
Abstract
To perform a systematic review and meta-analysis to examine the association between persistent pulmonary hypertension (PPHN) and receipt of therapeutic hypothermia (TH), compared to those who did not receive TH, among infants with moderate or severe hypoxic-ischemic encephalopathy (HIE). Systematic review and meta-analysis based on Ovid, Medline, Embase and Cochrane central searches from 01/01/2000 to 31/03/2025. We included only randomized control trials for meta-analysis and followed international guidelines for conducting systematic reviews. The primary outcome of the study was PPHN in infants undergoing TH for moderate to severe HIE. Among 185 articles identified using search strategy, 19 articles were assessed for eligibility. Eight randomized control trials (RCTs) met the inclusion criteria, and seven were included in meta-analysis. A random effects model used for the outcome of PPHN, comparing TH with NT or usual care, involving a pooled population of 1006 infants across seven studies. The relative risk of PPHN for TH versus NT was 1.13 (95% confidence interval 0.81 to 1.57). We noted risk of bias in the blinding of participants across included RCTs. We assessed nine observational studies and performed a narrative review. We noted that a considerable number of infants developed PPHN across TH and NT groups. We did not find evidence of an association between TH and PPHN in infants with moderate to severe HIE, although a considerable number of infants developed PPHN across both groups. We suggest that clinicians should be aware of the risk of PPHN to allow prompt investigation and management.
Keywords
Introduction
Hypoxic Ischemic Encephalopathy (HIE) due to perinatal asphyxia can lead to severe neurological depression, seizures, and long-term neurological sequelae (Shankaran et al., 1991). Therapeutic hypothermia (TH) is currently a standard management for term-born infants with moderate to severe HIE (Gunn and Gunn, 1998). The adverse effects of TH are impaired cardiac function, coagulopathy, increased sepsis and arrhythmias (Schwab et al., 1998).
In utero, pulmonary circulation is a high-resistance system. At birth, there is release of vasodilators such as nitric oxide and prostacyclin along with reduction in endothelin-1 and angiotensin, which result in significant drop in pulmonary vascular resistance and improves pulmonary blood flow. In persistent pulmonary hypertension of the newborn (PPHN), there is a failure of physiological transition in a drop of pulmonary vascular resistance. This could be because of perinatal asphyxia, sepsis and TH (Gagnon and Wintermark, 2016).
Perinatal asphyxia is a risk factor for developing PPHN. In animal studies, hypothermia has been linked to increased pulmonary vascular resistance. A one-degree drop in temperature can raise pulmonary vascular resistance by 1–2% (Rubini, 2005). These effects, when superimposed on the pulmonary compromise from hypoxia or meconium aspiration, may explain the higher incidence of PPHN in cooled infants compared to those managed with normothermia (Lapointe and Barrington, 2011). In neonates with perinatal asphyxia, it is suggested that the increased oxygen requirement during TH is likely due to PPHN and may have serious clinical consequences. Joanna R G et al., 2022 showed an increased incidence of PPHN following the introduction of TH in infants with HIE (Joanna R G et al., 2022).
Since the introduction of TH as standard of care treatment for HIE, PPHN during TH has been reported in most of the randomized control trials (RCTs). Whether PPHN is secondary to perinatal asphyxia itself or following initiation of therapeutic hypothermia has not been evaluated (Joanna R G et al., 2022). There is some evidence that among infants with moderate HIE, the development of PPHN is associated with increased risk of death or moderate/severe disability at 18–22 months (Agarwal et al., 2021). There is conflicting evidence in the literature on whether TH is associated with PPHN (Simbruner et al., 2010). While the Cochrane review of Cooling for infants with hypoxic ischemic encephalopathy examined PPHN during TH, their systematic review was published in 2013 (Jacobs et al., 2013).
It was observed that desaturation due to pulmonary hypertensive crisis was more common during the rewarming phase, so rigorous monitoring is required (Shah et al., 2010). Along with pre and post ductal monitoring for PPHN, there is emerging evidence that NIRS (Near Infra-Red Spectroscopy) monitoring of cerebral oxygenation be helpful in infants who develop PPHN during TH (Rallis et al., 2024). In PPHN, cerebral oxygenation will be reduced due to right to left shunting (Gagnon and Wintermark, 2016). Thus, treatment of PPHN may prevent brain injury and prevent neurodevelopmental impairment.
We aimed to conduct a systematic review and meta-analysis using contemporary data to examine the association between PPHN and receipt of TH, compared to those who did not receive TH, among infants with moderate or severe HIE.
Methods
This systematic review and meta-analysis were conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) checklist in Supplementary Data. The review was registered on PROSPERO (CRD42024513342), and amendments were submitted.
Data sources
We searched the following databases: MEDLINE, PUBMED, EMBASE, CINAHL, EMCARE, and COCHRANE. We performed a search for articles published from 01/01/2000 to 31/03/2025 using terms related to neonates, hypoxic ischemic encephalopathy, therapeutic hypothermia, persistent pulmonary hypertension in newborns, and neonatal intensive care units (Supplementary Table S1—Detailed search strategy). Only articles in the English language were included. Titles and abstracts were exported from the search results and imported into Rayyan, where artificial intelligence assisted with manual de-duplication.
