
Abstract
Objective:
This study aims to systematically review and summarize existing prognostic models for all-cause mortality in patients with diabetic foot ulcers (DFUs). It further evaluates their characteristics, performance, and methodological quality to inform future model development and clinical application.
Approach:
We searched eight databases from their inception to February 24, 2025. Extracted data included general study characteristics and model-specific information. The prognostic models were classified using the transparent reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis guidelines and evaluated using the Prediction Model Risk of Bias Assessment Tool (PROBAST) to assess the risk of bias (ROB) and applicability.
Results:
Of the 1,580 retrieved studies, 19 were included, reporting a total of 22 prognostic models. Reported mortality rates among DFU patients ranged from 4.2% to 48.5%, with follow-up durations varying from 12 weeks to 22 years. All studies exhibited a high ROB due to issues with data sources, small sample sizes, inadequate data handling, and model validation flaws. Across the included prognostic models, the most frequently reported predictors were age, cardiovascular disease, renal disease, ulcer severity, ischemia, and serum albumin.
Innovation:
Prognostic assessment of mortality risk in patients with DFUs is critical for effective clinical management. This study systematically evaluated 22 published prognostic models using the PROBAST, identifying key methodological limitations and commonly used predictors. The findings provide a scientific basis for the future development of higher quality, clinically applicable prognostic models. In addition, this work offers valuable insights to inform clinical risk stratification and decision-making for DFU patients.
Conclusions:
All included prognostic models demonstrated a high ROB according to the PROBAST assessment. Future research should focus on using larger sample sizes, rigorous study designs, and multicenter external validation to develop more reliable prognostic models. Given the multifactorial nature of mortality risk in DFU patients, multidisciplinary collaboration is essential to improve clinical outcomes.
INTRODUCTION
In recent years, the global prevalence of diabetes has continued to rise. In 2021, an estimated 537 million people worldwide were living with diabetes. This number is projected to reach 643 million by 2030 and 783 million by 2045. 1 China has the highest number of diabetes cases globally, with approximately 140 million individuals aged 20–79 affected. 2 It is estimated that 19–34% of individuals with diabetes will develop diabetic foot ulcers (DFUs) during their lifetime. 3 DFUs are common and serious complications of diabetes. They mainly result from lower extremity neuropathy or vascular disease, which can lead to local infection, ulceration, and even deep tissue necrosis. 4 Globally, the prevalence of DFUs is approximately 6.3%. 5
Patients with DFUs face high risks of recurrence and amputation. The 5-year mortality rate was as high as 50–70%, 6 comparable with that of many cancers. 7 Moreover, studies show that the mortality risk in DFU patients is 2.5 times higher than in diabetic patients without foot ulcers. 8
Although DFUs primarily manifest as a localized condition, their clinical prognosis is significantly influenced by systemic complications. 9 Brennan et al. found a strong association between the severity of DFUs and increased mortality risk. 10 The presence of peripheral artery disease (PAD) further increases the mortality rate in this population. 11 A systematic review identified cardiovascular disease and infection as the leading causes of death among patients with DFUs. 12 In addition, poor nutritional status may further increase the risk of both mortality and amputation. 13
Accurate prediction of mortality risk in patients with DFUs is essential for early intervention and personalized treatment. Clinical prognostic models estimate health outcome probabilities and support patient counseling and clinical decision-making. 14 A clinical prognostic model is a statistical tool that combines two or more predictors—such as patient characteristics, clinical findings, or laboratory results—to estimate the probability of a specific outcome in an individual. Common forms include risk scores and nomograms. A risk score assigns numerical points to each predictor based on its weight in the model, and the total score corresponds to a predicted probability of the outcome. 15 In contrast, a nomogram is a graphical tool that translates a multivariable regression model into a continuous scoring system, allowing clinicians to visually calculate the precise probability of an endpoint—such as disease progression or mortality—for an individual patient. 16 Well-developed and validated prognostic models for DFU patients can help bridge information gaps, improve the accuracy of mortality estimates, and provide health care professionals with evidence-based decision support. This, in turn, facilitates the management of modifiable risk factors and enhances long-term patient outcomes. 17 In recent years, research on DFU mortality prognostic models has grown; however, the quality of existing models varies significantly. Therefore, this study aims to systematically review and synthesize current DFU mortality prognostic models, assess their potential ROB, and provide guidance for selecting or developing high-performance models to support clinical prognosis management.
CLINICAL PROBLEM ADDRESSED
DFU is one of the most common and serious chronic complications of diabetes, associated with a high mortality rate. Although primarily localized, DFUs often coexist with systemic issues such as cardiovascular disease, PAD, and infections, which further elevate the risk of death. Therefore, accurately assessing the mortality risk in DFU patients is essential for early intervention and personalized treatment. However, the quality of existing mortality prognostic models varies widely. Thus, it is essential to conduct a systematic evaluation of these models to improve their scientific rigor and clinical utility. This will provide a solid foundation for health care professionals to select or develop high-performance prognostic tools and ultimately enhance the prognosis management of patients with DFUs.
MATERIALS AND METHODS
The study protocol was registered on PROSPERO (CRD420250652656, https://www.crd.york.ac.uk/PROSPERO/view/CRD420250652656), and no amendments were made after registration.
Terminology clarification
In this systematic review, we use the term “prognostic model” to refer to multivariable models developed to estimate the probability of future mortality in patients with DFUs. Although the term “predictive model” is sometimes used in the literature to describe similar models, we adopt “prognostic model” throughout this article for conceptual clarity and consistency. When citing external literature that uses different terminology, the original wording is retained.
Literature search strategy
To ensure a comprehensive and inclusive search, we conducted searches in both the Chinese and English databases. The databases searched included China National Knowledge Infrastructure, Wanfang Data, China Science and Technology Journal database, SinoMed, PubMed, Web of Science, The Cochrane Library, and Embase. All databases were searched from their inception to February 24, 2025. No additional sources, such as trial registers or conference proceedings, were searched. A combination of keywords was used, including: “diabetic foot,” “diabetic feet,” “diabetic foot ulcer,” “DF,” “DFU,” “prediction model,” “predictive model,” “risk prediction,” “risk factor*,” “risk assessment,” “prognostic model,” “risk score*,” “prediction tool,” “nomogram,” “predictive factor*,” “mortality,” “survival,” and “death.” The full electronic search strategies for each database, including all Boolean operators and field tags, are provided in Supplementary Data S1 to ensure reproducibility.
