
Abstract
Background/objective(s)/introduction:
Tissue engineered scaffolds fabricated by 3D printing promises to enhance the success rate in alveolar bone augmentation. The aim of this study was to construct and characterize a 3D printed poly(ε-caprolactone; PCL) scaffolds treated with bone morphogenetic protein 2 (BMP-2) and carrying human gingival mesenchymal stem cells (hGMSCs) for potential use in the augmentation of alveolar bone.
Materials and methods:
PCL scaffolds with defined pore geometry were fabricated by 3D printing using fused deposition modeling (FDM) and treated with O2 plasma to enhance BMP-2 and cell adhesion. The scaffolds were characterized by compression testing, scanning electron microscopy (SEM), and water contact angle measurement. BMP-2 was bound to the surface, and hGMSCs from gingival connective tissue were seeded onto the scaffolds. BMP-2 was quantified by elisa. The cells were identified as stem cells based on their differentiation capacity and immunophenotypic profile. Osteogenic differentiation on BMP-2 bound scaffolds was assessed using alkaline phosphatase (ALP) activity and calcium deposition assays.
Results:
Compressive modulus of the PCL scaffolds (73.2 ± 17.1 MPa) was close to human alveolar bone (96.2 ± 40.6 MPa). SEM revealed a porous design with continuous struts, creating an average pore size of 400 µm and zig-zag channels suitable for cell infiltration and adhesion. O2 plasma treatment decreased the water contact angle from 110° ± 4° to 59° ± 2°, indicating improved surface hydrophilicity. ELISA showed that over 98% of BMP-2 remained bound to the scaffold for 28 days, indicating prolonged growth factor presence during cell culture. Within the environment created, BMP-2 bound scaffolds led to a threefold increase in ALP activity and higher calcium deposition compared to controls, confirming enhanced osteogenic differentiation.
Conclusion(s):
3D printed PCL scaffolds functionalized with BMP-2 and seeded with hGMSCs exhibited highly improved in vitro osteogenic properties which promises to improve alveolar bone augmentation results.
Keywords
Key messages
Tissue engineered, 3D printed PCL scaffolds functionalized with BMP2 and seeded with hGMSC cells showed enhanced osteogenic potential in vitro.
The 3D printing process allowed fabrication of scaffolds with controlled pore distribution and internal architecture ensuring optimal cell performance.
hGMSCs exhibited high differentiation capacity, confirming their suitability as an accessible and potent stem cell source for bone tissue engineering.
Introduction
Dental implants are the most common treatment following tooth loss. 1 Alveolar bone deficiencies resulting from missing teeth may require procedures such as sinus lift, guided bone regeneration, or block grafting—using bone grafts or polymeric materials—to establish adequate bone volume for implant placement. While horizontal bone augmentation yields predictable outcomes, vertical bone augmentation carries a significantly higher complication rate. 2 Biodegradable polymers such as polylactic acid(PLA), polyglycolic acid(PGA), polylactic acid-co-glycolic acid (PLGA) and polyε-caprolactone(PCL) are the most common polymers used to fill the defect sites. One of the most popular and promising techniques to fill these sites is to use additively manufactured (3D printed) scaffolds especially for large bone defects to achieve a perfect fit with scaffolds with correct shape, inner architecture and highly controlled porosity. 3 Recent advances in additive manufacturing have facilitated the translation of 3D-printed scaffolds from preclinical research into early clinical applications for alveolar bone augmentation. In this context, a prospective clinical study by Mangano et al. 4 demonstrated successful bone regeneration and subsequent implant placement following the use of custom made scaffolds in patients with severe alveolar defects, showing favorable integration and minimal complications. More recently, in the review by Elrefaei et al., 5 digital customization was shown to enhance surgical precision and efficiency in bone regeneration, with improved bone gain and reduced operative time compared to conventional approaches. Supporting these findings, Perez et al. 6 reported favorable clinical and histological outcomes using 3D-printed calcium phosphate blocks for alveolar ridge augmentation, demonstrating new bone formation and vascularization after a 6-month healing period. In addition, recent clinical reports and technical studies have shown that patientspecific 3Dprinted scaffolds—such as PCL-based composite constructs—can achieve successful vertical ridge augmentation in severely atrophic mandibles, enabling subsequent implant rehabilitation with satisfactory stability and anatomical conformity. Despite these encouraging outcomes, current clinical evidence remains limited to case series and early-phase studies, and welldesigned randomized controlled trials with long-term follow-up are still required to establish the routine clinical applicability of 3Dprinted scaffolds in alveolar bone regeneration.4 –6 These scaffolds are designed using Dental Volumetric Tomography (DVT) data and printed with various manufacturing techniques, devices and materials.7,8 An appropriate material to be used as a scaffold in these cases is PCL, a polymer approved by the FDA (Food and Drug Administration of USA) for use in clinical applications. Its use has been reported in extraskeletal regeneration new bone formation. 9 PCL is very suitable due to its low glass transition (Tg) and melting temperatures (Tm) which enable 3D printability at relatively low temperatures such as 50°C–60°C.10,11 Tissue engineering is an interdisciplinary field that involves cell biology, materials science, engineering and clinical research, and aims to create new tissues and organs by bringing together polymeric scaffolds with patient cells. 12 Tissue engineering necessitates the use of appropriate cells for the construction of cell carrying scaffold suitable for the targeted repair. 13 Selection of the cells for tissue engineering is very critical and stem cells are widely used for dental applications due to their high proliferation and differentiation capacity. 14 Mesenchymal stem cells (MSCs) used in these applications are obtained from the oral area. These are generally dental pulp stem cells (hDPSCs) or subepithelial connective tissue gingival stem cells (hGMSCs). 15 MSC application within the scope of regenerative medicine practices can provide less invasive and more conservative treatment for patients of major dental branches such as endodontics, oral surgery and periodontics. Thus, dental treatments might become less costly and less complex. 16
In order to increase the bioactivity of bone cells, bone morphogenetic proteins (BMP) are used. 17 They are known to be osteoinductive growth factors. 18 BMP-2 especially plays a crucial role in stimulating and promoting cell proliferation. 19 As a member of the Transforming Growth Factor-β superfamily, it facilitates bone formation by guiding the differentiation of MSCs into osteoblasts and osteocytes, a process essential for producing the extracellular matrix of bone tissue.20,21 In order to exert its effect, BMP-2 should bind to its specific receptors and initiate a signaling cascade. 22 It typically binds to bone morphogenetic protein receptors (BMPRs) located on the surface of MSCs. This interaction triggers downstream signaling events that lead to osteogenesis. Studies have shown that long term BMP-2 activity is required for effective osteogenesis and bone formation. However, BMP-2 has a short half life in the body because it is rapidly cleared from the bloodstream, and this prevents long term effectiveness. In order to overcome this, large doses are often administered. 23 The larger BMP-2 doses, on the other hand, leads to a number of undesirable effects such as ectopic bone formation, osteoclast mediated bone resorption, as well as inappropriate adipogenesis. 24 Continuous local presence of low amounts of BMP-2 is, therefore, essential for effective osteogenesis. In this study, to address this need, BMP-2 was bound onto 3D printed PCL scaffolds which were then seeded with hGMSCs. The aim of this study was to investigate the in vitro osteogenic potential of a 3D printed PCL scaffold functionalized with BMP-2 and seeded with human gingival mesenchymal stem cells (hGMSCs) for potential use in alveolar bone augmentation.
Materials and methods
Materials
Polyε-caprolactone(PCL, MW: 50,000 g/mol) was from Polysciences, Inc (USA), dexamethasone, from Sigma-Aldrich (Germany), Bone Morphogenetic Protein-2 (BMP-2) from ThermoFisher Scientific (United States), TGF beta 1 protein (TGF-β) from Biolegend (USA). Alkaline phosphatase (ALP) kit from Randox (Northern Ireland), BMP-2 ELISA kit from SunRed (China) and antibodies for immunophenotypical characterizations were purchased from BD Biosciences (USA).
Cell source
The in vitro study was conducted in accordance with the ethical principles of World Medical Association’s Declaration of Helsinki (2008). The hGMSCs were isolated from gingival connective tissues of four donors with approval of Acibadem University and Acibadem Healthcare Institutions Medical Research Ethics Committee (ATADEK-2019/18). All donors were systemically healthy adults (age range: 22–26 years; two male and two female) with no history of periodontal disease, diabetes, smoking, or immunosuppressive therapy. Clinically, all donors presented with gingival thickness greater than 5 mm in the maxillary posterior region, with no signs of active infection or inflammation at the time of tissue harvest, and none had received antibiotic therapy within 2 months prior to tissue collection. The isolated cells were subsequently pooled to minimize inter-donor variability and obtain a representative cell population for the in vitro experiments.
3D printing of the scaffold
Polyε-caprolactone(PCL) scaffolds were fabricated by Fused Deposition Modeling (FDM) method using an Allevi 2 printer at 100°C under 100 psi, using a Gauge 25 (0.455 mm) nozzle. The samples were printed as cylindrical scaffolds (diameter 10 mm, height ca. 4.8 mm, 12 layers), with these macroscale dimensions selected to ensure compatibility with standard in vitro culture systems, allow homogeneous cell seeding, and maintain adequate nutrient and oxygen diffusion throughout the constructs. An interconnected porous architecture was designed with 400 μm gaps between struts, as this pore size is considered optimal for mesenchymal stem cell infiltration, adhesion, and osteogenic differentiation. In the present study, this design was particularly intended to support human gingival mesenchymal stem cell (hGMSC) behavior and to enhance the adsorption and retention of BMP-2 within the scaffold microstructure. Two different models were printedbased on mechanical properties, and cell and BMP-2 adhesion. Both models had layers oriented 90° to each other, with subsequent layers overlapping in Model 1 (Figure 1(a)), while subsequent layers shifted in Model 2 (Figure 1(b)). This single architectural difference resulted in Model 1 having continuous linear channels extending from top to bottom, whereas Model 2 possessed zig-zag channels with no continuous vertical path, which was intended to improve cell retention and BMP-2 adhesion within the scaffold structure.
