
Abstract
Purpose:
High symptom burden and poor prognosis faced by adolescents and young adults (AYAs; aged 15–29) with advanced or recurrent cancer significantly impact their sense of identity and purpose as they work to achieve developmentally significant goals. The combination of high symptom burden and goal interference may exacerbate suffering, yet palliative care interventions have not addressed the co-occurring symptom management and existential concerns of this population.
Methods:
Guided by the NIH Stage Model, we systematically developed a psychosocial symptom management intervention to address the needs of AYAs with advanced or recurrent cancer. Quantitative and qualitative data were obtained from AYAs (N = 20) and caregivers (N = 13) who completed semi-structured interviews and self-report measures to assist with intervention development of refinement. Rapid qualitative analysis was used.
Results:
Intervention development interviews confirmed high symptom burden and the need to develop a psychosocial symptom management intervention targeting this population. A four-session intervention (“SMILE:
Conclusions:
SMILE is a novel integration of three evidence-based approaches to provide AYAs skills to address symptoms that interfere with valued and meaningful action. The feasibility and acceptability of SMILE will next be examined in a pilot randomized controlled trial.
Keywords
Introduction
In the United States, >30,000 adolescents and young adults (AYAs) aged 15–29 are diagnosed with cancer annually.1,2 Improvements in morbidity and mortality outcomes for AYAs have lagged behind those for younger pediatric and older adult patients with cancer, and AYAs are more likely to present with advanced disease, have more aggressive tumors, and have worse prognosis.3–9 As a result, AYAs often have high symptom burden (e.g., pain, fatigue, emotional distress), with >90% endorsing distressing symptoms during treatment and nearly half experiencing ≥3 symptoms.10–12 These symptoms are often interrelated and co-occur,13–15 with patients reporting a median of four symptoms toward the end-of-life. 15
For AYAs, the diagnosis of cancer occurs in the early stages of adult life, a critical developmental period when they are working to achieve complex, age-related goals such as completing their education, building their career, and fostering relationships.16–19 AYAs may experience changes in identity and life purpose as the goals they had been pursuing are made more difficult or impossible by their diagnosis, treatment, symptom burden, and poor prognosis. The age-related challenges of AYAs with cancer are particularly pronounced for those with advanced disease. In an effort to prolong life, AYAs with advanced cancer often choose aggressive treatments that result in additional side effects and lower quality of life. 20 They must cope with high symptom burden and living with a life-limiting illness while their peers are establishing autonomy and building their futures. In contrast, AYAs with advanced cancer often experience a loss of independence as they increasingly rely on others for physical, emotional, and financial support, 21 and assistance with symptom management.22,23 The combination of high symptom burden and challenges to achieving developmental milestones may exacerbate suffering,24,25 yet the unique, age-related needs of AYAs with advanced cancer often go unrecognized.
It is recommended26–28 that AYAs with advanced cancer have routine access to palliative care interventions to assist with symptom management and improving quality of life.29,30 However, AYAs are underserved in palliative care, and the integration of palliative care with standard treatment remains suboptimal for AYAs.13,27 Adult palliative care services primarily treat older patients; thus, most psychosocial symptom management interventions have been tested among patients aged ≥ 40.31–34 Pediatric palliative care services are often focused on patients aged < 15;22,27 providers may be less familiar and/or comfortable delivering services to AYAs, and referral to palliative care for AYA patients remains low. 28 To address this gap, AYA-specific palliative care interventions are needed to facilitate symptom management and target the unique needs of this population.
Informed by the NIH Stage Model, 35 our objective was to systematically develop and refine the first psychosocial intervention targeting the unique symptom management needs and existential concerns of AYAs with advanced or recurrent cancer. It was hypothesized that an intervention integrating traditional behavioral symptom management strategies with key skills and concepts from two evidence-based therapies, Meaning-Centered Psychotherapy (MCP)33,36,37 and Acceptance and Commitment Therapy (ACT),38,39 would be beneficial.12,40,41 Traditional behavioral symptom coping strategies, such as relaxation training and activity pacing, are widely accepted within palliative care as efficacious42–47 but are still relatively novel within AYA oncology and may be valuable tools for promoting self-management of physical and emotional symptoms. Both MCP and ACT have been associated with decreased distress and symptom burden and improved quality of life among patients with cancer, including those with advanced cancer,37,45,48–53 though their use among AYAs with advanced cancer has also been limited. Concepts from MCP and ACT are complementary in their focus on engagement in values-congruent meaningful action. MCP33,36,37,50 focuses on identifying sources of meaning in one’s life and working to actively engage with and build meaning. ACT38,39 involves techniques to gain helpful perspective on uncomfortable thoughts and physical and emotional experiences rather than working to change their content or frequency to allow for flexible movement toward value-congruent, meaningful action. By incorporating questions from MCP to help patients identify valued and meaningful life areas impacted by symptoms along with training in traditional behavioral symptom coping strategies and ACT-based strategies to promote self-management of symptoms and psychological flexibility, it was our hope that the intervention would assist AYAs with better navigating symptoms to allow for continued movement toward important and developmentally relevant goals in the face of life-limiting illness. To date, no intervention of this kind has been developed.
Methods
Setting and participants
Duke University Institutional Review Board approval was obtained. Participants were recruited between January and August 2023 and identified using electronic health records from a comprehensive cancer center and an affiliated children’s hospital. AYAs and/or their parent or guardian (if aged <18) were sent a letter via mail or message in the electronic health system introducing the study and then contacted via phone. AYAs were asked for permission to contact their primary caregiver to approach for participation.