We utilized the PICOTS framework, recommended by the Critical Appraisal and Data Extraction for Systematic Reviews of Prediction Modeling Studies checklist. 18 This system helps frame the review’s aim, search strategy, and study inclusion and exclusion criteria. 19 The key items of our systematic review are described below:
Inclusion and exclusion criteria
The inclusion criteria for this review were as follows: (1) studies involving patients diagnosed with DFUs as the primary population, regardless of whether these patients had comorbidities such as peripheral neuropathy or PAD; (2) observational study designs, including cohort, case–control, or cross-sectional studies; (3) development and/or reporting of a mortality risk prognostic model; and (4) the primary outcome of interest was all-cause mortality. Studies reporting only cause-specific mortality were excluded to maintain consistency in outcome definition and comparability across studies.
Studies were excluded if they met any of the following criteria: (1) no mortality risk prognostic model was developed or reported; (2) the study focused exclusively on specific causes of death rather than all-cause mortality; (3) the publication was not in English or Chinese; (4) the full text was unavailable despite attempts to contact the authors; (5) the study population consisted solely of DFU patients who had received specific interventions, such as prior lower limb amputation, vascular stenting, or revascularization surgery; (6) included mixed patient populations where DFU was not the primary study population; (7) follow-up limited to the hospitalization period only; or (8) a total sample size of fewer than 100 participants.
Study selection and screening
The study selection process was independently conducted by two reviewers (G.Y.H. and Z.J.Y.). Initially, duplicate records were removed using EndNote software. The remaining titles and abstracts were screened based on the predefined inclusion and exclusion criteria. Subsequently, full-text articles of potentially eligible studies were retrieved and reviewed. The reference lists of all included studies were also manually screened to identify additional relevant studies. Any disagreements during the selection process were resolved through discussion or consultation with a third reviewer (Z.H.R.).
Data extraction
Data extraction was independently performed by two reviewers. Any discrepancies were resolved through discussion, with a third reviewer consulted when consensus could not be reached. The primary outcome of interest was all-cause mortality in patients with DFUs, and all reported mortality outcomes during follow-up were extracted, excluding in-hospital mortality. When multiple follow-up time points were available, all relevant time points were recorded. If a study reported more than one prognostic model, all eligible models were included for analysis. Descriptive statistics were collected for each study.
The extracted data were categorized into two groups: (1) General study characteristics, including first author, publication year, country, study design, population characteristics, data source, follow-up duration, sample size, and mortality rate. (2) Model-related information, such as handling of missing data, modeling methods, predictor variables, model discrimination, calibration techniques, and validation approaches. As part of this process, the included studies were classified according to the transparent reporting of a multivariable prognostic model for Individual Prognosis Or Diagnosis guidelines to assess reporting transparency and completeness. Initial data extraction was conducted by one reviewer and subsequently cross-checked by a second reviewer to ensure accuracy and consistency. An electronic laboratory notebook was not used for data collection or management in this study.
All eligible studies were summarized descriptively due to heterogeneity in study design, predictors, outcome assessment, follow-up duration, and model development methods. Study characteristics and model features were tabulated for comparison, without performing meta-analysis, statistical conversions, or sensitivity analyses.
Quality assessment
ROB and applicability of the included studies were independently assessed by two reviewers using the Prediction Model Risk of Bias Assessment Tool (PROBAST), as recommended by Cochrane. PROBAST consists of 20 signaling questions across four domains: participant selection, predictors, outcomes, and analysis. Each question is rated as “Yes/Probably yes,” “No/Probably no,” or “No information.” For ROB, if all four domains were rated as low risk, the overall study risk was considered low; if any domain was rated as high risk, the overall study risk was considered high. Applicability was assessed in three domains: participant selection, predictors, and outcomes, with each rated as “low,” “high,” or “unclear” concern. Studies with all three domains rated as low concern were considered to have good applicability.
RESULTS
Study selection
Figure 2 illustrates the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 flowchart, detailing the comprehensive search process and screening results.
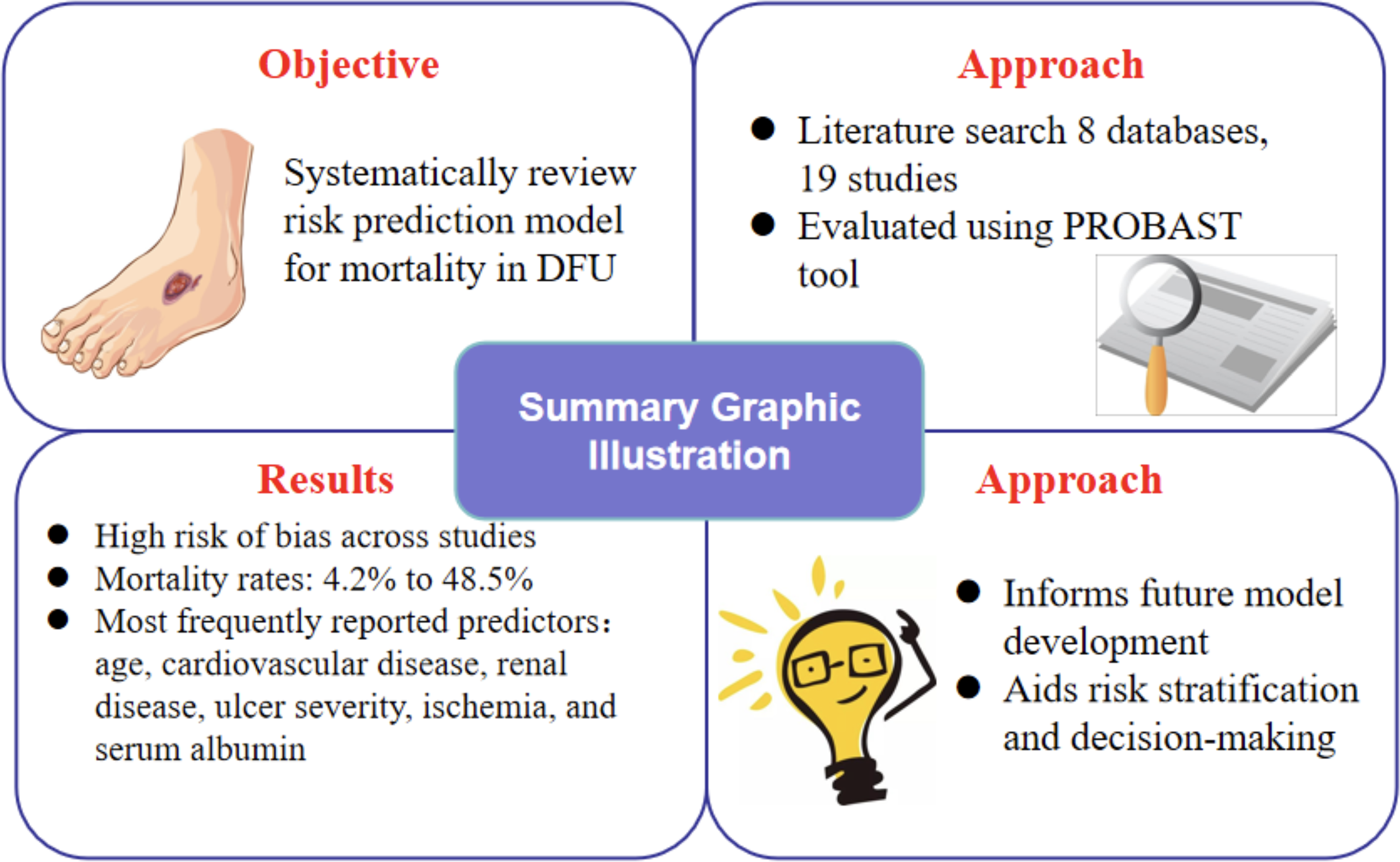
Summary of graphic illustration.
