
Abstract
Background
There is a need for more studies to validate the role of gut microbiota in Alzheimer's disease (AD).
Objective
This study aims to explore the causal association between new gut microbiota and AD using Mendelian randomization.
Methods
Using genome-wide association study (GWAS) of 473 gut microbiota species and AD in IEU Open GWAS database, independent genetic loci related to gut microbiota were extracted as instrumental variables. The inverse variance weighting method was employed as the main indicator for evaluation. The stability and reliability of the results were further verified by heterogeneity test, outlier detection, horizontal pleiotropy test and leave-one-out analysis.
Results
Following a thorough screening process, a total of 14 intestinal microbiota were included in the final analyses. The elevated abundance of Agathobacter, Citrobacter A, Clostridium E sporosphaeroides, Eubacterium R, Megamonas funiformis, and Pseudomonas aeruginosa can reduce the risk of AD. Higher abundance of Bifidobacterium, Holdemania massiliensis, Hydrogenophaga, Intestinimonas massiliensis, Megasphaera, Paenibacillus J, Prevotella, and Raoultella could increase the risk of AD. The MR-Egger analyses at 14 “genus” levels showed no horizontal pleiotropy and the p values were all more than 0.05. The leave-one-out analysis showed that results were relatively stable.
Conclusions
This study revealed a causal relationship between 14 specific gut microbiota and the risk of AD occurrence. Some bacteria are protective, while others increase the risk of AD. These findings are of clinical significance for the treatment and prevention strategies in clinical practice, and it also provides new perspectives for related research on the “gut-brain axis”.
Keywords
Introduction
Alzheimer's disease (AD) is a progressive neurodegenerative disorder and the most prevalent form of dementia. 1 It has emerged as one of the deadliest and most burdensome diseases. 2 Research indicates that the prevalence of AD significantly increases with age, affecting approximately 5–10% of individuals over 65 years old, with a mortality rate ranking fifth among all causes of death. 3 Among those aged 85 and older, the prevalence can reach as high as 30–50%, with men exhibiting lower rates than women. 4 However, the etiology of AD remains unclear. Currently, management strategies for AD focus on alleviating symptoms or delaying disease progression.
In recent years, the “gut-brain axis” theory has gained prominence, highlighting the interaction between gut microbiota and the central nervous system as an emerging hotspot of medical research. 5 However, studies investigating the relationship between gut microbiota and AD have predominantly concentrated on correlation analyses and animal models,6–9 lacking direct causal evidence from human subjects. There is a need for more clinical studies to validate the causal role of gut microbiota in AD pathogenesis.10,11 Mendelian randomization (MR) is a method that utilizes genetic variation as an instrumental variable to evaluate the causal relationship between exposure factors and outcomes. 12 It offers a promising approach to address this gap and may guide future clinical intervention studies. 13 A study employed two-sample MR to explore potential causal relationships between 271 types of gut microbiota and AD, revealing significant associations with increased risk for developing AD from five intestinal microorganisms. 14 In 2022, Qin et al. identified 473 types of gut microbiota through metagenomic functional analysis, and it is the latest gut microbiota data that remains to be studied at present. 15 The new connections between intestinal microbiota composition and AD warrant further investigation. Due to its relative novelty within research contexts, it has become an area ripe for exploration.
This study aims to elucidate potential causal relationships between the new gut microbiota and AD through MR, providing new biomarkers for the early screening, risk assessment and personalized treatment of AD. It also could provide new perspectives for related research on the “gut-brain axis”.
Methods
Data collection
Exposure data collection
Genetic data of gut microbiota (GCST90032172 - GCST90032644) could be obtained through the IEU Open GWAS platform (https://gwas.mrcieu.ac.uk/). This data included a correlation analysis of 2801 microbiota and 7,967,866 variants in 5959 individuals and showed a total of 473 types of gut microbiota data.
