
Abstract

Cancer-directed treatment innovations have improved our ability to diagnose, treat, and offer long-term survival to adolescent and young adult (AYA) cancer patients; however, many people with cancer do not benefit equally from these advances. Health care disparities in certain populations of interest include AYAs (age 15–39 years) as well as ethnic, sexual, and gender minorities and rural residents. Furthermore, within the AYA cancer population, disparities exist based on place of residence, insurance status, SES, sex, gender orientation, race, and ethnicity, all of which compound the differences in outcomes for these underrepresented minorities.1,2 Data show that inequities in health care exist across the entire cancer care continuum (CCC) from diagnosis to survivorship and span medical treatment, supportive care as well as survivorship care. 3
For AYAs, cancer care delivery is influenced by numerous factors unique to the patients’ developmental stage, psychosocial and economic status, and cancer subtype. Efforts to address these outcome disparities must be innovative and multilevel, including patient, provider, and institutions, and global, in part because AYAs are geographically dispersed and mobile. Since most AYAs treated for cancer are expected to become long-term survivors, the financial and survivorship ramifications of cancer can also persist for decades. 4
Guidelines
There is an urgent need to develop and test effective strategies and multilevel interventions targeted to reduce current disparities in access, quality, and care for all AYAs with cancer. Policy Statement/Guidelines have been published by ASCO, NCCN, COG, and AACR over the last decade and provide guidance to institutions and providers to adapt their services toward AYA cancer patients’ needs.5–8 In order to address the disparity in outcomes seen in the AYA population, dedicated AYA programs are emerging throughout the country; however, not every institution or practice has the capability to form these multidisciplinary programs.9,10
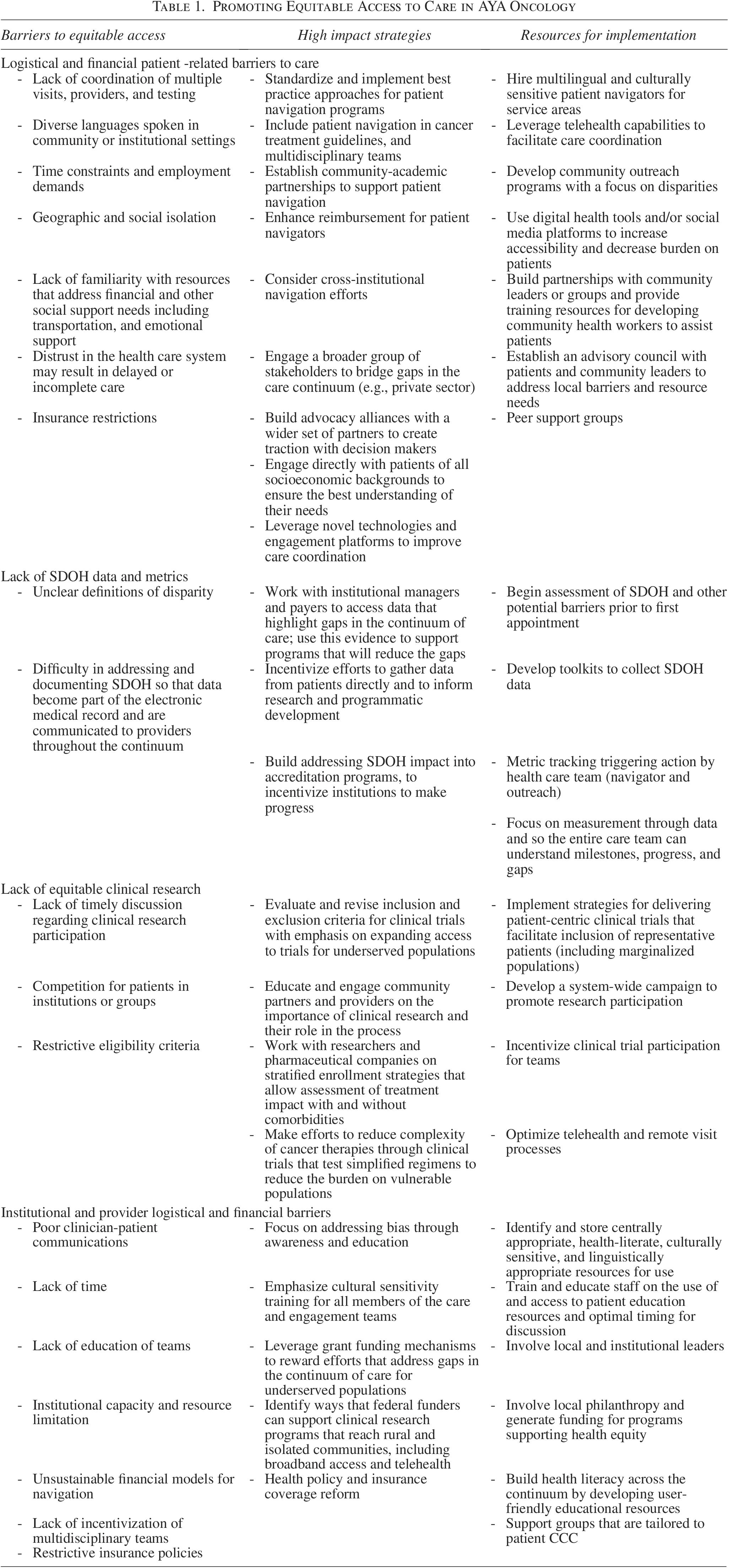
Even though these guidelines exist, a framework must be developed to integrate them into AYA programs and institutional standards of care. There is not a standard pathway for practitioners and multidisciplinary teams to implement strategies in their practice; however, there are existing high-impact practices utilized by some programs to improve care delivery for marginalized populations. These interventions can be at various levels, including patients, providers, institutional, or systems, and in various domains, including cancer-directed care, research, supportive care, and survivorship (see Table 1). Examples of some areas in which innovative strategies are being utilized by programs include community engagement, patient advocacy, patient navigation, incentivization to improve clinical trial enrollment, virtual support groups, peer groups, and creating education and awareness tools regarding resources among patients and these disparities among providers.11–13