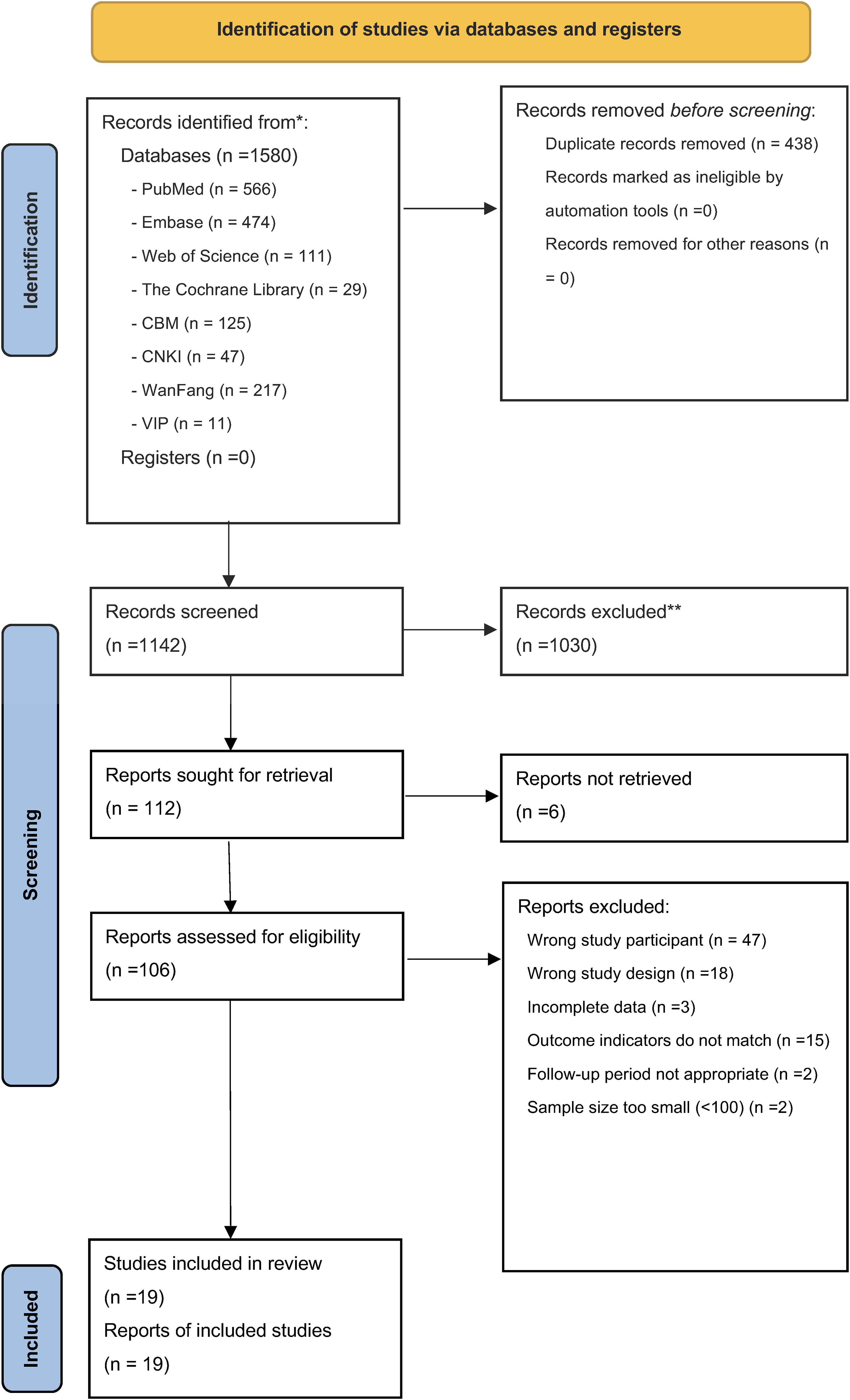
Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 flow diagram for the selection of studies.
A total of 1,580 articles were initially identified through database searches. After removing 438 duplicates using EndNote X9 reference management software, 1,142 articles remained. Following title and abstract screening, 1,030 articles were excluded. Subsequently, 112 reports were sought for retrieval, of which six could not be obtained, leaving 106 full-text articles assessed for eligibility. Based on the predefined inclusion and exclusion criteria, 19 studies were finally included in this systematic review.
