
Abstract
Advancements in cancer research, treatment protocols, and supportive care interventions have contributed to an increasing population of adolescent and young adult cancer survivors (AYA-CS). Impaired cardiorespiratory fitness is a key modifiable risk factor in AYA-CS, linked to several conditions, in particular cardiovascular disease. This scoping review describes and synthesizes previously published data that has documented the cardiorespiratory fitness in AYA-CS. Secondary objectives were to synthesize the assessment methodologies used to measure cardiorespiratory fitness and to explore whether exercise interventions improve AYA-CS fitness. CINAHL, EMBASE, MEDLINE, and SPORTDiscus were systematically searched from [28/02/2025]. Original articles that assessed cardiorespiratory fitness in AYA-CS (aged between 15 and 39 at the time of cancer diagnosis and had completed treatment) were eligible. A total of 3049 articles were identified from the database search. After screening, 10 studies were included, representing 494 participants (59.7% female). AYA-CS exhibit markedly reduced cardiorespiratory fitness with peak oxygen uptake values 20–47% below healthy controls when measured via cardiopulmonary exercise test. There was wide variability in both the measures used to assess cardiorespiratory fitness and the types and mode of prescribed exercise interventions. Exercise interventions were primarily individualized and aerobic, demonstrating good feasibility and high acceptability among AYA-CS. This scoping review highlights that AYA-CS experience persistent impairments in cardiorespiratory fitness post-treatment. Future research is required to standardize fitness assessment measures, establishing cardiorespiratory fitness norms to help guide clinical interventions and the development of targeted interventions aimed at improving fitness and health outcomes.
Keywords
Introduction
Each year, around 1.2 million adolescent and young adults (AYA), between the ages of 15 and 39, are diagnosed with cancer worldwide.1,2 Advancements in cancer research, treatment protocols, and supportive care interventions have contributed to an increasing population of adolescent and young adult cancer survivors (AYA-CS), with 5-year survival exceeding 80%.1,3 Despite these improvements in survival, many AYA-CS experience long-term consequences as a result of their cancer treatment. Two out of every three will experience a late effect, and one in four faces severe or life-threatening complications. 4 Compared with healthy peers, AYA-CS have an increased risk of multimorbidity, including hypertension, diabetes, obesity, poor physical and mental health, secondary cancers, and more than a 2-fold increased risk of cardiovascular disease.5–8 Cardiovascular disease is among the most debilitating late effects experienced by AYA-CS and is a leading cause of nonrelapse-related morbidity and mortality in this population.6,9–14 There are multiple factors that contribute to this risk, including cancer treatments, in particular anthracycline chemotherapies, poor health behaviors such as low levels of physical activity (PA), and impaired cardiorespiratory fitness.13–16
Impaired cardiorespiratory fitness is of particular interest in AYA-CS, as it represents a potentially modifiable risk factor that is linked to cardiovascular disease, death from cancer, and overall cancer-related mortality.17–20 Furthermore, insufficient cardiorespiratory fitness has been linked to the development of multimorbidity, including conditions such as metabolic syndrome, type 2 diabetes, and hypertension.14,17–20 PA and exercise interventions in cancer survivors have been shown to mitigate treatment-related late effects, reduce the risk of developing multimorbidity and cancer recurrence, and improve overall survival.21–26 As such, cardiorespiratory fitness is vitally important for AYA-CS, especially considering that fitness naturally declines with age.27,28
In view of these risks, early identification of functional impairments, along with individualized interventions, may mitigate adverse effects and improve long-term health outcomes in AYA-CS. It is crucial, therefore, for clinicians and researchers to accurately measure and assess cardiorespiratory fitness in this population. The cardiorespiratory impairments observed in AYA-CS, the methods of assessment, and characteristics of exercise interventions aimed at improving cardiorespiratory fitness have not been comprehensively explored in AYA-CS.29–31 This scoping review aims to provide a descriptive summary of the existing evidence on cardiorespiratory fitness impairments in AYA-CS, while identifying critical areas for further research.
Review Question
The primary objective of this scoping review was to describe the cardiorespiratory fitness of AYA diagnosed with cancer at various time points post-treatment completion. The secondary objectives were to synthesize the assessment methodologies used to measure AYA-CS cardiorespiratory fitness and the types and characteristics of exercise interventions used to improve cardiorespiratory fitness.
Methods
This review was guided by the Joanna Briggs Institute’s framework for scoping reviews, with the review protocol registered on Open Science Framework on the 17th of September 2024 (https://doi.org/10.17605/OSF.IO/A59YG). 32 The study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews checklist for conducting and reporting study findings. 33
Search strategy
The comprehensive search strategy was developed by the authors in collaboration with a medical librarian. Search terms included both database-specific Medical Subject Headings (MeSH) terms and keywords encompassing the concept, context, and population (Table 1). The systematic search was performed on 28th February 2025 in the following electronic databases: CINAHL, EMBASE, MEDLINE, and SPORTDiscus. The search covered literature published between January 2000 and February 2025.
