
Abstract
Background:
Olfaction has enabled humans to survive and reproduce throughout their evolutionary history. Certain odors have been historically associated with danger while others, pleasure. Further, olfactory impairment is one of the earliest manifestations of neurodegeneration, such as Alzheimer's disease. Therefore, olfactory tests have the potential to reveal insights into a person's brain health. The landscape of orthonasal olfactory tools is vast, and many have been adapted for populations living in low- and middle-income countries, but challenges remain in the awareness of the utility of olfactory testing, effective deployment, and scalability.
Objective:
This report explores the current landscape of olfactory tests, the potential for digital tests to provide scalable data in low-resource settings, and their potential applicability in the Alzheimer's disease and brain health space. We also describe the ScentAware digital odor identification test and present some preliminary findings from its use in Egypt, a site for the Davos Alzheimer's Collaborative's Global Cohorts Program.
Methods:
The American University in Cairo in partnership with University College London collected olfactory data using the ScentAware test from 125 participants from the North African Dementia Registry, a longitudinal study of community dwelling adults over age 55 in Egypt and the surrounding Middle East and North Africa region.
Results:
Participants’ olfactory function measured by the culturally adapted ScentAware test somewhat correlated with language and memory, as assessed by the Egyptian Harmonized Cognitive Assessment Protocol battery.
Conclusions:
Our adaptation of the ScentAware test suggests that digital olfactory assessment holds promise for cost-effective deployment at scale in a low-resource setting.
Keywords
Introduction
Olfaction plays a crucial role in survival, memory, and emotion, and is often underestimated compared to other senses. Humans detect odors orthonasally (through the nose) and retronasally (through the mouth). 1 Odorant molecules bind to olfactory sensory neurons, sending signals via the olfactory nerve to the olfactory bulb. Olfactory signals bypass the thalamus, directly influencing emotions and memory, highlighting the evolutionary significance of smell in survival and procreation. 2 Despite having fewer olfactory receptor genes than some animals, humans can detect odorants at extremely low concentrations and distinguish enantiomers. 3 This suggests that olfaction is more refined and essential than previously believed, impacting both safety and experience.
Olfactory impairment is often one of the earliest signs of Alzheimer's disease (AD) 4 and Parkinson's disease (PD) 5 and can be a valuable indicator that neurodegeneration has begun. 6 The olfactory bulb is one of the first parts of the brain to be damaged by AD. The entorhinal cortex, a region associated with olfactory memory, is one the first regions to exhibit the accumulation of neurofibrillary tangles in patients with preclinical AD.7,8 It is estimated that this initial degradation leads to compensatory activity by surrounding olfactory regions, such as the hippocampus and olfactory bulb, leading to further degradation. In this pathway, pathologic P-tau proteins tend to accumulate in the olfactory bulb and in areas like the piriform cortex, anterior olfactory nucleus, entorhinal cortex, and amygdala that are involved in olfactory processing.9,10
Individuals with poor odor identification show a higher risk of cognitive decline over 5 years.11,12 Tau accumulation in medial temporal and olfactory regions strongly correlates with longitudinal cognitive decline. 13 Odor identification impairment precedes memory loss, making it a potential early biomarker for AD. About 85–90% of early AD and 90% of PD patients experience olfactory dysfunction.9,14 Further, less than 25% of people with olfactory dysfunction are aware of it. 15 Only 6% of early AD patients report problems with olfaction when actually, over 80% of them experience serious problems with olfaction. Olfactory loss occurs to a lesser extent or is absent in other movement disorders like multiple system atrophy, corticobasal degeneration, and progressive supranuclear palsy. Hence, olfactory testing can be used as a differential diagnosis for PD.16,17
The global burden of neurodegenerative diseases is rapidly increasing in low- and middle-income countries (LMICs), where healthcare systems often lack the infrastructure for early diagnosis and intervention. 18 The p-tau217 (phosphorylated tau 217) biomarker is a promising blood-based biomarker for AD, showing strong correlations with cerebrospinal fluid (CSF) and positron emission tomography (PET) biomarkers, making it a reliable and less invasive alternative for early AD diagnosis. 19 Blood-based biomarkers are a promising solution, offering a less invasive and more scalable alternative to CSF tests and PET imaging, but real-world implementation challenges remain, especially in underserved regions. The World Health Organization emphasizes the need for accessible and cost-effective diagnostics, especially in LMICs where dementia cases are rising. Blood-based biomarker testing for AD in LMICs faces challenges such as limited healthcare infrastructure, high costs, and the need for stable sample storage and transport. 20
