
Abstract
Due to its exigency and humanitarian nature, health aid is less political and thus less vulnerable to domestic and international criticism than other types of foreign aid. Ironically, this makes health aid an effective policy tool for donors to cultivate or improve relations with recipients that have divergent foreign policy preferences from donors. This implies that health problems caused by pandemics/epidemics and associated health aid can create an opportunity to ameliorate historically troubled relationships between states. By examining the link between bilateral health aid flows and differences in foreign policy preferences between 24 donors and their recipients from 1990 to 2017, this paper presents findings that support this claim. The theoretical arguments and empirical findings of this paper offer novel insights into the politics of health aid.
Introduction
With the deterioration of global environmental and health conditions in many parts of the world, particularly during COVID-19 pandemic (Gheorghe et al., 2020), health aid has become increasingly important in addressing health challenges in developing countries. One of the issues faced by health aid is the mismatch between need and supply. One of the fundamental reasons for this asymmetry is that, given limited resources, donor states need to prioritize their assistance to recipient states. Here, strategic consideration can play an important role in the decision process. How do donors select their targets of health aid? Is the disbursement of health aid driven by factors similar to the ones that account for flows of other types of foreign aid such as military and economic aid?
It is well known that strategic considerations along with humanitarian motives significantly affect foreign aid disbursement. Such considerations include the political importance of recipients in international politics (e.g. the membership of the United Nations Security Council (UNSC)) (Hwang, Sanford, and Lee, 2015; Kuziemko and Werker, 2006), economic ties or security partnership (Alesina and Dollar, 2000), and political alignment of recipients with donors (Gibler and Rider, 2004; Wolford, 2015). According to the political economy approach, donors tend to provide aid to states that maintain similar foreign policy preferences (Fleck and Kilby, 2010). By offering foreign aid to states that maintain similar foreign policy preferences, donor states can consolidate their political and military ties with recipients especially if recipients are their security allies (Gibler and Rider, 2004; Wolford, 2015).
Therefore, it is reasonable to speculate that health aid, much like other types of foreign aid, also flows to states that are friendly with donor states in terms of political alignment over foreign policy issues. However, as Figure 3 which portrays the flow of health aid from 24 major donor states between 1990 and 2017 shows, the results do not conform to patterns observed in previous research on foreign aid. Contrary to the trends observed in other forms of assistance, a greater amount of health aid from donor states tends to be allocated to recipient states with divergent foreign policy preferences than to those maintaining similar foreign policy preferences, although they are not necessarily the ones that need it most. For example, during the COVID-19 pandemic, the United States has given a great amount of health aid to Ethiopia and Syria, although they suffer from the pandemic relatively less than others and maintain very divergent foreign policy positions from the United States. 1 This puzzling finding implies that disparate theoretical mechanisms may account for the disbursement of health aid as compared with the flows of military or economic aid.
This paper argues that by nature, health aid is less politically salient and thus less vulnerable to domestic and international criticism than military or economic aid. This makes health aid a preferred form of aid for donors to provide to recipients that maintain divergent foreign policy preferences. Health aid can serve as a policy tool for donors to cultivate or construct positive relations with their rivals in foreign policy, while it is difficult for donor states even to provide military or economic aid to recipients endorsing opposite policy preferences in the context of world politics. By examining the link between bilateral health aid flows and differences in foreign policy preferences between 24 donors and their recipients from 1990 to 2017, this paper presents findings that support this claim. The theoretical arguments and empirical findings of this paper offer novel insights into the politics of health aid.
The politics of health aid and foreign policy preferences
Foreign health aid is essential for many developing states to address various issues such as fighting epidemics or pandemics, offsetting the health problems caused by lack of medical supplies and vaccines, and tackling the health problems of migrants and refugees. Studies report that health aid is positively associated with improvements in health outcomes such as life expectancy and mortality in the recipient (e.g. Bendavid and Bhattacharya, 2014). Nevertheless, mismatches between health needs and aid flows persist (Dieleman et al., 2014; Esser and Bench, 2011).
The asymmetry between the need and supply of health aid is portrayed in Figure 1. The figure shows the trend of Development Assistance for Health (DAH), disability-adjusted life-years (DALY) and the total number of deaths caused by health-related diseases.
