
Abstract
Background
While statin use is linked to cognitive impairment, causal relationships with specific dementia subtypes remain unclear.
Objective
To investigate causal effects of statin medication, genetically mimicked statin effects, and plasma lipids on various cognitive impairments using Mendelian randomization (MR).
Methods
Utilizing summary genome-wide association studies data, we identified genetic variants associated with statin medication, cholesterol-dependent/independent statin effects, and dementia subtypes, such as Alzheimer's disease (AD), dementia in Alzheimer's disease (ADD), late-onset Alzheimer's disease, dementia with Lewy body (DLB), dementia with Lewy body in APOE ε4+ carriers, frontotemporal dementia, Parkinson's disease dementia, and vascular dementia. Univariable MR assessed causality, primarily via inverse variance weighting (IVW). Mediation effects were evaluated using the coefficient product method. Sensitivity analyses ensured robustness.
Results
IVW-MR indicated statin medication significantly reduced AD risk but increased ADD and DLB risk. Elevated total cholesterol (TC) increased dementia, ADD, and DLB, while higher low density lipoprotein cholesterol decreased AD risk. Specific DHCR24 variants reduced DLB risk, while HMGCS1 variants increased it. RAC1 variants lowered AD risk, whereas RHOC mitigated ADD risk. Critically, TC mediated 93.91% (95% CI = 68.27%∼119.55%) of statins’ effect on dementia, 84.37% (95% CI = 62.21%∼106.52%) on ADD, and 61.94% (95% CI = 43.47%∼80.42%) on DLB. The genetically mimicked effect of statins does not show a mediating role.
Conclusions
Statin medication, plasma lipids, and their genetic proxies exhibit causal links to cognitive impairment. Crucially, TC mediates statin-associated risks for cognitive impairment.
Introduction
Cognitive impairment is a pressing public health concern. Currently, an estimated 55 million individuals around the globe are grappling with cognitive impairment, and the global cost of this disease amounts to US $1.3 trillion. 1 Due to aging population, the global population living with cognitive impairment is anticipated to soar to approximately 150 million by 2050. 2 Dementia is a memory and cognition-related neurological disorder, with various subtypes including Alzheimer's disease (AD), dementia with Lewy body (DLB), Parkinson's disease dementia (PDD), frontotemporal dementia (FTD), and vascular dementia (VaD). 3 Nevertheless, without advancements in treatments or preventive therapies, it is crucial to continue investigating risks and protective factors, thus providing the potential for more expedited and significant enhancements in patient care and public health.
Around the world, there are currently more than 200 million individuals who are taking statin therapy. 4 The widespread use of statins necessitates careful assessment of their effects on the body. The majority of these patients are senior citizens who also face a heightened risk of cognitive deterioration. It has been suggested that statins can impact cognitive functioning; however, their precise effects, whether positive or negative, remain a subject of debate. Loera-Valencia et al. have proposed that using statins to restrict hypercholesterolemia in midlife can reduce dementia risk later in life. 5 A recent longitudinal registry-based cohort study found that individuals diagnosed with AD dementia (ADD) who take statins have cognitive improvement in a way related to the dose. 6 Nevertheless, clinical trials generally show no evidence that statin therapy benefits the progression of dementia symptoms.7,8 Case reports have highlighted the potential adverse effect of statin use on cognition, such as memory loss. 9 The conclusions drawn from Zhang et al.'s systematic review do not indicate that the use of statins in late life can prevent cognitive decline or dementia. 10 Moreover, the U.S. Food and Drug Administration has issued a serious alert about the possible detrimental effects of statins on cognitive function. Despite numerous observational cohort studies and handful statins clinical trials, observational studies with inherent epidemiological biases or a heterogeneous designs have led to biased conclusions.
Genome-wide association studies (GWAS) have made it possible to examine millions of genetic variations in individual genomes to uncover the relationship between genotype and phenotype. 11 Mendelian randomization (MR) techniques employ genetic variants as instrumental variables (IVs) to ascertain the causal linkage between an exposure and a specific outcome. 12 This approach provides an answer to the challenges of confounding and reverse causation that are commonly faced in observational research. 13
In this research, we performed an MR analysis to explore the causal link between the statin medication, genetically mimicked statins’ biological effects, plasma lipids, and various forms of cognitive impairment (such as AD, FTD, DLB, PDD, and VaD), using publicly accessible summary statistics. Subsequently, we investigated whether genetically mimicked statins’ biological effects and lipids act as potential mediators in the process from statin medication to cognitive impairment.