Digital tools, including mobile apps, artificial intelligence (AI)-powered diagnostics, and wearable sensors, enable early detection of neurodegenerative diseases by tracking cognitive, behavioral, and motor changes remotely. AI-driven data integration from speech, handwriting, and movement patterns enhances predictive accuracy, improving early diagnosis and intervention. By enabling early detection, affordable screening, and remote monitoring, digital tools can bridge diagnostic gaps in LMICs, supporting timely interventions and better patient outcomes despite healthcare limitations. 21
Traditional diagnostic tools such as neuroimaging and CSF analysis are prohibitively expensive and inaccessible in a plurality of LMIC settings. Olfactory testing, by contrast, offers a low-cost and scalable approach to early disease detection. While current olfactory assessments, such as the University of Pennsylvania Smell Identification Test (UPSIT) and Sniffin’ Sticks test, are effective clinical tools, they were primarily developed for high-income countries and rely on odorants that might not be culturally familiar or relevant to LMIC populations. 22 Moreover, their cost, cultural limitations, and requirement of trained administrators make them less viable for scalable, low-cost deployment in resource-limited settings. Digital and locally adapted solutions may provide more sustainable alternatives.
In this report, we review various olfactory test methods and introduce a digital olfactory assessment platform ScentAware, which is currently being piloted in three studies funded through the Davos Alzheimer's Collaborative (DAC). We share preliminary findings from a study being conducted by one of the DAC Global Cohorts in Egypt.
Methods
DAC Global Cohorts Program
The Davos Alzheimer's Collaborative (DAC) Global Cohorts Program is a global initiative aimed at diversifying AD research and enhancing early detection, prevention, and treatment strategies.23,24 Historically, AD research has focused on white, Western European populations, limiting insights into the disease's full diversity. 25 DAC seeks to broaden participation by supporting studies in low- and middle-income countries and underrepresented populations. The program establishes a global network of AD cohorts, collecting diverse data to refine disease modeling and biomarker discovery. It validates blood biomarkers, genetic markers, and digital cognitive tools while exploring risk reduction strategies like FINGERS. 26 DAC promotes cross-cohort collaboration and training, standardizes data collection methods, and integrates digital biomarkers (cognitive, olfactory, and speech) for scalable AD detection. By contributing anonymized data to the Alzheimer's Disease Data Initiative (ADDI) platform, DAC fosters global collaboration to accelerate discoveries and ensure more inclusive, equitable AD research and care. The ScentAware Digital Olfactory test is being piloted in three DAC global cohorts: Egypt, Kenya, and India.
DAC global cohort in Egypt
The Egypt study, led by The American University in Cairo in partnership with University College London, focuses on scalable approaches for early AD detection and risk reduction, and is part of the North African Dementia Registry (NADR). The NADR is a longitudinal study to characterize cognitive, sensory, genetic, and biomarker profiles in community dwelling older adults over age 55. The current study emphasizes diagnostic biomarker identification, genomic risk assessment, and capacity building in neurodegeneration research. It aims to advance AD detection, monitoring, prevention, and treatment in Egypt and the surrounding Middle East and North Africa region, where research participation has historically been low. The collaboration is gathering digital phenotyping data (cognitive, olfactory, and speech) and blood samples, generating local validation data for AD tests. Our preliminary findings are an analysis of 125 participants from the NADR. ScentAware test data was collected using Android mobile devices. A single ScentAware test kit was used to collect data from multiple individuals. Memory functions were assessed using the Egyptian Harmonized Cognitive Assessment Protocol (HCAP) test. 27
Participant recruitment and selection
Data was collected as field-based assessments under natural environmental conditions. Participants were consecutively recruited from outpatient clinics during their routine visits for health check-ups, chronic condition management, or cognitive evaluations. Relatives accompanying participants were invited to serve as informants to provide additional insight into the cognitive and functional status of the participants. Hospital staff were excluded to avoid potential bias. Table 1 provides the description of the portion of the study cohort analyzed in this report.