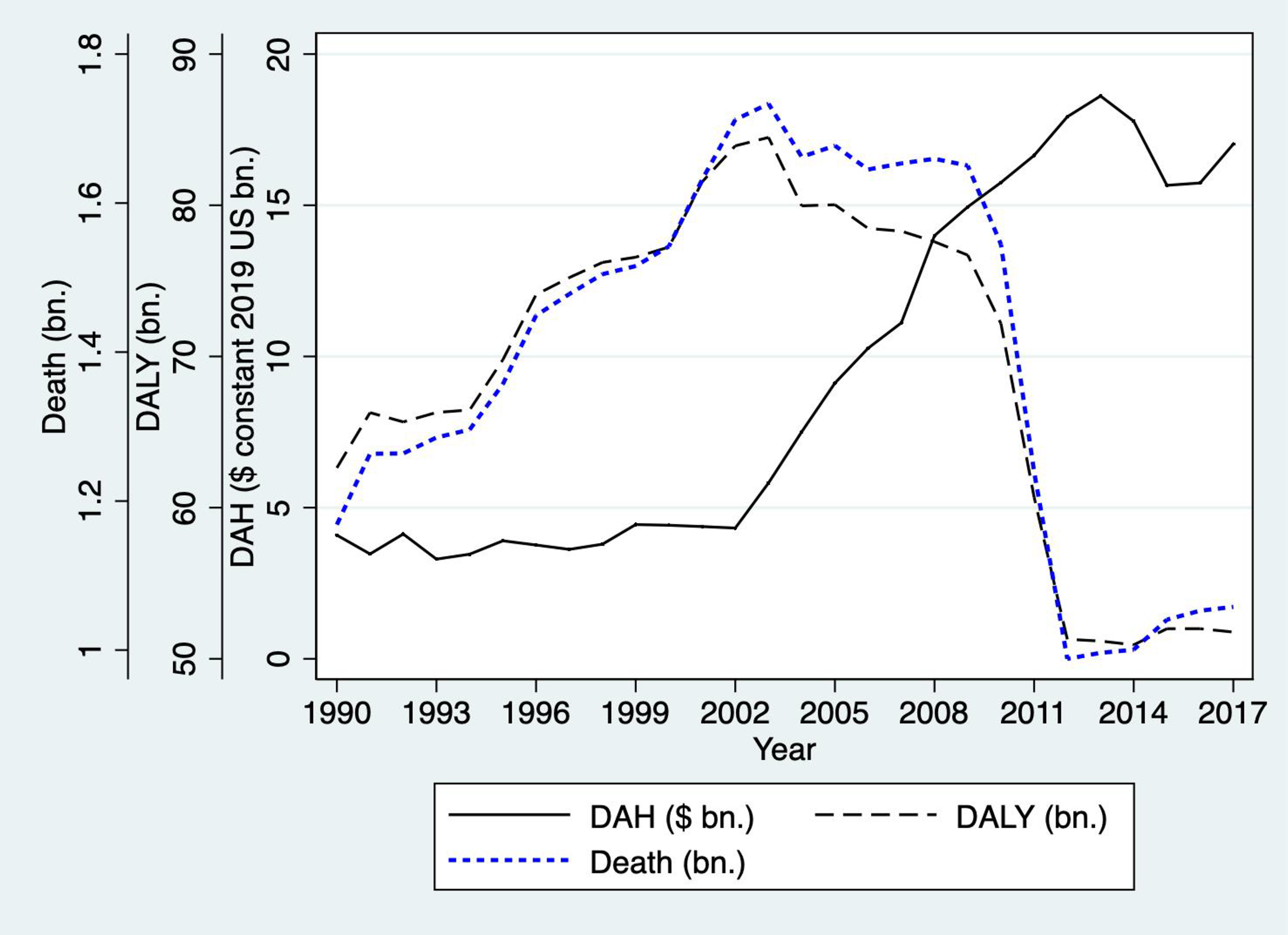
Health aid needs and disbursement (1990–2017).
DAH is “the financial and in-kind resource transferred from major health development agencies to low-income and middle-income countries with the primary intent of improving or maintaining health” (IHME, 2020, 2). DALY has been promoted by the World Health Organization (WHO) and other international institutions as an important concept defining health conditions. It measures the number of years of life lost due to premature deaths combined with the number of years lived with disability due to diseases (Global Burden of Disease Collaborative Network, 2020).
As the figure shows, there is a significant mismatch between actual health aid flows and demand for health aid. Although their scales are different, it clearly appears that there existed a large gap between health needs and supply before 2003 at the global level. While the numbers of DALY and deaths increased rapidly from 1990 to 2002, DAH did not show a large change during the same period. Interestingly, after 2002, DAH continued to increase, while the numbers of DALY and deaths decreased significantly after 2008. The trend shown in the figure may invite multiple interpretations. 2 Notwithstanding the numerous possible explanations, the numbers show that the disbursement of health aid is not directly commensurate with actual health needs, implying that strategic considerations may play a role in the decision of health aid disbursement. 3
Three main different approaches account for foreign aid disbursement (Bueno De Mesquita and Smith, 2009; Milner and Tingley, 2010): the need-based, the social environment-based, and the donor-interest-based strategic approaches. These three approaches are not necessarily substituting. Rather, they complement each other to account for health aid allocation politics. The need-based approach focuses on the needs of recipients. Serious security, economic, or humanitarian challenges facing recipients such as poverty alleviation and rescue from natural disasters may explain foreign aid flows to some extent (Alesina and Dollar, 2000; Boone, 1996; Collier and Dollar, 2002). The practical needs of the recipient, such as poverty alleviation, sustainable development, and rescue from pandemics or natural disasters, are significant factors that may explain foreign aid flows.