Result data collection
Searching with the keyword “Alzheimer's disease”, we selected a genome-wide association study (GWAS) study (ebi-a-GCST90027158) with a relatively recent publication year, including 111,326 AD patients and 677,663 controls. The genome-wide meta-analysis involved a total of 487,511 samples and 209,21,626 single nucleotide polymorphisms (SNPs). Given that all statistical analyses rely on publicly available data, no ethical approval is required.
Selection of instrumental variables
MR analysis must satisfy three primary assumptions: 1) The selected instrumental variables were closely associated with the exposure factors; 2) The instrumental variables were independent of any confounding factors; 3) The instrumental variables affected the outcome solely through the gut microbiota exposure pathway.
This study investigated the causal relationship between gut microbiota and AD, focusing on gut microbiota at the “genus” level as an exposure factor. Analyzing data at the “genus” level allows for a more precise identification of specific microbial taxa; moreover, microbial species within the same genus often show similar metabolic and ecological functions. Therefore, making preliminary causal inferences at the genus level is biologically reasonable and can provide a clear direction for further research on functional mechanisms at the species or strain level. In this study, the TwoSampleMR package in R software (version 4.4.2) was used to extract relevant SNPs. According to p < 5.0 × 10−8. SNP sites with significant relevance to the gut microbiota were selected based on a threshold of p < 5.0 × 10−8, with parameters set at r2 < 0.001 and a window size of 10,000 kb to eliminate the interference of linkage disequilibrium.16,17 We collaboratively compiled GWAS data regarding the gut microbiota and SNPs exhibiting identical alleles in GWAS results, using effect values of exposure and outcome data for correspondence. Furthermore, the F-statistic was used to evaluate the instrumental variable effect of each SNP, in order to avoid the bias of weak instruments. F > 10 indicated no significant weak instrument bias; SNPs with F > 10 were selected for the subsequent MR analysis. 18 To ensure the independence assumption and the exclusivity assumption, the MR-Egger method was finally adopted, and the horizontal pleiveness test of the instrumental variables was conducted based on the intercept of the MR-Egger regression and its p-value. 19
Mendelian randomization analysis
This study utilized the two-sample MR approach to assess the potential causal relationship between gut microbiota and AD. The primary analytical methods included Inverse Variance Weighting (IVW), MR-Egger regression, Weighted Median Estimator (WME), Weighted Mode (WM), and Simple Mode (SM) methods. Given IVW showing superior testing efficiency compared to other methods, this study adopted IVW as the principal analytical method for estimating the causal effect between intestinal flora and AD. 20 A p-value threshold of p < 0.05 was established for statistical significance; when the 95% confidence interval (95% CI) of the Odds Ratio (OR) did not encompass 1, a significant causal effect was inferred—where OR >1 indicated an increased risk, while OR <1 suggested a protective effect.
Result quality evaluation
Heterogeneity among instrumental variables was assessed using Cochran's Q test. A result with p < 0.05 in this test indicated significant heterogeneity; conversely, if p ≥ 0.05, it suggested no substantial heterogeneity. Potential outliers were identified and addressed through MR-PRESSO global analysis; a p-value less than 0.05 in this context signified the presence of outliers within our data set. The MR-Egger intercept test was conducted to evaluate horizontal pleiotropy: if p < 0.05 for the intercept term, it denoted significant horizontal pleiotropy warranting prioritization of MR-Egger regression results; If the intercept term p ≥ 0.05, it indicated no significant pleiotropy and the IVW results were reliable. The Leave-one-out analysis assessed the impact of individual instrumental variables one by one on the estimation of the overall effect to evaluate result robustness. These methods must adhere to fundamental assumptions and employ various analytical techniques to correct potential biases and confounding factors, including eliminating polymorphic genetic variations based on biological or statistical evidence. If any instrumental variable was excluded sequentially yet remained statistically significant (p < 0.05), this further supported that our findings are robust.