Characteristics of study participants.

ScentAware digital olfactory test
The ScentAware test was inspired by the original Sniffin’ Sticks (Burghart Instruments, Wedel, Germany) olfactory identification subtest consisting of 16 distinct odors delivered in felt-tip pens.31,32 In the ScentAware test, we used inhaler tubes as the odor delivery device. This format was chosen because it is globally familiar, commonly used for Vicks inhalers. The ScentAware test contains 15 different odors (Banana, Clove, Cinnamon, Orange, Lemon, Peppermint, Pineapple, Leather, Lavender, Rose, Smoke, Wood, Garlic, Eucalyptus, Coffee) with a second odorant for peppermint to comprise a total of 16 odorants. The two items for peppermint help determine intra-rater test-retest reliability. Odorants used are essential oils used without any dilution or diluted in mineral oil. Adsorbent wicks were soaked in the separate odorants and tubes assembled. Labels with QR codes for the 16 different odorants were applied.
Statistical analysis
Statistical analysis was performed using GraphPad Prism 5.0 (GraphPad Software, Inc., San Diego, CA).
Results
Overview of olfactory tests
Chemosensory function can be evaluated through stimulus identification (e.g., distinguishing odors or tastes), discrimination (e.g., recognizing differences between stimuli), and detection threshold (determining the lowest concentration detectable). Other measures include odor/taste memory, intensity perception, and hedonic attributes. Most clinical tests typically assess only orthonasal stimulation.33,34 This approach is largely based on findings that performance across various chemosensory measures tend to be highly correlated. 35
Odor delivery plays a crucial role, ensuring consistency in chemical identity and concentration. High-end research utilizes olfactometers, while clinical settings rely on scratch-and-sniff labels, odor-impregnated pens with adsorbent matrices. 36 Tests differ in cost, duration, and administration requirements, influencing their feasibility for clinical, public health, or research settings. The rise in chemosensory dysfunctions due to COVID-19 increased interest in chemosensory tests among researchers and funders. Table 2 below lists various odor identification tests.
Orthonasal olfactory tests.

To create this table, Google Scholar was manually searched for literature that contained the names of validated olfactory tests using keyword groupings such as “olfactory tests, low-and middle-income countries, LMICs, global health, international health, cultural adaptation” (returned 327 total results on June 9, 2025) and “orthonasal olfactory tests, cultural adaptation, countries” (returned 656 total results on June 9, 2025). This table attempts to include all orthonasal olfactory tests validated in adults and countries in which they were validated.
Traditional olfactory tests have several limitations that hinder their scalability, accessibility, and clinical integration. Manual administration and scoring make them time-intensive and require trained personnel, which limits their feasibility in resource-constrained settings and busy clinical workflows. Cost is another barrier, as some tests require disposable materials and labor-intensive administration, making them expensive and unsuitable for large-scale deployment. Furthermore, existing tests rely on binary scoring (correct/incorrect), which fails to capture partial recognition or the nuanced nature of olfactory dysfunction, such as parosmia (distorted smells) and phantosmia (odor hallucination).
Public and healthcare professional awareness of olfactory function and its clinical significance remains limited. Healthcare professionals, including general practitioners in both high income and LMICs receive minimal education on olfactory disorders, with medical, nursing, and dental curricula largely omitting chemosensory science.60–62 As a result, many providers lack the knowledge to recognize olfactory dysfunction as an early biomarker for neurodegenerative diseases, such as AD and PD, or to employ appropriate diagnostic tools.