Methods
Study design
The study encompasses three key aspects as shown in Figure 1: investigating the causal links of statin medication on nine dementias (step 1), evaluating genetically mimicked statins’ biological effects and plasma lipids on four dementias (step 2), and conducting a mediation analysis of these genes and lipids in the process from statin medication to the development of dementias (step 3). Single-nucleotide polymorphisms (SNPs) were designated as IVs. MR is predicated on three stringent assumptions: (1) the IVs are highly linked to exposure factors; (2) IVs should be independent of any confounding variables; (3) IVs can only have an impact on the outcome through exposure, and not directly. 14 This research did not involve animal or human subjects, nor any data containing personal information, no ethics committee approval was required.

Study overview. Step 1 illustrates the causal relationships between statin medication and dementias. Step 2 represents the causal relationships between genetically mimicked statins’ biological effects and dementias. Step 3 demonstrates the mediating analysis of genetically mimicked statins’ biological effects within the process linking statin medication to dementias. Path c encompasses the overall impact of statin path a represents the causal influence of statin medication on genetically mimicked statins’ biological effects; path b represents the causal influence of genetically mimicked statins’ biological effects on dementias.
Genetic instrument choosing for exposures
The information regarding the summary statistics of SNPs related to statin medication with p-values <5 × 10−7 were derived from the IEU Open GWAS repository (https://gwas.mrcieu.ac.uk/), which restricted participants to Europeans, with 68,782 cases and 150,010 controls. The GWAS summary data of total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) were derived from the IEU Open GWAS database, with SNPs meeting a significance level of 5 × 10−8 as the threshold. All the chosen SNPs were grouped based on a linkage disequilibrium (LD) threshold value of r2 < 0.001 and a distance >10,000 kb using a European LD reference panel. 15 Subsequently, the remaining SNPs were investigated in the LDlink database (http://www.ldlink.nih.gov/) to ascertain whether these SNPs were correlated with confounding factors, including less education, hearing loss, smoking, depression, social isolation, physical inactivity, air pollution, traumatic brain injury.16,17 The rest of the SNPs were employed to compute the F-statistic and explained variance (R2) parameters, which are utilized to assess the strength of IVs. 18 The F-statistics that have a value below 10 are deemed to be weak instruments. 18 Each R2 and F are shown in Supplemental Tables 1 and 2.
To assess the possible impact and underlying processes of statins on multiple dementia types, expression quantitative trait loci (eQTL) data with a p-value < 5 × 10−7 were retrieved from the eQTLGen database (https://www.eqtlgen.org/cis-eqtls.html), in an effort to genetically replicate the effects of statin treatment. 19 We utilized whole-blood cis-eQTL in a ±5 kilobases flank around 25 genes encoding proteins involved in cholesterol synthesis, and approximately 20 Rho GTPase gene regions. 20 Our aim was to genetically replicate the cholesterol-dependent and independent effects of statins.
Genetic instrument selection for outcomes
The data on GWAS summary for dementia, including AD, ADD, FTD, VaD, PDD, DLB, and DLBA, were derived from the IEU Open GWAS repository, with participants restricted to European descent. The GWAS summary data on late-onset Alzheimer's disease (LOAD) were extracted from the study carried out by Wightman et al., 21 and are now accessible in the GWAS Catalog database (https://www.ebi.ac.uk/gwas/). Detailed information can be found in Supplemental Table 3.
MR primary analysis
The potential impact of the exposure on the outcome was evaluated through a two-sample MR study that incorporated inverse variance-weighting (IVW) with random effects, along with four additional sensitivity methods, namely, MR-Egger, weighted median, weighted mode and simple mode. The IVW approach was employed as the primary analytical technique, while the Wald ratios test was applied for variables with a single IV. 22 The MR findings were expressed as odds ratios (ORs) along with their corresponding 95% confidence intervals (CI). The findings were deemed statistically significant if the IVW p-value was lower than 0.05, and there was concordance between the IVW and MR-Egger findings.
Mediation analysis
A two-sample MR study was utilized to examine the effect of statin medication on the genetically mimicked statins’ effects and lipids, as well as the genetically mimicked statins’ effects and lipids on various dementia outcomes. The mediation analysis was carried out using the IVW method’ β value. To evaluate the indirect influence of statin medication on dementias outcome, we multiplied the results of the two MR analyses. The mediation proportion was computed using the product-of-coefficients method.23,24 Additionally, we determined the proportion of mediated effects using the formula of indirect effect divided by overall effect.