All analyses were conducted using R Studio and related software packages (such as TwoSampleMR, MR-PRESSO). By constructing funnel plots and forest plots, the existence of horizontal pleomorphism in MR Analysis was visualized, and the reliability of the results was further verified.
Reverse Mendelian randomization analysis
In the final results, there were intestinal microbiota that had an impact on AD. A reverse MR analysis would be further conducted, with AD as the exposure and intestinal microbiota as the outcome. This will explore the impact of AD on the intestinal microbiota, avoiding the reverse causal relationship interfering with the results of this study. The flowchart was shown in Figure 1.

The assumptions and flowchart of MR analysis in this study.
Results
Characteristics of instrumental variables
Following a thorough screening process, a total of 766 instrumental variables associated with AD were identified, encompassing 40 types of intestinal microbiota. 19 unnamed microbiota were excluded, resulting in the retention of only those at the “genus” level. Ultimately, 14 intestinal microbiota were included in the final analyses. The F-values for all instrumental variables exceeded 10, indicating that there were no weak instrumental variables (Figure 2). Given the inclusive nature of classifications within gut microbiota, it was plausible that significant overlap existed among SNPs and their corresponding sequences across various types of gut bacteria.

Heat maps of F-values for various gut microbiota instrumental variables related to AD.
Mendelian randomization analysis results
Using the “genus” level of intestinal flora as the exposure variable and AD as the outcome variable, we found that all 14 genera exhibited a significant causal relationship with AD. The brief introductions of all 14 genera were as shown in Supplemental Table 1. Based on the IVW analysis method, Agathobacter, Citrobacter A, Clostridium E sporosphaeroides, Eubacterium R, Megamonas funiformis and Pseudomonas aeruginosa were negatively correlated with the risk of AD occurrence, while Bifidobacterium, Holdemania massiliensis, Hydrogenophaga, Intestinimonas massiliensis, Megasphaera, Paenibacillus J, Prevotella and Raoultella were positively correlated with the risk of AD occurrence (Figure 3 and Table 1). Additionally, among different species analysis methods, the beta values for most intestinal microbiota were consistent except for Megamonas funiformis (Figure 4).

The forest plots of various gut microbiota related to AD based on IVW method.

The SNP effect diagrams of each gut flora related to AD. (a) The SNP effect plot of Agathobacter, showing a negative correlation with AD; (b) The SNP effect plot of Bifidobacterium, showing a positive correlation with AD; (c) The SNP effect plot of Citrobacter A, showing a negative correlation with AD; (d) The SNP effect plot of Clostridium E sporosphaeroides, showing a negative correlation with AD; (e) The SNP effect plot of Eubacterium R, showing a negative correlation with AD; (f) The SNP effect plot of Holdemania massiliensis, showing a positive correlation with AD; (g) The SNP effect map of Hydrogenophag, showing a positive correlation with AD; (h) The SNP effect plot of Intestinimonas massiliensis, showing a positive correlation with AD; (i) The SNP effect plot of Megamonas funiformis, showing a negative correlation with AD; (j) The SNP effect plot of Megasphaera, showing a positive correlation with AD; (k) The SNP effect plot of Paenibacillus J, showing a positive correlation with AD; (l) The SNP effect plot of Prevotella, showing a positive correlation with AD; (m) The SNP effect plot of Pseudomonas aeruginosa, showing a negative correlation with AD; (n) The SNP effect plot of Raoultella, showing a positive correlation with AD.
Mr analyses for each gut microbiota related to AD.

A total of 14 genera exhibited a significant causal relationship with AD. MR: Mendelian randomization; AD: Alzheimer's disease; IVW: inverse variance weighting.
Result quality assessment
Cochrane's Q test showed that there was no heterogeneity among the 11 intestinal microbiota except for Agathobacter (p < 0.001), Clostridium E sporosphaeroides (p = 0.041), and Eubacterium R (p = 0.028). The MR-PRESSO results indicated that the p values of the included gut microbiota were all > 0.05. The MR-Egger analyses at 14 “genus” levels showed no horizontal pleiotropy, and the p values were all more than 0.05 (Table 2). The “Leave-one-out” results showed that phasing out any SNP would not affect the overall results. Therefore, this MR Analysis had good robustness (Figure 5).