The social environment-based approach emphasizes the social environment surrounding donors and/or recipients in explaining a regional or global trend of foreign aid. International norms, cultures, and activities that are associated with foreign aid may generate pressure upon states to behave similarly (Shiffman, 2006), producing a common trend across states which may contribute to the mismatch between the need and the supply of health aid. Global health networks and their varying roles in shaping health issues may explain different outcomes of funding and states’ health policies (Shiffman et al., 2016).
The donor-interest-based strategic approach posits that foreign aid flows may be determined by donors’ political or strategic interests. In view of this approach, health aid is considered as a policy tool for donors to promote their national interests. For example, it is well known that states holding political power in the UN Security Council as temporary members tend to receive larger amounts of foreign aid more frequently than do other nonmembers (Hwang et al., 2015; Kuziemko and Werker, 2006). This example shows that the underlying motivation beneath foreign aid flows may be political. In addition to political considerations, economic factors may also affect donor states’ allocations of foreign aid. Donor states may want to assist their economic or security partners in order to consolidate their ties and promote mutual interests (Alesina and Dollar, 2000; Jung et al., 2018). Moreover, as political leaders in a donor state need to consider the distributional effects of foreign aid in their home economy (Milner and Tingley, 2010), foreign aid is likely to flow into a recipient whose economy is closely tied to the donor's economy.
Alignment of foreign policy preferences may also affect disbursement of foreign aid. By offering foreign aid to states that maintain similar foreign policy preferences, donor states can consolidate their political and military ties with recipients especially if recipients are their security allies (Gibler and Rider, 2004; Wolford, 2015). For example, during the Cold War, South Korea, and the other Asian Tigers received tremendous amounts of foreign aid from the United States and other allies (Dreher et al., 2013). Foreign aid provided by the United States to European states under the Marshall Plan is another example of foreign aid widely considered to have the political motivation of securing allies. By providing seed money for the recovery of Western Europe, the Marshall Plan transformed its beneficiaries from poverty cases into partners (Kunz, 1997).
Despite extensive research into the disbursement of foreign aid, few studies have examined the differences between health aid and other types of aid such as military or economic aid. The question of whether health aid disbursement is driven by factors similar to those that explain military or economic aid has thus not yet been extensively addressed.
In comparison with military or economic aid, health aid disbursement can be driven more by humanitarian purposes. Nevertheless, much like other types of foreign aid, health aid can also be utilized as a policy tool to promote donors’ national interests. In 2009, the Assistant Secretary of State Kerri-Ann Jones in the United States affirmed that “better global health promotes stability and growth, which can deter the spread of extremism, ease pressure for migration, reduce the need for humanitarian and development assistance and create opportunities for stronger political alliances and economic relations” (Jones, 2009). These priorities have prompted the U.S. government to invest heavily in new mechanisms to implement ambitious global health initiatives while at the same time securing favorable perceptions in a changing diplomatic space (Kates et al., 2010). Bliss (2011) reports that with several decades of experience engaging in overseas development assistance for humanitarian, strategic, and ideological purposes, Russia and China have become more active on global health policy issues within WHO, the UN, and in other regional and global fora. Both countries seek to use their position as donors in the global health sphere to cement influence, secure access to raw materials in foreign countries, and protect their own sovereign interests. In a similar context, based on case studies of the United Kingdom, Brazil, Norway, and Switzerland, Gagnon (2012) claims that the primary reason that these countries have decided to focus more on global health is driven by self-interest: that is, to protect their national and international security as well as economic interests. Investing in global health is also seen as a way to enhance a state's international reputation and to serve the domestic economic objectives of donor states. For example, China today utilizes development assistance for health not only to expand its global influence and improve its international image, but also to serve the market and resource needs of its domestic economic development (Huang, 2014). Arguably, other states including the United States also disburse aid for similar reasons.
Previous research makes it possible to infer that strategic considerations may act as explanatory factors for health aid disbursement in addition to other forms of foreign aid. However, while strategic considerations may play a part in most forms of foreign aid, large discrepancies exist in terms of the target recipients of health aid as compared with targets of military or economic aid. Figure 2 portrays the relationship between flows of development aid and foreign policy preference differences between donors and recipients from 1990 to 2012. The data was collected from William & Mary's Global Research Institute (Tierney et al., 2011).