Eligibility criteria for AYAs included: (1) age ≥ 15 and ≤29; (2) diagnosed with advanced (i.e., incurable cancer or distant metastases) or recurrent cancer; and (3) able to speak/read English. Eligible caregivers were (1) aged ≥ 18; and (2) able to speak/read English. Exclusion criteria for all participants included active serious mental illness or visual, hearing, or cognitive impairment that would interfere with participation. All participants aged ≥ 18 provided written informed consent. Parents/guardians of AYAs aged < 18 provided written informed consent, with the AYA providing written assent.
Intervention development
Recruitment letters/messages were sent to N = 53 AYAs, with n = 42 (79.2%) screened for eligibility (Fig. 1a). Of these, n = 17 (40.5%) consented. Among those who consented, n = 15 (88.2%) participated in intervention development interviews. Two individuals consented but did not complete interviews, though each completed the self-report surveys. N = 18 caregivers were approached (Fig. 1b), and n = 16 (88.8%) were screened for eligibility. Of these, n = 13 (81.3%) consented, with n = 11 (84.6%) completing interviews and n = 2 (15.4%) being lost to follow-up after completing the self-report surveys.
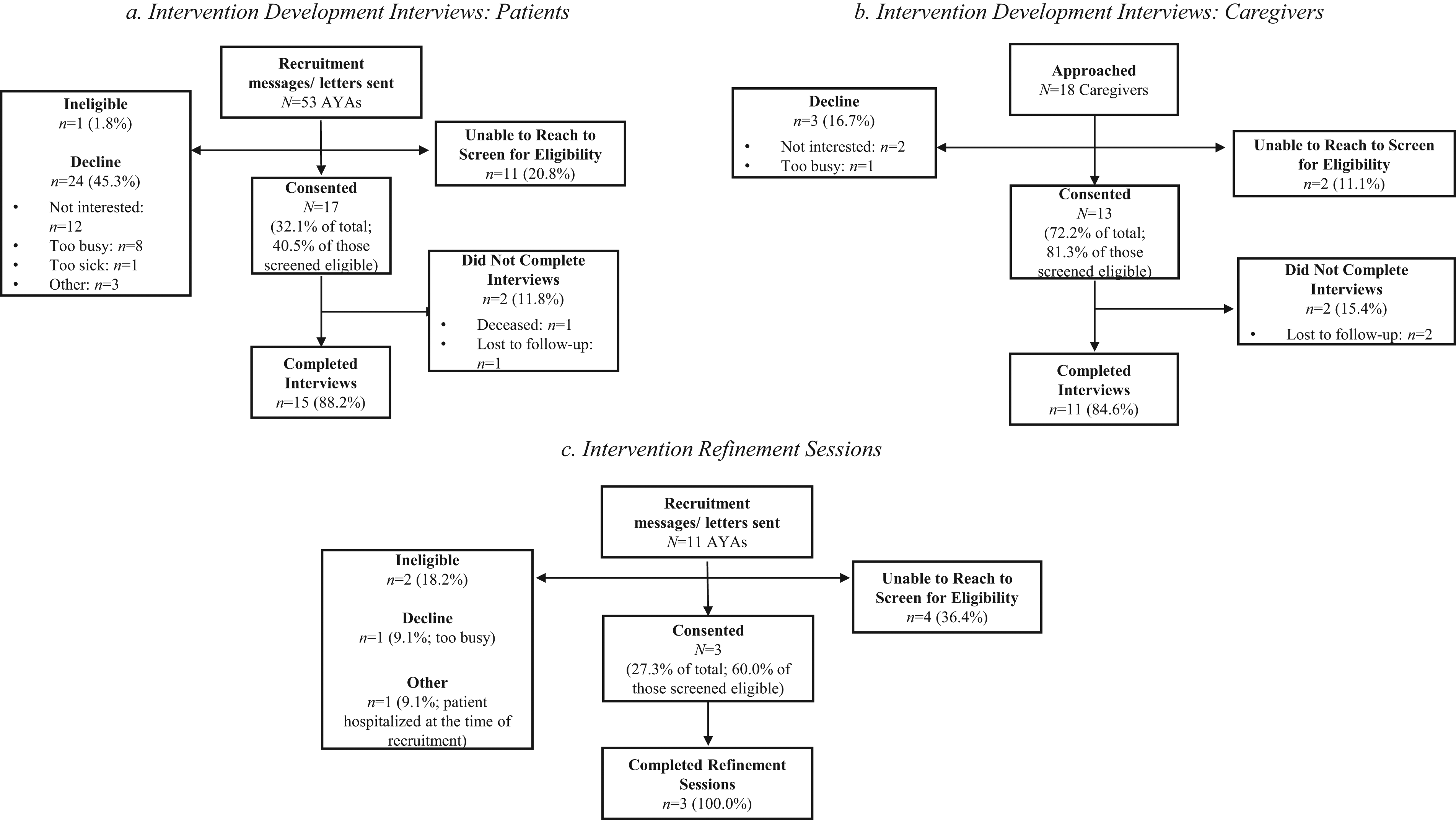
Study flow diagrams.
Intervention development interviews were conducted via videoconferencing in a group (three patient groups with n = 2 patients per group; one caregiver group with n = 3 caregivers) or individual (n = 6 patients; n = 5 caregivers) format to accommodate preferences and scheduling needs. Three interviews were conducted with patient–caregiver dyads (one dyad per interview). Semi-structured interview guides were used. Participants shared about AYAs’ symptom concerns, symptom management experiences, the role of caregivers in symptom management, and perceptions of a psychosocial symptom management intervention for AYAs (e.g., need for the intervention, barriers/facilitators to participation). To gauge the utility of including strategies from ACT and MCP in the intervention, participants were also asked about the impact of cancer and cancer-related symptoms on their abilities to engage in developmentally relevant values-consistent goals and sense of meaning. Interviews were ∼60 minutes, audio/video-recorded, and transcribed. Participants were compensated $20.
