less intrusive with more advanced technology, data collection became more invasive. Physical and psychological health, and environmental signals, can be measured and predicted, perhaps unbeknownst to users, as technological designs of wearables are increasingly integrated into daily living. This may lead us closer to realizing a future in which chips are embedded in the body, collecting integrated signals which in turn deliver substantial and substantive information (Andreu-Perez et al., 2015).
Collected health information is increasing in range and depth due to increasing sophistication in software and algorithms; more detailed attributes and higher levels of measurement can be obtained. Such trends indicate that extant privacy concerns of wearable health users (Becker, 2018) are legitimate. Further, the average user may not know how to protect the data that is collected by their wearable devices (Cilliers, 2019), increasing the risks of deviant misuse of data.
Additionally, collected signals and information can now span beyond users’ physiological measures to monitor their environments. Should law enforcement agencies be allowed to request for an individual’s wearable camera or smart glasses to retrieve evidence of a crime nearby? To what end should wearable health companies protect this data? Regulation of privacy of collected health data (Kumar et al., 2013) and educating users’ on how to protect their data (Cilliers, 2019) should continually remain part of the considerations in the advancement of wearable technologies, so as to improve user comfort levels and ensure ethical implementations of increasingly invasive wearable technology.
With the increase in the popularity of wearables as a consumer-level technology, bringing devices closer to ubiquity, and the potential of their effectiveness in healthcare, we believe that in the near future, factors such as cost (Fisch et al., 2016) will no longer impede wide-scale organizational policies. In fact, there have been nationwide initiatives such as National Step Challenge (MOH, 2020; Tan & Varghese, 2016) and the TraceTogether COVID-19 token involving the distribution and use of trackers in Singapore. With further development and acceptance of wearables devices, we predict that health wearables will become ubiquitous at the organizational and community levels. Alongside such trends, it is imperative to address user concerns of increasing invasiveness. There is a need to engage in policy discussions and foster debate on how this accumulated data should be handled, before large-scale applications put users at greater risks.
Overall, our review notes the de-emphasis on psycho-social mechanisms in current research, and the lack of transdisciplinary research that can move the field forward in a holistic manner. Future research—particularly by communication scientists—can plug these two gaps, by linking input and output factors with theory-driven mechanisms that will in turn inform development of input factors and application for efficacious outputs. Similarly, with imminent developments, we encourage researchers to apply their expertise in transdisciplinary projects to move the field forward in an effective and ethical fashion.
Supplemental Material
Appendix_A – Supplemental material for The state of wearable health technologies: a transdisciplinary literature review
Supplemental material, Appendix_A for The state of wearable health technologies: a transdisciplinary literature review by Caining Li, Sapphire H. Lin and Arul Chib in Mobile Media & Communication
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.