Combination of Database-Specific MeSH Terms and Keywords
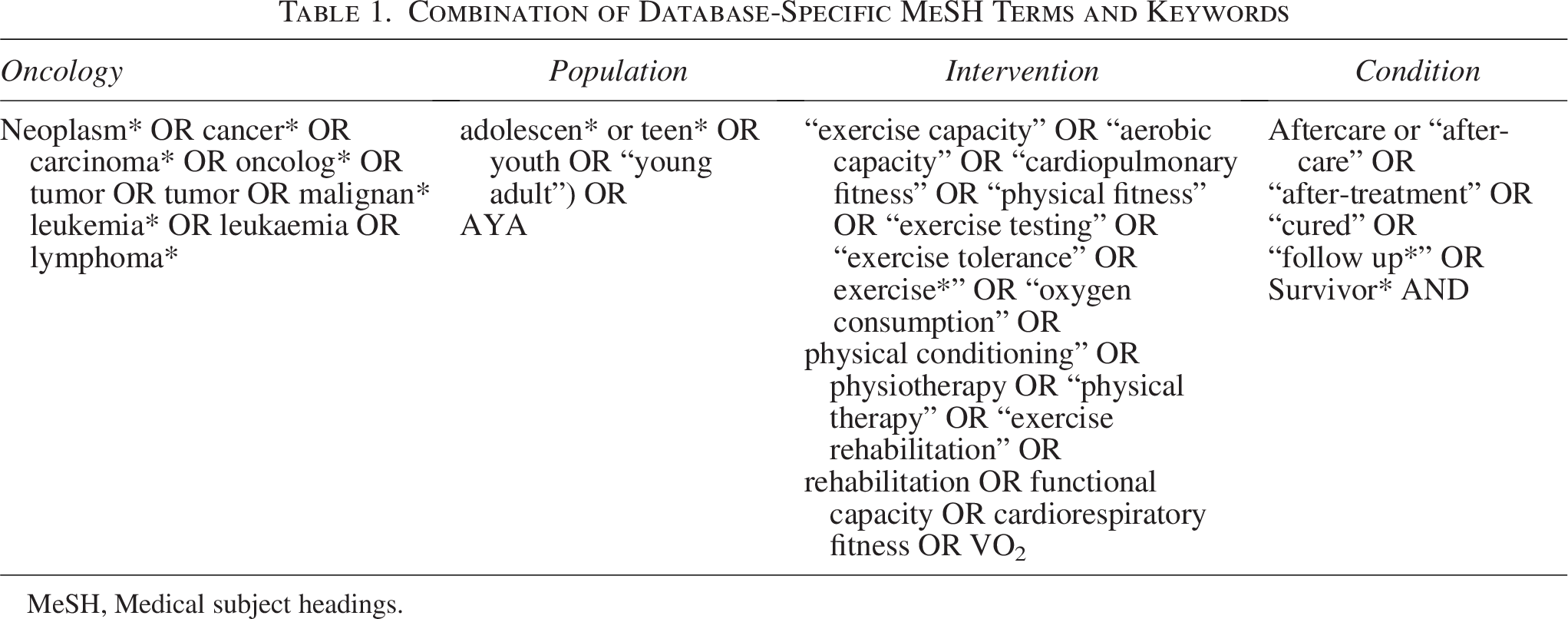
MeSH, Medical subject headings.
Study eligibility criteria
Original articles that assessed cardiorespiratory fitness in AYA-CS, who were aged between 15 and 39 at the time of cancer diagnosis and had completed treatment, were eligible for inclusion. Cardiorespiratory fitness is defined as the body’s ability to perform whole-body, large-muscle exercise at moderate to high intensity for an extended period of time. 34 Other terms used to describe cardiorespiratory fitness include cardiorespiratory endurance, functional capacity, aerobic fitness, and aerobic capacity, among others. Various methods are used to measure cardiorespiratory fitness, including maximal tests conducted in a laboratory, such as cardiopulmonary exercise test (CPET), maximal oxygen uptake (VO2max) and submaximal tests conducted in the field, such as the six-minute walk test (6MWT).35,36 Studies using any test that provided an objective measure of cardiorespiratory fitness were included. Additional eligibility criteria were papers written in the English language and published in a peer-reviewed journal between January 2000 and February 2025 to reflect modern cancer treatment and health care. This timeframe aligns with the growing AYA oncology movement and the increasing focus on survivorship care for young adults with cancer.37–40
Studies were excluded if the fitness assessment did not objectively measure cardiorespiratory fitness, for example, assessments of muscular power or strength, gait analysis, balance, agility, flexibility, or measures of self-reported fitness. Conference abstracts, case studies or reports, meta-analyses, systematic and scoping reviews, thesis publications, protocol papers, and letters to the editor were also excluded. Studies involving both adult and pediatric participants (with a mean age outside the specified age range) were included only if data were analyzed or presented separately for AYA participants. In cases of mixed diagnosis (cancer and noncancer) or mixed treatment status (on-treatment and post-treatment), studies were included if >75% of participants had a cancer diagnosis or were post-treatment, or if study findings were presented separately for these groups.
Study selection
All articles identified during the systematic search were uploaded to EndNote (Version 21) where duplicates were removed by bibliographic software and then manually checked by one reviewer (A.M.). The remaining records were transferred into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia, accessed via Deakin University, available online at www.covidence.org) to facilitate the selection process.
Initially, one reviewer (A.M.) independently assessed study titles, keywords, and abstracts for full-text review. Relevant full-texts were reviewed by two reviewers (A.M. & SF) to confirm eligibility using the same standardized approach. Any conflicts were discussed between the two reviewers to reach a consensus. Finally, the reference lists of included studies were manually reviewed to identify any additional articles.
Data extraction and presentation
The lead author (A.M.) extracted data from all included articles, which was then verified by a second author (S.F.F.). To address the primary objectives of this review, the following information was extracted: authors, publication year, country; design; sample size; cancer diagnosis; subjects’ age at time of diagnosis; current age; time since treatment completion; sex/gender; test measure and protocol; fitness level results and comparisons to healthy controls (Table 2). We did not differentiate between sex and gender, as authors did not always specify which one was assessed.