Selection process
We screened and reviewed RCTs, non-randomized control trials, cross-sectional studies, cohort studies, case-control studies, and comparative studies. To avoid bias or confounding from unbalanced comparator groups, only RCTs were included in the final meta-analysis, and a narrative review was conducted for observational studies. Case series, case reports, experimental or mechanistic studies, as well as laboratory or animal studies, were excluded. There were no restrictions based on the income level of the country.
We included infants born at ≥36 weeks who were diagnosed with moderate or severe HIE. HIE was classified as Sarnat stage 2 or 3, and eligibility for treatment with TH was according to the relevant regional or national guidelines. TH was defined as achieving a core temperature of 33°C–34°C. This encompassed instances where TH was initiated, and the target temperature reached despite early rewarming. Our definition of NT included servo-controlled NT or infants receiving antipyretic medication.
We excluded infants with major congenital abnormalities, metabolic disorders, or severe hemorrhage, as these infants would not qualify for treatment with TH.
We included studies describing our primary outcome of PPHN, ideally defined by clinical and/or echocardiographic criteria.
Two reviewers (R.J., H.G.) independently screened all titles and abstracts, and disagreements were resolved by discussion. Subsequently, full articles were obtained and reviewed from included abstracts.
Data extraction
We utilized Rayyan (Rayyan Systems Inc, Cambridge USA, 2022) for data management. Relevant data were extracted and entered into a Data Collection Form in Excel.
We collected the following data items: study methodology; data collection period; setting including country, single or multi-center; population include gestational age and study definition of HIE; TH delivered; NT delivered; and definition of PPHN as an outcome.
Data synthesis
We performed a meta-analysis of RCTs using a random effects model in STATA 18.0 (StataCorp, College Station, TX, USA) to produce forest plots and funnel plots, employing I2 as a measure of heterogeneity. Where meta-analysis was not possible, we intended to utilize narrative synthesis.
Quality assessment