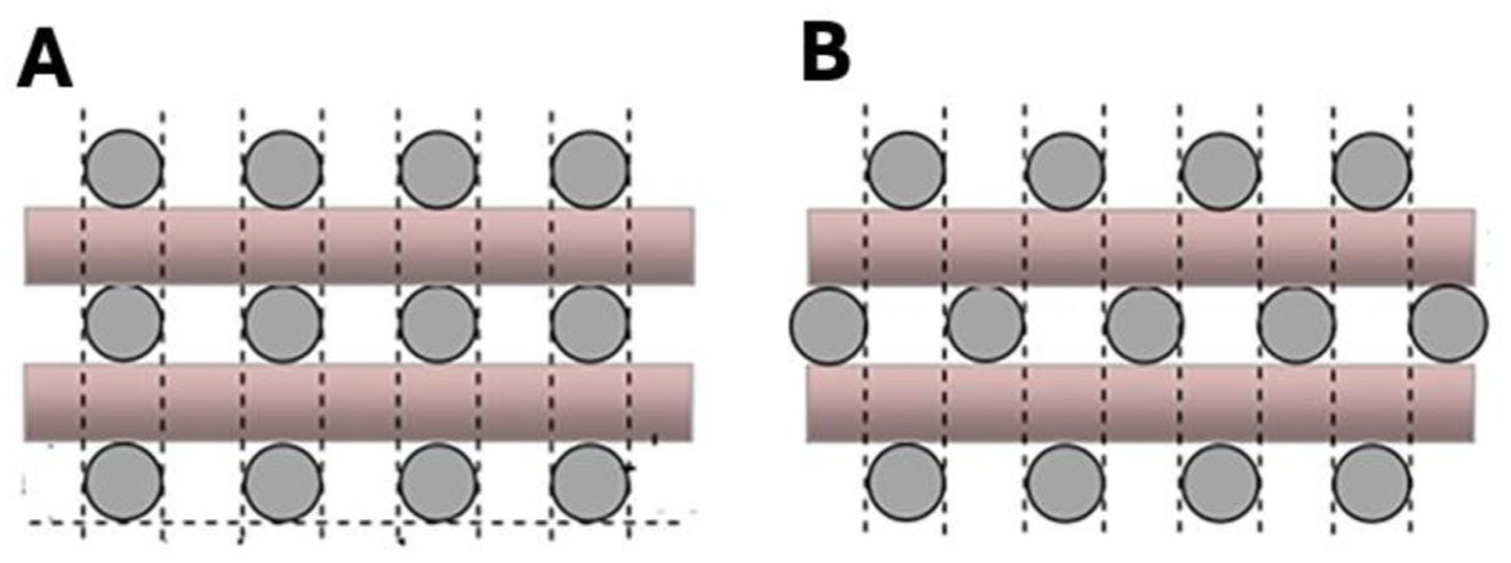
Designs of 3D printed PCL implant: (a) Model 1 and (b) Model 2,Side View.
Characterization of 3D printed PCL scaffolds
Microscopic examination of PCL scaffolds with SEM
The scaffolds were examined with a scanning electron microscope (SEM, Zeiss Evo, MA 10, Germany) after sputter coating with gold to examine the organization of the struts. Analyses were performed on three independent samples (n = 3), and representative regions across each scaffold were imaged to assess structural uniformity. Pore size measurements were done using SEM images to measurethe distance between adjacent struts. Multiple measurements of different regions of each scaffold were made to account for potential variations, and the results are presented as average values.
Mechanical properties
In order to produce a scaffold with a mechanical strength closer to that of the human alveolar bone, the compressive mechanical properties of the scaffolds (diameter 10 mm, height ca. 5 mm) were determined using a mechanical tester (Shimadzu AGS-X Universal Test Machine, Japan). The test was performed at a rate of 1 mm/s and a maximum load of 20 N. Measurements were performed on three independent samples (n = 3), and the results are presented as mean ± standard deviation.
Determination of porosity
Porosity of the product could be calculated by the print dimensions as there are predefined pores in the model but to determine the accuracy of the printing, the scaffolds were studied with scanning electron microscope (SEM, Zeiss Evo, MA 10, Germany) for the strut dimensions and the gaps in between. Measurements were conducted on three independent samples (n = 3), with multiple regions evaluated per sample.
Water contact angle
Water contact angles of both the untreated and the O2 plasma treated (power 50 W, 12 s) PCL films were determined by a contact angle goniometer (Kruss Scientific, Drop Shape Analyzer DSA 100, Germany) using the sessile drop method. Due to the porous and absorptive nature of the scaffold surface, a single droplet was applied per sample. Measurements were performed on three independent samples (n = 3), and results are reported as mean ± standard deviation.
Attachment of BMP-2 on the scaffolds
Attachment of BMP-2 on PCL scaffolds was achieved by treating the scaffolds with oxygen plasma (50 W, 10 s) in an oxygen plasma system (Diener Pico, Germany) system and then immediately immersing BMP-2 solution (5 ng/mL) for 10 min. The scaffold was then introduced to distilled water (5 mL) for 1 min and dried under vacuum.
Release of BMP-2 attached on the scaffolds
The release profiles of BMP-2 were obtained for 28 days by incubating the scaffolds in 1 mL PBS (pH 7.4, 37°C). At specific time points (days 1, 4, 7, 14, 21, and 28), 100 μL aliquots were collected and replaced with an equal volume of fresh PBS. Quantification of BMP-2 concentrations in the collected samples was carried out using a human BMP-2 ELISA kit (Sunred, SRB-T-87684) following the manufacturer’s protocol. In order to construct a calibration curve, BMP-2 solutions in distilled water (12.5, 25, 50, 100, and 200 pg/mL) were prepared. Samples were treated with biotinylated anti-BMP-2 antibody, followed by reaction with streptavidin–horseradish peroxidase (HRP). 25 The enzymatic conversion of the chromogenic substrate was continued for 10 min, and absorbance at 450 nm was measured using a microplate reader. The amount of BMP-2 released at each time point was calculated.
Isolation and culture of hGMSCs derived from palatal subepithelial connective tissue samples
The cell source was gingival connective tissue samples (2 × 2 × 1 mm3) obtained from 4 patients with tooth deficiency in the maxillary posterior region and gingival thickness greater than 5 mm (ATADEK-2019/18 Ethics Committee Approval). Samples were cut into small pieces (0.5 mm3) with scalpel and cultured in α-MEM medium supplemented with fetal bovine serum (FBS, 10%, v/v) in a CO2 incubator at 37°C. The cells isolated from tissue samples of four patients were pooled in equal numbers (5 × 105 cells) at passage 1, cultured and characterized for characterization of the mesenchymal stem cell.
Characterization and differentiation of the isolated mesenchymal stem cell (MSCs)
Immunophenotypic characterization of human gingival mesenchymal stem cell (hGMSCs)
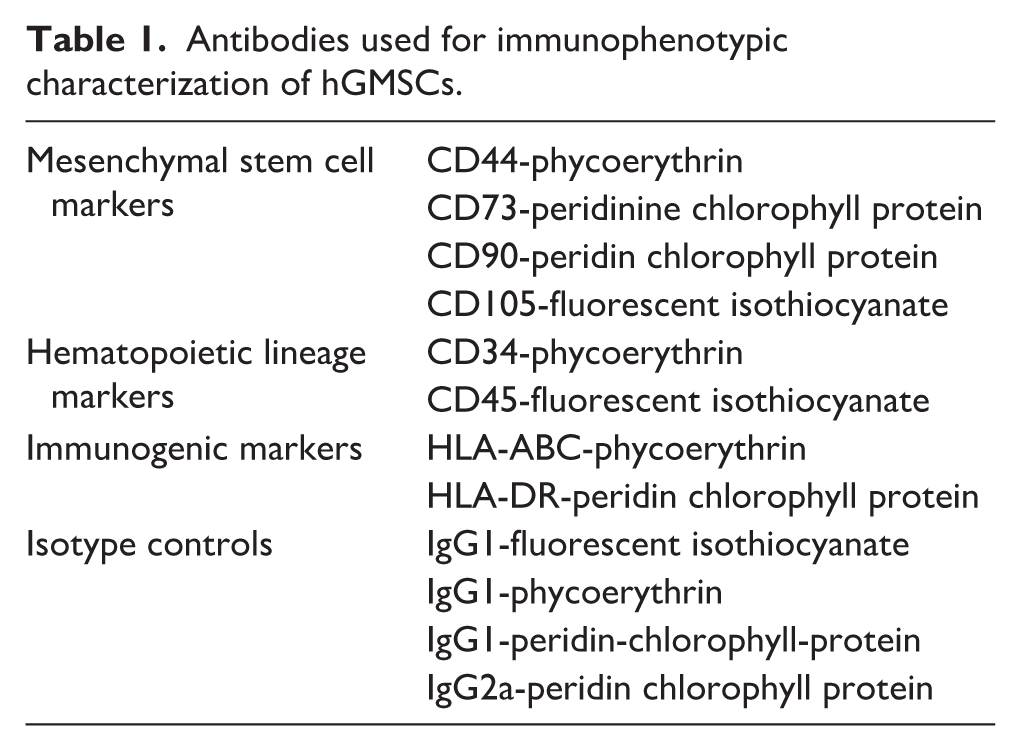
Immunophenotypic characterization of the donor cells was carried out to confirm their identity as mesenchymal stem cells (MSCs). Cells at passage 4 were trypsinized and detached from tissue culture flasks, centrifuged and cell pellets (5 × 105 cells/mL) were fixed with paraformaldehyde (PFA, 4%). Then nonspecific bindings were blocked through incubation in Bovine Serum Albumin (BSA, 1%, w/v in PBS containing 1:1000 sodium azide) for 1 h. Antibodies against cell surface markers (Table 1) were added onto the cells and incubated at 4°C for 1 h. The cells were studied by flow cytometry (BD, Accuri C6 plus, USA) for the cell surface antigens associated with MSCs. CD44, CD73, CD90, and CD105 were the positive MSC markers, and CD31 and CD45 the negative markers. Immunophenotypic analyses were conducted using three replicates (n = 3). Cells were initially gated based on FSC-A versus SSC-A parameters to exclude debris and define the main cell population. During this step, events outside the main population cluster, including potential doublets and aggregates, were excluded by gating, and the analysis was restricted to the primary cell population. Marker expression analysis was subsequently performed within this gated population. In order to control for nonspecific binding and background fluorescence, both unstained cells and appropriate isotype controls were included for each fluorochrome (PerCP IgG1, PerCP IgG2a, PE IgG1, and FITC IgG1). Marker expression was determined based on these controls, and the threshold for positivity was defined according to the endpoint of the corresponding isotype control histogram. Signals exceeding this threshold were considered positive. Furthermore, the presence of immunogenic antigens on cell surfaces was examined using antibodies against HLA-ABC and HLA-DR antibodies.