Study characteristics
Table 1 summarizes the key characteristics of the 19 included studies in this systematic review, encompassing a total of 22 prognostic models for mortality in patients with DFUs. Among these studies, one reported three models, 24 one reported two models, 34 and the remaining studies each developed a single prognostic model. These studies were published between 2007 and 2024, with seven conducted in China,20,22,33,35–38 two in Italy,23,31 two in Romania,24,34 two in the United Kingdom,27,32 and one each in South Korea, 21 France, 25 Australia, 26 Saudi Arabia, 28 Tanzania, 29 and Spain, respectively. 30 Among the included studies, five were prospective cohort studies,25,29,30,32,33 and 14 were retrospective cohort studies.20–24,26–28,31,34–38 Two studies used data sourced from databases,21,27 while the remaining 17 collected data from health care institutions,20,22–26,28–38 among which 13 were single-center studies,20,22–26,28,31,33,34,36–38 and four were multicenter studies.29,30,32,35 The mean or median age of participants ranged from 52.4 to 72.2 years, with a predominance of males between 54.6% and 69.5%. Sample sizes varied widely, ranging from 103 to 71,000 participants. Follow-up durations ranged from 12 weeks to 22 years, and mortality rates varied between 4.2% and 48.5%, indicating substantial heterogeneity across studies.
Characteristics of the Included Studies
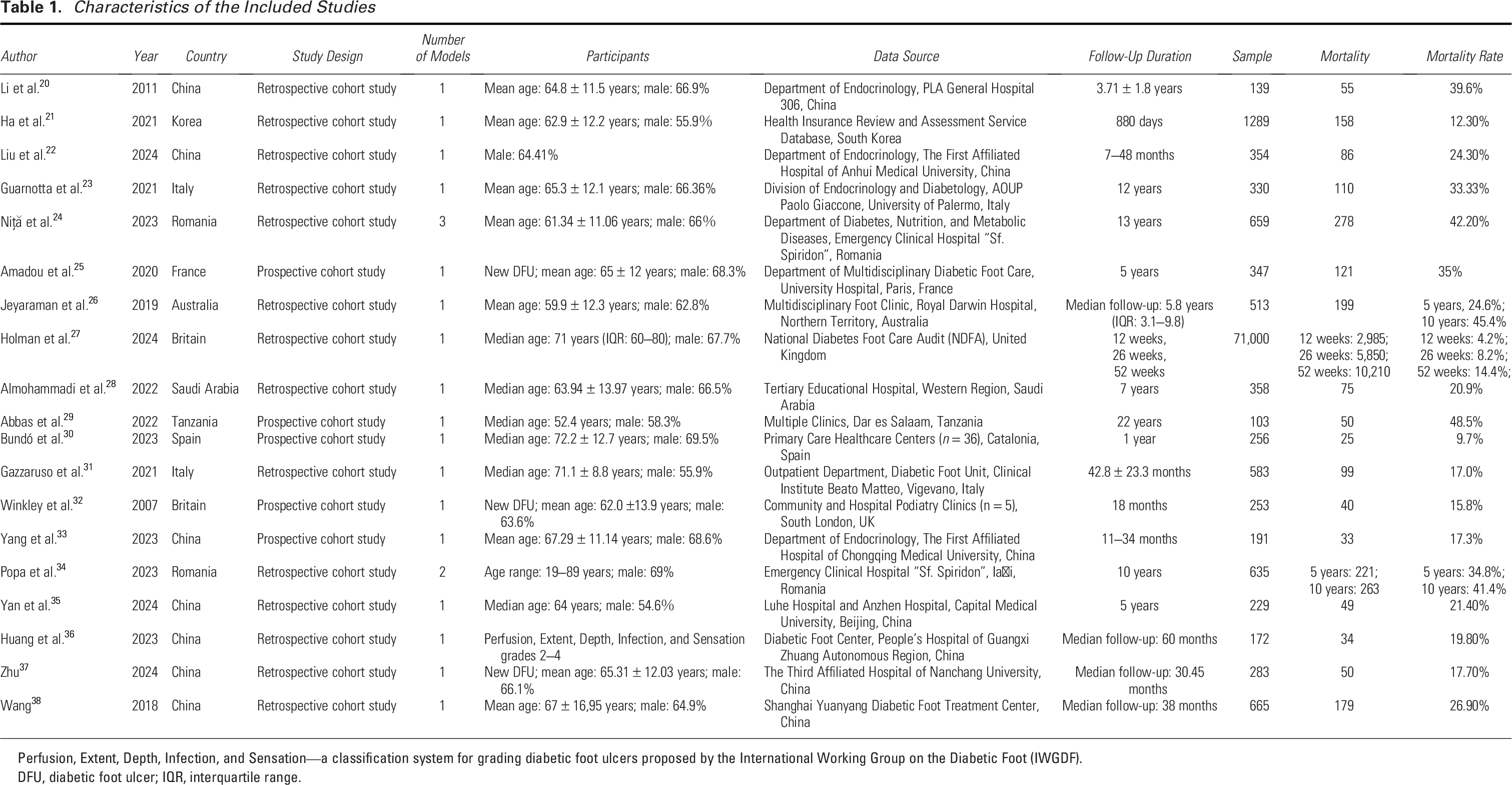
Perfusion, Extent, Depth, Infection, and Sensation—a classification system for grading diabetic foot ulcers proposed by the International Working Group on the Diabetic Foot (IWGDF).
DFU, diabetic foot ulcer; IQR, interquartile range.
Table 2 summarizes the characteristics of the 22 prognostic models derived from the 19 included studies. Among the 22 models, 16 were developed using the Cox proportional hazards models, as reported in 14 studies.20–26,29,30,32,33,36–38 Two models used standard logistic regression models,28,35 one model using a Poisson regression model, 27 one using a multivariable logistic regression model, 31 and two using a multilayer perceptron approach within a single study. 34 Sixteen models did not report how missing data were handled,20–32,38 including three models from a single study. 24 Only four models reported the area under the curve (AUC), with values ranging from 0.68 to 0.742, including two models from a single study. 34 The reported AUC values indicate moderate model discrimination (AUC >0.60).22,34,36 Calibration was reported in four models, three of which were from a single study, 24 and one from another study. 31 All models used the Hosmer–Lemeshow goodness-of-fit test. Internal validation of the prognostic model was performed in only one model. 34 None of the included models conducted external validation.