We performed a critical appraisal for the risk of bias using the Joanna Briggs Institute (JBI) Checklist for RCTs (Barker et al., 2023). The domains included randomization, allocation concealment, blinding, follow-up, and outcome assessment. Our risk of bias assessment focused on our primary outcome of interest (PPHN) rather than the study’s original primary outcome, specifically related to bias in measuring outcomes. We presented the findings of our quality assessment as a ‘traffic light’ grid and did not exclude studies based on our quality assessment; rather, this contributed to our discussion and conclusions. We utilized the appropriate JBI Checklists for observational studies (cohort or case control as appropriate; Fig. 2).
Results
One hundred and 85 articles were identified using the search strategy. During the initial screening, 164 non-relevant articles were excluded after reviewing the titles and abstracts of the articles. Nineteen articles were fully assessed for eligibility. Of the articles considered relevant to the study objectives, eight RCTs met the inclusion criteria, and seven were included in the meta-analysis. (Azzopardi et al., 2009; Eicher et al., 2005; Faix et al., 2025; Gluckman et al., 2005; Rakesh et al., 2018; Shankaran et al., 2005; Simbruner et al., 2010; Thayyil et al., 2021). Reasons for exclusion were incorrect study type (e.g., systematic review, n = 1; non-randomized trials, n = 9) and inappropriate population (mild hypoxic-ischemic encephalopathy, n = 1; Fig. 1 PRISMA flow chart). We included nine observational studies for narrative synthesis.
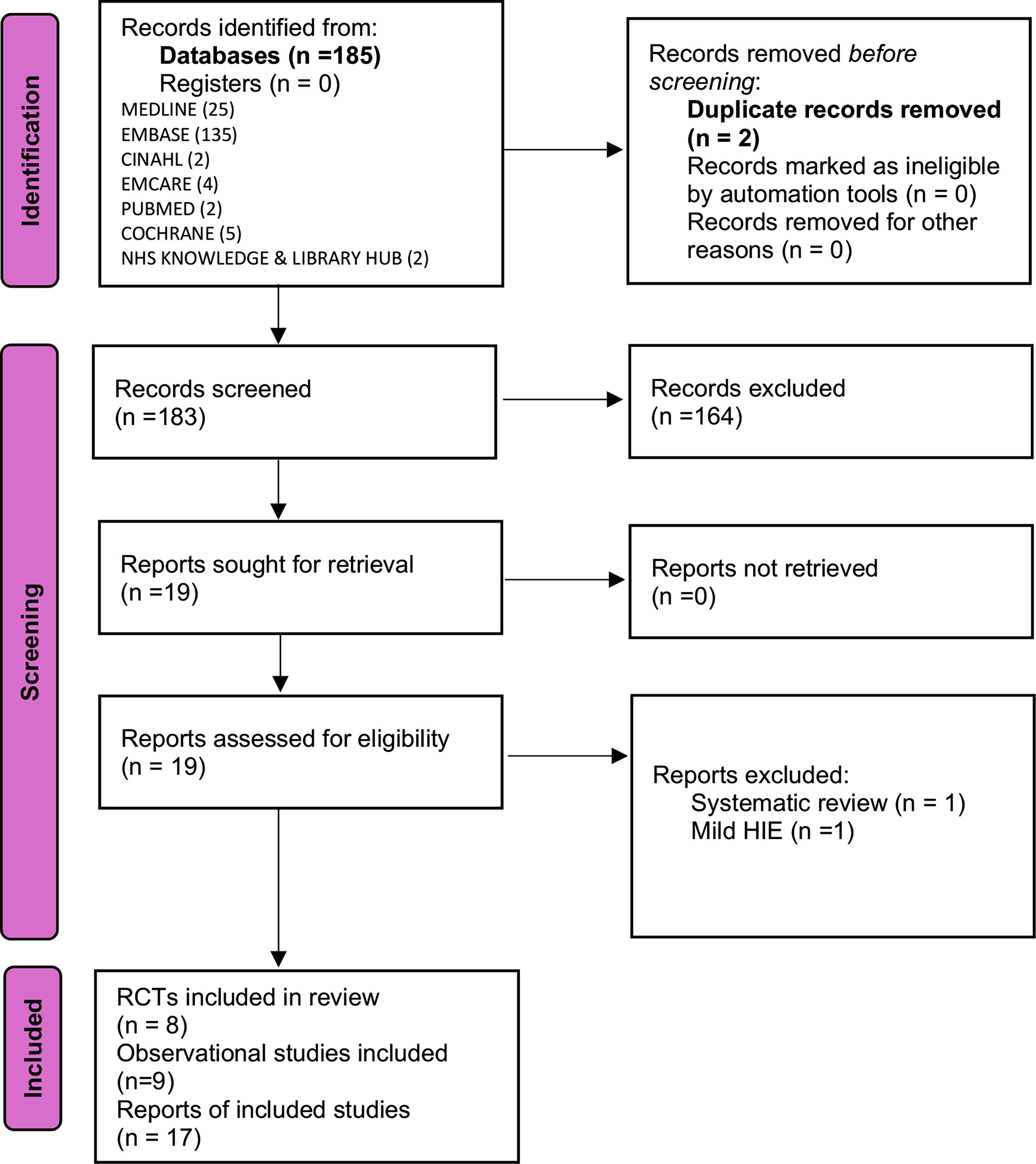
PRISMA flow diagram.
Study characteristics
Table 1 describes the RCTs included in the review, focusing on the primary outcome of PPHN in TH versus NT group for HIE. Of the eight RCTs identified, the majority were conducted in high-income settings, with the exceptions of the studies by Thayyil et al. and Rakesh et al. Our search identified one RCT involving late preterm infants between 33 and 35 weeks of gestation (Faix et al). After discussion among authors, it was felt the article was relevant to include in the systematic review.
Characteristics of RCTs on TH and PPHN Outcomes
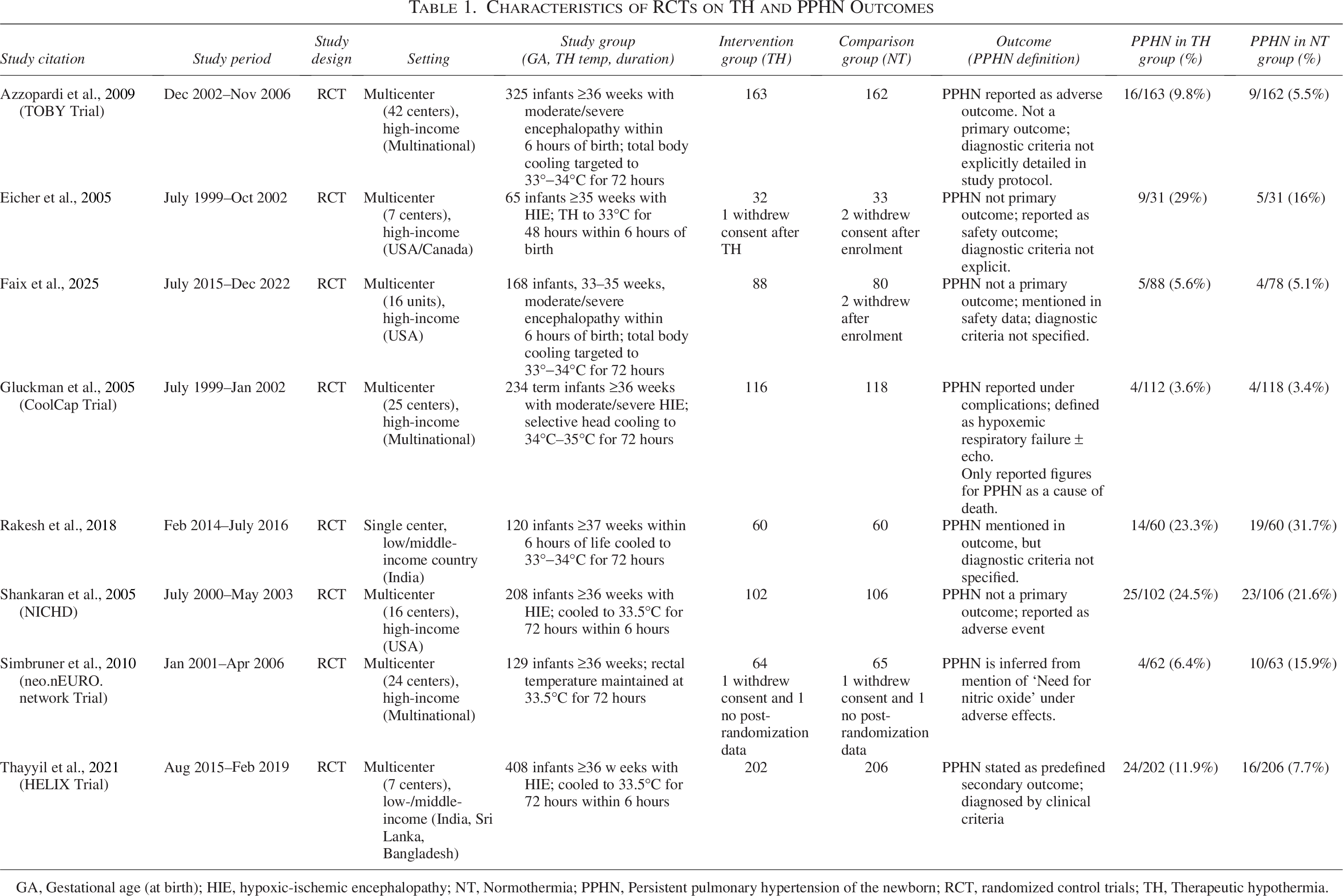
GA, Gestational age (at birth); HIE, hypoxic-ischemic encephalopathy; NT, Normothermia; PPHN, Persistent pulmonary hypertension of the newborn; RCT, randomized control trials; TH, Therapeutic hypothermia.