Intervention refinement
A second group of AYAs with advanced or recurrent cancer (N = 11) was approached to review the prototype intervention materials (Fig. 1c). Of those reached, 42.8% (n = 3) consented and completed the intervention refinement session. Prior to each session, participants were mailed paper copies of the prototype patient manual. AYAs were asked to provide input on intervention content, presentation (e.g., look/feel of the materials), relevance of content to AYAs with cancer, and study procedures. The ∼60-minute sessions were conducted using videoconferencing, audio/video recorded, and transcribed. Participants were compensated $20.
Study measures
AYA and caregiver participants completed an electronic assessment comprised of self-report questionnaires to assess sociodemographic and medical variables and evaluate key psychosocial and symptom management domains. For AYAs, the assessment included measures of symptom burden [Patient Reported Outcome Measurement System (PROMIS) Depression, Anxiety, and Fatigue Computer Adaptive Tests 54 ]; pain severity and interference (Brief Pain Inventory-Short Form 55 ); self-efficacy for symptom management (6-item Self-Efficacy for Managing Chronic Disease Scale 56 ); meaning/peace and faith (Functional Assessment of Chronic Illness Therapy-Spiritual Well-Being Scale57,58); and psychological flexibility (Acceptance and Action Questionnaire-II 59 ). Caregivers completed measures assessing their perceptions of their AYA’s self-efficacy and their own self-efficacy in supporting their AYA’s symptom management (adapted versions of the 6-item Self-Efficacy for Managing Chronic Disease Scale 56 ). Each measure had good internal consistency reliability (αs = 0.798–0.983). See Supplementary Data for measure details.
Analytic strategy
Descriptive statistics (e.g., mean, percent) were used to characterize the sample. Rapid qualitative analysis (RQA) was used to analyze interview data and responses from intervention refinement sessions.60,61 RQA has been recommended for use in intervention development as it provides a quick, systematic approach for analyzing qualitative data62,63 while allowing for the identification of intervention elements and barriers/facilitators of a program 64 without sacrificing validity. Interview and refinement sessions were summarized by two study team members (B.H., N.A.A.) using standardized templates derived from the semi-structured interview guides. ∼24% of transcripts were analyzed by both team members; the team members, along with the study PI (C.S.D.), met regularly to ensure consistency and reconcile discrepancies in interpretation between team members prior to team members analyzing transcripts independently. The summaries were then transferred into a matrix (participant by domain) to create an at-a-glance summary of key information, examine the breadth and depth of responses, and allow for easy identification of similarities, differences, and trends in responses. 65 Responses from interview participants were used to develop the prototype intervention, and feedback obtained during the refinement sessions informed subsequent updates to the intervention.
Results
20 AYAs (n = 17 intervention development; n = 3 intervention refinement) participated (Table 1). AYAs were M = 23.4 years old (range = 15–29). The majority identified as White/Caucasian (n = 16, 80%), non-Hispanic (n = 19, 95%), and female (n = 13, 65%). Cancer types varied across participants. Two AYAs had been diagnosed with >1 cancer, and 55% (n = 11) experienced a recurrence. The average time since last treatment was 4.66 weeks (SD = 11.00). Symptom burden was high, with 70% (n = 14) endorsing at least one significant symptom (i.e., worst pain in last week ≥ 4; PROMIS depression, anxiety, or fatigue score ≥ 55). Among those endorsing significant symptoms, the mean number of symptoms was 2.5 (SD = 1.09). Self-efficacy for symptom management was moderate (M = 6.52/10, SD = 2.61).
Sociodemographic and Medical Characteristics and Symptoms Experienced by AYA Participants by Study Phase (N = 20)
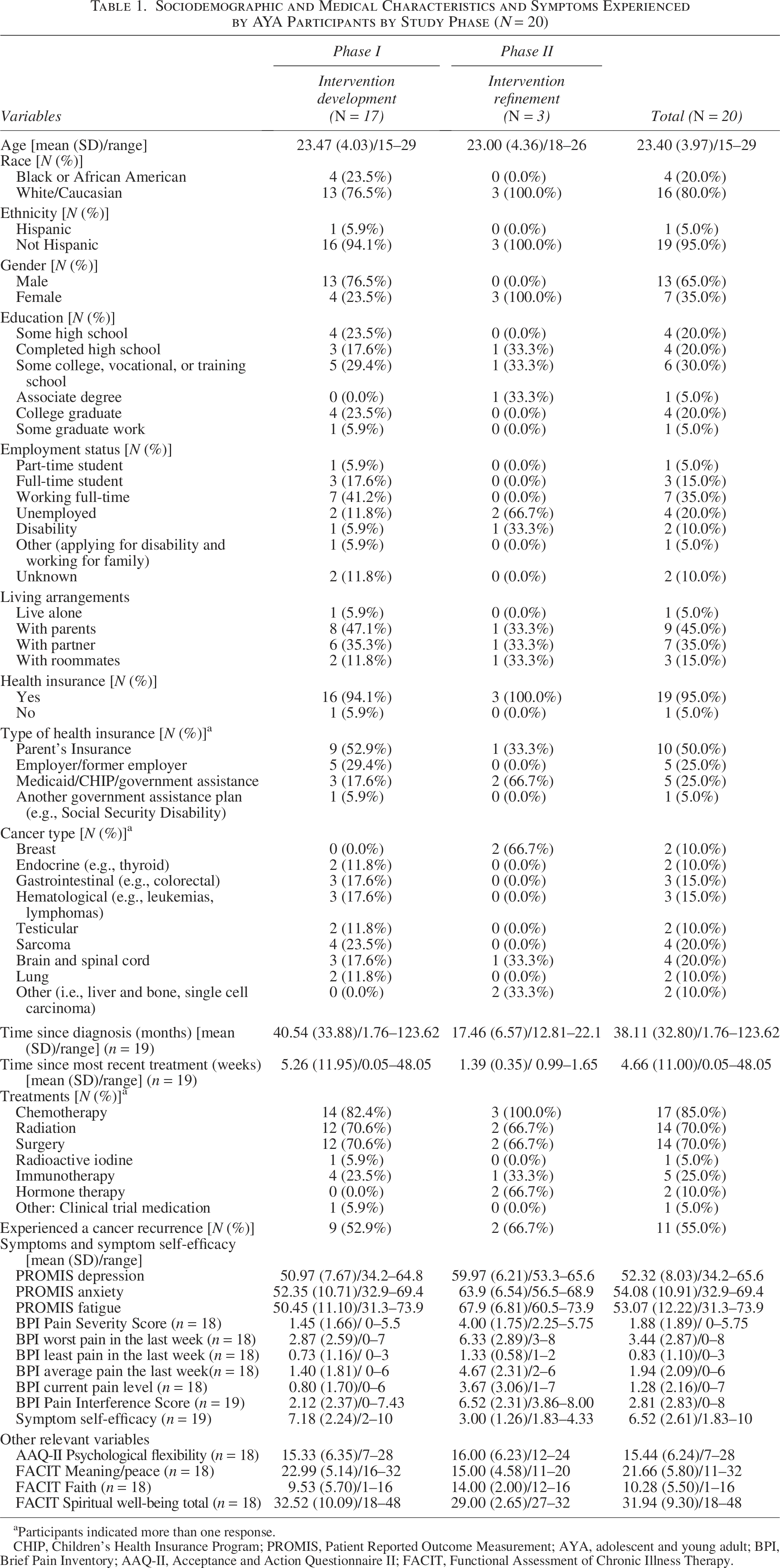
Participants indicated more than one response.