Summary of the Study Characteristics, Measures of Cardiorespiratory Fitness, and Fitness Level of AYA-CS
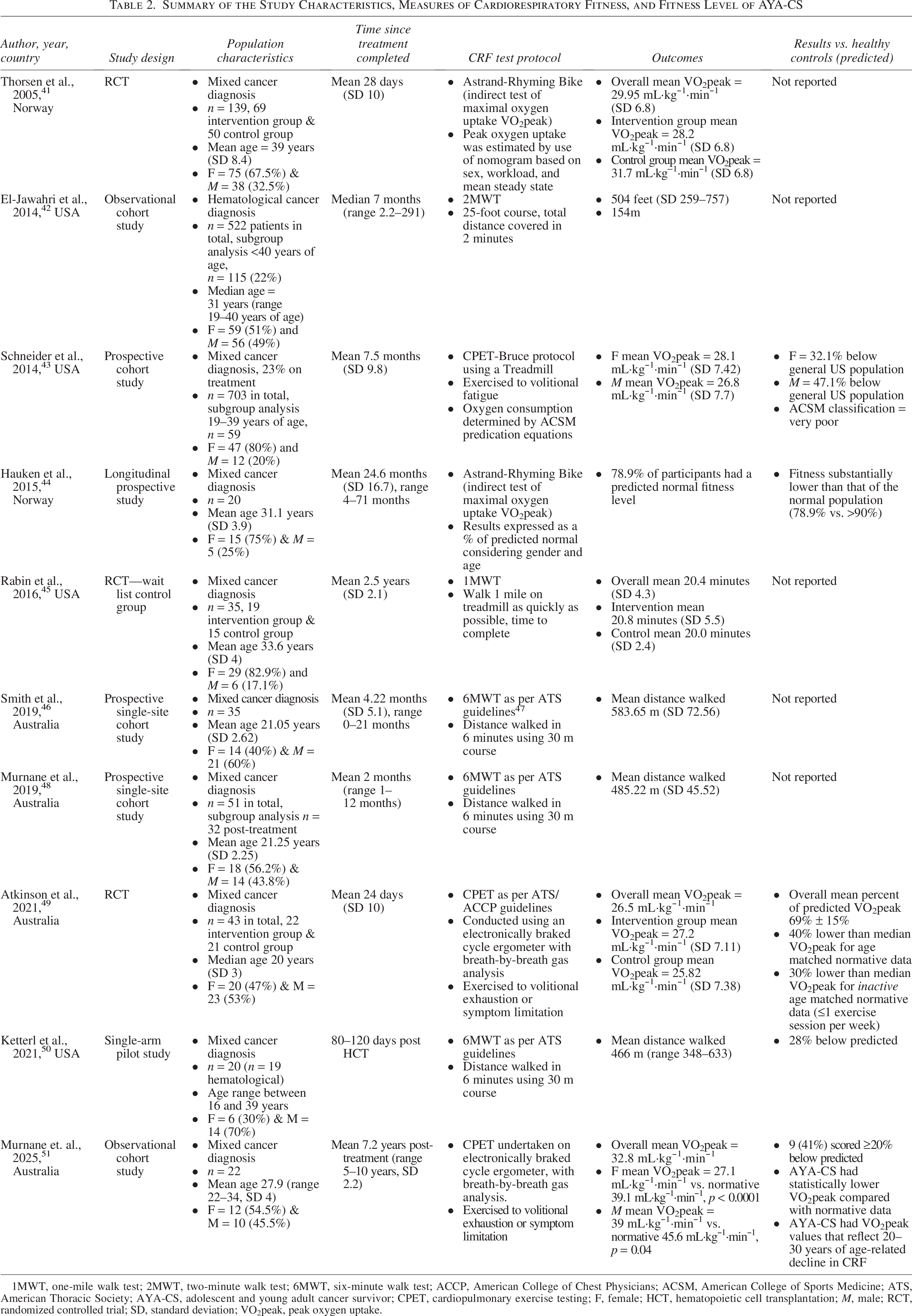
1MWT, one-mile walk test; 2MWT, two-minute walk test; 6MWT, six-minute walk test; ACCP, American College of Chest Physicians; ACSM, American College of Sports Medicine; ATS, American Thoracic Society; AYA-CS, adolescent and young adult cancer survivor; CPET, cardiopulmonary exercise testing; F, female; HCT, hematopoietic cell transplantation; M, male; RCT, randomized controlled trial; SD, standard deviation; VO2peak, peak oxygen uptake.
To meet our secondary objectives, data were extracted on exercise intervention features and aims; including location, frequency, intensity, type, duration, progression; control condition if applicable; adherence and compliance with interventions; follow-up assessments time-points; and outcomes/results (Table 3).