Antibodies used for immunophenotypic characterization of hGMSCs.
Differentiation of the hGMSCs into osteogenic, chondrogenic, and adipogenic cells
In order to confirm the stem cell properties of hGMSCs, their multilineage differentiation capacity was examined by inducing osteogenic, chondrogenic, and adipogenic differentiation in specific induction media. Differentiation was assessed using histochemical staining methods, including Alizarin Red and von Kossa staining for osteogenic differentiation, Oil Red O staining for adipogenic differentiation, and Safranin O staining for chondrogenic differentiation. These stainings allowed the visualization of lineage specific features of calcium deposition, lipid droplet formation, and glycosaminoglycan production, respectively.
For osteogenic differentiation, cells (3 × 104 cells/mL) were cultured in osteogenic induction medium, DMEM Low Glucose medium supplemented with FBS (1%, v/v), penicillin/streptomycin (1%, v/v), dexamethasone (100 nM), β-glycerophosphate (10 mm), and ascorbic acid (50 μg/mL) for 28 days. Osteogenic differentiation of the cells were determined by staining with using Alizarin Red and von Kossa staining to show the calcified deposits upon differentiation.
For adipogenic differentiation, cells (3 × 104 cells/mL) were cultured in adipogenic induction medium, α-MEM medium supplemented with FBS (10%, v/v), for 3 days to reach confluency. Medium was changed with adipogenic induction medium, DMEM Low Glucose medium supplemented with FBS (1%, v/v), penicillin/streptomycin (1%, v/v), dexamethasone (1 µM), insulin (10 µg/mL), 3-isobutyl-1-methylxanthine (100 µg/mL), and indomethacin (100 μM). Adipogenic differentiation of the cells were performed by using Oil Red O staining to observe oil droplets.
For chondrogenic differentiation, cells (3 × 104 cells/mL) were cultured in a chondrogenic induction medium consisting of α-MEM medium supplemented with FBS (10%, v/v) for 3 days to reach confluency. Then, the medium was replaced with chondrogenic induction medium consisting of DMEM Low Glucose medium supplemented with FBS (1%, v/v), penicillin/streptomycin (1%, v/v), dexamethasone (100 nM), TGF-β (10 ng/mL), ascorbic acid (50 μg/mL), insulin (10 μg/mL), BMP-6 (0.025 μg/mL), and insulin-transferrin-selenium (1%, v/v). Chondrogenic differentiation of the cells were examined using Safraning O staining to observe the presence of glycosaminoglycans (GAG). 26
Culture and differentiation of the hGMSC on the PCL scaffolds
Cylindrical, 3D printed PCL scaffolds were sterilized with 70% EtOH for 30 min, treated with oxygen plasma (10 s, 50 W) in a oxygen plasma chamber and, then immersed in BMP-2 (5 ng/mL in PBS) for 10 min. The samples were dried overnight and hGMSCs were seeded dropwise onto scaffolds at a density of 2 × 104 cells/scaffold and incubated for 2 h to ensure cell attachment, and cultured with osteogenic differentiation medium (DMEM Low Glucose medium containing 10% FBS, 1% penicillin/streptomycin supplemented with 100 nM dexamethasone, 10 mM β-glycerophosphate, and 50 μg/mL ascorbic acid) in a CO2 incubator at 37°C. Osteogenic differentiation of hGMSCs on the 3D printed PCL scaffolds were determined on days 14 and 21 by determining the alkaline phosphatase (ALP) enzyme activity and Alizarin Red staining of the deposited calcium phosphate.
Morphology of hGMSCs seeded onto the BMP-2 bound PCL scaffolds were examined after staining the cytoskeleton and nucleus with Phalloidin and DAPI, respectively, on days 14 and 21 of osteogenic differentiation, with a fluorescence microscope (Zeiss, Axio Imager M2, Germany). 27 Calcium phosphate deposition on the scaffolds as an indicator of osteogenic differentiation was examined with stereomicroscope following Alizarin Red staining. ALP enzyme activity was determined using the Randox ALP assay kit (Randox, AP542) according to the manufacturer’s instruction. 28 The assay is based on the enzymatic conversion of p-nitrophenyl phosphate (pNPP) to p-nitrophenol (pNP), a yellow colored product. Firstly, scaffolds were washed three times with PBS and transferred into Falcon tubes. Cells were lysed using 0.1 M Tris buffer (pH 8.8) containing 0.1% Triton X-100. The samples were subjected to three freeze-thaw cycles (−20°C to 37°C) to ensure complete cell lysis, followed by sonication on ice at 95% amplitude for 10 min (30 s on/30 s off cycles). The lysates were then centrifuged at 2000 rpm for 10 min, and the supernatants were collected for analysis. For the ALP assay, pNPP substrate solution was prepared by mixing substrate reagent with buffer solution. A total of 240 µL of substrate solution was added to each well of a 96 well plate, followed by the addition of 10 µL of sample supernatant. The enzymatic reaction was monitored by measuring absorbance at 405 nm at 2 min intervals for 16 min using a microplate reader. The increase in absorbance was monitored, and the slope of the absorbance vs time curve was calculated. A calibration curve was generated using p-nitrophenol standards, and ALP activity was calculated accordingly (µmol/min). Measurements were performed in three replicates (n = 3) at days 14 and 21 of osteogenic differentiation. Statistical analysis was performed using two-way ANOVA followed by Bonferroni’s comparisons test. Data are presented as mean±standard deviation (SD), and p < 0.05 was considered statistically significant.
Results
Characterization of the 3D printed PCL scaffolds
Microscopic examination of PCL scaffolds
The 3DP constructs were examined using a stereomicroscope and a SEM (Figure 2). The pore size of the scaffolds was determined to be around 400 µm in both Model 1 and 2 using the SEM images.