CHIP, Children's Health Insurance Program; PROMIS, Patient Reported Outcome Measurement; AYA, adolescent and young adult; BPI, Brief Pain Inventory; AAQ-II, Acceptance and Action Questionnaire II; FACIT, Functional Assessment of Chronic Illness Therapy.
Caregivers (N = 13; Table 2) were M = 49.4 years old (range = 26–61), and the majority were White/Caucasian (n = 9, 69.2%), non-Hispanic (n = 12, 92.3%), and female (n = 10, 76.9%). Caregivers were AYAs’ parent (n = 11, 84.6%) or spouse/partner (n = 2, 15.4%). Most caregivers were residing with the patient all (n = 10, 76.9%) or some (n = 2, 15.4%) of the time. Caregivers’ self-efficacy for helping the AYA manage symptoms was moderate (M = 5.85/10, SD = 2.59) and slightly lower than their perception of their loved one’s own symptom management self-efficacy (M = 6.08/10, SD = 2.87).
Caregiver Sociodemographic Characteristics and Medical Information about Their Loved One (N = 13)
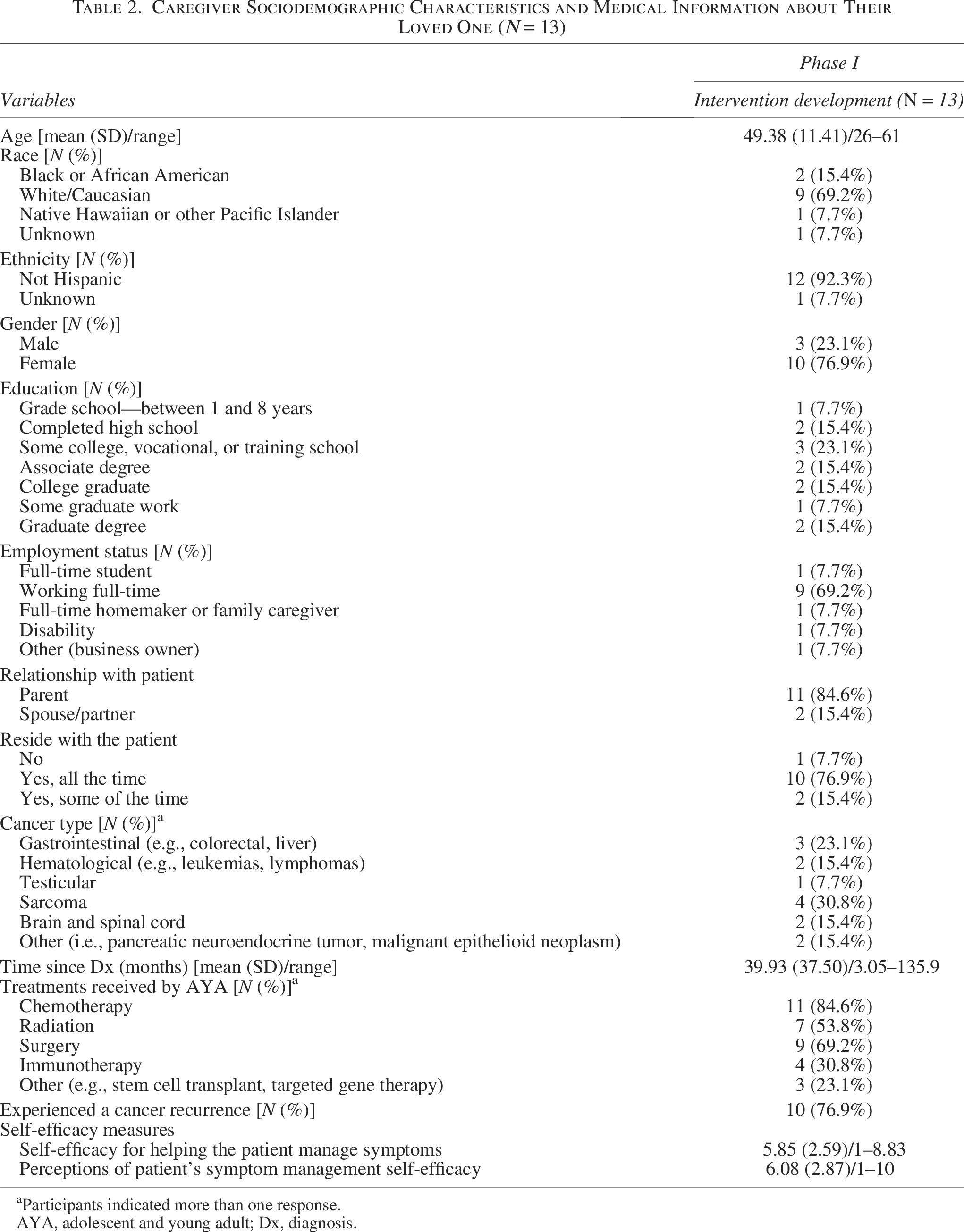
Participants indicated more than one response.