A digital olfactory test could address these issues by automating test administration, response collection, and data analysis. Self-administered, app-based olfactory assessments could increase access to use of this valuable biomarker and integrate with electronic health records, allowing for pre-screening at home before clinical visits. Additionally, AI-driven scoring algorithms could quantify olfactory impairment more precisely, incorporating response latency, test-retest reliability, and graded accuracy.
Development of the ScentAware odor identification tests
The ScentAware test is based on the 16-item Sniffin’ Sticks test with some modifications. It is designed to be self-administered using the ScentAware test kit and a mobile device and data collected digitally. Odorants are presented in inhaler tubes labelled with unique QR codes. Participants scan the QR code, uncap the inhaler, and identify the odor from four multiple-choice options or select “no odor detected.”
The test is operated using the SensifyAware app. The app engages the camera on the mobile device. Scanning the QR code on the inhaler tube triggers the display of a forced choice question on the screen displaying the options. Participants open the cap and smell with intent, placing the inhaler tubes at least 2 cm away from the nostrils and select their response on the display. The test then moves on to the next item (Figure 1A). There is no set pattern of selection, and any tube can be picked. The order of the four responses is also randomized so that there is no learning bias if longitudinal measurements are taken. Once all 16 items have been tested, the test ends, and the test results are securely stored in a HIPAA-compliant cloud infrastructure. Researchers can use this web-based data management system to set up studies, record additional metadata, and retrieve and analyze results (Figure 1B). The flexibility of the system allows for multiple modalities of administration, including by telephone, Zoom call, or self-administration.

(A) Workflow of use of the ScentAware digital odor identification test. (B) Components involved in the digital odor identification test platform.
QR codes are a critical part of the ScentAware workflow. While QR codes are designed for flat surfaces, they can be scanned on curved surfaces, though with potential challenges in readability and scanning accuracy. On the cylindrical surface, inhaler tubes have an average diameter of 16 mm. We tested different sizes of the QR code label from 10 mm × 10 mm, 9 mm × 9 mm, and 8 mm × 8 mm. We observed poor readability for 10 cm × 10 cm and 9 cm × 9 cm QR codes using either Android or iOS mobile devices. 8 mm × 8 mm provided the best readability with 95% successful scans in 3 seconds or less, hence QR codes of 8 mm × 8 mm dimensions were used on the cylindrical surface. We also investigated applying the QR code label on the flat surface at the base of the tube. The circular flat surface has a diameter of 17.5 mm and offered a better option for readability and scanning accuracy. We created dot labels with QR codes of 9 mm × 9 mm for the bottom label. This worked with a 100% scanning accuracy in 3 seconds or less on Android (Samsung Galaxy S22) or iOS devices (iPhone 15, iPhone 15 Plus). QR code labels on both the cylindrical surface (8 mm × 8 mm) and the flat bottom surface (9 mm × 9 mm) were applied (Figure 2A).

(A) QR codes on cylindrical curved surface and flat surface used in the ScentAware digital odor identification test. (B) Screenshot of a mobile device with options being displayed. (C) Screenshot of a mobile device indicating the “please select a different tube” message if the same item is scanned more than once.