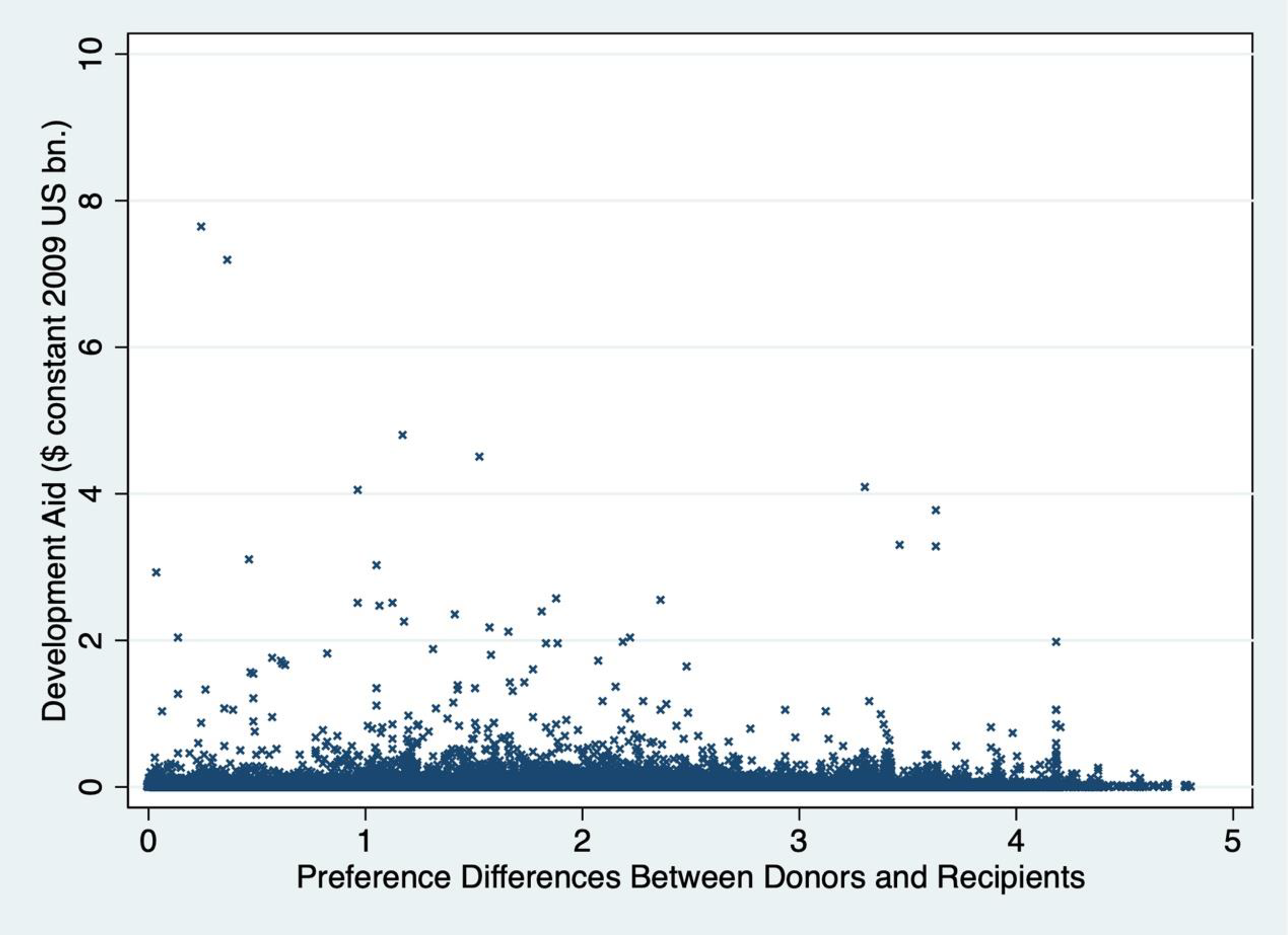
Foreign policy preferences and development aid (1990–2012)†. † Foreign policy preference differences are measured by the absolute values of ideal point estimate differences between a donor and a recipient produced by Bailey et al. (2017).
While the figure does not present a striking pattern between development aid and foreign policy preference differences, it is possible to observe that larger sizes of development aid tend to flow to recipients that reveal foreign policy preferences similar to those of their donors. The result is consistent with the previous argument that foreign aid tends to go to strategic partners that maintain similar foreign policy preferences and provide political support for donor states (Fleck and Kilby, 2010).
When it comes to health aid, however, the relationship between foreign aid flows and foreign policy preference differences diverges from that shown in the previous Figure 2. As Figure 3 shows, a large scale of health aid frequently tends to go to recipients that maintain divergent foreign policy preferences from donors, which is puzzling. Why do states send health aid to recipients with foreign policy positions that do not align with their own rather than to those that maintain similar policy positions? 4 We argue that one of the reasons is that health aid may serve as an effective policy tool for donors to cultivate and improve relations with states which have foreign policy preferences which are divergent from their own.