AYA, adolescent and young adult; Dx, diagnosis.
Intervention development
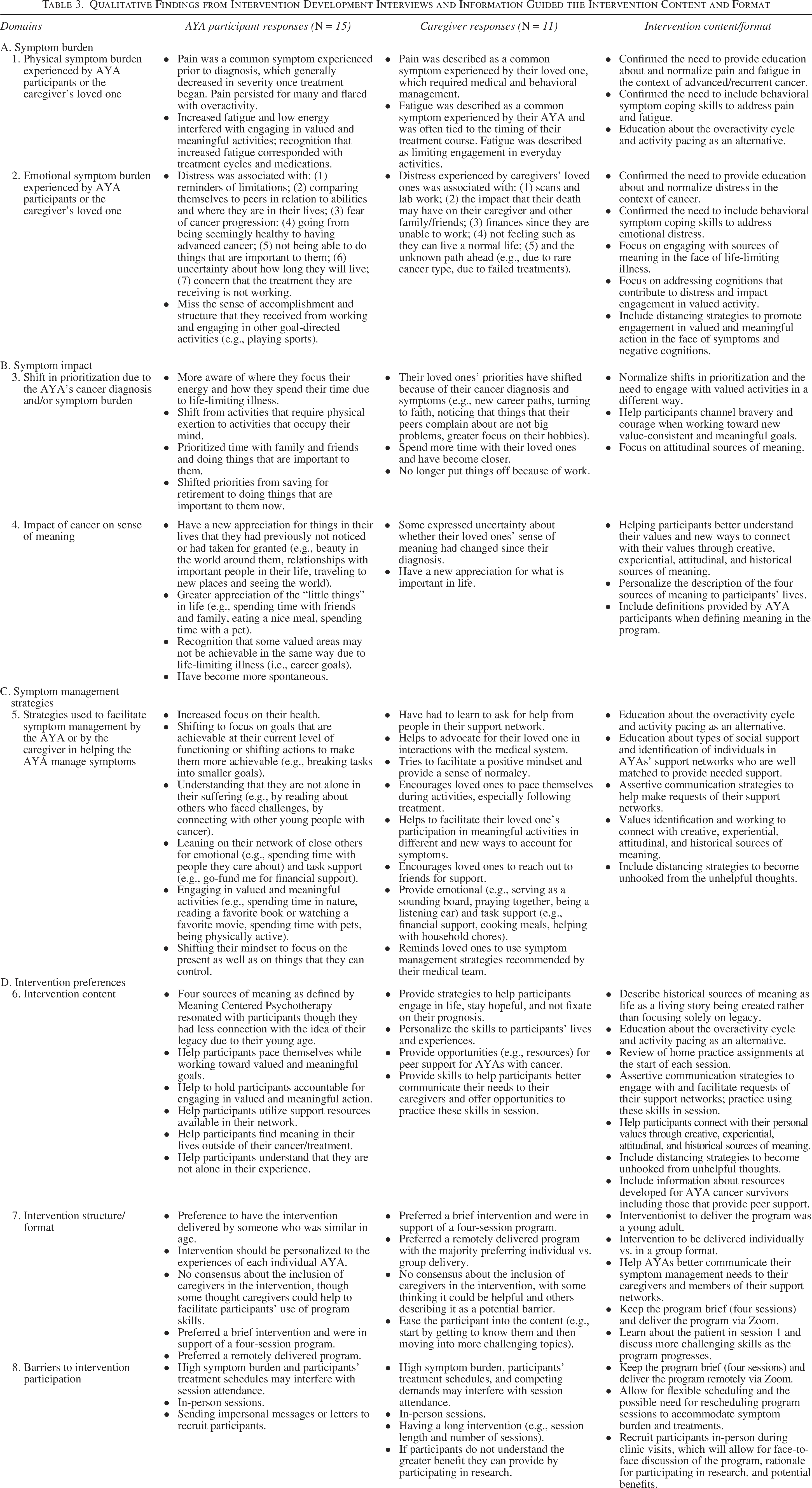
N = 15 AYAs and N = 11 caregivers completed intervention development interviews. Four domains (Table 3) were assessed, including (1) symptom (i.e., physical and emotional) burden; (2) symptom impact; (3) symptom management strategies; and (4) intervention preferences.
Qualitative Findings from Intervention Development Interviews and Information Guided the Intervention Content and Format
Symptom burden
Participant responses
AYAs and caregivers acknowledged pain, fatigue, and emotional distress as common symptoms experienced by AYAs with advanced or recurrent cancer. Pain was often present prior to diagnosis. For some, pain decreased after initiating treatment; for others, pain was persistent. Pain flares were common and associated with overactivity. Fatigue was often tied to the timing of patients’ treatments (e.g., more severe in the days immediately following treatment). The interference of fatigue on AYAs’ valued and meaningful activities was emphasized by both AYAs and caregivers. AYAs’ distress was related to advanced cancer stage, prior failed treatments, fear of disease progression, and limited life expectancy. Other factors contributing to distress included finances, concerns about the impact of their illness and subsequent death on family/friends, not being able to achieve desired goals, and comparing themselves with their peers.
