
Abstract

Valid, reliable, and timely screening and assessment strategies are critical to center the experiences of adolescents and young adults (AYAs) and ensure they get the quality care they need and deserve. The National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines for AYA Oncology recommend screening AYAs with cancer for a variety of complex issues including treatment, fertility, reproductive endocrine and sexual health, psychosocial and behavioral factors, and genetic risk assessment. 1 The NCCN guidelines and the Alberta Health Services (AHS) Guideline Resource Unit-Clinical Practice Guidelines state that, at the time of diagnosis or intake, a comprehensive, multidimensional initial assessment of AYA-specific challenges should be completed and documented. Additionally, the AHS guidelines specify that AYA-specific screening and reassessment should be documented regularly to account for the fluidity of AYAs’ needs and particularly at times of transition (e.g., change in treatment, end of treatment).
Operationalizing Guidelines in Screening and Assessment
AYA oncology programs often assume the role of coordinating and augmenting existing services and resources available in oncology clinical care. 2 This requires identifying AYAs’ individual needs and connecting them with referrals or resources that address those needs. In this context, it is helpful to distinguish between initial screening and triage and a more in-depth assessment of issues within any given health-related quality of life domain. The AYA oncology program staff will likely assume responsibility for the initial screening process. A more in-depth assessment may fall to the various specialists to whom an AYA is referred. For example, initial screening may identify needs related to physical function, resulting in referral to a physical therapist. The physical therapist may then assess physical function in more detail to inform treatment options. In some instances, the AYA team may assume responsibility for the more in-depth assessment if the team is comprised of relevant expertise. For example, psychosocial issues identified via screening may be further assessed by an AYA team social worker. Below, we have focused on the initial screening and triaging of needs (i.e., needs assessment) as this is a critical piece of AYA cancer care, which is most often facilitated by the AYA team.
Needs assessment tools
The objective of a needs assessment is to identify and connect AYAs to the services and resources they might need. While screening for specific psychosocial needs may be common (e.g., depression, anxiety, general distress, fatigue),3–6 AYAs often have multiple, interrelated physical, psychosocial, and practical challenges that merit a broad-based approach. 7 Implementing a standardized, multidimensional screening tool can ensure that patient needs are assessed comprehensively and systematically. Such tools have been developed specifically for the AYA population. For example, Patterson et al. adapted the NCCN Distress Thermometer and Problem List to create the AYA Psycho-Oncology Screening Tool (AYA POST), which has since been validated with an international sample of newly diagnosed AYAs.8,9 AYA POST includes a global rating of distress, followed by a problem checklist, which includes physical, emotional, practical, social, and information needs. Similarly, Haines et al. developed the AYA Needs Assessment and Service Bridge (NA-SB), a 57-item measure which assesses AYAs’ unmet needs across nine domains. 10 A subsequent pilot study suggested that NA-SB is feasible, acceptable, and appropriate to implement from both the patient and provider perspectives and useful in identifying and addressing AYAs’ unmet needs. 11 It is preferable to implement a needs assessment tool that has demonstrated feasibility, validity, or other supporting evidence (e.g., AYA POST or NA-SB); however, AYA programs may have institutional resource constraints, or their AYA patient population may have unique needs. Such programs may benefit from tailoring existing strategies to optimize an “in-house” needs assessment tool. For example, AYA programs might consider drawing from existing patient-reported outcome measures validated among AYAs and identifying those health-related quality of life domains that matter most to their patients.12–14 The chosen needs assessment tool should be tailored to AYA-specific challenges and comprehensive of the full constellation of physical, practical, and psychosocial needs that AYAs experience during and after cancer treatment.15,16 To promote equitable cancer care delivery among AYAs, needs assessments should be inclusive of items related to social determinants of health, social risk factors, and social needs.17,18
Administering needs assessment tools
Administering needs assessments in routine cancer care presents several logistical challenges. 19 Extant studies have disagreed on the optimal approach for administration in terms of electronic versus paper delivery and in the clinic versus outside of the clinic. 20 Maximizing the patient-level reach may require a flexible approach to administration, in which AYAs are asked to complete the needs assessment at multiple time points through multiple platforms. For example, an AYA might be prompted to complete a needs assessment prior to an upcoming appointment via a patient portal message. If incomplete, they might be approached again in the clinic with an iPad and asked to complete it then. Text-based approaches may also be considered. Moreover, a needs assessment should be administered at multiple time points during a patient’s cancer trajectory to account for the dynamism of needs; this requires the establishment of structured intervals for reassessment.