There was heterogeneity in the assessment of PPHN as an outcome, with most studies not explicit about how it was defined, some using clinical criteria (Thayyil et al.), “Need for nitric oxide” (Simbruner et al., 2010), or clinical/echocardiographic criteria (Shankaran et al., 2005). All RCTs used whole body cooling with blanket devices, except the Gluckman et al., 2005 “Coolcap” study.
Table 2 outlines the observational studies included in our narrative synthesis. The study designs comprised cohort studies (n = 8) and a case-control study (n = 1). The Lakshminrusimha et al., 2018 study was a cohort study utilizing data from two trials, which included the Shankaran et al., 2005 RCT. There was a mix of studies from high-income and low/middle-income countries, and while most studies included infants born at 36 weeks and above, some (Herrera et al., 2018; Rao et al., 2017) included more preterm infants.
Characteristics of Non-RCTs on TH and PPHN Outcomes
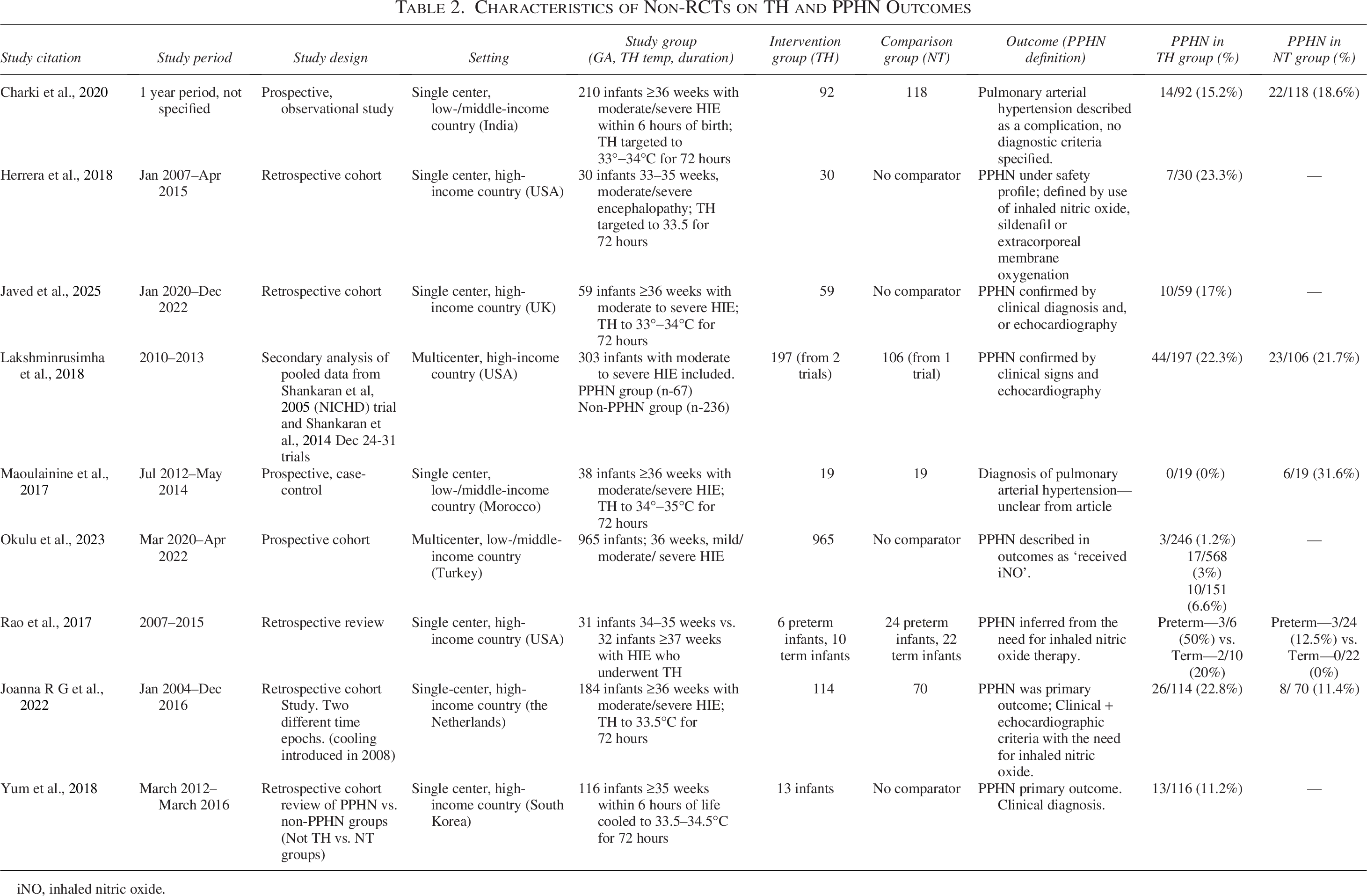
iNO, inhaled nitric oxide.