The analyses chart of each gut flora related to AD by leave-one-out method.
Result quality assessment of each gut microbiota showing a causal relationship with AD.

The MR-Egger analyses at 14 “genus” levels showed no horizontal pleiotropy (p > 0.05). MR: Mendelian randomization; AD: Alzheimer's disease; IVW: inverse variance weighting.
Reverse Mendelian randomization results
Among 473 gut microbiota, 21 identified as being significantly influenced by AD were finally obtained. Five MR Methods (IVW, MR-Egger, WME, WM, and SM) were used to analyze the causal relationship between AD and the 21 gut microbiota. Comparative analysis with positive MR results revealed that out of the 14 gut microbiota exhibiting causal associations with AD, only Raoultella genus group demonstrated a reverse causal relationship with AD, while no reverse causal relationship was observed for the remaining 13 microbiota. Further sensitivity analysis was performed on the reverse MR results between the AD and Raoultella genus groups. These analyses confirmed the absence of heterogeneity or horizontal pleiotropy in the findings for Merdibacter massiliensis. Reverse MR results indicated that AD was positively correlated with Akkermansia muciniphila B, Alistipes shahii, Eisenbergiella, Faecalicatena lactaris and Merdibacter massiliensis, while negative correlations were observed with Aliivibrio, Demequina, Pandoraea, Raoultella, Terrisporobacter and Turicibacter (Table 3).
Sensitivity analysis of the reverse MR results between AD and Raoultella genus groups.
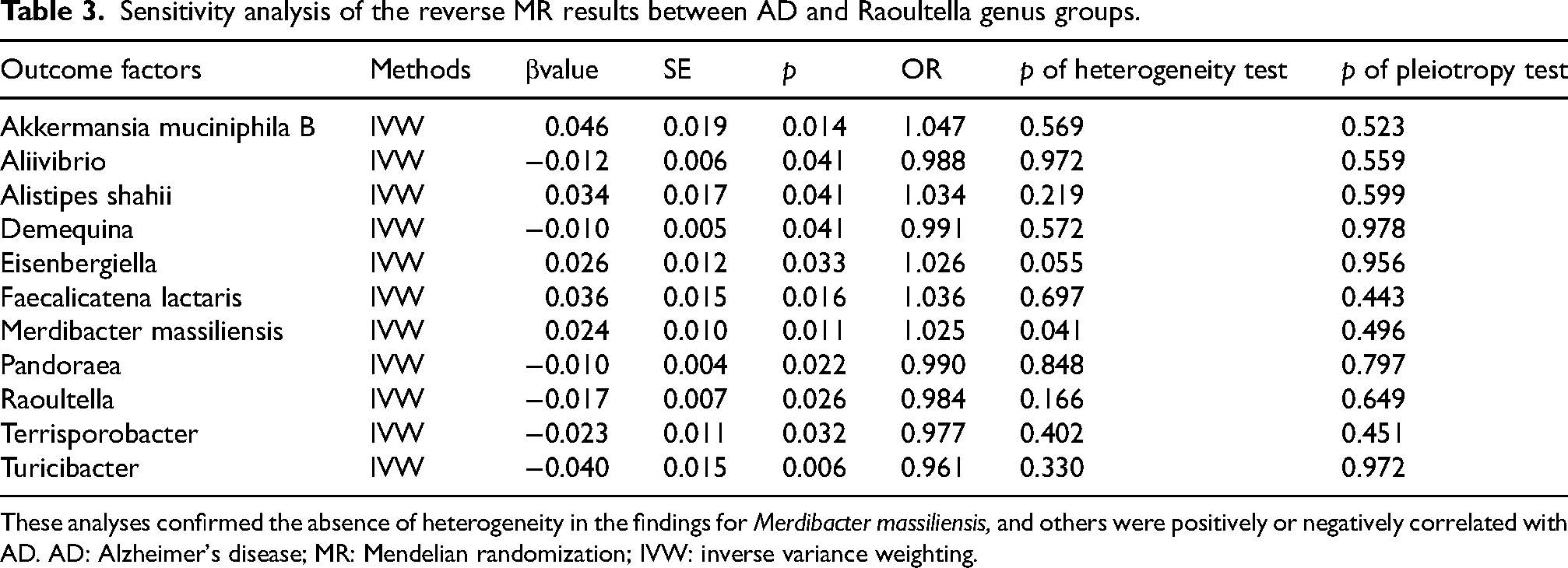
These analyses confirmed the absence of heterogeneity in the findings for Merdibacter massiliensis, and others were positively or negatively correlated with AD. AD: Alzheimer's disease; MR: Mendelian randomization; IVW: inverse variance weighting.