Sensitivity analysis
To interpret the heterogeneity, we utilized Cochran's Q statistic and its corresponding I2 index that presents the degree of heterogeneity as a percentage. 25 Additionally, we employed the MR-PRESSO package to detect and remove outlier SNPs for accuracy improvement and created scatter plots to visualize the MR results. 26 We conducted a leave-one-out analysis to assess the effect of each SNP on the results by excluding one SNP at a time and applying an IVW method to the rest SNPs to determine their possible influence on the estimates. The MR-Egger intercept was utilized to investigate the possibility of pleiotropic effects. 27
All statistical analyses were carried out utilizing R (version 4.3.3) statistical software. The MR analysis was conducted using the “TwoSampleMR” package (version 0.6.2), which is also available in R. In MR analysis, p < 0.05 is typically considered as evidence of a causal link between the exposure and outcome variables.
Results
Causal effects of statin medication on multiple dementia types
In the UVMR analysis, the IVW analysis showed that an increase of one standard deviation in genetically predicted statin medication was linked to a 5.1% decrease in the risk of AD, with an OR of 0.949 (95% CI = 0.921∼0.977, p = 0.000) (Figure 2). The effects of statin medication on dementia were (OR = 1.067, 95% CI = 1.003∼1.136, p = 0.041), as well as on ADD (OR = 1.145, 95% CI = 1.053∼1.244, p = 0.002), DLB (OR = 1.181, 95% CI = 1.047∼1.332, p = 0.007), and LOAD (OR = 1.141, 95% CI = 1.065∼1.223, p = 0.000) (Figure 2). However, the sensitivity analysis revealed a possibility of horizontal pleiotropy in LOAD. The IVW and MR-Egger analyses yielded no indication of statin medication having a causal effect on DLBA, VaD, PDD, or FTD (Figure 2, Supplemental Table 4). We observed a range of low to moderate heterogeneity in the MR estimates derived from individual studies (Supplemental Table 5).

Forest plots presenting MR results for statin medication on multiple dementia types.
Causal effects of the cholesterol-dependent genetically mimicked statins’ effect and lipids on multiple dementia types
To replicate the genetic effect of statins on dementia, eQTL data (sourced from the eQTLGen Consortium) for a total of 21/25 genes involved in the cholesterol biosynthesis pathway were chosen for analysis based on a strong correlation with at least one identified SNP. 20 Moreover, TC/HDL-C/LDL-C-related SNPs were retrieved from the IEU Open GWAS to investigate the causative link of cholesterol-dependent pathway in dementia.
In the UVMR analysis, the associations of LDL-C, DHCR24, and HMGCS1 with DLB were found with ORs of 1.200 (95% CI = 1.033∼1.393, p = 0.017), 0.722 (95% CI = 0.544∼0.956, p = 0.023), and 5.392 (95% CI = 1.175∼24.740, p = 0.030), respectively (Figure 3, Supplemental Figure 1). However, the sensitivity analysis revealed a possibility of horizontal pleiotropy in LDL-C. The effects of TC on dementia were (OR = 1.161, 95% CI = 1.029∼1.310, p = 0.016), as well as on ADD (OR = 1.320, 95% CI = 1.095∼1.591, p = 0.004), and DLB (OR = 1.285, 95% CI = 1.038∼1.591, p = 0.022) (Figure 3, Supplemental Figure 1). Additionally, LDL-C was discovered as a protective element in the prevention of AD (OR = 0.908, 95% CI = 0.864∼0.955, p = 0.000) (Figure 3, Supplemental Figure 1). In general, the degree of heterogeneity among these analyses varied from mild to moderate, and the examination for horizontal pleiotropy did not reveal any significant evidence, except as mentioned above (Supplemental Tables 6 and 7).