Study quality
We evaluated all studies across the JBI domains for RCTs (Fig. 2) and found that no included studies employed blinding of participants (i.e., infants’ families) or providers (neonatal clinical teams), although some studies did blind assessors. Nevertheless, all studies exhibited a low risk of bias across domains regarding randomization, baseline similarity, adequate follow-up, intention to treat analysis, and appropriate statistical methodology. None of the studies provided clear definitions of echocardiography features of PPHN, nor confirmed the presence of PPHN by echocardiogram in all participants, which introduced a risk of bias in the assessment of our outcome of interest.
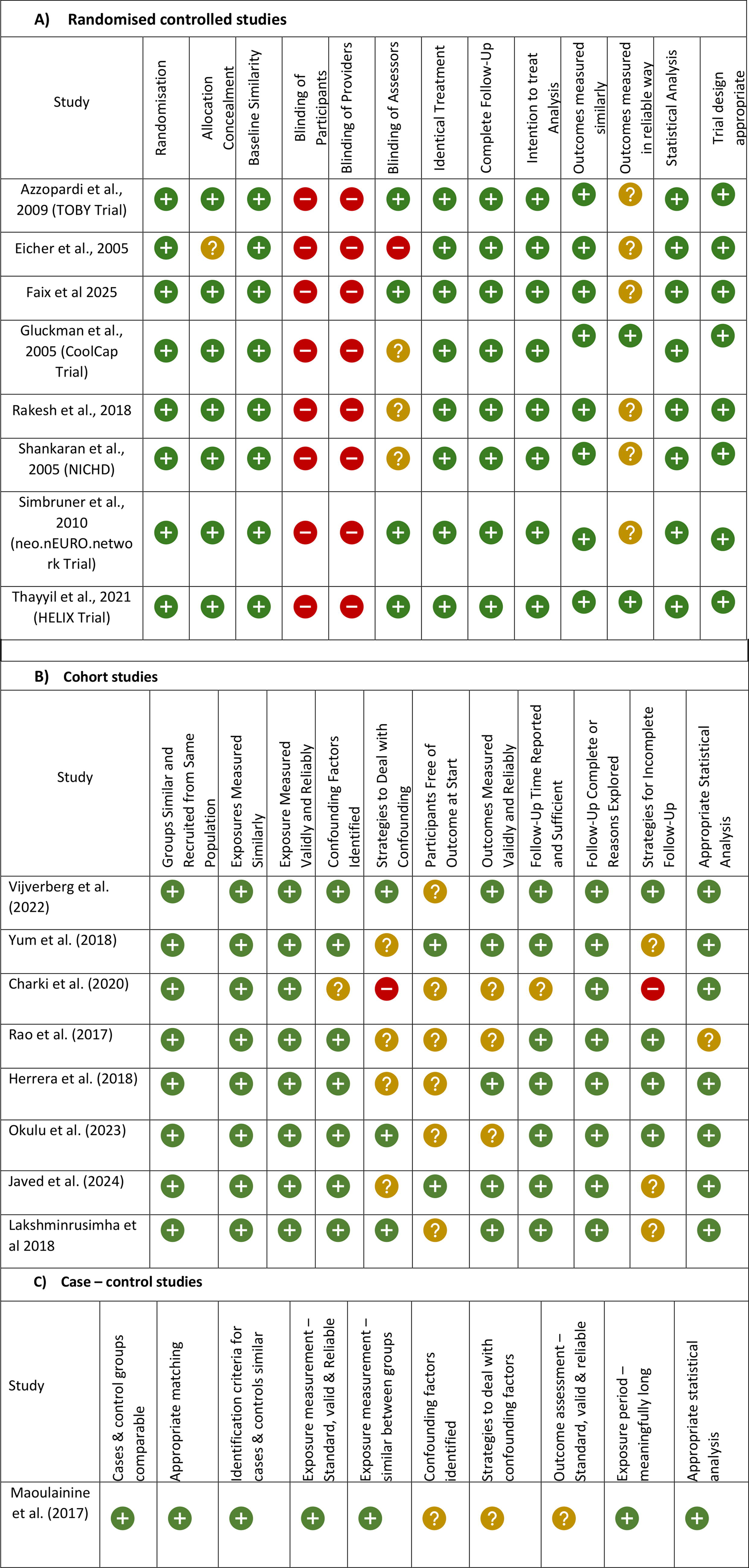
Results of Risk of Bias summary: Review of authors’ judgements regarding each risk of bias domain for each included study.
Across observational studies, the risk of bias was identified in strategies for dealing with confounding, participants free of outcomes at the start, outcomes measured validly and reliably, and strategies for incomplete follow-up domains. Notably, there was variation in how PPHN was defined, from receipt of inhaled nitric oxide (iNO) to echocardiography.
Primary outcomes
We conducted a meta-analysis using a random effects model for the outcome of PPHN, comparing TH with NT or usual care (Fig. 3), involving a pooled population of 1006 infants across seven studies. The overall relative risk was 1.13 (95% confidence interval 0.81 to 1.57), with no statistically significant evidence of an association between TH and PPHN. Moderate heterogeneity was observed across studies (I2 28.5%), although the 95% confidence intervals of all studies crossed one.