Discussion
As a neurodegenerative disease, AD has a complex etiology, involving multiple factors such as genetics, environment and lifestyle.21,22 Although existing therapies can alleviate clinical symptoms, they still cannot effectively delay or prevent the disease progression. 23 In recent years, multiple studies have suggested that the imbalance of gut microbiota may be involved in the pathological process of AD through the “gut-brain axis” mechanism.24,25 Qin identified 473 core gut microbiota based on metagenomic functional analysis 15 ; among them, new strains/subspecies were discovered, and there were still research gaps in the biological functions concerning the occurrence and development of AD. Through MR Research, not only can the potential role of gut microbiota in the etiology of AD be revealed, but it may also provide a theoretical basis for the development of precise intervention plans targeting the microbiota.
Our results showed significant causal relationship between 14 gut microbiota and AD. Among them, Bifidobacterium, Holdemania massiliensis, Hydrogenophaga, Intestinimonas massiliensis, Megasphaera, Paenibacillus J, Prevotella, and Raoultella exhibited positive correlations with the AD risk. At present, the abundance changes of Bifidobacterium in AD studies show differently. Based on the North American population, Vogt et al. verified that the abundance of this genus decreased in the intestines of AD patients, 26 while other study including our study observed an increase in its abundance. 7 It is worth noting that geographical regional differences may affect the colonization characteristics of Bifidobacterium through factors such as dietary structure and environmental exposure. 6 This might partially clarify the differences in results among different studies. The genus Holdemania may be related to succinic acid metabolism and activate the inflammatory phenotype of macrophages. 27 Current studies mainly focus on its association with depression, and its relationship with AD remains to be explored. 28 The main mechanism of Hydrogenophaga is hydrogen metabolism, which plays a crucial role in maintaining intestinal redox balance. Hydrogen metabolism serves as a key regulator of microbial fermentation in the anaerobic ecosystem, and it may represent a fundamental driver shaping the composition and function of gut microbiota. 29 While its metabolic network may indirectly affect AD, the precise mechanism remains to be clarified. Intestinimonas may affect intestinal barrier function by producing metabolites such as butyric acid,25,30 which can enhance the integrity of the blood-brain barrier and inhibit neuroinflammation. 31 The Megasphaera, predominantly involved in the conversion of lactate to propionate, contributes to host energy metabolism and glucolipid homeostasis regulation. 32 These two types of microbiota may be related to abnormal metabolism of short-chain fatty acids (SCFAs). 33 SCFAs, as important microbiota-derived metabolites, exhibit anti-inflammatory and neuroprotective effects.34,35 These compounds can modulate the intestinal immune response, enhance the intestinal barrier function, reduce chronic intestinal inflammation, and thereby influence the systemic immune status. 36 Paenibacillus demonstrates antimicrobial activity through bacteriocin secretion, 37 and at the same time exhibits immunomodulatory properties, thereby providing defense against viral and bacterial pathogens. 38 These characteristics suggest its potential therapeutic value for intestinal health and immune-related diseases. Consequently, the Paenibacillus microbiota that regulates immune responses may provide a novel therapeutic avenue for AD. Prevotella can produce SCFAs by fermenting dietary fiber, 39 and also modulates intestinal immunity through interactions with dendritic cells, macrophages, and T cells. 40 Notably, Prevotella may help regulate the immune system and reduce neuroinflammatory responses by promoting regulatory Treg cells, thereby influencing the occurrence and progression of AD. 41 However, these mechanisms require further experimental validation. Khedr et al. indicated that the abundance of Prevotella was more abundant in AD group than in control group, 42 with a negative correlation between Prevotella levels and cognitive performance, a finding consistent with our results. Raoultella, an opportunistic pathogen, may trigger neuroinflammatory processes by endotoxin (lipopolysaccharide) release, triggering local or systemic inflammation. These inflammatory factors can cross the blood-brain barrier, activate glial cells, and exacerbate neuronal damage, a pathological cascade central to AD progression.9,26