Foreign policy preferences and health aid (24 donors)†. † Foreign policy preference differences are measured by the absolute values of ideal point estimate differences between a donor and a recipient produced by Bailey et al. (2017).
Health aid toward states with dissimilar foreign policy preferences
From a theoretical viewpoint, foreign aid can be sent even toward rival or hostile states as an inducement or a reward for their policy cooperation with donors. Relatedly, Early and Jadoon (2016) report that the imposition of economic sanctions by the United States is positively associated with foreign aid flows to a target, which is motivated by donors’ self-interest in political or commercial benefits. In other words, states can utilize both inducement and punishment methods to increase its chance to achieve certain policy goals. In this vein, foreign aid can be used to complement or substitute other foreign policy options such as initiation of military action against rivals (Palmers, Wohlander, and Morgan, 2002; Peksen, 2019). Practically, however, foreign aid faces various limitations in serving this end. First, political leaders in donor states may face strong political criticism or opposition domestically and internationally if they provide aid to their enemies or rivals. Bueno de Mesquita and Smith (2007) argue that leaders make aid and policy decisions with an eye to how they influence political survival. If this is the case, when foreign aid is offered to states that reveal extremely divergent foreign policy preferences and stand against the donor states over contentious issues in world politics, leaders in donor states are likely to pay high political costs domestically.
Second, buying votes or drawing political concessions from enemies would be costly (Bueno de Mesquita and Smith, 2009). When recipients consider foreign aid to be a means for donors to coopt the recipients rather than an expression of sincere benevolence, foreign aid may fail to draw positive sentiments from the public or policy cooperation from the recipient governments (Kegley and Hook, 1991). This is particularly the case when the recipients hold foreign policy preferences that differ widely from those of donors. Simply put, foreign aid may not serve effectively to draw policy cooperation from a hostile state.
Third, it is possible that foreign aid provision may signal the weakness of donor states, which may eventually make negotiations with their rivals/enemies more difficult. Electing to employ carrots over sticks as a foreign policy mechanism can transmit information regarding dovish foreign policy and weakness of a donor state to a hostile recipient. This information may weaken the donor's bargaining leverage, making it more difficult to draw policy concessions from the recipient state. This perspective is consistent with Lektzian and Sprecher's (2007) argument on the relationship between economic sanctions and military force. Since the use of sanctions may signal the sender's indecision or weakness by not employing military force, the senders often fail to achieve their policy goals and are likely to be involved in a militarized dispute after using sanctions. Such a possibility poses obstacles for donor states when determining whether to utilize foreign aid as a policy option towards rival/hostile states. Even if the donor state is willing to provide foreign aid, the nature of foreign aid as an outcome resulting from negotiations makes disbursement impossible without consent from the recipient state. States that are not friendly to donor states’ foreign policy positions are less likely to agree to receive aid than states that share similar policy preferences with donors. Overall, although utilizing foreign aid (particularly economic aid) as a policy tool in negotiating with rival or hostile states is possible in some cases, obstacles posed by workings within donor and recipient states prevent it from becoming the dominant trend observed in international politics.
Meanwhile, health aid differs from economic or military aid in many aspects. First, even if health aid is disbursed to unfriendly states, leaders in donor states are less likely to face strong political criticism or opposition domestically and internationally. The insalubrious impacts of health problems such as pandemics on public health and well-being are widespread and severe. Without proper assistance from international communities, people in societies hit hard by health problems suffer significantly. Health problems engender pervasive ramifications that often call for immediate and copious amounts of assistance, and the nature of health aid is often strongly humanitarian. Thus, the international or domestic audience costs that leaders in donor states may pay for electing to provide health aid is often minimal in health aid as compared to economic or military aid.
Second, while it is possible for recipient states to perceive economic aid as a bribe and thus potentially balk at accepting it, health aid is less likely to generate such negative reactions from recipient states. By nature, health aid is unlikely to be employed as a reward conditional on the political cooperation of a recipient in the interests of the donor state. Thus, health aid, if provided at an appropriate time, can generate positive sentiment towards a donor from both citizens and the government in the recipient state. For example, a health aid program targeted to address HIV and AIDS substantially improved perception of the United States (Goldsmith et al., 2013).
In a study of the effects of different types of foreign aid, Dreher et al. (2008) reported that general budget support or grants generate political support for donor states in the recipient state while loans and food aid are not effective in doing so. This implies that benevolent health aid can be appreciated even by hostile states and their citizens. While development aid may not benefit but harm the recipient's citizenry (Bueno de Mesquita and Smith, 2009), health aid is likely to benefit not only political leaders but also the citizens in recipient states. One reason for this is that public health aid comes via smaller-scale projects that are often directly supported by non-governmental organizations and other multinational donors, making such aid projects less dependent on recipient institutions (Dietrich, 2011). In this regard, in comparison with development aid, recipients are more likely to regard health aid as a public good rather than a private good.