Summary of the Intervention Characteristics That Aimed to Improve Cardiorespiratory Fitness in AYA-CS
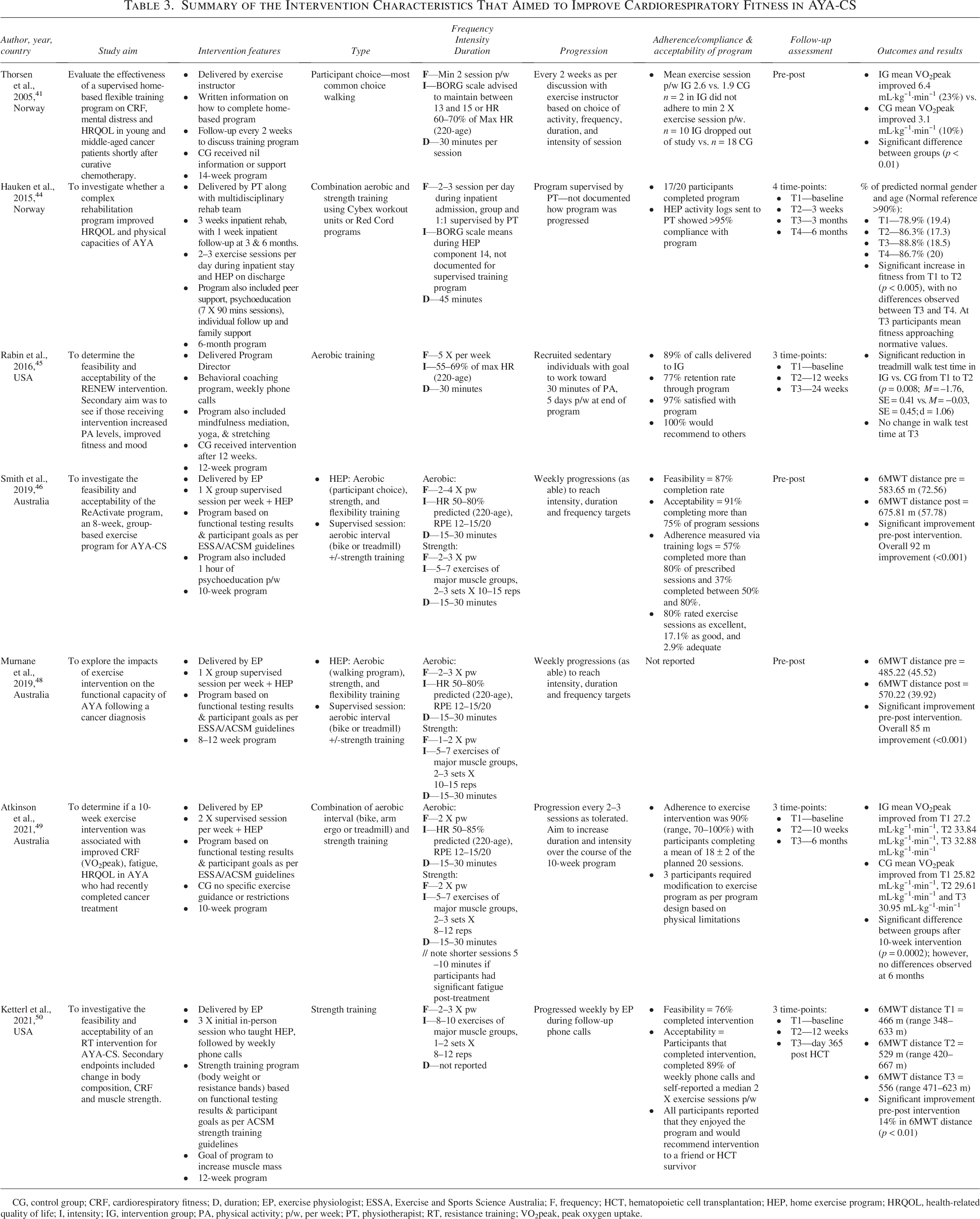
CG, control group; CRF, cardiorespiratory fitness; D, duration; EP, exercise physiologist; ESSA, Exercise and Sports Science Australia; F, frequency; HCT, hematopoietic cell transplantation; HEP, home exercise program; HRQOL, health-related quality of life; I, intensity; IG, intervention group; PA, physical activity; p/w, per week; PT, physiotherapist; RT, resistance training; VO2peak, peak oxygen uptake.
Quality appraisal
Consistent with the Joanna Briggs Institute methodology for scoping reviews, no formal quality appraisal or risk of bias assessment of included studies was undertaken. The purpose of this review was to map and summarize the existing evidence related to cardiorespiratory fitness in AYA-CS, rather than evaluate methodological quality of individual studies.
Results
Search strategy and study selection
The search yielded 3049 articles, and after removing duplicates, 2190 articles underwent abstract and title screening (Fig. 1). Following title/abstract screening, 2142 articles were excluded, leaving 48 for full-text review. Ten articles met the eligibility criteria and were included in the scoping review.