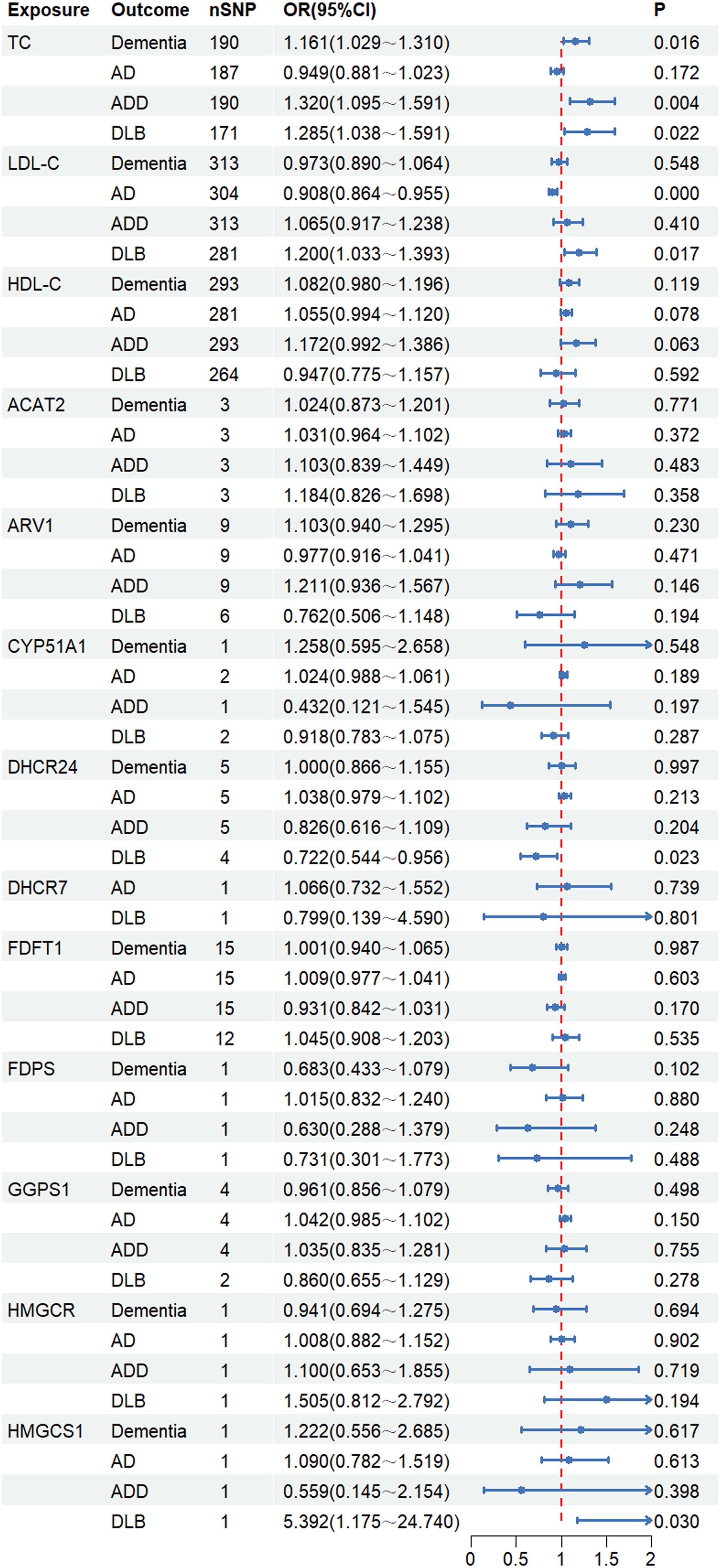
Forest plots presenting the associations between the genetically mimicked statins’ biological effects through cholesterol-dependent (through lipids and cholesterol biosynthesis pathways) and dementias.
Causal effects of the cholesterol-independent genetically mimicked statins’ effect on multiple dementia types
Subsequently, a total of 14 out of 20 genes belonging to the Rho GTPase family were chosen for investigation utilizing eQTLGen Consortium-derived eQTL data. 20
Through the use of MR analyses that incorporated SNPs in these gene regions, a connection was established between RAC1 and AD (OR = 0.896, 95% CI = 0.847∼0.948, p = 0.000), as well as RHOC and ADD (OR = 0.782, 95% CI = 0.629∼0.973, p = 0.027) (Figure 4, Supplemental Table 8), suggesting that statins may reduce the development of AD and ADD through a cholesterol-independent pathway. These analyses exhibited varying levels of heterogeneity, ranging from nonexistent to minimal, with no evidence of horizontal pleiotropy (Supplemental Table 8).