Third, instead of signaling weakness as is often the case in economic aid, health aid may allow a donor state to effectively signal its benevolent intentions to the recipient. In addition, it would be easier for donors and recipients to agree on the transfer of health aid. Due to deteriorating health conditions and the urgency of addressing health issues, health aid can be transferred to recipients in need relatively easily.
Overall, in many aspects, health aid is viewed to be less political and thus faces less domestic and international criticism or opposition than economic or military aid. Ironically, these characteristics make health aid a powerful tool for donor states that aim to build up or improve relations with rivals or unfriendly states in the long run. By offering health-related assistance, donor states may have a better chance to improve their historically troubled relations with recipients like in the case of the United States toward Cuba (Morrison and Gannon, 2015) or draw support for political stances like in the case of China toward African states in the 1960s with respect to diplomatic recognition over Taiwan (Huang, 2014). By sharing resources and exchanging scientific and medical knowledge, states can secure the chance to work together and learn lessons about how to promote cooperation among themselves. Based on this speculation, we present the following hypothesis to test our argument.
Hypothesis: As foreign policy preference differences between a donor and a recipient increase, the volume of health aid from donor to recipient is also likely to increase.
Research design
Variables and data
The dependent variable is bilateral health aid flows between 24 donors and their recipients from 1990 to 2017. Development Assistance for Health includes health aid flows to eight different areas: newborn and child health, reproductive and maternal health, HIV/AIDS, tuberculosis, malaria, other infectious diseases, non-communicable diseases, and sector-wide approaches and health system strengthening. This study utilizes the actual disbursement of DAH between states. A natural log form of DAH is used. The data was collected from the Institute for Health Metrics and Evaluation (IHME, 2020).
The key explanatory variable is the foreign policy preference difference between a donor and a recipient state. Scholars of international relations have frequently utilized states’ voting data in the UN General Assembly to estimate states’ foreign policy preferences (i.e. ideal points). Following this common practice, we use the estimates produced by Bailey et al. (2017). We measure foreign policy differences by the absolute values of estimate differences between a donor and a recipient. As discussed above, we expect that as foreign policy preference differences between a donor and a recipient increase, the volume of health aid is likely to increase.
Several control variables that are essential in understanding health aid flows and strongly associated with foreign policy preference differences are included in this study. Some of these variables possibly generate confounding effects on the link between foreign policy preference differences and health aid, causing a spurious association between the key variables. Regime types of a recipient or alliance ties between a donor and a recipient are possible candidates. We performed robustness tests of the models by including and subsequently excluding these variables in our models. Considering that most donor states in our data are advanced democracies, we expect that democratic states are likely to receive a high volume of health aid. In terms of alliance, we expect that a recipient that has an alliance tie with a donor is likely to receive more health aid than a nonally.
The conventional wisdom tells us that states with a conflict history are less likely to exchange foreign aid with each other than others. When it comes to health aid, however, we may not be able to observe such negative externalities. Due to political motivations to cultivate relationships and/or humanitarian reasons, donor states may send health aid to hostile states with conflict history as much as they do to nonhostile states. Militarized Interstate Disputes (MIDs) variable is coded as one if two states have had an MID in the last three years and otherwise zero. The data comes from the Correlated of War project (Maoz et al., 2019).
In addition, we control for the needs of health aid in a recipient. Both disability-adjusted life years and the number of deaths caused by health-related diseases in a recipient are used to this end (Global Burden of Disease Collaborative Network, 2020). Due to the shared understanding of the urgency caused by health issues and the impact that these issues may have, states that have experienced serious health-related causalities are more likely to disburse health aid to others afflicted by a similar health crisis. In this regard, we also control for DALY and the death numbers occurring in donor states. These variables are log-transformed.
In addition to disease burden, GDP per capita also affects health aid flows. It has been observed that high-burden, low-income countries receive a large amount of DAH regardless of health focus areas (Dieleman et al., 2014). By including GDP per capita (constant 2010 US dollars) in our models, we control for this factor. The data comes from the World Bank (World Bank, 2021). Geographical proximity is also a factor that may influence health aid flows. It is likely that donor states prioritize health aid to recipient countries when the health problem may potentially spread to the donor state, affecting its public health. Thus, concerns about the spread of infectious diseases to citizens within the donor state may motivate health aid flows. To account for such strategic interests, we control for geographical distance between donor and recipient states. A natural log form of geographical distance in miles between states is used. We expect that as the geographical distance increases, the volume of health aid provided to the recipient will decrease. The political and strategic value that a recipient carries may also affect health aid flows. To control for the political importance of a recipient, we also control for the recipient's member status in the UNSC. A member of the UNSC is more likely to receive health aid than non-members. In addition to political value, the economic value of a recipient may also impact decisions of donor states. To control for such interests, we include trade ties between a donor and a recipient in the models. A natural log form of bilateral trade volume is used.
