
Abstract

Introduction
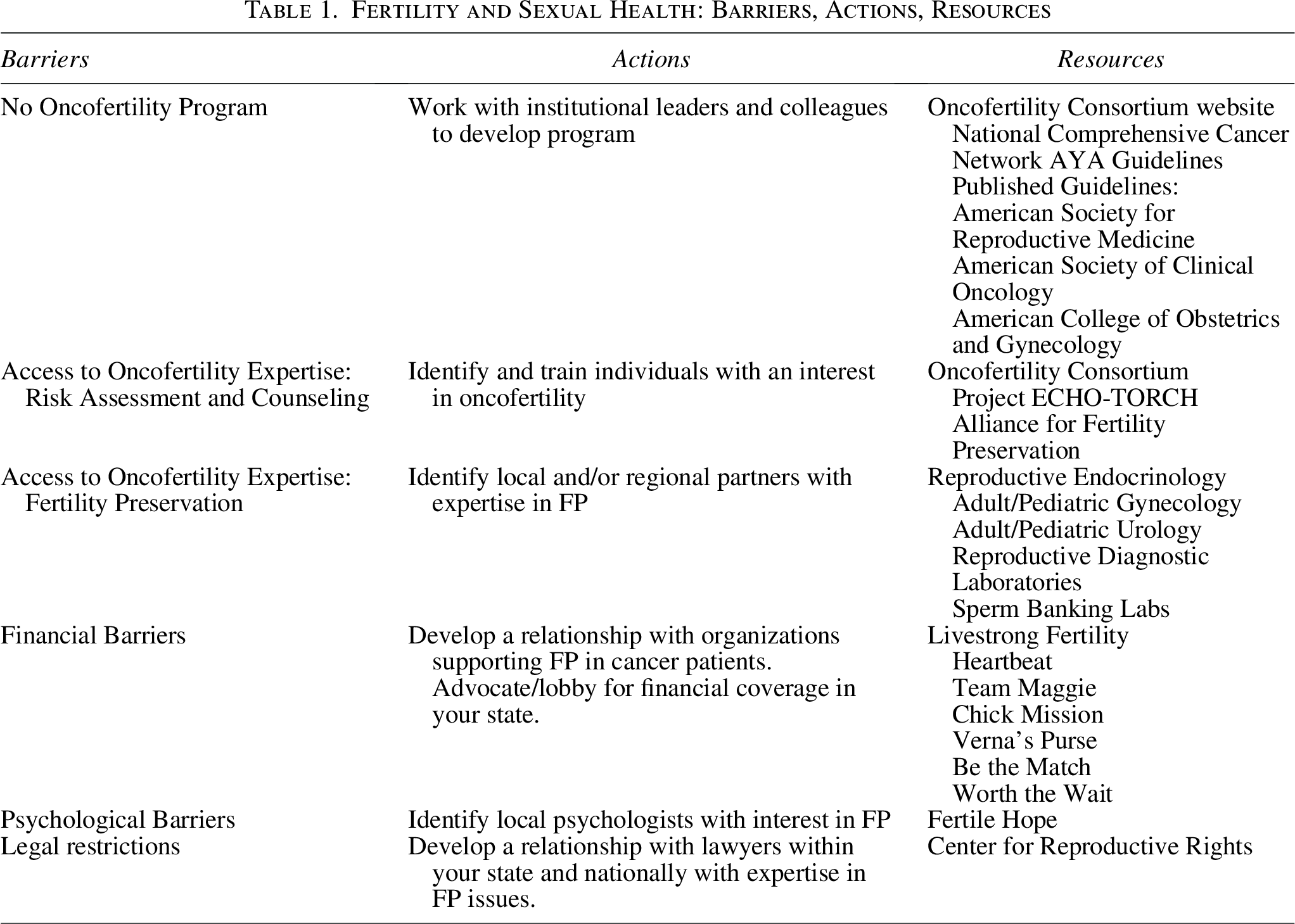
Fertility preservation (FP) has been identified as an important issue for both male and female survivors of adolescent and young adult (AYA) cancer. 1 Several cooperative groups have published position statements and guidelines supporting the importance of risk assessment and counseling regarding FP for cancer patients, including the American Society of Clinical Oncology and American Society of Reproductive Medicine.2,3 In addition, the sexual health needs of AYA cancer patients are often unaddressed, both during and after treatment. Issues relating to contraception and sexual dysfunction are critical to patients in this age group and are routinely not addressed by oncology providers. All AYA programs must be prepared to address these critical issues and provide patients with access to resources to support their choices and overcome barriers in these areas (Table 1).
Fertility and Sexual Health: Barriers, Actions, Resources
Factors influencing fertility risk include sex and pubertal status, the type of chemotherapy used, the total dose of alkylating chemotherapy agents (expressed as cyclophosphamide equivalent dose), the dose and location of radiation therapy, and impact of surgery on reproductive organs and brain. The Pediatric Initiative Network of the Oncofertility Consortium has published risk stratifications for both male and female cancer patients. 4 See Figure 1 for females and Figure 2 for males.