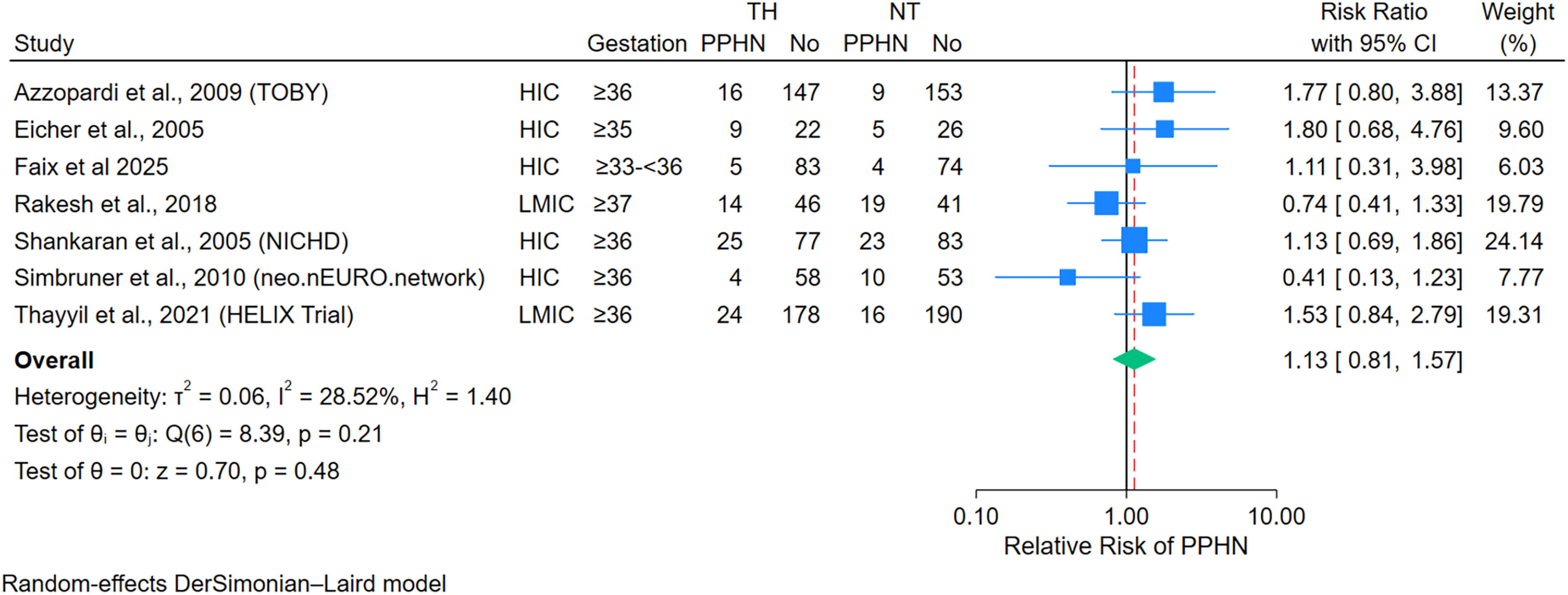
Forest plot of randomized control trials (RCTs) of therapeutic hypothermia (TH) vs. normothermia (NT) for the outcome of persistent pulmonary hypertension of the newborn (PPHN), by included gestation and high-income country (HIC) versus low-/middle-income country (LMIC). Heterogeneity is presented using as the measure of I2.
We did not include the “Coolcap” study by Gluckman et al. as this study only reported figures for PPHN when it was a major cause of death; therefore, it was not suitable for meta-analysis alongside the non-comparable outcome of any PPHN (Gluckman et al., 2005). Therefore, all remaining studies in our primary meta-analyses used whole-body cooling using servo-controlled devices.
We performed further analyses to examine for associations between TH and PPHN within subgroups, however no significant associations were observed. Subgroup meta-analysis of RCTs performed in HICs (n = 5) showed a relative risk of PPHN with TH of 1.13 (95% confidence interval 0.78 to 1.64, I2 40.4%). Meta-analysis of the remaining two RCTs in low/middle income countries produced a relative risk of 1.06 (95% confidence interval 0.52 to 2.17, I2 65.3%). After exclusion of the single RCT of preterm babies (Faix et al., 2025), meta-analysis of the six studies of babies born ≥35–37 weeks gave a relative risk of 1.13 (95% confidence interval 0.78 to 1.64, I2 40.4%).
Examining the funnel plot of RCTs, there was a broadly symmetrical distribution of studies, with no studies outside the pseudo 95% confidence intervals, suggesting a lack of evidence for publication bias (Fig. 4).