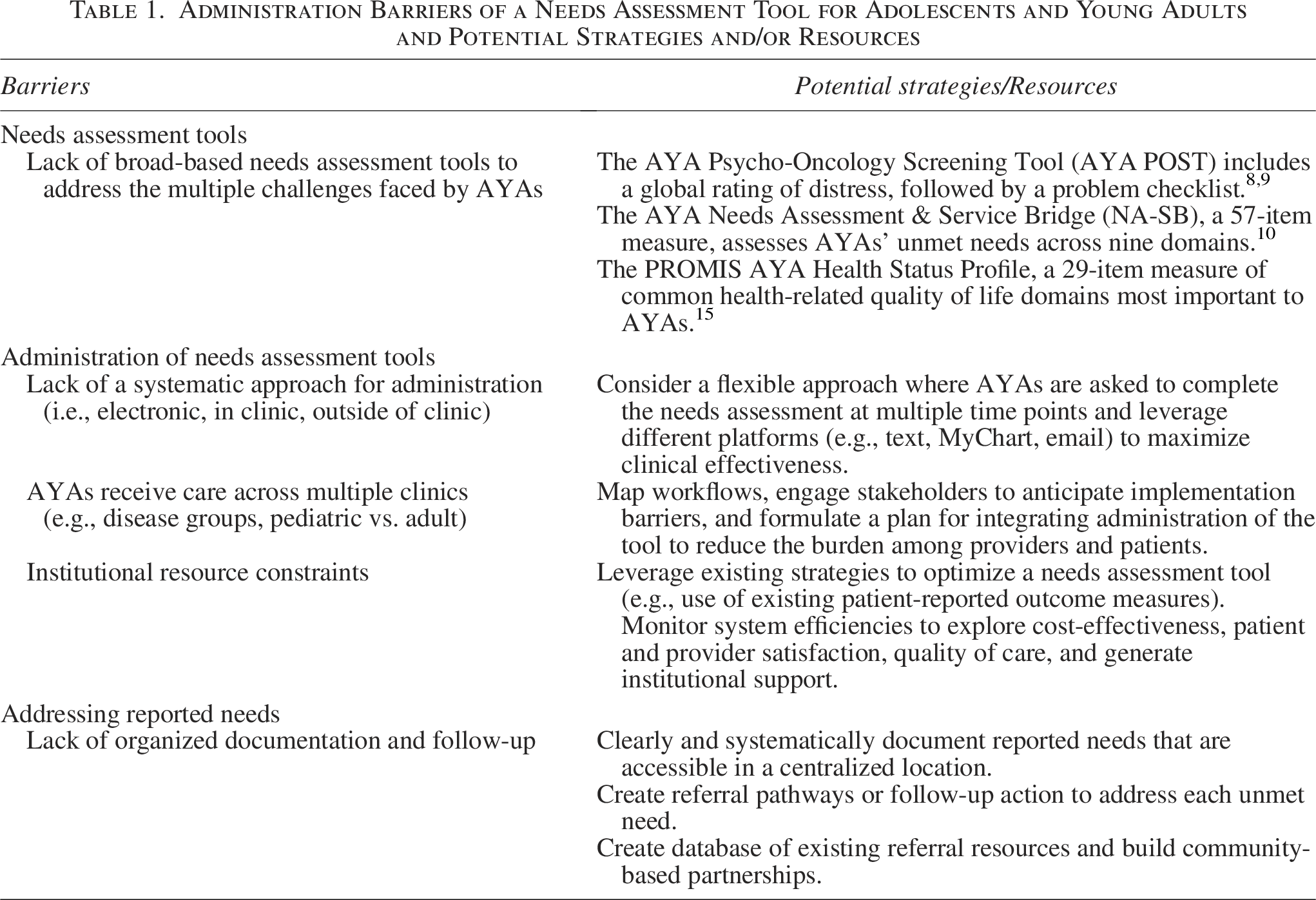
There are unique barriers to implementing a needs assessment for AYAs. AYAs receive care across pediatric and adult oncology clinics, and across various disease groups, all of which have their own idiosyncratic workflows and documentation systems. Integrating a needs assessment tool across all settings is challenging, and sensitivity must be taken to minimize redundancy with other clinic-specific screening efforts. AYA programs should consider mapping existing workflows and engaging with key stakeholders to anticipate implementation barriers. With this information, they can then formulate a plan for integrating the administration of a needs assessment tool such that it is minimally burdensome to both providers and patients. Table 1 presents potential strategies and resources for overcoming potential challenges.
Administration Barriers of a Needs Assessment Tool for Adolescents and Young Adults and Potential Strategies and/or Resources
Addressing reported needs
After administration of a needs assessment, robust processes for following up on reported needs are critical to improving cancer outcomes and equity. Needs assessment data must be systematically documented in a centralized location accessible to the providers tasked with addressing unmet needs. Each need assessed must have a corresponding referral pathway or follow-up action to address the need. Creating a detailed catalogue of existing services and resources available either in-house or through community partnerships can inform the identification of such referral pathways. Some studies have explored the automation of referrals. 21 However, responding to unmet needs often requires dedicated personnel to triage, refer, and ensure that services and resources are received.
There are resources to guide AYA programs in establishing processes to follow up on reported needs. CanTeen created an AYA Psychosocial Care Manual (https://www.canteen.org.au/health-education/measures-manuals/aya-oncology-psychosocial-care-manual), which provides guidance on how to create a care plan based on responses to the AYA POST. Likewise, NA-SB pairs a needs assessment with integrated referral pathways; Haines et al. recommend that, prior to implementing NA-SB, institutions tailor the map of referral pathways to resources available in their own setting.
Call to Action
AYAs experience many unmet needs during and after cancer treatment. Their needs are individual, multidimensional, and they fluctuate as AYAs move through their disease trajectory. Given that unmet needs are associated with a number of negative outcomes (e.g., psychological distress), holistically assessing and addressing AYAs’ needs at the individual level represents an important piece of care delivery for this population; this can be done through the implementation of a multidimensional and patient-centered needs assessment tool paired with robust processes for following up on reported needs. In addition to better addressing AYA needs at the individual level, implementing a standardized needs assessment approach can provide data to illuminate the most pressing needs for a given patient population and existing gaps in institutional service and resource capacity to address those needs.