Female risk stratifications. Risk stratifications for females, published by the Pediatric Initiative Network of the Oncofertility Consortium. Note. See Meacham LR, et al. Standardizing risk assessment for treatment-related gonadal insufficiency and infertility in childhood, adolescent, and young adult cancer: the Pediatric Initiative Network risk stratification system. J Adolesc Young Adult Oncol. 2020 Dec;9 (6):662–6.
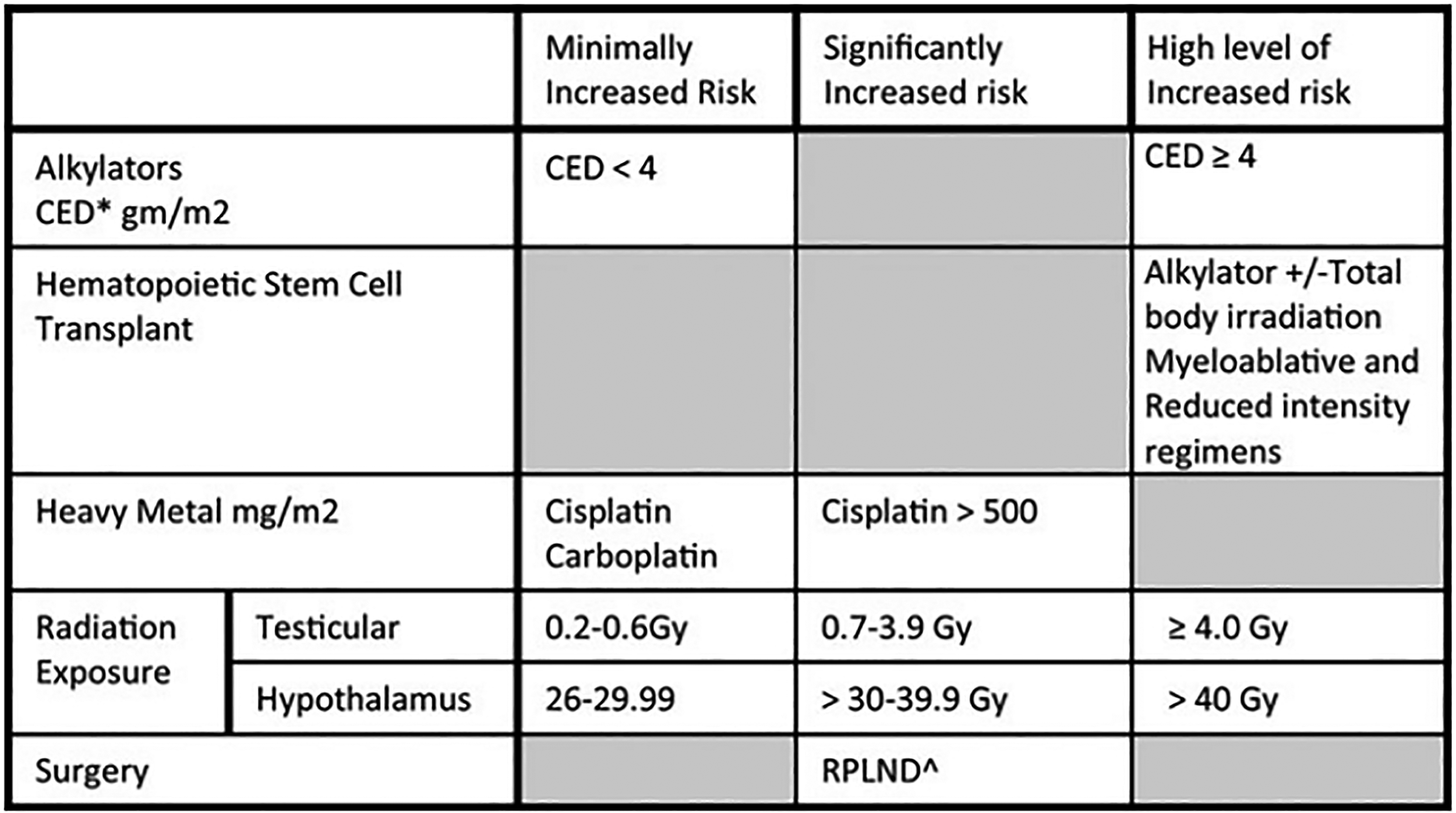
Male risk stratifications. Risk stratifications for males, published by the Pediatric Initiative Network of the Oncofertility Consortium. Note. See Meacham LR, et al. Standardizing risk assessment for treatment-related gonadal insufficiency and infertility in childhood, adolescent, and young adult cancer: the Pediatric Initiative Network risk stratification system. J Adolesc Young Adult Oncol. 2020 Dec;9 (6):662–6.