Estimation
Since our data has a panel data structure, we utilize pooled OLS/WLS regression with Driscoll–Kraay standard errors. These standard errors are heteroskedasticity consistent and robust to general forms of cross-sectional and temporal dependence. By using four lags of the dependent variable, we address the concern of a high order of autocorrelation. In addition, to account for possible temporal and/or donor-specific effects, we include a set of year-fixed effects and/or donor-state fixed effects. 5
Results
Table 1 reports test results from models with different combinations of control variables. As expected, the variable of foreign policy preference differences has positive significant effects on the flow of health aid in all four models. For example, in Model 1.4, the results indicate that a one unit (or one standard deviation) increase of preference differences is likely to promote health aid by about 110% (or 72.9%), which is a substantively significant change. 6
Divergent foreign policy preferences and health aid (1990–2017).
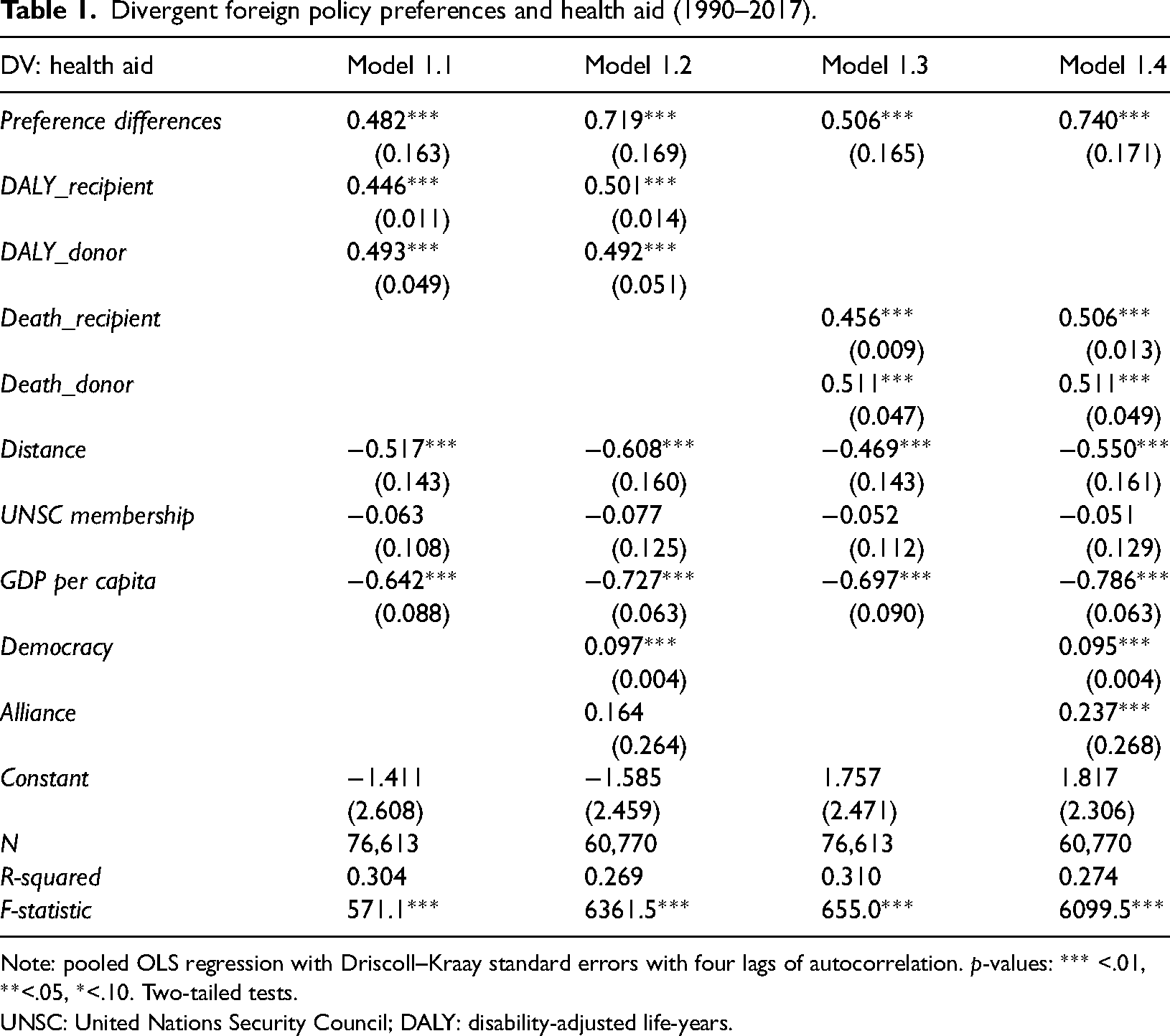
Note: pooled OLS regression with Driscoll–Kraay standard errors with four lags of autocorrelation. p-values: *** <.01, **<.05, *<.10. Two-tailed tests.