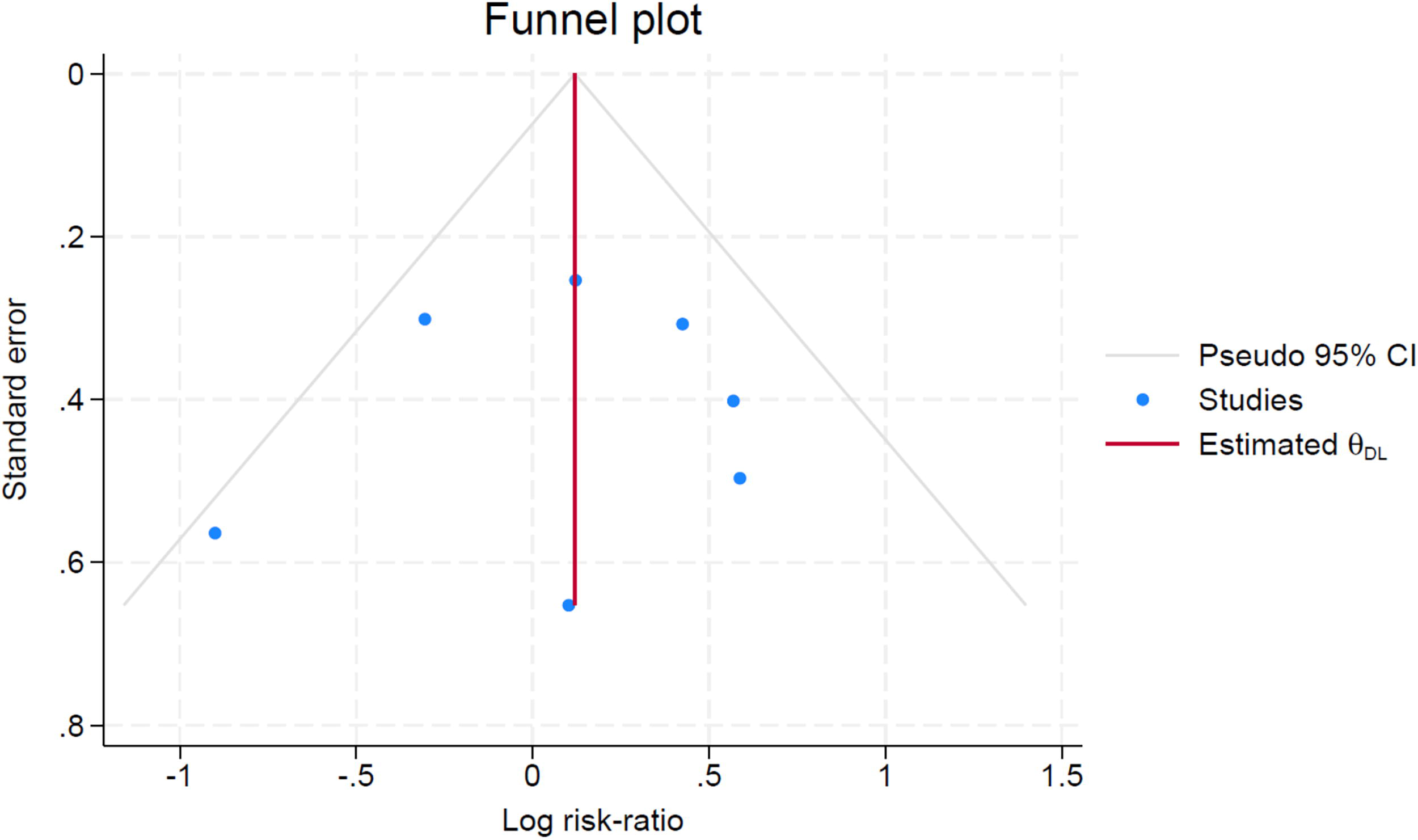
Funnel plot of randomized control trials (RCTs) of therapeutic hypothermia vs. normothermia for the outcome of persistent pulmonary hypertension of the newborn (PPHN).
Across observational studies, PPHN was not uncommon in both TH and NT groups. Studies showed 11% to 32% of infants with PPHN. Some studies found the same percentage of infants with PPHN in both TH and NT groups (Lakshminrusimha et al., 2018). Although PPHN was more common among infants receiving TH than those in the NT group in the Joanna R G et al., 2022 study, the opposite was found by Maoulainine et al.
Of note, among studies examining the more preterm population with HIE, the Herrera et al., 2018 cohort study of infants born at 33–35 weeks found that 23% of infants developed PPHN. The Faix et al. RCT of infants born at 33–35 weeks found a lower percentage with PPHN (5% to 6%), with no difference between the TH and NT groups. Rao et al. conducted a retrospective review of preterm infants (34–35 weeks) compared to term infants over 37 weeks with HIE who underwent TH. A greater proportion of preterm infants developed PPHN (19.4%) compared to 6.3% of term infants. From these preterm infants’ studies, there was no clear evidence that gestational age had any influence on development of PPHN in HIE infants undergoing TH.
Discussion
This systematic review was undertaken to assess the association between TH and PPHN. We performed a meta-analysis of seven RCTs and found no significant association between TH for HIE and PPHN. Despite the inclusion of several studies since the previous systematic review over a decade ago, there remains relatively limited data on the risk of developing PPHN among infants undergoing TH. In all the RCTs, the primary outcome was focused on death or neurodisability, whereas PPHN and the need for nitric oxide were considered as adverse events.
Most included RCTs did not designate PPHN as a primary outcome, leading to lack of consistent data collection regarding its diagnosis and management. The majority described it as an adverse outcome without clear diagnostic criteria, even inferring its presence purely by the administration of iNO. Some of the observational studies explained the diagnostic criteria of PPHN by clinical and/or echocardiography (Javed et al., 2025; Joanna R G et al., 2022; Rallis et al., 2024). Studies did not report whether PPHN occurred before, during or after the TH, neither did they classify the severity of PPHN, which limited interpretation of the review. Due to inconsistent PPHN definitions, meaningful clinical implications could not be drawn. Non-randomized and observational trials have also explored the association between TH and PPHN. There was considerable variability in the percentage of infants who developed PPHN. This variation may be due to differences in study settings, populations, and the definition of PPHN.