Optimally, referral and counseling regarding fertility risk and FP should be done prior to the start of therapy.
FP Options
Females
Accepted methods of FP in females include embryo cryopreservation, mature oocyte cryopreservation, ovarian tissue cryopreservation, and ovarian transposition. An oncofertility program should be able to offer rapid access to these services. Also, because embryo and mature oocyte cryopreservation require ovarian stimulation, and time is important in most cancer cases, access to reproductive endocrinologists with experience in immediate or random start ovarian stimulation is critical. The use of GnRH agonists for ovarian suppression has not definitively been shown to protect fertility but can be offered if other alternatives are not available to a patient.
Males
Sperm cryopreservation (sperm banking) for FP should be offered to all pubertal and peri-pubertal males, preferably prior to the initiation of chemotherapy. In cases where samples cannot be obtained through masturbation due to medical or psychosocial impediments, interventions such as vibratory stimulation, electro-ejaculation, urinary sperm retrieval (for retrograde ejaculation), or Testicular Sperm Extraction or Aspiration should be considered. Testicular tissue cryopreservation is currently the only available option for prepubertal boys and can be considered in the AYA population in certain instances. It is experimental, however, and should not be performed outside of a clinical trial. GnRH agonists have not been shown to have utility for FP in men and should not be considered.
In addition to pretreatment counseling, post-treatment monitoring of gonadal and hormonal function should be offered throughout the survivorship continuum as prompt consultation and intervention for post-treatment FP should occur with any concern for gonadal function decline or impending failure. 5 Ongoing medical management and hormone replacement therapy may be required. Finally, programs should provide access to counseling for issues related to FP, including mental health, genetics (in particular as it relates to preservation of embryos, tissue, or gametes for patients that have or could have a cancer predisposition syndrome or other inheritable diseases), and financial support.
Sexual interest in AYA patients has been shown to be similar to that among age-matched peers, and prior work has suggested that less than half of sexually active patients used contraception, making it critical that providers serving this population discuss contraceptive use as part of their counseling.6,7 Chemotherapy can negatively impact the health of both the patient and the fetus in pregnant female cancer patients.8–11 In addition, due to their immunocompromised state, AYAs may be more susceptible to sexually transmitted infection. 12 Unfortunately, there are no definitive guidelines for contraception in cancer patients available. 13 In general, long-acting reversible contraceptives, such as IUDs and birth control implants, have excellent efficacy (99%) in preventing pregnancy and require little effort on the part of the patient. Care must be taken during patient selection to avoid complications of insertion, such as bleeding or infection. Oral contraceptives are also over 90% effective, but higher estrogen products should be avoided due to the risk of venous thromboembolism in cancer patients. Similarly, the added risk of osteopenia/osteoporosis caused by depot medroxyprogesterone in an already high-risk population makes this a method that should only be considered on a case-by-case basis. Other methods, such as vaginal rings or hormonal patches may also be considered for pregnancy prevention. Condoms are the best method to prevent STIs for both male and female cancer patients, as well as the primary method to prevent pregnancy for male cancer patients
The AYA period typically encompasses many developmental milestones that contribute to psychosexual development, including intimacy and relationships, body image, and sexuality, among others. A significant portion of AYA childhood cancer survivors have perceived a negative impact of their diagnosis and treatment on their sexual lives.14–16 Furthermore, prior research has shown an estimated 20–50% of survivors report symptoms of sexual dysfunction, including issues with arousal, desire, interest, orgasm, other physical problems, including pain, challenges in their relationships, and sexual satisfaction.17–19 Females are more likely than males to report sexual problems.20–22
While the provision of information regarding sexual health is important in this population, health care providers typically do not address sexual function. 23 Providers have cited concerns regarding timing of when to have these conversations, lack of knowledge regarding the topic, challenges in facilitating these conversations, and an inability to provide sufficient informative resources as reasons for this.24,25 AYA preferences for conversations regarding sexual function include having patient-provider rapport, having ongoing, personalized conversation, and the utilization of screening tools to facilitate conversation and notification prior to engaging in these conversations. 26 Importantly, intervening with education may be helpful in alleviating distress and improving body image, 27 and recommendations regarding interventions for sexual problems in people with cancer have been published, 28 though further investigation in this unique population is needed.
Footnotes
Acknowledgment
The authors would like to acknowledge the following individuals who assisted in the preparation of this article: Lindsay Frazier, Amy Kimble, Jennifer Lischwe, James Ludemann, and Sara Meehan.
Author Disclosure Statement
The authors have no financial or personal interests to disclose.
Funding Information
This project was supported by Faculty Affairs and the Department of Psychosocial Services at St. Jude Children’s Research Hospital (SJCRH). Support to SJCRH is provided by the American Lebanese Syrian Associated Charities (ALSAC).