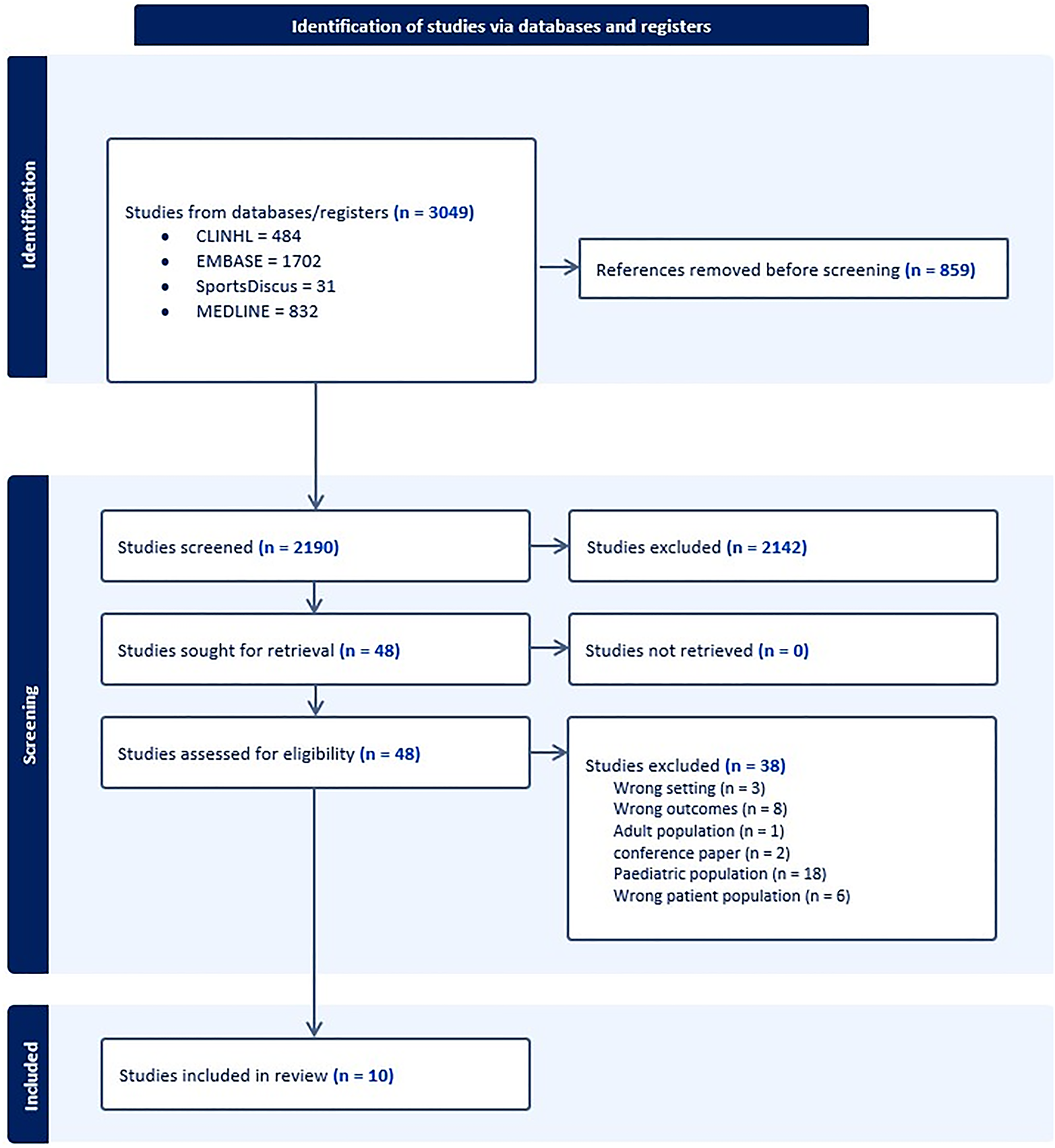
Preferred Reporting Items forSystematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-SCR) flow diagram.
Characteristics of included studies
The characteristics of the 10 included studies are summarized in Table 2. These studies comprised two randomized controlled trials (Thorsen et al., 2005; Atkinson et al., 2021), one randomized controlled trial with a wait list control (Rabin et al., 2016), three prospective cohort studies (Schneider et al., 2014; Murnane et al., 2019; Smith et al., 2019), one longitudinal prospective study (Hauken et al., 2015), one single-arm pilot study (Ketterl et al., 2021), and two observational cohort studies (El-Jawahri et al., 2014; Murnane et al., 2025).41,45,49,52–58
In total, 494 post-treatment AYA-CS (59.7% female) were included across the studies, with time since treatment completion ranging from 1 month to 10 years. All studies involved a mix of cancer diagnoses, except for one study that included participants with hematological malignancies only (El-Jawahri et al., 2014). Three studies provided subgroup analysis based on age at diagnosis or post-treatment status (El-Jawahri et al., 2014; Murnane et al., 2018; and Schneider et al., 2014). Seven of the 10 studies included measurements of cardiorespiratory fitness as part of an intervention aimed at improving functional capacity, initiated between 28 days and 2.5 years post-treatment completion (Thorsen et al., 2005; Hauken et al., 2015; Rabin et al., 2016; Smith et al., 2018; Murnane et al., 2019; Atkinson et al., 2021; Ketterl., 2021).
Assessment measures of cardiorespiratory fitness
Among the 10 studies included in this review, three used the 6MWT to measure cardiorespiratory fitness (Smith et al., 2019; Murnane et al., 2019; Ketterl et al., 2021). Three other studies performed a maximal CPET to measure peak oxygen uptake. Of these, two used a cycle ergometer, with breath-by-breath analysis (Atkinson et al., 2021; Murnane et al., 2025), while the third study used the Bruce treadmill protocol (Schneider et al., 2014). Two studies assessed fitness using the Astrand 6-minute cycle test, a submaximal test that provides an estimate of oxygen uptake (Thorsen et al., 2005; Hauken et al., 2015). In addition, one study measured fitness using the two-minute walk test (El-Jawahri et al., 2014), and another performed the one-mile walk test (Rabin et al., 2016), which requires participants to walk 1 mile on a treadmill as quickly as possible.