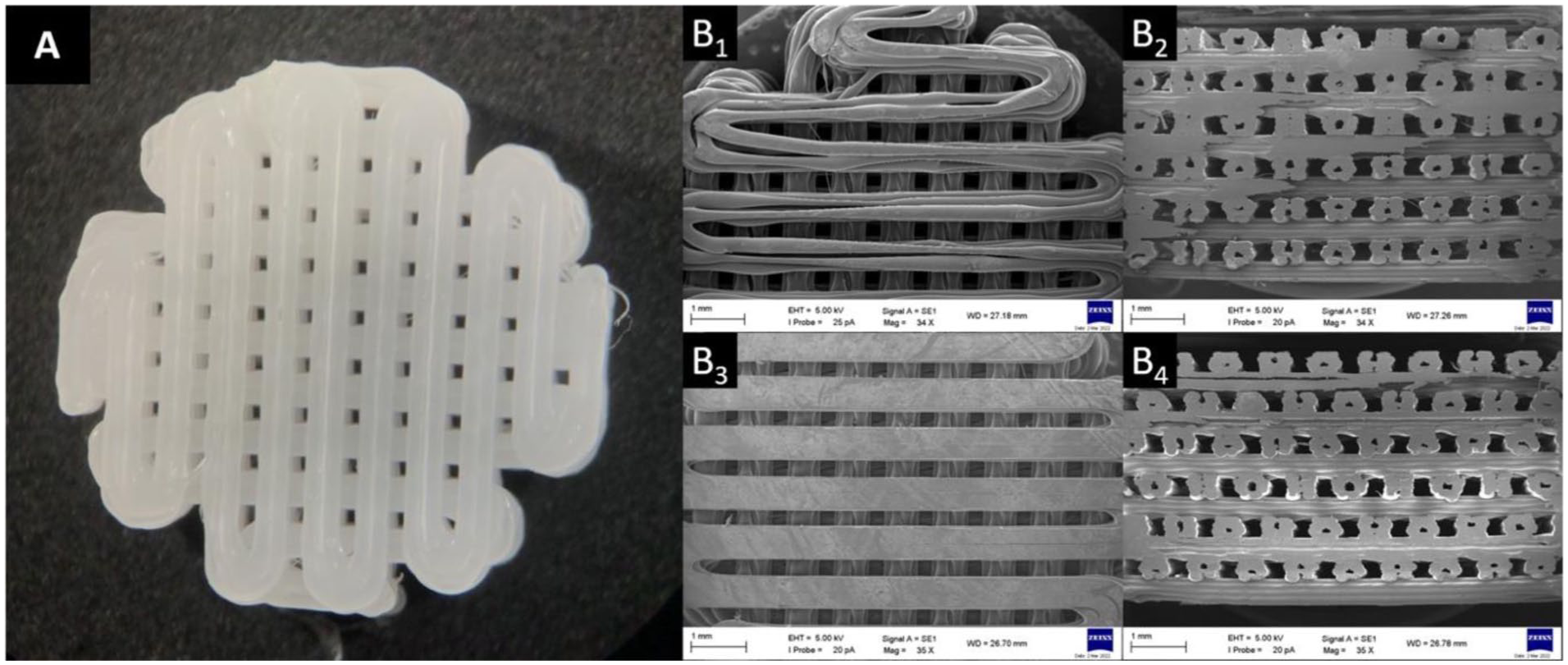
Microscopic images of the 3D printed samples: (a) stereomicroscopy image of Model 1 and (b) SEM images. Model 1: (B1) top view and (B2) side view. Model 2: (B3) top view and (B4) side view. Scale bar: 1 mm.
Mechanical properties of the 3D printed PCL implant
The compressive modulus of the scaffolds were calculated from the slopes of the initial linear region of the stress-strain plots (Figure 3) and were calculated as 58 ± 8 and 73 ± 2 MPa for Model 1 and Model 2, respectively. The compression modulus of Model 2 was closer to that of the human alveolar bone (96 ± 4 MPa).
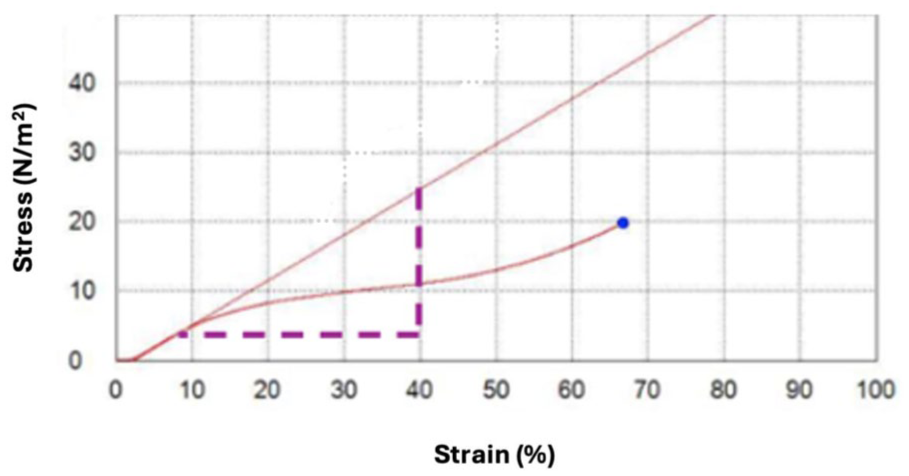
Compressive mechanical test (stress-strain) of the Model 2 implant.
Surface contact angle measurement
In the study, the modification of scaffold surface with O2 plasma treatment (50 W, 12 s) and contact angles of the treated and untreated PCL films were determined with a goniometer and were measured as 59.1° and 110.1°, respectively (Figure 4).
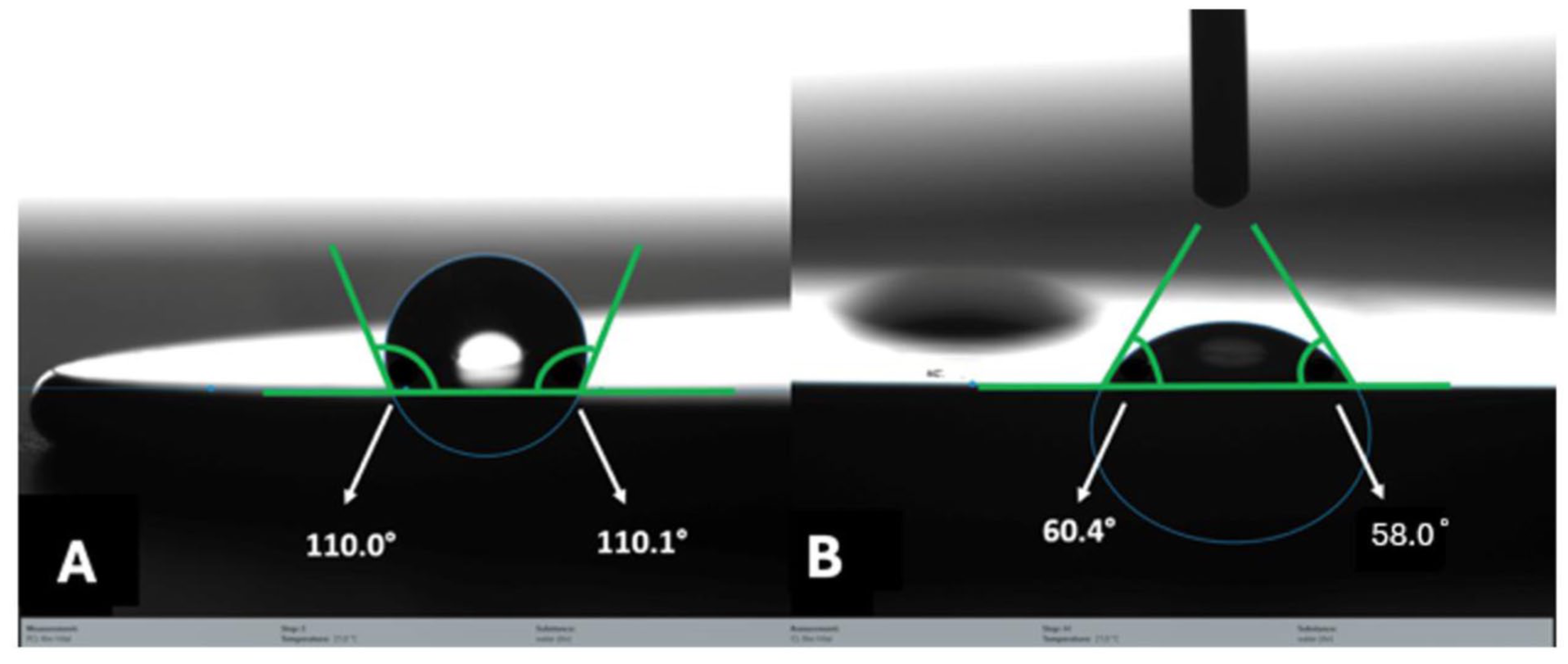
Water contact angles of PCL films: (a) untreated PCL and (b) O2 plasma treated PCL.
Attachment of BMP-2 onto the PCL scaffolds
For attachment of BMP-2 on the scaffolds, 5 ng of BMP-2 was dissolved in PBS (1 mL) and the scaffolds were introduced into this medium for 10 min. ELISA analysis performed showed that 59.37 and 62.03 pg of unbound BMP-2 were detected for Model 1 and Model 2 scaffolds on day 0, respectively. This indicated that almost all (98.8% and 98.7%, respectively the BMP-2 was bound on both types of the implant.
The BMP-2 release behavior from these scaffolds was determined for 28 days again with ELISA test. The ELISA results revealed that only around 2% of the attached BMP-2 was released over 28 days, indicating that 98% remained on the PCL scaffolds (Figure 5).
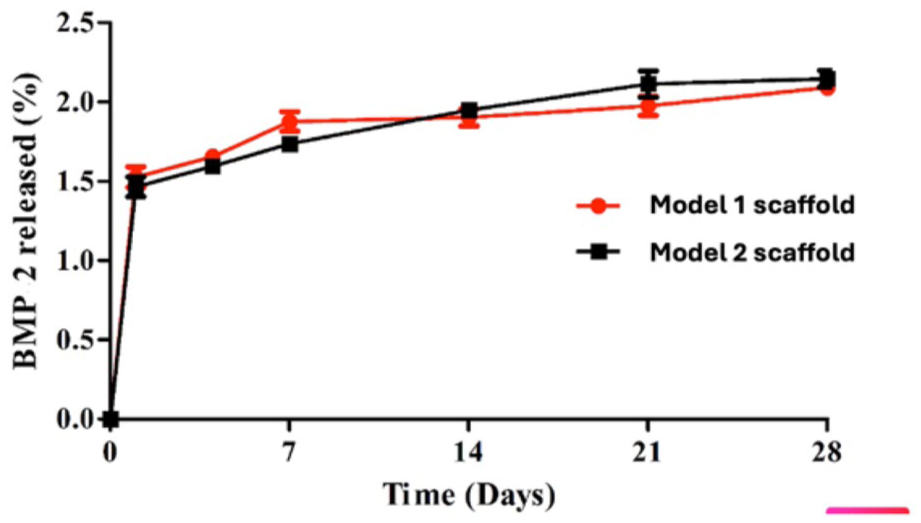
Release of BMP-2 from the PCL scaffolds.