The results of MR analysis showed that Agathobacter, Citrobacter A, Clostridium E sporosphaeroides, Eubacterium R, Megamonas funiformis, Pseudomonas aeruginosa demonstrated negative correlations with the AD risk. Agathobacter may enhance intestinal immune tolerance through SCFAs-mediated immunoregulatory mechanisms. Lv et al. found significantly reduced Agathobacter abundance in AD patients, showing a negative correlation with cognitive impairment. 43 Animal experiments demonstrated that Agathobacter rectalis increased beneficial symbiotic bacteria, significantly improved pathological damage, and inhibited the activation of microglia. This was consistent with our results. An increase in Citrobacter microbiota can lead to impaired intestinal barriers and elevated expression of inflammatory factors in the blood and brain tissues. 44 It may affect cognitive function through pathways such as neurotransmitters and neuroimmune responses. However, the current research on its relationship with AD is still unclear. Some species of Clostridium (such as Clostridium butyricum) may be potential producers of SCFAs. Their decrease may exacerbate AD pathology by reducing neuroprotective metabolites (such as butyric acid), and the abundance change of this flora was significantly correlated with AD biomarkers. 45 Meanwhile, Clostridium is markedly diminished in AD patients’ gut microbiota, potentially contributing to AD pathogenesis through metabolic dysfunction, compromised intestinal barrier integrity, and systemic inflammation. However, the high abundance of Clostridium leptum may counteract SCFAs benefits, highlighting the need for microbiota modulation strategies that balance protective and pathogenic effects. However, Zha et al. reported that the abundance of Clostridium (such as Clostridium beijerinckii) was significantly increased in mouse models, showing positive correlation with Aβ plaques burden. 46 Clostridium contains multiple strains, and different strains may play opposite roles in AD. These divergent findings suggested strain-specific roles in AD pathogenesis that may depend on disease stage, underscoring the need for refined taxonomic classification and multi-omics approaches to elucidate these complex interactions. Eubacterium species primarily generate SCFAs through fermentation of carbohydrates and proteins. 47 Verhaar et al. pointed out that the abundance of the Eubacterium ventriosum group was significantly decreased in patients with positive amyloid protein, a pathological marker of AD (OR = 0.76, p < 0.01). 45 This finding suggested that it may exert neuroprotective effects through SCFAs. Cammann et al. highlighted that certain specific genera within this microbiota, such as Eubacterium fissicatena and Eubacterium nodatum group, may lower the risk of AD through anti-inflammatory, metabolic regulation and genetic interaction mechanisms. 48 Notably, there were distinct differences in the specific functions of these strains. The dysbiosis associated with Megamonas has been confirmed to correlate significantly with the rapid progression of mild cognitive impairment. 49 As an anaerobic bacterium, it may influence gut-brain communication by altering the REDOX state within the intestine. Additionally, abnormal abundance of Pseudomonas may be involved in AD pathology by regulating neurooleic acid metabolism. Animal experiments demonstrated that a decrease in its abundance was correlated with the improvement in cognitive function, suggesting that its underlying mechanism may involve SCFAs metabolism and regulation of neuroinflammation. 50 These findings implied that the dynamic changes in specific bacterial genera may serve as microbial markers for the early diagnosis of AD.