Intervention content/format
Results confirmed the need to provide symptom education; to normalize pain, fatigue, and emotional distress as common symptoms; and to include skills to address these symptoms (e.g., activity pacing, relaxation training, engaging with sources of meaning in the face of life-limiting illness, and addressing cognitions that interfere with valued and meaningful action).
Symptom impact
Participant responses
AYA participants and caregivers explained that the diagnosis of advanced or recurrent cancer and associated symptom burden shifted AYAs’ prioritization for how they spend their time (e.g., more time with family and friends), where they focused their energy (e.g., activities that occupy their mind vs. those that require physical exertion), and their perception of the relative importance of everyday annoyances. Many AYAs described a newfound appreciation for “the little things in life” (e.g., beauty in the world, relationships, travel, eating a nice meal, spending time with a pet); this shift was countered by recognition that some life areas they had previously valued and strived toward (e.g., career goals) may no longer be achievable.
Intervention content/format
Based on these responses, intervention content included strategies to help participants (1) better understand their values; (2) connect with their values through creative, experiential, attitudinal, and historical sources of meaning; and (3) channel bravery and courage when working toward value-consistent and meaningful goals.
Symptom management strategies
Participant responses
Symptom management strategies involved techniques that were both cognitive (e.g., focusing on goals that are achievable, understanding that they are not alone in their experience of suffering, focusing on the present and things within their control) and behavioral (e.g., breaking tasks into smaller steps, turning to their support network for emotional and task support, activity pacing, engaging in valued and meaningful activities).
Intervention content/format
Results supported including strategies to facilitate activity pacing and help AYAs connect with sources of meaning. Responses also suggested including strategies to foster social support (e.g., matching network members’ skills with AYAs’ needs; using assertive communication to make support requests) and distancing strategies for managing unhelpful thoughts associated with situations outside of their control.
Intervention preferences
Participant responses
AYAs and caregivers were overwhelmingly supportive of a psychosocial intervention to facilitate symptom management tailored to the unique experiences of AYAs with advanced or recurrent cancer. They felt that the program would provide useful, actionable tools for symptom management and that the program would hold participants accountable for engaging in valued and meaningful action. Participants felt the program should be brief, personalized to AYA’s individual experiences, and flexible to accommodate for AYAs’ treatment schedules, competing demands, and symptom burdens. There was no consensus about including caregivers in the program, though participants stressed the value of helping AYAs better communicate their symptom management needs to caregivers. AYAs and caregivers expressed value in helping AYAs understand that they are not alone in their experiences by engaging similar-aged individuals in program recruitment and delivery and by including information about AYA-specific resources.