Promoting Equitable Access to Care in AYA Oncology
Barriers to AYA care delivery
There are various critical system-level barriers, such as limited reimbursement, lack of administrative resources and support, and time available to spend with patients, that impede implementation of strategies to optimize AYA care delivery across the CCC. These include institutional and provider-level barriers such as weak financial models for navigation programs, competition for patients in institutions, restrictive eligibility on trials, lack of research metrics and reimbursement barriers, and difficulty in recording social determinants of health. Patient level barriers such as low health literacy, diverse languages spoken in community or institutional settings requiring multilingual navigators; geographic and social isolation within underserved communities; lack of familiarity with resources that address financial and other social support need, distrust in the health care system, which may result in delayed or incomplete care; and time constraints and employment demands also impact implementation of interventions to enhance care delivery.14–16
Recommendations
Because of the complexity of U.S. health care, a collaborative approach is needed to address disparities along the CCC, including systematic changes that can provide harmonized care to address barriers within each domain while helping implement programs that bridge care from one domain to the next. 17 Some high-impact strategies are described in Table 1. Of note, some interventions are also desired at the level of health policy reform to address the need for adequate insurance coverage and increase focus on social determinants of health in cancer care. For example, specific recommendations include extending current health insurance and enhancement initiatives to state and federal levels, adequate reimbursement of navigation services, and securing higher reimbursement rates for clinicians caring for these populations.18–23
In conclusion, to target the well-being of specific marginalized populations, we need to consider their individual needs and coordinate a collaborative and convenient plan to deliver cancer-directed treatment and promote global health and wellness. Using evidence-based responses, the health care system must be flexible in supporting AYAs through cancer-directed treatment, prevent adverse events of treatment, and facilitate engagement in long-term survivorship or palliative care. This can be done by being deliberate about collecting the most informative data, leveraging existing resources and structures within the institution and community, leveraging community partnerships, appealing for health care system change, and collaboratively developing viable interventions to optimize equitable, superior cancer care.
Footnotes
Acknowledgment
Sandra Jones APN, St Jude’s Children’s Research hospital and Lindsay Klosterkemper, Msc, Dana Farber Cancer Institute, Boston.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.