Adaptation of ScentAware to the Egyptian population
The American University in Cairo collaborated with Sensify Inc., to adapt the ScentAware olfactory test for the Egyptian population, selecting culturally familiar odorants and distractors based on initial interviews as part of DAC's cohort study in Egypt. Cultural adaptation was done by Arabic translation of the user interface. Adaptation of olfactory assessments are achieved by either changing the odors themselves or the options for the distractors. The 16 odors were deemed culturally familiar by the local research team. However, during our study, we observed that eucalyptus is not a familiar smell in Arabic cultures; there is no specific description for eucalyptus. The same set of options are used in other studies in the DAC Global Cohorts Program. The ScentAware test is programmed to run with 16-test items or 8-test items. These preliminary 16-item datasets, collected across diverse countries and cultural backgrounds, will inform future analyses to identify potential cultural biases and guide the development of an abbreviated version if warranted. We assumed older Egyptian adults may have limited familiarity with mobile technology, and due to the continuous field-based nature of the participant recruitment process, the test required support from a trained administrator. However, after completing the first test item, participants quickly grasped the workflow. Figure 2B shows an example of options displayed upon scanning an item in the test. If the same tube is scanned twice, the app displays “Please Scan a Different Tube” and the test does not proceed until a new untested item is scanned. This prevents the same item being tested more than once in a test (Figure 2C). The test kit's large cover also serves a practical function by holding already-tested items, helping to streamline the testing process. From a usability standpoint, we are confident that future implementations could be self-administered with minimal training or supported by a family member at home, thus enhancing feasibility and scalability.
Test durations were calculated based on the time elapsed between the first QR-code scan using the mobile device and the response to the 16th item in the test. The time taken for each response is also recorded as the time from one QR-code scan to the next. The average completion time for the test was 7 min, with participants spending an average of 25 seconds per item. Table 3 lists the odors and the choices used in the study. It also lists the frequency (%) of responses.
List of odors and choice response frequencies (%).