Characteristics of the Included Prognostic Models
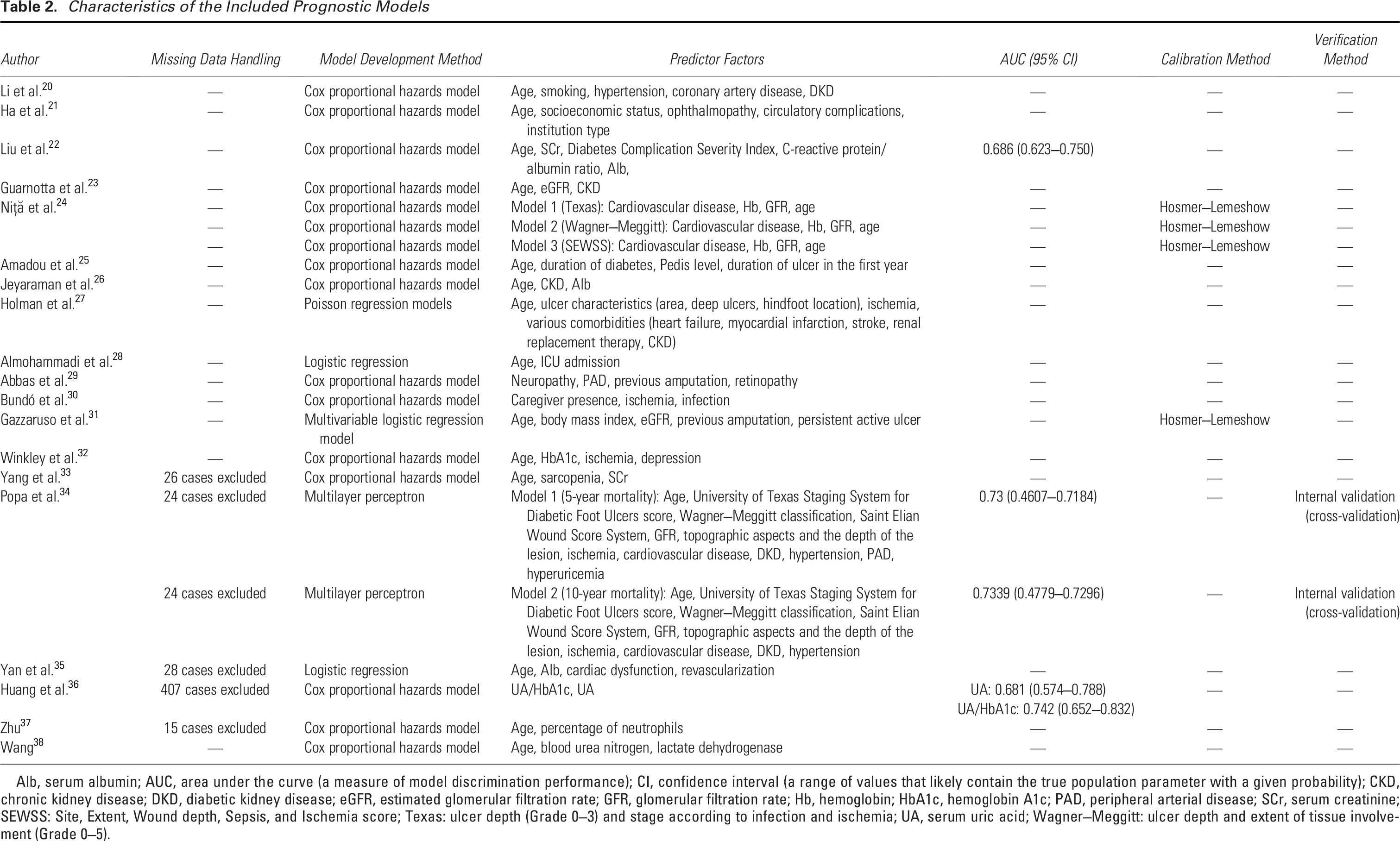
Alb, serum albumin; AUC, area under the curve (a measure of model discrimination performance); CI, confidence interval (a range of values that likely contain the true population parameter with a given probability); CKD, chronic kidney disease; DKD, diabetic kidney disease; eGFR, estimated glomerular filtration rate; GFR, glomerular filtration rate; Hb, hemoglobin; HbA1c, hemoglobin A1c; PAD, peripheral arterial disease; SCr, serum creatinine; SEWSS: Site, Extent, Wound depth, Sepsis, and Ischemia score; Texas: ulcer depth (Grade 0–3) and stage according to infection and ischemia; UA, serum uric acid; Wagner–Meggitt: ulcer depth and extent of tissue involvement (Grade 0–5).
Quality assessment
Table 3 presents the results of ROB and applicability assessments of the included prognostic models using the PROBAST, together with brief rationales for each judgment. All models were rated as having a high ROB, indicating methodological limitations in either the development or validation of the prognostic models. In the “Participants” domain, bias was primarily related to data sources. According to the PROBAST criteria for low ROB in prognostic models, prospective cohort studies, registry data, or high-quality datasets are recommended as appropriate sources. 39 However, 13 models were rated as having a high ROB in this domain, primarily due to their use of retrospective cohort designs based on nondatabase sources, including three models from Niță et al., 24 and two models from Popa et al., 34 with the remaining models from other single-model studies.22,23,26,28,31,35–37 An additional three studies were rated as having unclear ROB,20,33,38 mainly because the exclusion criteria were not explicitly stated, making it difficult to assess the representativeness and consistency of the study populations. In the “Predictors” domain, one model was rated as having unclear ROB, 37 primarily due to the lack of a clear definition or assessment method for the predictors. In the “Outcome” domain, all models were rated as having a low ROB. In the “Analysis” domain, 20 models were rated as having a high ROB.20–33,35–38 This was mainly attributed to several factors: failure to address missing data,20–32,38 insufficient sample size to support model development,20,29 lack of reporting on model calibration performance,20–23,25–30,32–38 and the absence of any internal or external model validation.20–33,35–38
Domain-Level PROBAST Risk of Bias and Applicability Assessments with Brief Rationales
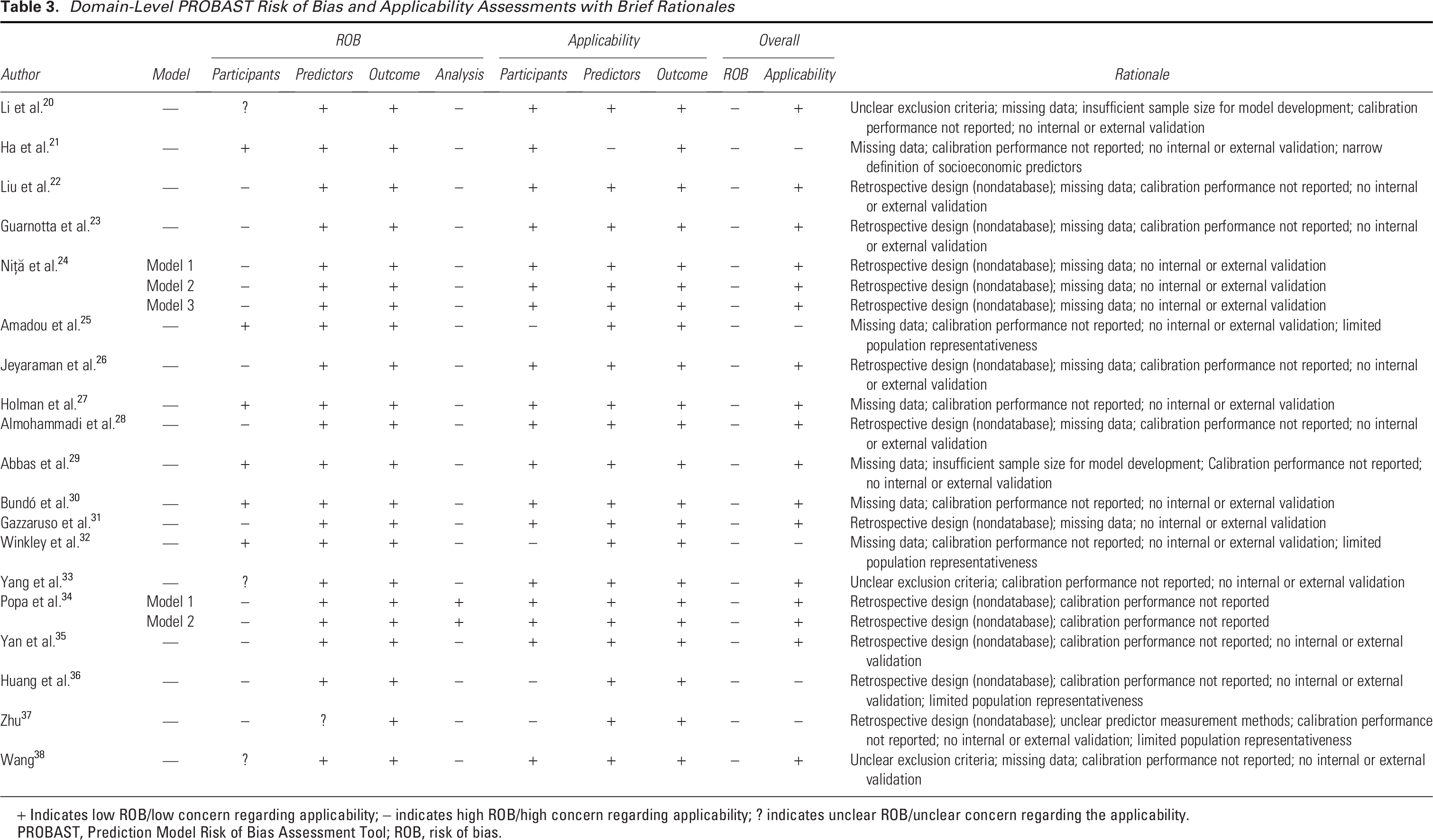