In vitro studies
Determination of the stemness of the cells and immunogenicity of the scaffolds
Cells isolated from palatal subepithelial connective tissue were cultured in α-MEM medium supplemented with 10% FBS and 1% penicillin/streptomycin. These cells displayed a fibroblast-like morphology when expanded in vitro (Figure 6). Flow cytometry was employed for the immunophenotypic characterization using antibodies against CD34, CD44, CD45, CD73, CD90, CD105, HLA-ABC, and HLA-DR (Figure 7). Results revealed that undifferentiated cells expressed MSC markers CD44 (100%), CD73 (100%), CD90 (100%), CD105 (9%), but not the hematopoietic lineage markers CD34 and CD45. The immunophenotypic characterization in this study is consistent with the minimal criteria for mesenchymal stem cell identification as defined by the International Society for Cellular Therapy (ISCT). 29 The cells were found to be positive for CD44, CD73, CD90, and CD105, and negative for CD31 and CD45, supporting their mesenchymal phenotype.
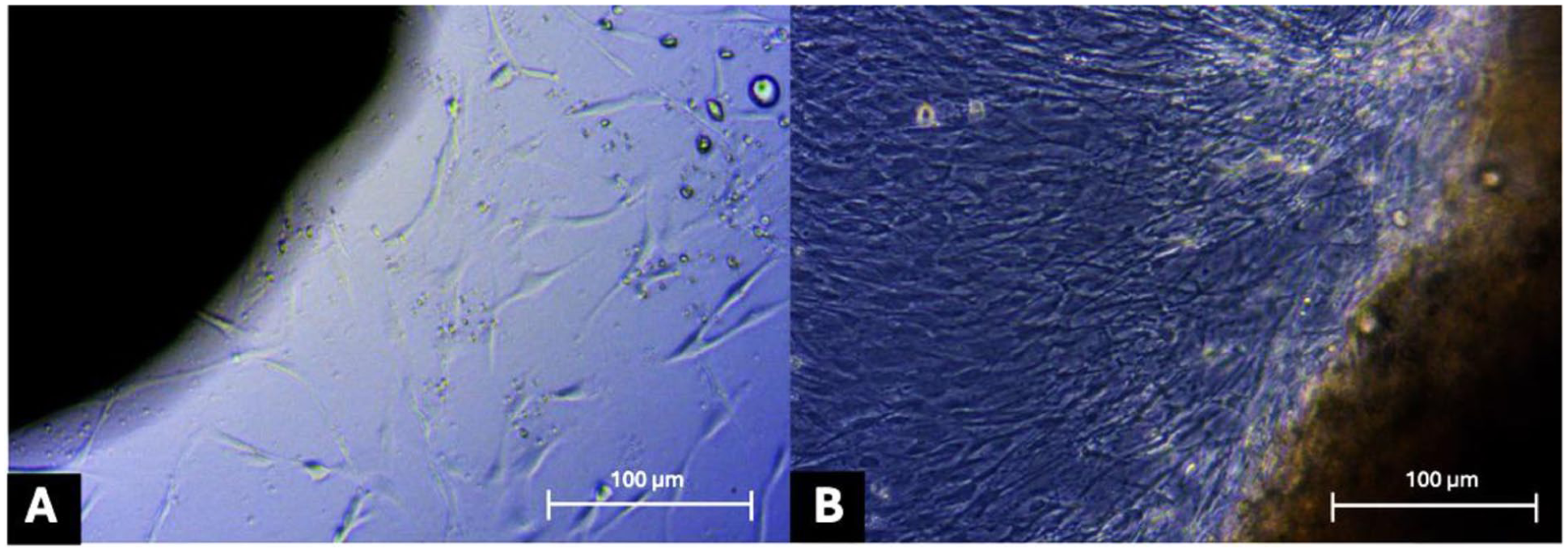
Light microscopy of cells migrating away from the palatal connective tissue and their proliferation. Culture duration (days): (a) 9 and (b) 20. Scale bar: 100 µm.
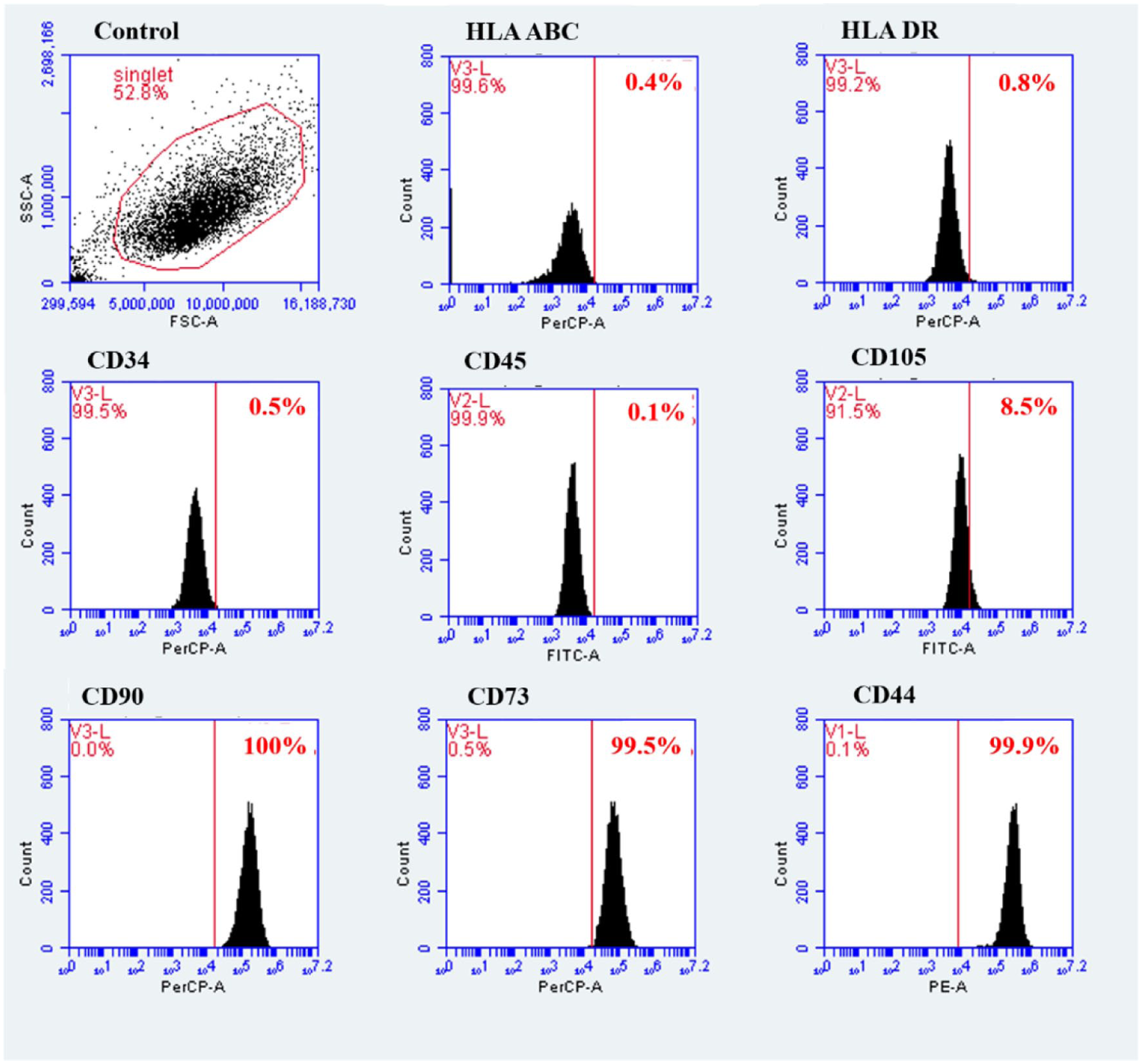
Expression of cell surface markers by hGMSCs as determined by flow cytometry. hGMSCs expressed MSC markers, positive for CD44, CD73, CD90, CD105, negative for hematopoietic lineage markers, CD34 and CD45.
In order to assess the stemness and differentiation potential, hGMSCs were induced to differentiate into osteoblasts, adipocytes, and chondrocytes by culturing them in the specific induction media.
For detection of osteogenic differentiation, calcium deposition was studied on day 28 of induction and the crystals were observed to be stained with Alizarin red (Figure 8(e)) and von Kossa (Figure 8(f)) while the undifferentiated cells were not stained with either of them (Figure 8(a) and (b)).