The test completion rate was high, with 85% of the participants completing the test. The test has no mandated pattern of odor selection. The positions of the four distractors are randomized in every test, but the last position is always the “No Odor Detected” option. If a particular test item is scanned the second time, the program will identify it and display a request to scan a new tube. The cover of the ScentAware test kit is big and is used to hold the already tested items. This ensures easy operation of the test. We observed participants selected the “No Odor Detected” option not only when they were unable to perceive an odor, but also when they could detect a scent but were unable to identify it or did not find a matching label among the choices. This option is scored as 0. The frequency of choosing “No Odor Detected” is shown in Figure 3A. 51.2% of the participants did not use the “No Odor Detected” option, and another 31.2% selected the option one or two times in the test. Banana and cinnamon were the most common scents identified as “No Odor Detected” (Table 3). In addition, the four distractor options are also randomized from one test session to the next. The fifth and final option position is reserved for the “No Odor Detected” option.
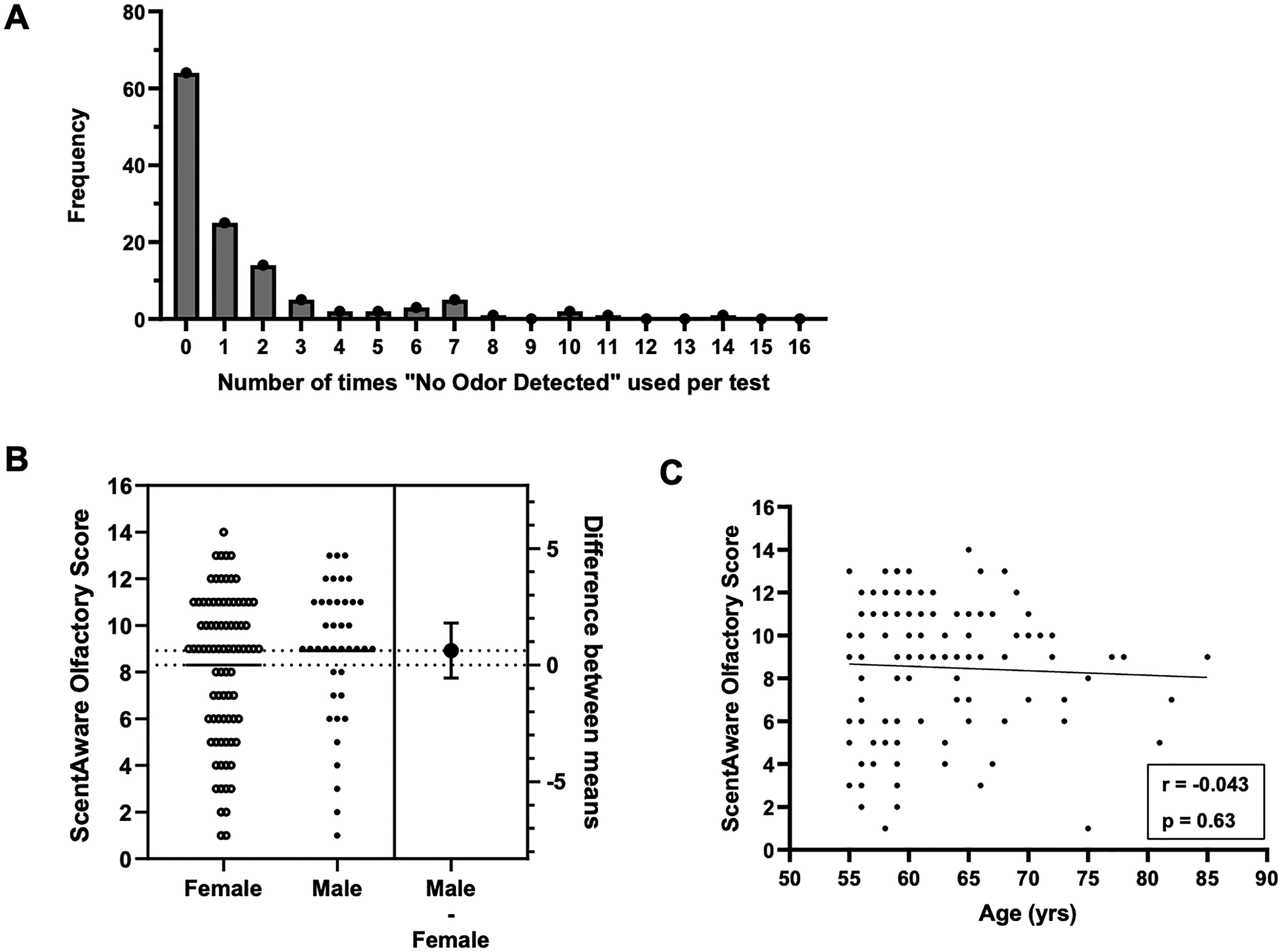
(A) Frequency of use of “No Odor Detected” option, x-axis represents the number of times the option was used, and y-axis is the number of tests. (B) No gender-based differences observed in ScentAware scores. (C) Association between age and olfaction in the participants analyzed.
Since the test consists of two items for peppermint, we used the responses to determine intra-rater consistency (or intra-rater reliability) that measures how consistently the same rater (or test-taker) provides the same ratings or responses across multiple instances of the same test or measurement. The percentage agreement was 75% (percentage agreement = (number of consistent responses/total responses) × 100). The Pearson correlation coefficient (r = 0.66, p < 0.0001) indicates moderate consistency in participants’ relative performance between test and retest, suggesting that individuals generally maintained their rank order despite the variability of field-based conditions. The intraclass correlation coefficient (ICC (1,1) = 0.45) reflects moderate agreement in absolute scores, which is reasonable given the field-based data collection approach where environmental and contextual factors may have introduced additional variability. The participants included 80 females and 45 males (Table 1). The ScentAware scores followed a normal distribution (Shapiro Wilk W = 0.939, p < 0.0001). Test scores ranged from 1–14 for females (mean = 8.925, SD = 2.96) and 1–13 for males (mean = 8.301, SD = 3.15). There was no statistically significant difference between ScentAware scores among males and females (Figure 3B). Although a negative trend was observed between olfactory scores and age, the correlation was not statistically significant (r = –0.043, p = 0.634), indicating no reliable linear association in this sample. (Figure 3C). This may be attributed to the restricted age range of the cohort, which predominantly included older adults (55–85 years).