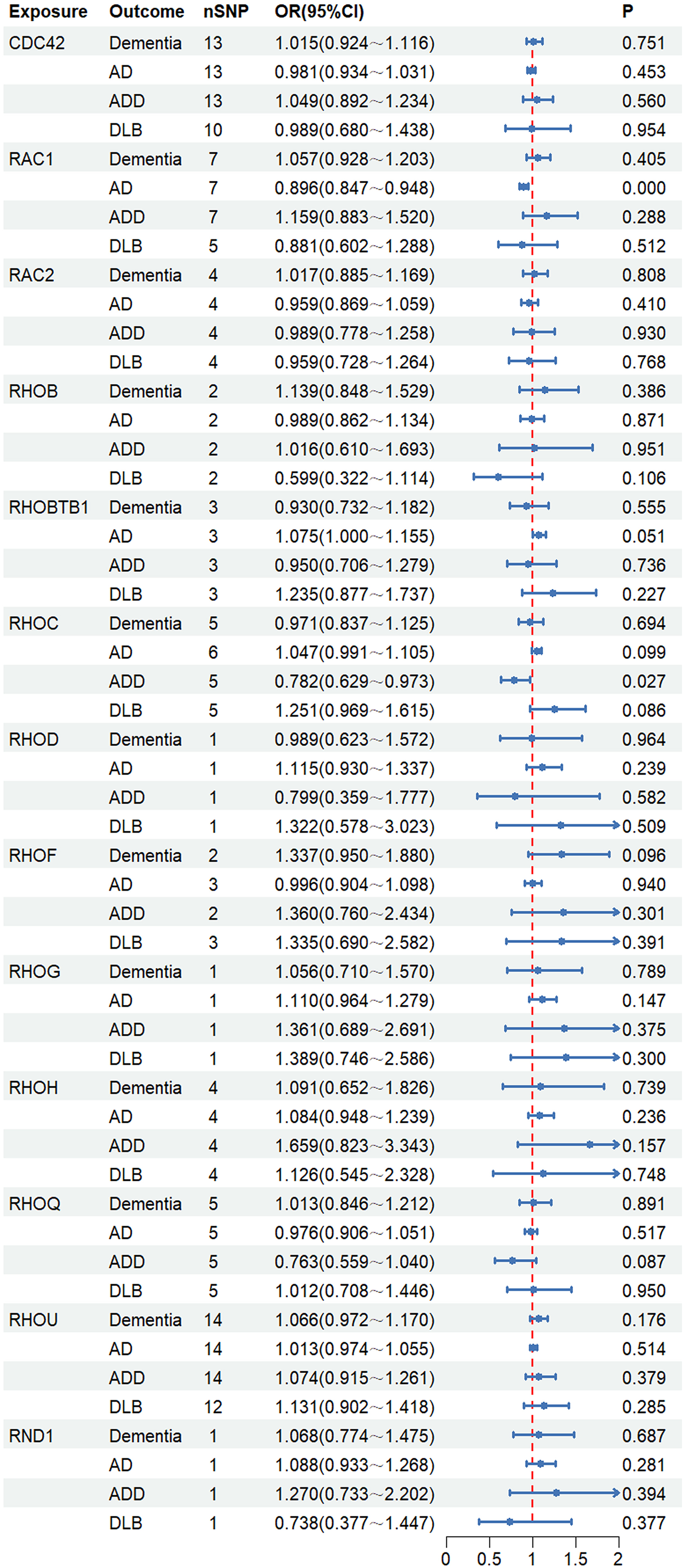
Forest plots presenting the associations between the genetically mimicked statins’ biological effects through cholesterol-independent via Rho GTPases and dementias.
Mediation analysis
This study found that both statin medication, plasma lipids, and the genetically mimicked statins’ effects had causal effects on dementias. These genes appeared to act as a mediator in the link between statin medication and dementias. After matching statin medication and DHCR24, HMGCS1, RAC1, or RHOC, no SNP can be used as IVs, indicating that these genes did not serve as a mediator in the connection between statin medication and dementias.
Mediation analysis revealed that statin medication's causal effects on dementia was largely mediated by TC, amounting to 93.91% (95% CI = 68.27%∼119.55%) of the overall effect. Additionally, the mediating proportion of TC in the relationship between statin medication and ADD was found to be 84.37% (95% CI = 62.21%∼106.52%), while that between statin medication and DLB was calculated to be 61.94% (95% CI = 43.47%∼80.42%). The illustration of these findings can be seen in Figure 5 and Supplemental Table 9.

MR estimates of proportions mediated by TC in the causal link between statin medication and dementias. Histograms demonstrate the mediated proportions (95% CIs).