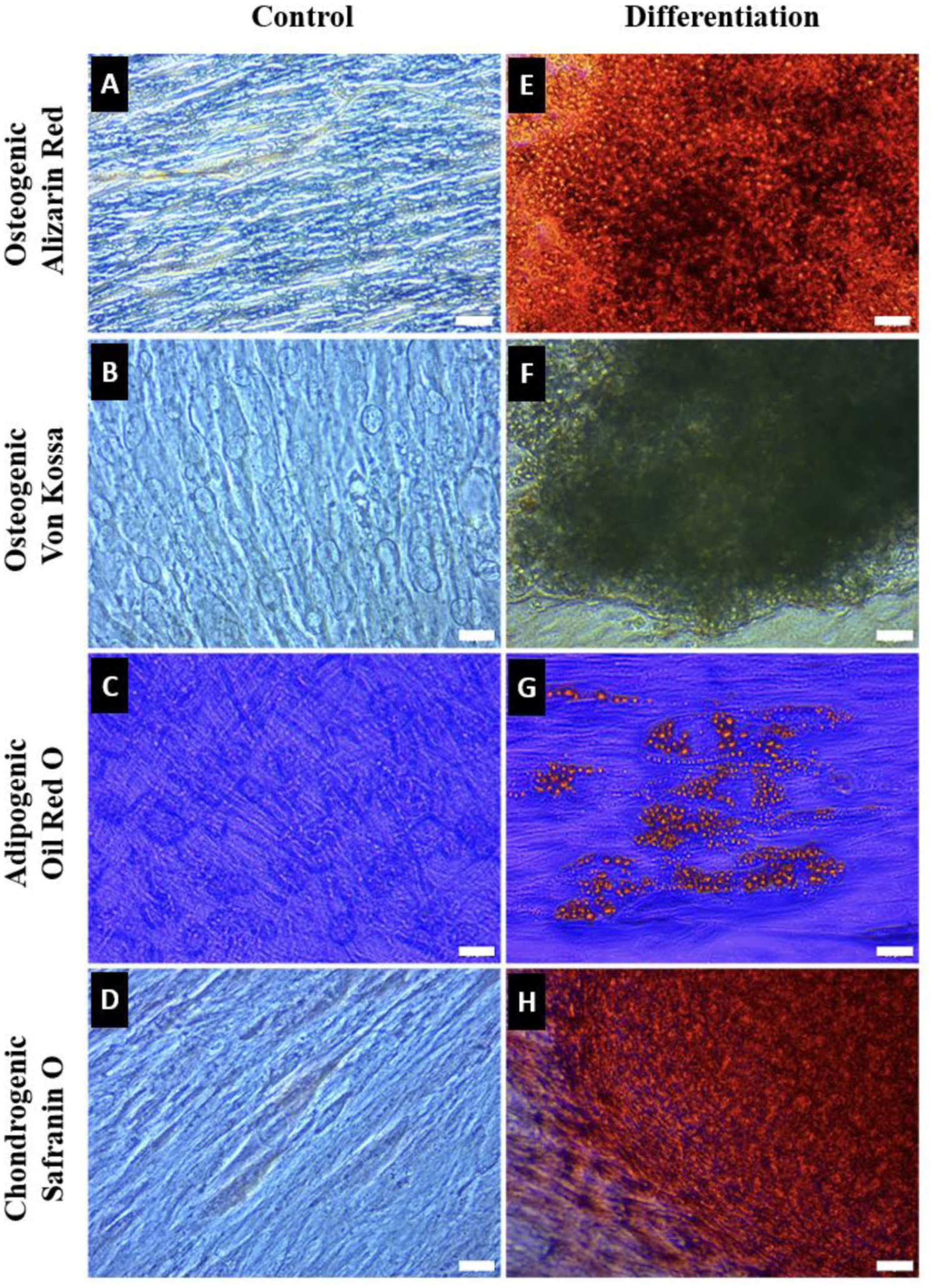
Multilineage differentiation of hGMSCs. Osteogenic differentiation: (a and e): Alizarin red staining showed no calcium deposits in the undifferentiated (control) cell group, whereas calcium deposits (red) were observed in the differentiated group; (b and f) similarly von Kossa staining showed no black calcium deposits in the control group while calcium deposits were observed in the differentiated samples. Adipogenic differentiation: (c and g): Oil Red O staining did not show any lipid droplets (red) in undifferentiated cell group while oil droplets were observed in the differentiated samples. Chondrogenic differentiation: Similar to the other groups (d and h) Safranin O staining showed no glycosaminoglycans (red) in the undifferentiated control cells while distinct GAG staining was observed in the differentiated samples. Scale bar: 20 µm.
On day 14 of adipogenic induction, hGMSCs displayed numerous lipid droplets in their cytoplasm which stained positive for Oil Red O (Figure 8(g)) while undifferentiated cells showed no lipid droplets and were not stained with Oil Red O (Figure 8(c)).
On day 14 of chondrogenic induction, glycosaminoglycans produced were stained intense red with safranin O (Figure 8(h)) while undifferentiated cells were not stained (Figure 8(d)).
These findings confirmed that the cells are stem cells that possess the ability to differentiate into osteoblasts, adipocytes, and chondrocytes proving that they can be used with the scaffolds for the regeneration damaged tissue.
Cell attachment and distribution on the PCL scaffolds
In this study, hGMSCs were cultured on PCL scaffolds with and without attached BMP-2. Morphology and distribution of cells on the scaffolds were assessed on days 14 and 21. Cytoskeleton (Phalloidin, green) and nuclei (DAPI, blue) stainings showed that hGMSCs attached to the struts of both the BMP-2 free and BMP-2 carrying PCL scaffolds (Figure 9). Cells exhibited elongated morphology oriented parallel to the struts of scaffolds on both days 14 and 21. Cell densities were notably higher on BMP-2 carrying scaffolds than the BMP-2 free scaffolds, showing that the presence of BMP-2 increased hGMSC proliferation on the implant. Furthermore, on day 21, the hGMSCs were spread and connected with each other across the struts, particularly on PCL scaffolds with BMP-2, indicating the initiation of cellular network formation (Figure 9(d)).
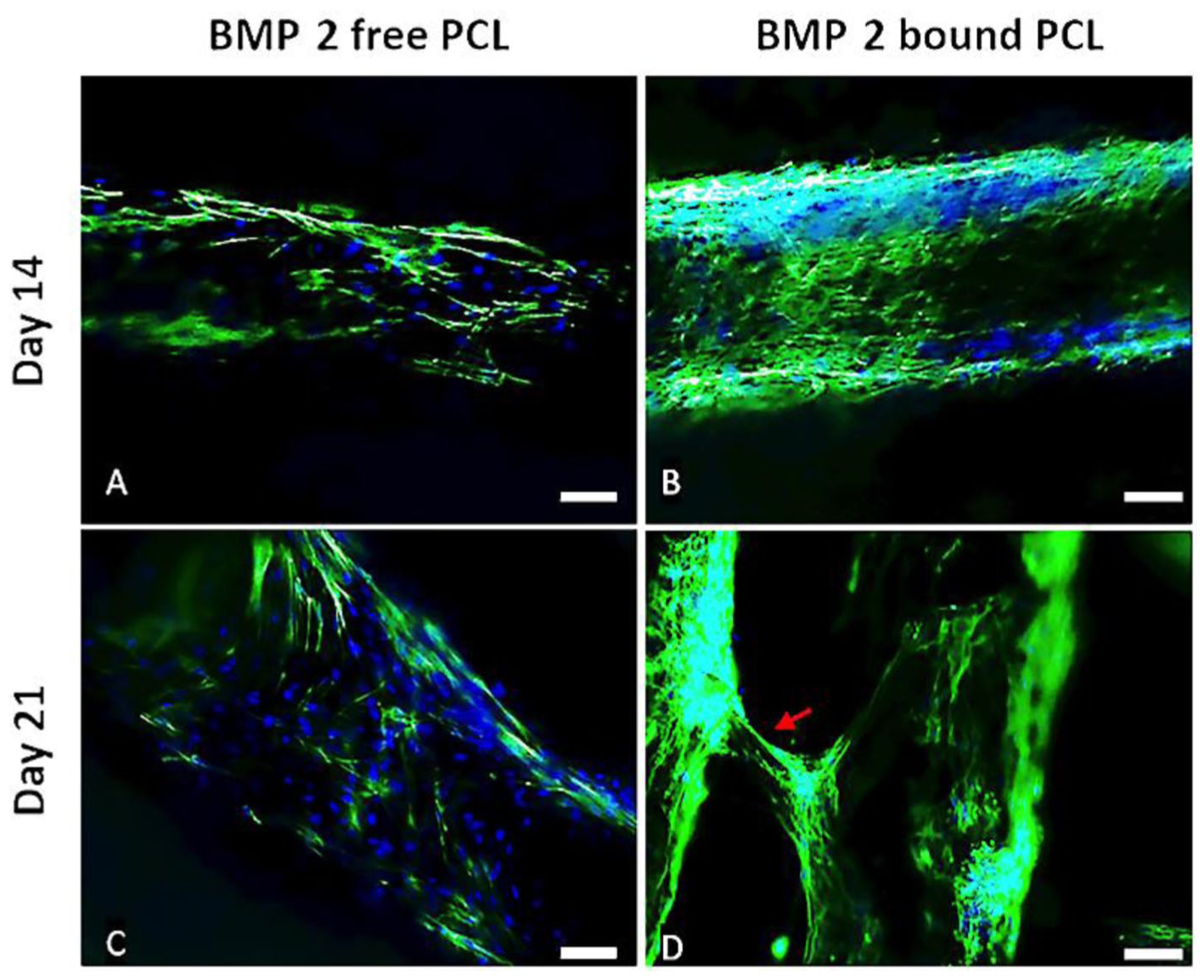
Fluorescence micrographs of the hGMSC cells on the PCL scaffolds. Cells were stained with DAPI (blue) for nuclei and FITC-Phalloidin (green) for cytoskeleton (A,C) BMP-2 bound and (B,D) BMP-2 free scaffold. Scale bars: 100 µm. Red arrow shows the extension of the cytoskeleton between the two struts of the implant.