We conducted a correlation analysis between olfactory function and the cognitive domains assessed by the Egyptian HCAP battery. The Egyptian HCAP quantifies cognition using T-scores (mean = 50, SD = 10), with scores ≤35 indicating impairment. It assesses orientation, memory, executive function, language fluency, and visuospatial skills. Informant tools (IQCODE, Blessed Scale) provide complementary insight. Validated Egyptian HCAP used the combined scores from participants and informants to yield high diagnostic accuracy against clinical AD diagnoses using the Global Deterioration Scale. 27 We found a moderate correlation between language (r = 0.43, p < 0.0001) and a weak but significant correlation between memory (r = 0.23, p = 0.01) with olfaction. Executive function, orientation, and visuospatial skills showed no correlation with olfaction (Figure 4).

Association between cognitive domains of language (A), memory (B), executive function (C), orientation (D), and visuospatial skills (E) with olfaction.
Discussion
Our adaptation of the ScentAware test confirms that digital olfactory assessment can be applied and holds promise for cost-effective deployment at scale in an LMIC setting. However, as these results are based on an initial subset of participants, they should be interpreted with caution. A full analysis of the complete cohort and among the different global cohorts will provide more definitive conclusions and contribute valuable data to the global understanding of olfactory and cognitive impairments in neurodegenerative conditions. One key limitation of using a fixed set of items in olfactory testing is the challenge of cultural adaptation. The 16-item ScentAware test overcomes that and provides a foundational framework for future development of abbreviated versions—such as an 8-item test—tailored for specific applications across the lifespan, including but not limited to neurodegenerative conditions. A proposed approach involves a two-step process: first, piloting the full 16-item test in a local cohort to identify the most effective items; second, selecting those items to construct a culturally relevant, shortened version optimized for the intended use case. As a digital platform, future versions of the test could also incorporate image-based response options, further enhancing accessibility and user experience. With further validation, standardized olfactory testing could become a routine part of healthcare, enabling early detection and monitoring of cognitive decline in aging populations. Some of the earliest variants of COVID-19 resulted in olfactory dysfunction. Our future analysis will consider the effect of Long COVID on cognitive and sensory functions in the participants based on medical reports.
Globally standardized olfactory tests are necessary to accurately capture the biological and time-based relationship between olfactory dysfunction, mild cognitive impairment, and AD in diverse populations. AD is rising in LMICs, but little data has been collected there compared to that of high-income countries like Europe, North America, and Canada. The Davos Alzheimer's Collaborative sees the use of digital biomarkers as a means for scalable deployment of screening tools. It has helped launch several cohort studies using a culturally adapted digital olfactory test with the purpose of validating their use in LMIC populations and contributing to the literature around clinically validated tests for early AD. Digital olfactory tests in combination with other accessible biomarker tests can facilitate widespread screening, particularly for early disease detection and decentralized clinical trials. Strengthening provider education and public health messaging will enhance early diagnosis, improve patient care, and establish olfactory testing as a valuable, standardized biomarker in clinical practice. Digital olfactory tests could become standard in LMICs, enhancing efficiency and reducing variability in global studies while enabling routine healthcare integration for the early detection of cognitive decline. By eliminating manual data entry, reducing costs, and improving accessibility, digital olfactory testing could revolutionize early detection of neurodegenerative diseases, making olfactory assessments a scalable, standardized, and clinically viable tool for global health applications.
Footnotes
Ethical considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Review Boards of the American University in Cairo (Case # 2023-2024-181).
Consent to participate
All study subjects and their informants provided written or oral informed consent, and the study adhered to strict ethical standards. This included data protection and subject confidentiality measures aligned with General Data Protection Regulation.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Davos Alzheimer's Collaborative for digital tools for cognitive assessment. Grant number: DAC-GC-22240710.01
Declaration of conflicting interests
SM and FW are the founders of Sensify Inc., which developed the ScentAware odor identification test. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data will be made available through the Alzheimer's Drug Discovery Initiative (ADDI) Workbench.