UNSC: United Nations Security Council; DALY: disability-adjusted life-years.
The results remain significant even when we include year and donor fixed effects and trade as controls in models in Table 2. For example, in Model 2.2, a one-unit increase in preference differences is likely to expand health aid by about 27%.
Foreign policy preference differences and health aid (1990–2017).

Note: pooled OLS regression with Driscoll–Kraay standard errors with four lags of autocorrelation. p-values: *** <.01, **<.05, *<.10. Two-tailed tests.
UNSC: United Nations Security Council; DALY: disability-adjusted life-years.
Control variables also appear to perform as expected. The level of health needs is positively associated with health aid. In Model 1.4, a 10% increase in a recipient's DALY is likely to promote health aid by 4.9%. Similarly, a 10% increase in the number of deaths increases health aid by about 4.8%. As the geographical distance between donors and recipients increases, the size of health aid tends to decrease. Moreover, states with lower GDP per capita are likely to receive a large size of health aid than more affluent ones. Democratic states are likely to receive health aid more than non-democratic states.
As expected, trade partners tend to receive health aid more from donor states. Interestingly, donor states also tend to send health aid more to states with a conflict history (i.e. at least one militarized interstate dispute in the last three years) than to those without a conflict history. This surprising finding is consistent with the main claim of this research. For the strategic purpose of cultivating relationships, health aid can be allocated to states with dissimilar foreign policy preferences or hostile history.
Meanwhile, we fail to find evidence that temporary members of the UNSC receive more health aid. Allies of donor states tend to receive health aid more than non-allies. However, the performance of the alliance variable is not stable particularly in Table 2. This inconsistent finding may be caused by many missing values due to the inclusion of trade variables in Models 2.3 and 2.4. Further speculation and examination would be desirable.
In sum, our findings show that, unlike other forms of foreign aid such as military or economic aid, health aid is likely to flow to states that have dissimilar foreign policy preferences from those of donor states. The results support our claim that donor states may utilize health aid out of strategic interest to cultivate and improve their relations with their rivals or historically troubled states.
Conclusions
This study examined the underlying mechanisms explaining the asymmetry between need for health aid and actual aid flows. We claim that donor-interest-based motivations could be significant factors that contribute to the asymmetry. In terms of donors’ strategic interests, however, health aid may differ from military or economic aid.
The possible factors affecting their differences include the political costs for leaders in donor states, the costs imposed by recipient states in the negotiation progress, and the signal sent to a recipient by the act of disbursing foreign aid and its possible impact on future negotiations. In the case of economic and military aid, giving aid to rival/hostile states often incurs significant political costs and potentially threatens the political survival of leaders in donor states. Moreover, there are high costs involved in buying votes or drawing political concessions if the recipient reacts negatively to attempts to give foreign aid. In addition, when recipient states are hostile, disbursement of military or economic aid may signal weakness of the donor state and paradoxically make future negotiations more difficult. In the case of health aid, however, the humanitarian and often urgent nature of health crises ensure that the national and international political costs associated with disbursing aid is comparatively low. Moreover, health aid is more effective as a way to signal benevolent intention of donor states to recipient states when compared to other forms of aid.
Due to these differences, the disbursement of health aid can be driven by a different set of donors’ interests. While other forms of aid are often allocated with the purpose of consolidating political and military ties with recipient states, health aid tends to flow more to recipients that maintain vastly different foreign policy preferences in world politics from donors possibly with the aim of cultivating or improving relations with them. Our findings offer empirical support for this claim.
Ironically, the argument and findings imply that global/regional health problems caused by pandemics/epidemics can create opportunities for states to utilize health aid and diplomacy as a policy tool to improve their relations with historically troubled or hostile others. In the sense that multiple policy options including both punishment methods such as economic sanction and military actions and inducement methods such as foreign aid can be jointly utilized even toward rival or hostile states to draw policy cooperation, donor states can explore opportunities created by global/regional health disasters to engage with recipient states. When offered at appropriate times with benevolent intentions, health aid can serve as a stimulus to improve relations between donors and recipients at least in the long run. In this regard, further studies will benefit by exploring how health aid and diplomacy have worked in promoting cooperation between states particularly those with dissimilar foreign policy preferences.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Korea Foundation.