Influence of BMP-2 on the osteogenic differentiation of hGMSCs
The impact of BMP-2 bound to the scaffold struts on osteogenic differentiation was studied. Results showed that hGMSCs cultured on BMP-2 bound PCL scaffolds exhibited significantly higher (3.5-fold) ALP activity (Figure 10), indicating that BMP-2 bound on the struts stimulated early osteoblastic differentiation. This observation was supported by Alizarin Red staining, which confirmed calcium deposition (Figure 11). The ALP activity and Alizarin Red staining results indicate that osteogenic differentiation of hGMSCs was effectively promoted by BMP-2 attached onto the struts of the scaffolds, leading to mineralization of the bone matrix (Figure 10).
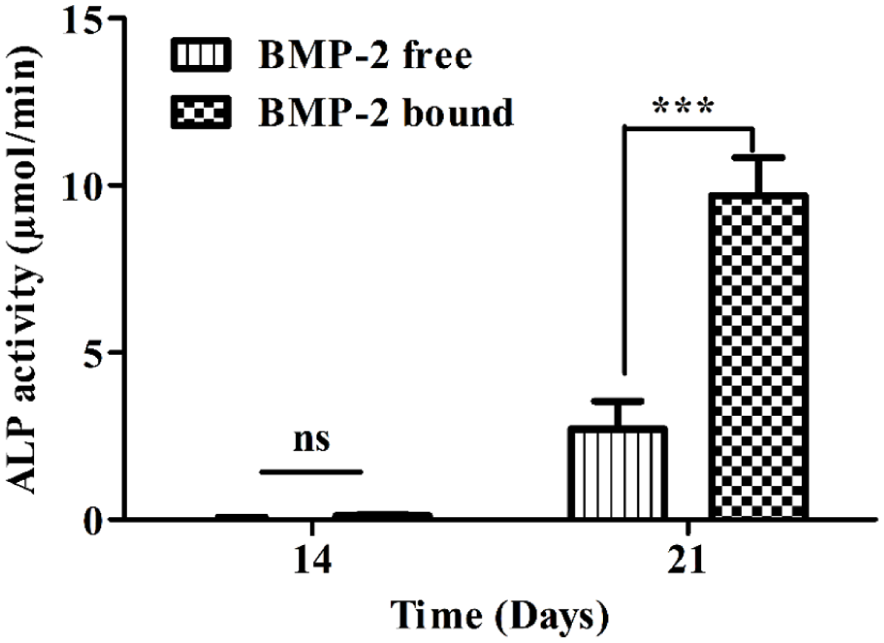
Influence of BMP-2 on alkaline phosphatase (ALP) activity of hGMSCs seeded on PCL scaffolds. Days 14 and 21. Data represent mean ± SD. ns: p > 0.05, ***p < 0.001.
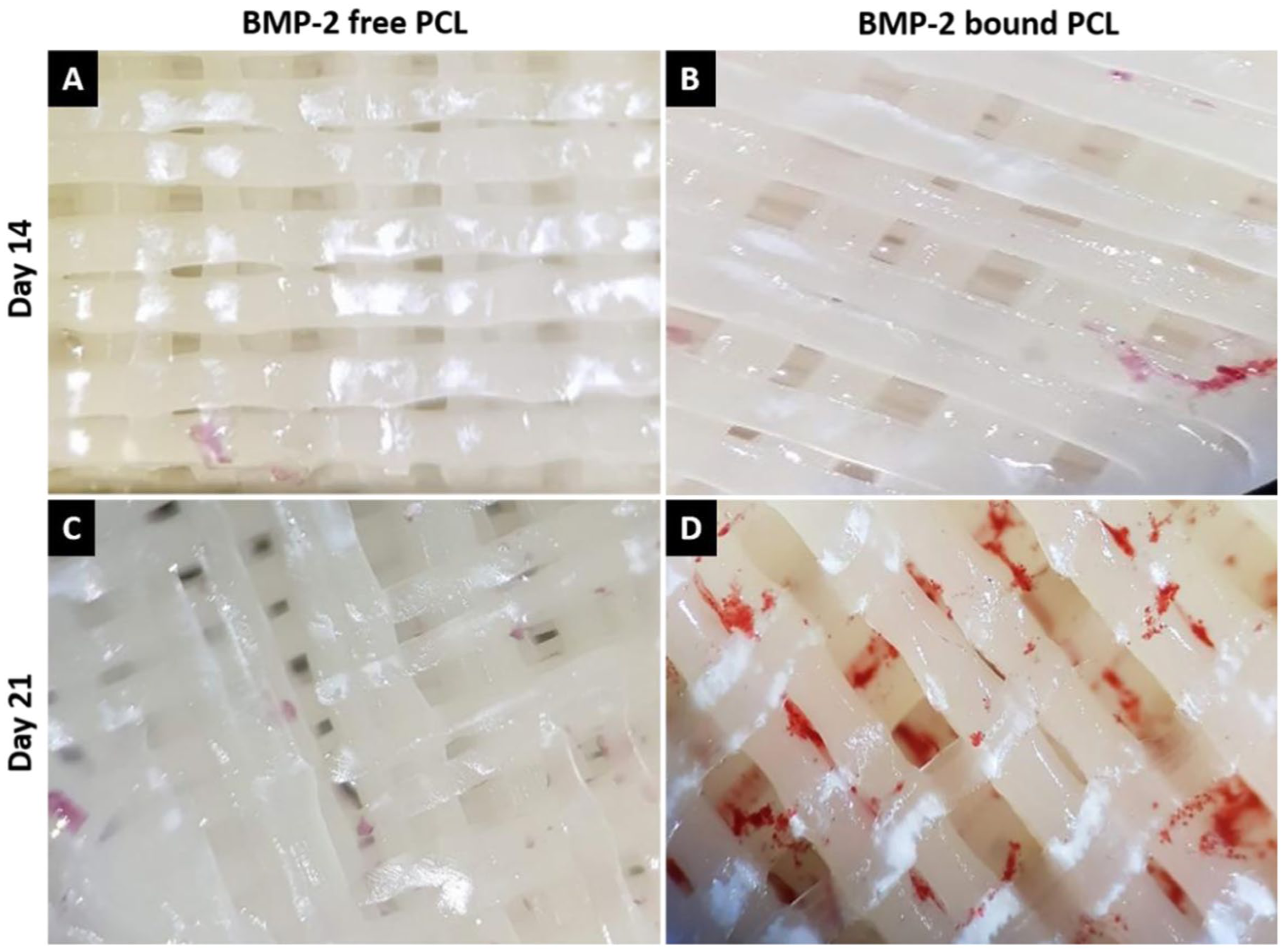
Stereomicrographs of PCL scaffolds stained with Alizarin Red stains for calcium mineral deposits (red) on days 14 and 21 of the cell culture. (a and c) BMP-2 free; (b and d) BMP-2 attached. Magnification: 4×.
Discussion
PCL dental scaffolds were produced with 3D printing using the fused deposition modeling (FDM) in order to achieve augmentation of alveolar bone applications of patients with insufficient bone volume through tissue engineering. Two different designs were printed to be chosen based on mechanical properties, cell and BMP-2 adhesion. Both designs had layers oriented 90° to each other, with subsequent layers overlapping in Model 1 (Figure 1(a)), while shifting laterally in Model 2 (Figure 1(b)). All other printing parameters were kept identical for both models, including printing temperature (100°C), print pressure (100 psi), nozzle size (Gage 25, 0.455 mm), pore size (400 µm), number of layers (12), and scaffold dimensions (diameter 10 mm, height ca. 4.8 mm). The only intentional difference between the two models was therefore the interlayer structure offset, which resulted in Model 1 with continuous linear channels extending from top to bottom, whereas Model 2 possessed zig-zag channels with no continuous vertical path. It is known that properties such as porosity of the scaffolds are important for the penetration and distribution of the cells within structure. 30 In the current design the pore size (400 µm) is critical for the mechanical strength of the scaffold and also for the rate of tissue ingrowth. However, the pore distribution in 3D is different in the two models. As intended, the implants produced were suitable for cell survival, expansion and tissue regeneration.31,32 Because the main difference between the two models was that Model 1 with a continuous channel extending from top to bottom which might lead to seeded cells to be washed through the channel formed. With Model 2, no continuous, linear channels exist, they are in the form of zig-zag channels and this might help retain more cells. Compared to conventionally fabricated bone grafts and sintered ceramic scaffolds, the 3Dprinted PCL scaffold in this study offers precise control over internal architecture, pore size, and strut configuration. This architectural advantage is in line with findings by Bartnikowski et al., 11 who reported that 3Dprinted resorbable PCL scaffolds with non-linear internal channel geometries significantly improved cell retention and uniform distribution throughout the construct in alveolar defect models. Similarly, Yeo et al. 31 demonstrated that offset layer configurations in 3Dprinted PCL/β-TCP scaffolds directly enhanced cell infiltration and osteogenic activity compared to non-offset designs, confirming that internal architecture is a decisive parameter in scaffold performance beyond pore size alone. Unlike many reported scaffolds that rely solely on pore size optimization, the present study demonstrates that interlayer offset—an architectural parameter often overlooked—plays a decisive role in both mechanical performance and cellular behavior. The compressive mechanical properties of the scaffolds were distinctly different than each other (Model 1: 58 ± 8 MPa and Model 2: 73 ± 2 MPa) with the shifted version (Model 2) being much closer to that of the human alveolar bone (96 ± 4 MPa). This difference in mechanical performance is a result of the offset subsequent layers in Model 2 unlike the directly overlapping struts of Model 1, representing a key biomechanical advantage. This observation indicates that Model 2 may contribute to improved load distribution and structural support during the early stages of bone regeneration. However, this comparison is presented as a descriptive reference rather than a direct statistical evaluation, and further in vivo and longterm studies are required to fully establish the clinical relevance of these findings. 33
Notably, while composite PCL scaffolds incorporating hydroxyapatite or β-TCP have been widely reported to achieve mechanical reinforcement,7,31 they require more complex fabrication processes and additional regulatory considerations. The present study demonstrates that a singlematerial PCL scaffold with a layered architecture can achieve mechanically comparable results, simplifying manufacturing while maintaining biomechanical suitability. Vaquette et al. 8 similarly showed that additively manufactured resorbable PCL scaffolds with appropriate mechanical design maintained structural integrity and dimensional stability during extraskeletal bone regeneration, further supporting the importance of mechanical optimization in scaffold design for clinical translation.