Cardiorespiratory fitness level
Across studies, mean peak oxygen uptake (VO2peak) values in AYA-CS ranged from 26.5 to 32.8 mL·kg−1·min−1, representing approximately 20–47% lower fitness than age- and sex-matched healthy controls.45,53,55 Fitness-level comparisons with healthy controls (Table 2) were reported in five studies (Schneider et al., 2014; Hauken et al., 2014; Atkinson et al., 2021; and Ketterl et al., 2021; Murnane et al., 2025). CPET showed significant deconditioning in AYA-CS with VO2peak scores considerably lower than normative data. Schneider et al. (2014) recorded VO2peak values that were classified as “very poor” per American College of Sports Medicine guidelines, with significant differences in female (26.1 mL·kg−1·min−1 vs. 36.1 mL·kg−1·min−1, p < 0.0001) and male AYA-CS (26.8 mL·kg−1·min−1 vs. 43.3 mL·kg−1·min−1, p < 0.0001). 55 Atkinson et al. (2021) recorded a mean VO2peak of 26.5 mL·kg−1·min−1 within 2 months post-treatment, 53 approximately 30% lower than sedentary peers (men 46.9 ± 9.1 mL·kg−1·min−1; women, 36.7 ± 7.71 mL·kg−1·min−1) and more than 40% below healthy noncancer controls (54 ± 8. mL·kg−1·min−1 for men; 42.9 ± 7.6 mL·kg−1·min−1 for women).43,53 Similar findings were seen in Murnane et al. (2025), with AYA-CS recording VO2peak lower than normative data (female: 27.1 vs. 39.1 mL·kg−1·min−1, p < 0.0001; male: 39.7 vs. 45.6 mL·kg−1·min−1, p = 0.04), equating to 20–30 years of age-related decline. 45
Submaximal measures (Astrand 6-minute cycle test and 6MWT) further revealed significant deficits in AYA-CS. The mean distance walked in the 6MWT ranged from 466 to 584 m, which is considerably lower than the predicted distances for healthy individuals.41,56,57 For example, Ketterl et al. (2021) reported a mean distance of 466 meters (348 m to 633 m), which was 28% below predicted values reported for males 638 meters (SD, 44 m) and females 593 meters (SD, 57 m). In addition, the Astrand cycle test showed scores 21% below predicted normal values for age and gender.41,58 For studies that did not compare outcomes with normative values or a control group, values reported were consistent with other studies in this review and would therefore be considered low.
Interventions and impact on cardiorespiratory fitness
All exercise interventions in the included studies resulted in improvements in cardiorespiratory fitness, with primary outcomes measured by VO2peak, 6MWT distance, or time (Table 3). Atkinson et al. (2021) and Thorsen et al. (2005) observed a 21% and 23% improvement in VO2peak, respectively. Similarly, Smith et al. (2019), Murnane et al. (2019), and Ketterl et al. (2021) reported significant increases in 6MWT distance ranging from 63 to 92 meters improvement. Notably, the exercise program reported in Ketterl et al. (2021) focused on strength training, yet it significantly improved walk distance by 14%, suggesting that strength-based interventions even without an aerobic training component can lead to improvements in cardiorespiratory fitness among AYA-CS.
Rabin et al. (2019) reported a significant reduction in treadmill walk test time (p = 0.008), while Hauken et al. (2015) reported significant improvements in physical fitness, nearing normative values, even for individuals who were, on average, 2 years post-treatment completion. Four studies (Hauken et al., 2015; Rabin et al., 2016; Atkinson et al., 2021; Ketterl et al., 2021) assessed cardiorespiratory fitness longitudinally . Both Hauken et al. (2015) and Atkinson et al. (2021) reported significant increases in cardiorespiratory fitness during the supervised phase of the exercise program, followed by nonsignificant declines at 6-month follow-up. Atkinson et al. (2021) found a significant difference between the exercise and control groups at the end of the 12-week intervention (p = 0.0002), that was not maintained at 6 months, suggesting that the exercise program may have accelerated recovery. In contrast, Rabin et al. (2016) and Ketterl et al. (2021) demonstrated significant improvements in cardiorespiratory fitness from preintervention to postintervention, but no significant changes were observed at subsequent follow-up.
Key features of the exercise intervention
Four studies (Hauken et al., 2015; Smith et al., 2019; Murnane et al., 2019; Atkinson et al., 2021) delivered exercise interventions that incorporated both aerobic and strength training, tailored to the individual needs based on the results of functional testing . These interventions included supervised in-person sessions along with an independent home exercise program. Hauken et al. (2015) employed the most intensive model, incorporating a 3-week inpatient rehabilitation program, with 2–3 daily sessions, followed by 1-week follow-ups at 3 and 6 months. The other three studies (Smith et al., 2019; Murnane et al., 2019; Atkinson et al., 2021) featured interval training as a central component of the exercise program during the supervised sessions.
Ketterl et al. (2021) focused solely on strength training, beginning with three supervised sessions with an exercise physiologist before transitioning to a home-based exercise program with weekly phone reviews. The interventions in Thorsen et al. (2005) and Rabin et al. (2016) focused on behavior change, providing participants with exercise information, guidance, and advice on how to complete a home exercise program. Although there were no supervised sessions, participants had weekly or fortnightly follow-ups with the research team to discuss their progress and adapt the program as indicated. Participants in Thorsen et al. (2005) were free to choose their PA (commonly walking), while Rabin et al. (2016) recruited sedentary individuals with the aim to undertake 30 minutes of aerobic exercise, 5 days per week.
There was considerable variability in training protocols across studies in terms of frequency, intensity, and duration. The frequency of sessions ranged from 2 to 5 times per week, lasting 15–60 minutes. For aerobic training, intensity was typically prescribed at 50–85% of predicted max heart rate [formula %Max HR = (220-age)] or monitored using the Borg Rating of Perceived Exertion scale (12–15/20; somewhat hard, hard). 48 Regarding strength training, most programs instructed participants to complete 5–7 exercises targeting the major muscle groups, undertaking 2–3 sets of 8–15 repetitions, 1–3 times per week (Smith et al., 2019; Murnane et al., 2019; Atkinson et al., 2021). Ketterl et al. (2021) focused exclusively on strength training, with participants performing 8–10 bodyweight or resistance band exercises, performed in 1–2 sets of 8–12 repetitions.