Only one RCT looked into preterm population (33–35 weeks) which found no statistically significant increase in PPHN among infants with HIE undergoing TH (Faix et al., 2025). Among observational studies, two studies included preterm gestation, but they showed conflicting outcomes of PPHN (Herrera et al., 2018; Rao et al., 2017). Preterm infants may have an increased risk of developing PPHN, although there was inadequate data to draw strong conclusions.
The majority of RCTs took place in high-income countries, although meta-analysis of this subgroup found no significant association between TH and PPHN. Two studies took place in middle/low-income countries: a single-center RCT by Rakesh et al. and the larger multicenter HELIX trial RCT, the latter of which suggested a greater percentage of infants with PPHN in the TH group compared to the NT group. However, this was not statistically significant either within the HELIX trial or meta-analysis of the two low/middle income RCTs. Of the two observational studies in low/middle income countries that compared between groups (Charki et al, 2020; Maoulainine et al., 2017), there was a suggestion of greater proportion of babies with PPHN among the NT group.
We observed moderate statistical heterogeneity (I2 28.5%) within our primary meta-analysis. Heterogeneity remained moderate even after subgroup analyses excluding RCTs from low-income countries or the RCT of preterm infants. However, the statistical heterogeneity may still have arisen from heterogeneity between trials of other clinical factors such as the reporting or diagnosis of PPHN.
As there is no strong association found in the meta-analysis of RCTs, we cannot conclude that evidence supports an association between TH and PPHN. The lack of association observed in RCTs may have arisen due to underpowered studies, inconsistent definitions, and PPHN outcomes. Furthermore, discrepancies in findings of observational studies were due to heterogeneity of studies, small sample sizes, and risk of bias. In view of this, we were unable to draw conclusions from the observational studies examined.
Based on the available evidence, there is no contraindication for TH in infants with perinatal asphyxia and PPHN, provided they positively respond to PPHN management. However, in individual cases of severe and rapid deterioration from PPHN, the benefits of TH should be weighed against the risk of complicated fatal course. High admission FiO2 or high oxygen requirement during early phase of hypothermia is an indicator of development of PPHN which needs immediate management (Joanna R G et al., 2022). Prompt evaluation of PPHN by echocardiography, initiation of inhaled nitric oxide and maintaining appropriate blood pressure to prevent these infants sliding into refractive pulmonary hypertensive crisis (Joanna R G et al., 2022). Studies have shown the importance of evaluation for right ventricular dysfunction on echocardiography which predicts the need for nitric oxide or ECMO (Abman et al., 2015; Richardson et al., 2017). Optimizing hemodynamics by maintaining adequate blood pressure to prevent right-to-left shunting will help to limit episodes of desaturations observed in rewarming phase (Gagnon and Wintermark, 2016).
Strengths
This is the first systematic review and meta-analysis focusing specifically on the incidence of PPHN as a primary outcome in infants who underwent TH for HIE. Only RCTs were included and non-RCTs were excluded in the final analysis.
By restricting meta-analyses to RCTs, this review attempts to minimize confounding and strengthen causal inference where possible.
This study includes RCTs and observational data from both high and low-resource settings, increasing external validity and global applicability.
This review highlights a notable deficiency in the homogenous reporting and diagnosis of PPHN, setting a foundation for more standardized research protocols in the future.
Limitations
There was substantial variation in how PPHN was defined across the studies.
Given that PPHN was often a secondary or safety outcome, many studies were underpowered to detect meaningful differences in PPHN incidence between TH and NT groups.
Future Work
A large multicenter data evaluation is required to identify the incidence of PPHN in infants undergoing TH so appropriate safety measure can be recommended. Establishing international registries to enable consistent multinational large-scale data collection could significantly enhance the potential for predictive models including artificial intelligence, and real-time clinical decision support tools.
Conclusion
To conclude, PPHN during TH in infants with HIE is a perilous complication that requires prompt intervention. Our systematic review found no evidence of an association between TH and PPHN in infants with moderate to severe HIE. Infants needing high oxygen requirements will require prompt assessment for PPHN, so it can be managed with appropriate escalation of care. This could involve prompt evaluation of PPHN through echocardiography, initiation of inhaled nitric oxide and maintaining appropriate blood pressure to prevent these infants from slipping into refractory pulmonary hypertensive crisis.
Authors’ Contributions
H.G. conceptualized the idea. R.J. and H.G. did the screening of articles separately from search results. Any disputes were resolved with discussion. R.J. wrote the initial draft. T.J.V.H. performed statistical analyses. N.R. performed critical appraisal. All the authors have been involved in developing the methodology and protocols, writing and editing of this article, and reviewing all drafts before submission.
Footnotes
Acknowledgment
The authors sincerely thank to Mr. Philip O’Reilly, librarian at UHB, for conducting the literature search.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
T.J.V.H. (NIHR Academic Clinical Lecturer) is funded by the National Institute for Health Research. The views expressed in this publication are those of the authors and not necessarily those of the NIHR, NHS or the UK Department of Health and Social Care.
Ethics Approval
Ethical approval was not required for this systematic review. The authors have followed PRISMA reporting guidelines.
Data Sharing Statement
The raw data from the systematic review and meta-analysis may be provided upon reasonable request to the corresponding author.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.