Since BMP-2 is allowed (Food and Drug Administration, USA) for clinical use and PCL is commercially available in medical grade quality, BMP-2 bound, 3D printed Model 2 PCL scaffolds appeared to be suitable dental tissue engineering in clinical studies.
Material surfaces with a water contact angle of less than 90° are classified as hydrophilic and when the angle is in the 40°–70° range they are more suitable for cell adhesion.34,35 Thus plasma treatment had positive effects on the scaffold material. Water contact angle measurements indicated that treatment with O2 plasma converted the hydrophobic polymer surface into a hydrophilic one, a property which improves cell adhesion. The surfaces of the scaffolds were treated with O2 plasma and then BMP-2 was attached onto the scaffolds with dip coating in order to enhance osteogenic differentiation through the use of the growth factor. This was done in order to prevent the loss of BMP-2 during each medium change. This approach eliminated the need for high initial doses typically required to compensate for BMP-2 loss in conventional drug release systems. This also mitigated the potential side effects associated with high doses of the growth factor reported in the recent years.36,37
One of the most significant advantages of the scaffold presented in this study is the nearcomplete surface retention of BMP-2, with 98.8% and 98.7% of the attached BMP-2 maintained on Model 1 and Model 2, respectively, over 28 days. This level of retention represents a significant advantage over conventional BMP-2 delivery systems, particularly collagen spongebased carriersthe current clinical standardwhich are characterized by burst release that necessitates supraphysiological doses associated with ectopic bone formation, osteoclastmediated bone resorption, and inappropriate adipogenesis. 24 The surfacebound BMP-2 strategy employed in this study eliminates the need for high initial doses while maintaining prolonged local bioavailability, directly addressing one of the most critical limitations of current clinical BMP-2 delivery approaches. Oliveira et al. 36 reviewed various growth factor delivery strategies for bone tissue engineering and highlighted that sustained, localized delivery at low concentrations is far more effective and safer than bolus administration. The nearcomplete surface retention of BMP-2 achieved in the present study directly addresses this wellrecognized clinical limitation. Furthermore, Hauff et al. 25 demonstrated that matriximmobilized BMP-2 preserves receptorbinding bioactivity more effectively than freely diffusing BMP-2, providing additional mechanistic support for the surface-bound strategy employed here. Model 2, due to its higher mechanical strength and equal BMP-2 retention, was therefore used in the rest of the study. After selecting the scaffold type the cell properties were studied. The successful isolation and characterization of hGMSCs confirmed that cells derived from palatal connective tissue exhibit typical mesenchymal stem cell properties. Immunophenotypic analysis verified the expression of MSCpositive markers and the absence of hematopoietic markers. Although CD105 expression is quite low (9%) compared to the other MSC markers, it is reported that MSCs with negative CD105 expression have higher osteogenic differentiation capacity compared to CD105 positive cells,38,39 and therefore, the low CD105 is not a disadvantage for the present application. The cells were shown to be positive for the immunogenic surface antigen HLA-ABC and negative for HLA-DR indicating low immunogenicity, a critical advantage in tissue engineering applications as it shows that the scaffold is nonimmunogenic. Furthermore, the low immunogenicity profile of the hGMSCs used in this study—confirmed by HLA-ABC positivity and HLA-DR negativity—represents an additional advantage in terms of potential allogeneic applications, reducing the risk of immune rejection in tissue engineering contexts. Furthermore, the ability of these cells to undergo osteogenic, adipogenic, and chondrogenic differentiation demonstrated their multipotency. The presence of calcium deposits stained with Alizarin Red and von Kossa confirmed osteogenic differentiation, whereas the lipid droplets stained with Oil Red O and the Safranin O staining of glycosaminoglycans evidenced adipogenic and chondrogenic differentiation, respectively. These findings are consistent with previous reports showing that gingival derived MSCs possess multilineage differentiation potential comparable to that of bone marrow-derived.40,41
The use of hGMSCs as the cellular component of the present scaffold system offers a clinically meaningful advantage over cell sources used in comparable 3D printed scaffold studies. Unlike bone marrowderived MSCs or adiposederived stem cellswhich require more invasive harvesting proceduresgingival tissue is readily accessible in the oral cavity with minimal donorsite morbidity, making it particularly suitable for dental tissue engineering applications.15,16 Tomar et al. 41 reported that gingivaderived MSCs demonstrate superior proliferative and osteogenic differentiation capacity relative to bone marrowderived MSCs, while Sun et al. 40 confirmed comparable osteogenic potential between the two sources, with gingival MSCs offering the additional benefit of easier clinical procurement. Perhaps the most distinctive advantage of the scaffold system presented in this study is the integration of multiple functional components the 3Dprinted architecture, surface hydrophilicity modification, prolonged BMP-2 retention, and a highly osteogenic accessible cell sourceinto a single coherent tissue engineering construct. While individual components such as PCL scaffolds, BMP-2 delivery, or MSC seeding have been reported separately in the literature, their combined optimization within a single scaffold system specifically designed for alveolar bone augmentation represents a meaningful advance. In the present study, hGMSCs seeded on BMP-2-functionalized PCL scaffolds exhibited a 3.5fold increase in ALP activity and enhanced calcium deposition compared to controls. This level of osteogenic induction is consistent with, and in several respects exceeds, outcomes reported in similar in vitro studies employing dental pulp stem cells or bone marrow-derived MSCs on PCLbased scaffolds,15,16,40 confirming that these components act synergistically to promote osteogenic differentiation and further underscoring the suitability of hGMSCs as an accessible and potent cell source for this application. Thus, the combination of BMP-2, mesenchymal stem cells, and 3D printed PCL scaffolds shows promising in vitro potential for dental tissue engineering applications, particularly in alveolar bone augmentation; however, these findings require validation through in vivo studies and longterm assessments before clinical translation can be considered.
Conclusion
PCL scaffolds were produced with 3D printing with FDM for use in tissue engineered alveolar bone augmentation applications in patients with insufficient bone volume. The mechanical properties of the scaffolds were close to that of the human alveolar bone making them suitable for dental applications. The surfaces of the scaffolds were treated with O2 plasma and then BMP-2 was attached onto the scaffolds to enhance osteogenic differentiation. Cells isolated from palatal subepithelial connective tissue grafts were shown to have mesenchymal stem cell characteristics by immunophenotypic characterization and their osteogenic, adipogenic, and chondrogenic differentiation. ALP and Alizarin red staining results confirmed the osteogenic differentiation of hGMSCs was activated by BMP-2 bound on the struts of the scaffolds. Although BMP-2 is approved for clinical use and PCL is available in medical-grade quality, BMP-2bound 3Dprinted Model 2 (ABCD) PCL scaffolds should be considered as a promising approach for dental tissue engineering; nevertheless, their clinical applicability must be validated through comprehensive in vivo studies and clinical trials. This method may reduce the risk of side effects caused by using high doses of BMP-2 in the medium, which is a common drawback of conventional strategies to enhance bone formation. This study has several limitations that should be considered when interpreting the results. First, the findings are based solely on in vitro experiments, and therefore, do not fully replicate the complex biological environment of in vivo conditions, including vascularization, immune response, and mechanical loading. Second, the sample size used in the experimental analyses was limited, which may affect the statistical power and generalizability of the results. Third, longterm mechanical stability and degradation behavior of the scaffolds were not evaluated, which are critical parameters for their potential application in load-bearing bone regeneration. Additionally, while the scaffold architecture and pore size were defined based on computeraided design (CAD) parameters and qualitatively confirmed by scanning electron microscopy (SEM), quantitative porosity analysis using techniques such as micro-computed tomography was not performed, which limits the comprehensive evaluation of pore interconnectivity and spatial distribution. Furthermore, although BMP-2 functionalization demonstrated promising osteogenic potential, its controlled release profile and longterm biological effects were not investigated in this study. Therefore, further in vivo studies and long-term evaluations are required to validate the safety, efficacy, and clinical applicability of the proposed scaffold system. Coupled with the advantage of the implants perfectly fitting the defect site with appropriate design for tissue ingrowth shows that this approach has a significant potential to be tested in vivo.
Footnotes
Ethical considerations
The study protocol was approved by Acibadem University and Acibadem Healthcare Institutions Medical Research Ethics Committee (ATADEK-2019/18).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Acibadem University Scientific Research Project Commission (ABAPKO 2022/04/01).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.