+ Indicates low ROB/low concern regarding applicability; − indicates high ROB/high concern regarding applicability; ? indicates unclear ROB/unclear concern regarding the applicability.
PROBAST, Prediction Model Risk of Bias Assessment Tool; ROB, risk of bias.
In terms of applicability concerns, five models were rated as having high concern regarding applicability,21,25,32,36,37 while the remaining 17 models were classified as having low concern.20,22–24,26–31,33–35,38 In the “Participants” domain, four models were considered to have high concern regarding applicability due to limited representativeness of the included populations25,32,36,37 Specifically, some models restricted inclusion to newly diagnosed DFU patients,25,32,37 or those with Perfusion, Extent, Depth, Infection, and Sensation grades 2–4. 36 These restrictive inclusion criteria may limit the generalizability of the findings to the broader DFU patient population. In the “Predictors” domain, one model was rated as having high concern regarding applicability due to a narrow definition of socioeconomic status. 21 This model used only insurance type, income percentile, and residential area as indicators, omitting other key socioeconomic variables such as lifestyle and education level, which may compromise the external applicability of the prognostic model. In the “Outcome” domain, all models were rated as having low concern regarding applicability.
Prognostic factors in the included models
In this systematic review, a total of 19 studies were included, identifying 22 prognostic models for mortality risk in patients with DFUs. Across these models, 39 distinct predictors were identified. These predictors were categorized into five main domains: demographic characteristics, comorbidities and underlying conditions, laboratory and physiological indicators, foot ulcer-related factors, and hospitalization or treatment-related factors. For studies presenting multiple models,24,34 only predictors consistently identified across models were extracted to prevent duplication. Among these, the most frequently reported predictors across the included models were age, cardiovascular disease, renal disease, ulcer severity, ischemia, and serum albumin (Alb), as summarized in Table 4. It should be noted that the frequency with which a predictor appears across models does not necessarily reflect the magnitude of its statistical association with mortality, as inclusion may depend on study design, sample characteristics, and modeling strategies. As this review focuses on prognostic modeling rather than causal inference, these predictors should be interpreted as contributors to risk estimation rather than independent causal determinants.