Intervention content/format
Results suggested that a brief (i.e., four-session) psychosocial symptom management intervention delivered individually to AYAs would be acceptable and allow for personalization of program skills to each AYA’s experience and symptoms. Home practice assignments, reviewed at the start of each session, would hold AYAs accountable for using skills and participating in valued action and also provide opportunities for problem-solving and further personalization. Delivery using videoconferencing, allowing flexible scheduling (i.e., in terms of date/time), and rescheduling sessions as necessary would support participation. Rather than including caregivers, the program would teach assertive communication skills to help AYAs communicate their symptom management needs to their caregivers. Recruitment for and delivery of the intervention by a similar-aged peer (i.e., aged < 40) could help participants better connect with the program. AYA-specific resources (e.g., national organizations, online support groups) would be provided.
Prototype intervention
Data from AYAs and caregivers (Table 3) and input from content area experts (ACT: J.P.V.; MCP: W.S.B., J.G.W.; Symptom Coping: T.J.S., C.S.D.) guided development of the intervention prototype. The program (Table 4) entitled “SMILE:
SMILE Intervention Content by Session
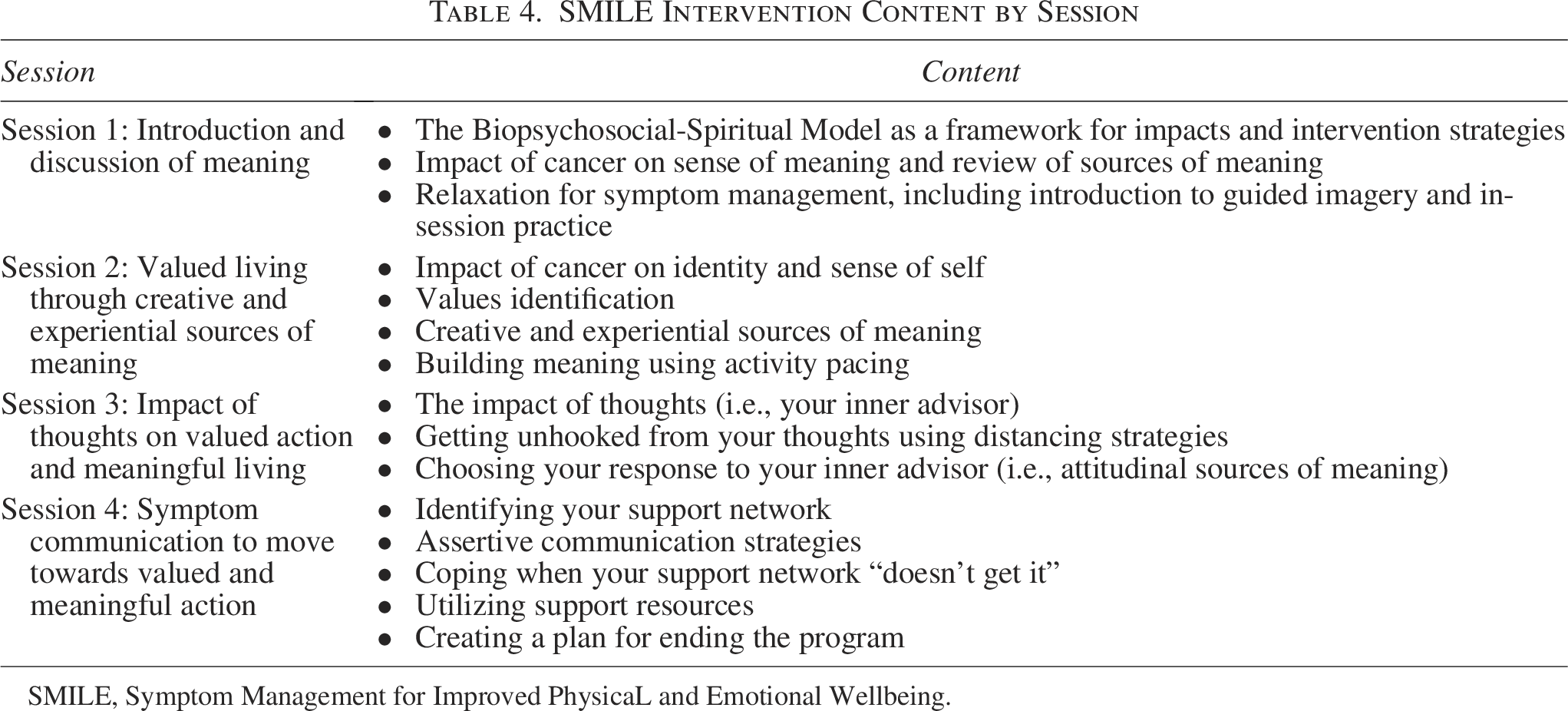
SMILE, Symptom Management for Improved PhysicaL and Emotional Wellbeing.
The four sessions were designed to be delivered using videoconferencing and conducted over an 8-week period to accommodate patients’ symptoms and competing demands. Printed manuals were developed (Fig. 2), which provided session-by-session educational content, resources, and worksheets, and were designed to be reviewed with the AYA by the interventionist. The manual also included home practice activities to support engagement with intervention content. AYA-specific examples and images were used to tailor content to the population.

Patient intervention manual example.
Intervention refinement sessions
The prototype patient manual was reviewed by N = 3 intervention-naïve AYAs (Table 5). AYAs liked the look and feel of the materials, felt that the intervention length was appropriate, and preferred delivery via videoconferencing over in-person or telephone-based delivery. Few modifications were suggested. Participants: (1) identified content areas that could be confusing (e.g., biopsychosocial-spiritual model), and clarifying language was added to the corresponding therapist manual; (2) suggested streamlining program content and using bullet points rather than large paragraphs; and (3) recommended developing a study website (Fig. 3) where relaxation recordings and other digital content (e.g., links to AYA-specific resources) could be accessed. Text message-based reminders were recommended to facilitate completion of assessments and intervention sessions.
SMILE website. SMILE, Symptom Management for Improved PhysicaL and Emotional Wellbeing.
Qualitative Findings from Intervention Refinement Sessions and Corresponding Modifications to the SMILE Intervention
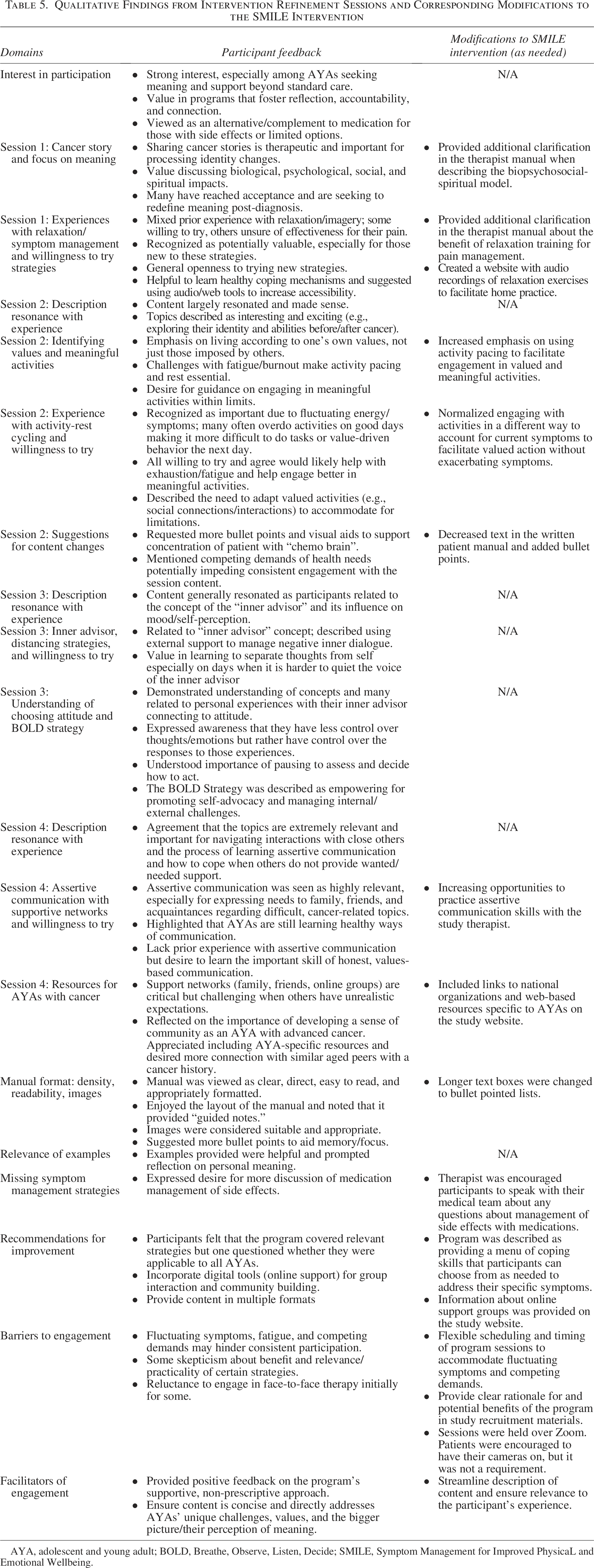
AYA, adolescent and young adult; BOLD, Breathe, Observe, Listen, Decide; SMILE, Symptom Management for Improved PhysicaL and Emotional Wellbeing.