Compared with previous MR research, this study showed both consistency and differences. For instance, Zhuang et al. reported that the Blautia was associated with a reduced risk of AD, and emphasized the hypothesis about the core role of microbial neurotransmitters in the gut-brain axis. 51 Yu Bozhu et al. utilized two-sample MR to explore the causal relationship between 271 intestinal microbiota and AD, and found that Defluviitaleaceae increased the risk of AD, while Ruminococcus gnavus group had a protective effect, and the latter mechanism was related to the production of short-chain fatty acids. 14 Another MR study revealed that multiple bacterial genera, including Prevotella, Adlercreutzia, and Haemophilus, were associated with AD. 52 It was consistent with the conclusion of our study that Prevotella was a risk factor for AD. However, our study identified a large number of significantly associated bacterial genera that were not reported in other studies, such as Agathobacter, Citrobacter A, Holdemania massiliensis, etc. This might be due to the fact that we used updated and more comprehensive GWAS data of 473 gut microbiota, covering more microbial taxonomic units that have not been fully studied.
Recently, a large number of clinical trials have presented that supplementing probiotics can significantly improve the cognitive function and metabolic status in patients with AD, thereby further supporting the role of gut microbiota in various diseases. 53 Nevertheless, the complex relationship between the gut microbiota and AD still requires more research to clarify, especially regarding the mechanisms by which specific microbiota and their metabolites exert the effects. This understanding is essential for identifying new targets for the prevention and treatment of AD.
There are also limitations in this study. Firstly, the data mainly originated from the European population, which may introduce bias due to different lifestyles and other factors affect the changes in intestinal microbiota. Secondly, the scarcity of data sources concerning intestinal microbiota presented a challenge: the datasets used for selecting SNPs and estimating SNP effect size derive from same cohort, potentially leading to selection bias. Additionally, GWAS database compiled horizontal statistical data rather than directly obtaining original clinical data; this limitation constrained opportunities for conducting in-depth analyses for various diseases. Finally, since the pathophysiology of AD is complex, strict multiple test corrections may unintentionally overlook the gut microbiota with a causal relationship with AD.
Conclusions
In conclusion, this study revealed a causal relationship between specific gut microbiota and the risk of developing AD. Some bacteria are protective, while others increase the risk of AD, which may serve as early biomarker for the development and microbiome-targeted prevention. These findings are of clinical significance in providing new strategies for AD treatment and prevention, and it also presents new perspectives for related research on the “gut-brain axis”. Future research should combine multi-omics data and experimental verification to elucidate the precise causal mechanisms underlying these associations and further diagnostic accuracy.
Supplemental Material
sj-docx-1-alr-10.1177_25424823261422629 - Supplemental material for The causal association between the new gut microbiota and Alzheimer's disease: A Mendelian randomization study
Supplemental material, sj-docx-1-alr-10.1177_25424823261422629 for The causal association between the new gut microbiota and Alzheimer's disease: A Mendelian randomization study by Fengwen Lin, Xueqiang Yang, Xuelong Xie, Lihua Qiu, Congyang Zheng, Xuxiang Zheng, Zhongxun Li and Bin Nie in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
Thank you very much to all the authors and colleagues for their support and contributions to this research.
Ethical considerations
Given that all statistical analyses rely on publicly available data, no ethical approval is required.
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by “Diagnostic Model and Mechanism of Serum Myelin-Associated miRNA in Patients with Alzheimer's Disease” (No. s19002), and Sichuan Medical Association (No. S20250056).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.