Prognostic Factors in the Included Models
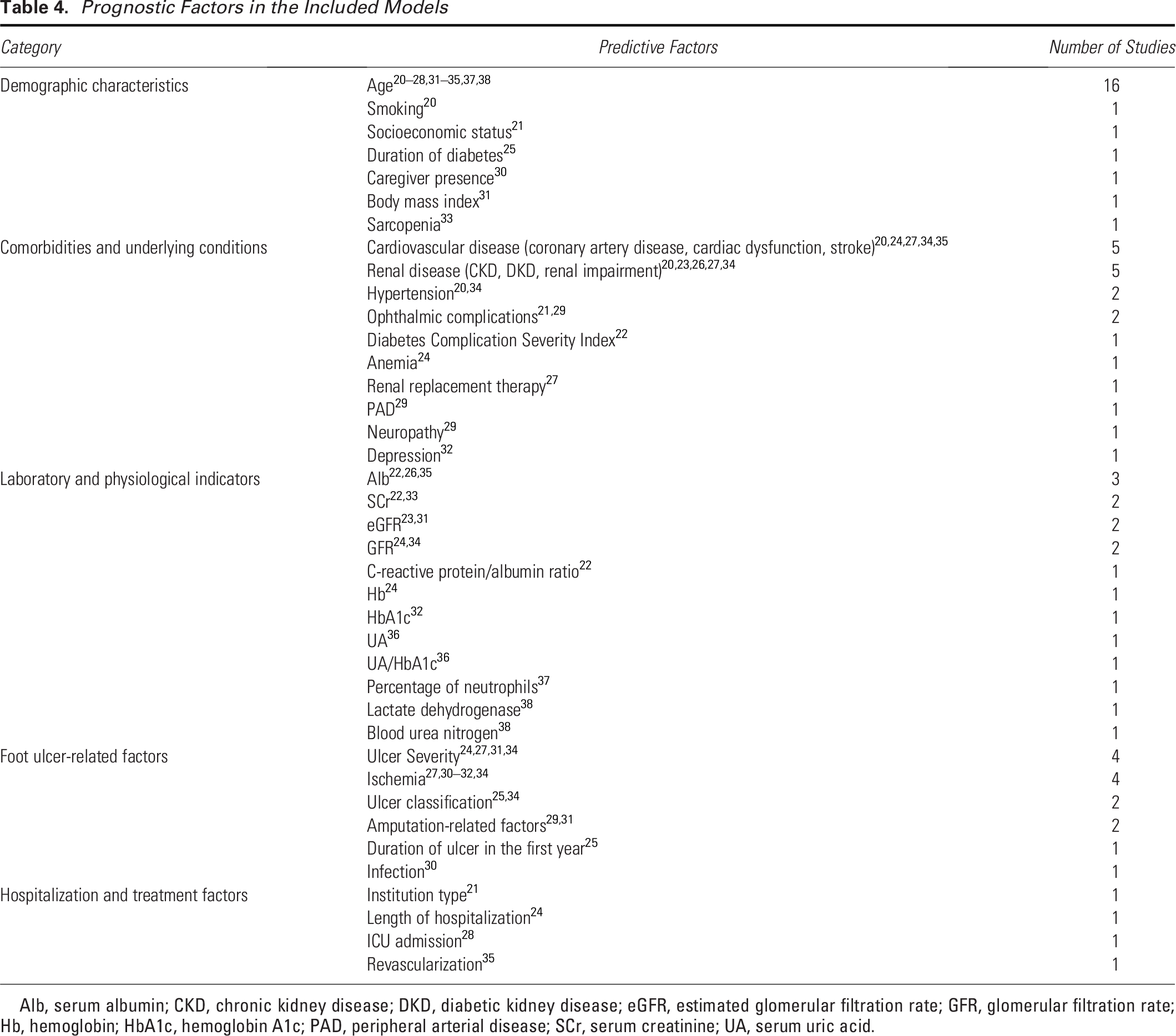
Alb, serum albumin; CKD, chronic kidney disease; DKD, diabetic kidney disease; eGFR, estimated glomerular filtration rate; GFR, glomerular filtration rate; Hb, hemoglobin; HbA1c, hemoglobin A1c; PAD, peripheral arterial disease; SCr, serum creatinine; UA, serum uric acid.
DISCUSSION
This systematic review identified and summarized 22 prognostic models for mortality risk in patients with DFUs, derived from 19 studies. The reported mortality rates varied widely, ranging from 4.2% to 48.5%. Several factors may explain this variation. One key factor is the length of follow-up. In general, longer follow-up periods result in more observed death events, leading to higher reported mortality rates. Geographic and population differences also play a role. Countries differ in health care quality, economic development, patient characteristics, health behaviors, and allocation of medical resources. Patients in resource-limited settings may face higher mortality risks due to delayed diagnosis and limited access to care. Previous research has shown a strong association between lower socioeconomic status and increased mortality risk in patients with DFUs. 21 Most included studies were retrospective and conducted at single centers, which limits the generalizability and external validity of the findings. This may also affect the accuracy of mortality estimates. Future research should prioritize prospective, multicenter studies to improve data quality and representativeness. Moreover, greater attention should be given to the role of social determinants of health in DFU-related mortality, particularly in low- and middle-income countries and regions.
This systematic review analyzed the characteristics, methodological quality, and applicability of the included models. According to the PROBAST assessment, all models were rated as having a high ROB with the Analysis domain being the primary contributor. Key limitations included inappropriate data sources, small sample sizes, inadequate handling of missing data, and lack of model calibration and validation. These limitations explain why most existing DFU mortality prognostic models fail to meet contemporary methodological standards and have limited reliability for clinical decision-making. High ROB may introduce systematic errors that distort predictor selection and inflate effect estimates, reducing both reproducibility and generalizability. Regarding applicability, five studies were rated as having high concern. The main limiting factors included restrictive inclusion criteria and narrowly defined predictors, which may reduce the external validity of the models in clinical settings. Therefore, when applying these models in practice, both the ROB and applicability limitations should be considered, and the results interpreted with caution. To enhance the robustness, generalizability, and clinical utility, future models should consider adopting prospective study designs or utilizing high-quality databases to ensure data representativeness and reliability. Clearly defined inclusion and exclusion criteria are essential to minimize population heterogeneity. Sample size should meet the recommended threshold of at least 10 outcome events per predictor variable. 40 Blinded assessment of both outcomes and predictors is recommended to reduce measurement bias. Continuous variables should be retained during analysis whenever possible. If categorization is necessary, internal validation and coefficient shrinkage should be performed to mitigate overfitting. 40 Evidence suggests that machine learning approaches such as support vector machines and back propagation neural networks may offer superior prognostic performance compared with the traditional statistical methods. 41 Therefore, future model development should incorporate a broader range of modeling techniques, including machine learning algorithms such as decision trees and random forests, to improve the identification of high-risk individuals and enhance model applicability. Importantly, both internal and external validations are essential to ensure prognostic performance and reduce bias risk. In summary, future DFU mortality risk models should follow PROBAST guidelines. Emphasis must be placed on sound methodology and thorough validation to produce reliable clinical tools.