Discussion
For many AYAs with advanced or recurrent cancer, life-limiting illness, aggressive treatments, and associated high symptom burden interfere with engagement in developmentally relevant, value-consistent goals. To date, few psychosocial symptom management interventions target these unique needs. By obtaining qualitative and quantitative data from AYAs and caregivers, we were able to characterize AYAs’ symptom burden and systematically develop and refine an intervention specifically targeting this population. Results pointed to four key findings: (1) high symptom (i.e., pain, fatigue, emotional distress) burden and relatively low self-efficacy for symptom management among this population; (2) the significant impact of symptoms and life-limiting illness on AYAs’ lives and associated goals; (3) the need for and use of both cognitive and behavioral strategies to manage symptoms; and (4) the value of creating a program that provided developmentally relevant support and actionable skills while addressing the unique experience of being an AYA with advanced or recurrent cancer.
Intervention development interviews and refinement sessions also highlighted the relevance and acceptability of including behavioral symptom coping strategies along with strategies from ACT and MCP in the intervention. While strategies derived from these evidence-based approaches are complementary, these approaches have not yet been combined. Through this novel integration, AYAs receive specific education and skills-based instruction to reduce symptom severity and facilitate engagement in valued and meaningful action even in the face of symptoms and life-limiting illness. Refinement sessions provided preliminary evidence for the acceptability of the intervention and allowed for further tailoring to the population and ensuring the appropriateness of the intervention content and format. The refined intervention is now ready to be delivered to AYAs to further evaluate feasibility and acceptability.
This study has several notable strengths. First, it was conducted using a systematic approach to intervention development guided by the NIH Stage Model. 35 Second, it targeted the needs of AYAs with advanced or recurrent cancer, who represent an underserved population in need of such interventions and resources. To ensure that the intervention addressed the population’s developmental stage and unique experiences, input was obtained from AYAs and their caregivers. Results suggested limiting the intervention to AYAs (vs. including caregivers), which is consistent with AYAs’ desire for independence from their families or origin, 66 while also including strategies to improve communication with caregivers and supportive others to facilitate symptom management. Other notable age-specific findings included interest in having similarly aged individuals involved in program recruitment and delivery, as well as the inclusion of information about AYA-specific resources to help patients understand that they are not alone in their experiences as both a young person and a young person with cancer. Finally, the sample included a wide representation of cancer types and treatments, allowing findings to be generalized across disease and treatment settings.
Despite these strengths, the study has several limitations. First, the relatively small sample sizes and limited racial/ethnic diversity (i.e., race, ethnicity) may impact generalizability. Second, intervention refinement sessions were completed with three AYAs. While participants were generally pleased with the intervention content, format, and structure and provided minimal suggestions for modifying or refining the intervention, we recognize that the small, relatively homogenous sample may further limit the generalizability of study findings. The intervention will next be evaluated for feasibility and acceptability through a pilot randomized controlled trial. During this phase, AYAs receiving the intervention will be asked to provide additional qualitative feedback to determine if any other modifications or refinements are needed prior to evaluating the intervention in a larger efficacy trial. Third, due to the project’s scope and focus on developing an intervention for patients, oncology providers were not recruited for participation during the intervention development and refinement processes. Future research would benefit from obtaining input from a variety of oncology providers (e.g., oncologists, advanced practice providers, palliative care specialists, social workers, psychologists) as well as clinical leaders to better understand the feasibility of implementing an intervention of this kind in clinical practice. Each of the aforementioned steps will move the intervention closer to becoming integrated into standard oncology care for AYAs with advanced or recurrent cancers to better support their physical and emotional well-being.
AYAs with advanced or recurrent cancer have generally been underrepresented in the behavioral symptom management literature. Results highlight the need to better understand the symptom experience of this population so that we can develop targeted interventions to address their unique needs. By taking a user-centered approach to intervention development guided by the NIH Stage Model, we have developed an intervention combining three novel, evidence-based approaches. This intervention has the potential to significantly improve symptom management and overall well-being among this underserved population of patients with cancer. Results also highlight the importance of symptom screening so that patients may be directed to targeted, developmentally relevant interventions such as the one developed in this study, which is responsive to the high symptom burden and developmental stage of AYAs with advanced cancer or recurrent cancer.
Authors’ Contributions
The article has been approved by all authors. Conceptualization: C.S.D., T.J.S., L.W., J.P.V., J.G.W., W.S.B., G.M., and C.M.C.; Methodology: C.S.D. and T.J.S.; Project administration: C.S.D., N.A.C., A.D., and T.J.S.; Formal analysis: C.S.D., B.H., and N.A.A.; Funding acquisition: C.S.D.; Writing—original draft: C.S.D., N.A.A., and N.A.C.; Writing—reviewing and editing: T.J.S., J.G.W., J.P.V., G.M., L.W., A.D., B.H., C.M.C., and W.S.B.
Footnotes
Acknowledgment
The authors thank Dr. Julia Kearney for her guidance with adapting Meaning-Centered Psychotherapy for adolescent and young adults with cancer.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
Dr. Caroline S. Dorfman was supported by a grant from the National Institutes of Health (R21CA263727-01A1).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.