Adverse events, feasibility, and acceptability of interventions
The available evidence regarding adverse events associated with fitness testing and interventions is limited and only reported in three studies (Atkinson et al., 2021; Ketterl et al., 2021; and Murnane et al., 2025). None of the three studies reported adverse events due to the exercise interventions, although Atkinson et al. (2021) and Murnane et al. (2025) observed six minor (grade 1) adverse events during CPET.
In terms of feasibility, adherence to the interventions was generally high across studies, with completion rates exceeding 70% in cases where reported (Table 3). Monitoring methods included follow-up calls (e.g., Rabin et al., 2016) and exercise logs (e.g., Hauken et al., 2015; Ketterl et al., 2021). Regarding acceptability, programs that incorporated personalized support, such as phone coaching or in-person supervision, reported greater participant satisfaction.
Discussion
The aim of the present review was to summarize and describe published data on cardiorespiratory fitness in AYA-CS post-treatment. The findings provide preliminary evidence that AYA-CS experience significant deficits in cardiorespiratory fitness compared with healthy controls. Notably, structured interventions were shown to significantly improve cardiorespiratory fitness levels in AYA-CS. However, this review also underscores the considerable variability in both the measures used to assess cardiorespiratory fitness and the types and modalities of exercise interventions.
Across the studies reviewed, the consistent finding was that AYA-CS exhibited markedly reduced cardiorespiratory fitness when assessed by various tests, including CPET, and submaximal measures such as 6MWT and Astrand 6-minute cycle test. Notably, findings from Schneider et al. (2014), Atkinson et al. (2021), and Murnane et al. (2025) stand out, as they utilized gold-standard CPET to measure fitness which highlighted that VO2peak values were 20–47% below healthy controls.45,53,55 These findings are consistent with existing literature on other cancer population groups, in particular pediatric survivors, and underscore the long-term consequences of cancer treatment, specifically chemotherapy and radiotherapy, which are known to contribute to deconditioning, and a marked reduction in cardiorespiratory fitness in these population groups.44,46,50,55 Moreover, AYA-CS also demonstrated deficits on submaximal assessments, with performances on tests such as the 6MWT and cycling capacity falling below normative values, further underscoring the significant impairments in physical functioning within this group.
This diminished cardiorespiratory fitness observed in AYA-CS likely stems from a combination of factors related to cancer treatment (e.g., chemotherapy-induced fatigue, muscle wasting/deconditioning, and cardiotoxicity) and the general sedentary lifestyle that may follow cancer treatment.14,17,42,51,59 This trend has been observed in previous studies, which report that only 30% AYA-CS meet the recommended exercise guidelines.59,60 While some degree of deconditioning is expected after the acute phase of treatment, the extent of these impairments on cardiorespiratory fitness suggests that more targeted and structured interventions are required to address these deficits. Such interventions should be incorporated into standard care practices, aimed not only at improving fitness but also at enhancing the overall health and well-being of AYA-CS long-term.
The gold-standard measure of cardiorespiratory fitness is via CPET, which assesses functional capacity including cardiac, pulmonary, vascular, and muscle aspects in the measure (VO2max or VO2peak).61,62 However, CPET is not routinely used in AYA-CS due to several factors, including limited availability, time constraints, the need for specialized clinician expertise, and cost. As a result, alternative tests are often employed in research and clinical settings to assess cardiorespiratory fitness. The validity of these alternative assessment measures varies, with each providing differing levels of accuracy in estimating true cardiorespiratory fitness.63,64 While CPET remains the gold standard due to its direct measurement of VO2peak, submaximal tests such as the Astrand cycle test and the 6MWT provide indirect estimates that, although strongly correlated with VO2peak, can be influenced by participant motivation and musculoskeletal limitations.63,65,66 Despite these limitations, such tests demonstrate good predictive validity and reproducibility in both cancer and noncancer populations and therefore represent practical and feasible alternatives when CPET is not possible.64,66,67 Accordingly, the variability in assessment methods observed across studies likely reflects a balance between methodological rigor and practical feasibility, with the 6MWT emerging as the most applied approach.
From a practical standpoint, incorporating fitness assessments into clinical follow-up requires feasible, standardized, and resource-appropriate approaches. Submaximal or field-based tests such as the 6MWT, step tests, or shuttle walk test can be conducted in outpatient or community settings by trained allied health professionals, requiring minimal equipment and time.36,64 Embedding these assessments into annual survivorship reviews or during routine cardiovascular screening may help identify AYA-CS with impaired cardiorespiratory fitness who could benefit from tailored exercise interventions.
Moving forward, it is essential for clinicians and researchers in this field to standardize assessment measures where possible. Doing so will provide the ability to establish reference norms for assessment and enhance comparability across studies and settings. While we recommend the use of CPET when accessible, there is significant potential for researchers to develop reference norms for simpler assessments such as the 6MWT. These reference data would help clinicians more effectively assess cardiorespiratory fitness, identify survivors at risk of cardiovascular disease, and guide exercise prescription for AYA-CS. Notably, research in childhood cancer survivors has already established reliable reference equations for the 6MWT that correlate well with VO2peak, though further efforts are needed to expand these findings to AYA-CS populations and to establish global reference standards. 66
All exercise interventions reviewed in this study aimed at improving cardiorespiratory fitness in AYA-CS showed positive outcomes, but they varied significantly in terms of how they were delivered (e.g., supervised or home-based) and timing when delivered (24 days to 2.5 years). Due to differences in the functional assessments used, and the types of exercise interventions implemented, it is difficult to make specific recommendations regarding the optimal type, mode, duration, frequency, intensity, or timing post-treatment to implement exercise programs, as noted in previous reviews.26,29,30 However, two key findings emerged. First, a slight decline in fitness or no further improvement was observed after the exercise intervention ended, whether in studies with in-person sessions or those using home-based programs with telephone follow-up. To address this, future interventions should incorporate strategies to sustain cardiovascular fitness after the intervention ceases, such as ongoing remote monitoring, regular assessments, or maintenance programs to prevent declines in fitness once structured sessions cease.