This study highlights the considerable heterogeneity of predictors across mortality prognostic models for patients with DFUs. The variables included in the reviewed models varied substantially, with no two models sharing an identical set of predictors. The most frequently reported predictors were age, cardiovascular disease, renal disease, ulcer severity, ischemia, and Alb. Age is a nonmodifiable factor closely associated with chronic comorbidities and declining physiological reserve. It has been repeatedly included in various models, indicating its consistency and predictive value in mortality risk estimation. Cardiovascular and renal diseases represent the multisystem involvement commonly seen in DFU patients and are strong predictors of mortality. This multimorbidity substantially increases the risk of death. A large-scale study involving 66,323 U.S. veterans with DFUs found significantly higher mortality rates among those with cerebrovascular, cardiovascular, and renal comorbidities. 10 A global systematic review and meta-analysis of DFU mortality reported that nearly 50% of deaths were attributable to cardiovascular causes. 12 Prior research also confirmed that active management of cardiovascular risk factors can reduce mortality in this population. 42 Ulcer severity reflects wound depth, area, infection status, and degree of ischemia. More severe ulcers are harder to manage, increasing the risk of complications such as sepsis, which is responsible for approximately 14% of DFU-related deaths. 43 Furthermore, a systematic review demonstrated that DFU patients with PAD (a common manifestation of ischemia) had a higher mortality risk compared with those without PAD (HR = 1.88). 12 Alb levels reflect nutritional status. Malnutrition impairs wound healing and may exacerbate cardiovascular and cerebrovascular disease, potentially triggering acute adverse events. 9 Certain nutritional factors have been shown to promote collagen deposition and support tissue repair, thereby facilitating wound healing. 44 From this perspective, nutritional status may represent a potentially modifiable determinant of prognosis in patients with DFUs. Therefore, a multidisciplinary and proactive approach is essential in DFU management. Optimal care should go beyond local wound treatment to comprehensively address comorbidities, vascular health, nutritional status, and systemic risk factors.
This review has several limitations, mainly related to the review process itself and the characteristics of the included studies. First, regarding the review process, this review may not have comprehensively captured all the existing mortality prognostic models for patients with DFUs. Unpublished models or those indexed in nonmainstream databases may have been missed, introducing selection bias. The literature search was restricted to English and Chinese publications, which may have excluded relevant evidence, particularly from low- and middle-income countries, thereby limiting the global applicability of the findings. In addition, to minimize confounding from specific interventions, studies enrolling only patients who had undergone amputation or revascularization were excluded; however, this restriction may have reduced the external generalizability of the results. Second, regarding the included studies, most prognostic models were developed using retrospective data and may therefore be subject to selection and information bias. When retrospective designs are used, propensity score methods can be considered to help reduce potential bias. Substantial heterogeneity existed across studies in model development methods, sample characteristics, follow-up durations, and validation strategies, which may lead to different accumulation of death events and thus complicate direct comparison and synthesis. Moreover, handling of confounding factors was inconsistent; for example, adjustment for key clinical variables such as ulcer and infection severity varied across studies, which may affect the stability and comparability of model performance. In addition, most studies did not stratify mortality by cause, and it was not possible to separate deaths directly attributable to DFU from deaths due to other comorbidities. Therefore, this review focused on all-cause mortality, which may limit the applicability of the prognostic models specifically to DFU-related deaths. These findings highlight the need for prospective, large-scale, multicenter studies with systematic adjustment for important confounders and a stronger external validation to improve the reliability and applicability of DFU mortality prognostic models.
KEY FINDINGS
All included models demonstrated high ROB, mainly due to issues such as inappropriate data sources, small sample sizes, inadequate handling of missing data, and insufficient model calibration and validation.
Age, cardiovascular disease, renal disease, ulcer severity, ischemia, and Alb were the most frequently included and clinically significant predictors across models.
This systematic review included 22 models. All models were rated as having a high ROB based on the PROBAST assessment, indicating that none met the current methodological quality standards. While the identified risk factors are not novel, our synthesis confirms their relevance and highlights consistent methodological limitations across studies. To improve the quality of future research, investigators should rigorously adhere to the PROBAST framework to improve future model development. Clinically, current DFU mortality prognostic models should be interpreted with caution due to their limited prognostic accuracy. Sole reliance on these models may result in misclassification of patient risk. This is particularly problematic when models are poorly calibrated, as risk estimates may systematically over- or underestimate true mortality probabilities in real-world settings. Until high-quality models are rigorously validated, clinicians should base decisions on comprehensive clinical assessments and prioritize consistently reported risk factors, including age, cardiovascular disease, renal disease, ulcer severity, ischemia, and Alb. Looking ahead, once rigorously validated, these models could be integrated into routine clinical workflows to enhance risk stratification and guide individualized management. For instance, embedding validated models into electronic health record systems could enable automated risk calculations at the point of care and trigger clinical alerts for high-risk patients, facilitating timely multidisciplinary interventions.
INNOVATION
DFUs are a serious complication of diabetes, often leading to increased mortality risk. Accurate prediction of mortality risk is essential for guiding timely clinical interventions and optimizing patient outcomes. This study systematically reviewed 22 published mortality prognostic models for DFU patients, derived from 19 studies. It identified key methodological limitations in the existing literature and synthesized high-frequency risk factors with stable predictive value to inform future model refinement and development. The findings provide useful guidance for improving risk stratification and support more personalized, evidence-based care for patients with DFUs.
AVAILABILITY OF DATA AND MATERIALS
All data collection forms, extracted data, and analysis materials used in this review are available from the corresponding author upon reasonable request. No public repository was used.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors declare no conflicts of financial or nonfinancial competing interest. This article was solely authored by the individuals listed, with no involvement of ghostwriters in its preparation.
Footnotes
FUNDING INFORMATION
The study was funded by the Health Science and Technology Project of the Pudong New Area Health Commission (grant/award number: PW2023A-09), the Academic Leaders Training Program of Pudong Health Bureau of Shanghai (grant/award number: PWRd2022-16), and the Tongji University “Third Year Action Plan for Discipline. Construction of School of Nursing” (Grant/Award Number: JS2210328).
ABOUT THE AUTHORS
Supplemental Material
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.