Second, there was a notable lack of reporting on adverse events that may have occurred during cardiorespiratory fitness testing or the interventions. Only two studies explicitly stated that no serious adverse events occurred during the exercise interventions, while Atkinson et al. (2021) and Murnane et al. (2025) reported six minor adverse events during CPET. 53 Moving forward, it is essential for clinicians and researchers working with AYA-CS to consistently document and report adverse events using checklists such as exercise-related harms. 68 This will help ensure that exercise programs are not only effective but also safe. Despite the limited reporting of adverse events, the exercise interventions overall demonstrated good feasibility and acceptability, with personalized interventions, support, and regular monitoring contributing to high adherence and participant satisfaction. These factors should be considered when designing future exercise-based interventions.
Beyond the underreporting of adverse events, a closer examination of methodological quality reveals several additional limitations across studies. Few studies provided adequate detail on intervention fidelity or the implementation procedures, and reporting on adherence, compliance, and program progression was inconsistent. Future research would benefit from using established reporting frameworks, such as the Consensus on Exercise Reporting Template or the TIDieR checklist to enhance methodological transparency and reproducibility.69,70
This review highlighted several important considerations for clinical practice and future research. There is a pressing need to better understand the underlying mechanisms contributing to fitness decline in AYA-CS, particularly the interplay between treatment-related factors (e.g., chemotherapy) and lifestyle-induced factors such as sedentary lifestyle. Identifying biomarkers of deconditioning across multiple systems, including muscular, cardiovascular, metabolic and neurological, could pave the way for more personalized interventions and improve outcomes for this vulnerable population.71,72
There is also a clear need for targeted exercise interventions that address the unique challenges faced by AYA-CS. Personalized exercise prescription that integrates both aerobic and resistance training appears to be the most effective in improving cardiorespiratory fitness and functional capacity. Although most interventions incorporated aerobic training, few explicitly examined the effects of resistance training. This represents a critical gap, given the well-documented muscle loss and treatment-induced sarcopenia observed in AYA patients.45,73 Evidence from Ketterl et al. (2021) suggests that strength-focused interventions can elicit meaningful improvements in cardiorespiratory fitness. 41 Future studies should therefore investigate optimal resistance training protocols, either alone or in combination with aerobic exercise, to better understand their impact on long-term health and survivorship outcomes.
Research is also needed to establish the optimal dosages of exercise (frequency, type, duration, and intensity) for this population. In addition, the ideal timing of intervention, whether implemented during the early post-treatment phase or at long-term follow-up, remains uncertain. Identifying strategies that help sustain these benefits over time is equally important. Possible approaches may include continued monitoring, booster sessions, or hybrid models that combine in-person and remote support, offering practical and scalable solutions for diverse populations. Further work is also needed to establish the most appropriate methods for assessing fitness in AYA-CS, to integrate these assessments into routine follow-up care, and to develop reference norms for fitness testing in this group. Implementing these measures will equip clinicians with better tools to identify patients at risk of deconditioning or cardiovascular disease, enabling timely interventions to mitigate these risks before adverse outcomes occur.
Study limitations
Despite the contribution this scoping review provides to understanding cardiorespiratory fitness in AYA-CS post-treatment, several limitations to our study are noted. Limitations include the broad scope of the review and the MeSH search criteria, which may have led to the exclusion of relevant articles. In particular, those that did not clearly define cardiorespiratory fitness or rehabilitation. Second, the heterogeneity across studies in how cardiorespiratory fitness was measured, along with differences in intervention types and delivery modes, complicated the ability to provide robust recommendations for assessing fitness and implementing effective interventions in AYA-CS. Finally, due to resource limitations, title and abstract screening was conducted by a single reviewer, raising the possibility some relevant articles were not identified. 74 We acknowledge this as a limitation and have thoroughly documented our process, adhering to the established inclusion and exclusion criteria during this review.
Conclusion
This scoping review highlights the significant deficits in cardiorespiratory fitness among AYA-CS compared with healthy controls and the potential of exercise interventions to mitigate the functional decline observed in this population. This review identified a lack of standardized measures for assessing fitness, along with considerable variability in exercise interventions across studies, making it challenging to provide clear recommendations for optimal exercise prescription for AYA-CS. Future research should focus on refining intervention dosages, mode of delivery, as well as developing cardiorespiratory fitness reference norms for AYA-CS. Low cardiorespiratory fitness is a modifiable risk factor for cardiovascular disease; however, it is not routinely screened in AYA-CS, and future work should look into routine screening of this in follow-up care for patients. A deeper understanding of the mechanisms underlying fitness decline is essential to ensure that exercise programs are safe, feasible, and effective for this population. Finally, while exercise interventions show promise, strategies to enhance long-term adherence and sustain the benefits of improved fitness are needed.
Authors’ Contributions
All authors conceived the study design. A.M. and S.F.F. performed the literature search and study selection. A.M. completed the data extraction from the included articles, and S.F.F. verified this information. A.M. interpreted the data. All the authors contributed to the writing of the article and have read and approved the final version of the article.
Footnotes
Acknowledgment
The authors thank Ramona Naicker (Scholarly Services Librarian, Deakin University) for her contributions to the review and refinement of their search strategies.
Author Disclosure Statement
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Funding Information
A.U. was supported by a Victorian Cancer Agency fellowship. No other funding was received for conducting this study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.