Discussion
This MR study sheds new light on the causal relationship between statin medication, their genetically replicated effects, plasma lipids, and diverse forms of cognitive impairment, with a focus on the role of lipids and these genes as mediators. Our research found that there is one positive and three negative causal relationships between the genetic liability for statin medication and dementia, as well as four positive and four negative connections between plasma lipids, genetically mimicked statins’ biological effects, and dementia. Of these, TC accounted for a large proportion in the association between statin medication and dementia (93.91%), statin medication and ADD (84.37%), as well as statin medication and DLB (61.94%). Genetically mimic statins biological effects did not act as mediating factors. These results emphasize the significance of considering genetic and environmental elements when comprehending the etiology of cognitive impairment, and the potential benefits and risks associated with statin medication.
AD is the widely recognized form of cognitive impairment, and it can be classified into two categories: early-onset and late-onset. 28 A burgeoning body of observational research has identified a link between the statin use and the onset of cognitive impairment, particularly AD. Statins have been linked to a reduced likelihood of developing dementia and a slowing down of the progression of AD. 29 A comprehensive meta-analysis, incorporating both observational studies and a randomized control trial, revealed a substantial protective effect of statin use against all-cause dementia and AD. 30 Our current research uncovered a correlation between statin medication and a reduced risk of AD, as determined by an MR study, which is in accordance with previous studies and provides further insight into existing studies. Statins are highly effective medications for lowering levels of LDL-C and TC. Our investigation also discovered that both LDL-C and TC were linked to a decreased risk of AD, with potential pleiotropy for the former. The current results provide insight into the role that statin medication and lipid levels play as genetic modifiers of AD risk. Nevertheless, increasing evidence indicates that the therapeutic advantages of statins can significantly vary according to the age, gender, race, education, alcohol use, and genotype of patients. Li and colleagues’ research discovered that the advantages were limited to individuals under 80 years of age, implying that statins may cease to be beneficial for cognition at a certain stage in life. 31 Our research discovered that statin medication could potentially raise the risk of dementia by 6.7% and lead to a 14.1% increased likelihood of developing LOAD, with potential pleiotropy for the later. Furthermore, we found that TC levels were linked to a 16.1% greater risk of developing dementia. A comprehensive analysis of global populations indicated that women have a greater susceptibility for developing dementia than men. 16 Rajan's research provides Class II evidence that among individuals aged 65 years or older, the initiation of statins is linked to a diminished risk of developing AD, particularly when an APOE ε4 allele is present. 32 Comparatively little knowledge is available on how statins affect cognitive decline in individuals with diagnosed AD. Statin use in AD patients didn’t improve cognition in clinical trials, possibly due to underpowered studies or less rigorous assessments.33,34 Contrary to previous research findings, 6 our study indicated that statin medication for diagnosed AD could potentially have detrimental effects on cognitive function, potentially due to biases in observational studies. In conjunction with previous studies, our findings indicate that statin medication and LDL-C are linked to a decreased risk of AD, but statin medication increases the risk of dementia and AD-related dementia, which is an extension of previous research.
In addition to AD, there are other subtypes of dementia. Consequently, given the diverse types of dementia, it is challenging to comprehensively assess the impact of statin medication on dementia through observational studies. DLB accounts for 25% of all dementia cases, making it the second well-known type of dementia following AD. 35 Currently, there are no medications available that have been approved to treat DLB in many regions. Targeting neuro-immune responses may be a promising therapy for DLB due to age-related inflammation affecting α-synuclein pathology. 36 Indeed, statins possess anti-inflammatory and immunomodulatory effects in addition to their lipid-lowering properties. 20 Our investigation discovered that both statin medication and TC level were linked to an elevated risk of DLB. However, the underlying mechanisms that contribute to the harmful effects of statins on DLB are yet to be explored.
Statins have multiple effects on cognition, which are mediated by a variety of neurodegenerative processes that may either depend on cholesterol or be independent of it. Statins reduce LDL-C levels by blocking the function of 3-hydroxy-3-methylglutaryl coenzyme A reductase (HMGCR). 37 We employed gene variants associated with HMGCR and other downstream targets to emulate the cholesterol-dependent impacts of statins in the context of dementia. MR results demonstrated that the genetic mimicry of statins through DHCR24 and HMGCS1 was found to have a causal role in DLB among Europeans. DHCR24 reduces the risk of DLB, while HMGCS1 obviously increases the likelihood of developing DLB. 24-dehydrocholesterol reductase (DHCR24) is a critical mediator of cholesterol synthesis and homeostasis. Knocking down DHCR24 in astrocytes can increase tau hyperphosphorylation, possibly leading to AD and other tauopathies. 38 Zhang and colleagues propose that DHCR24 ameliorates AD-related pathology and cognitive decline in 5xFAD mice by elevating hippocampal cholesterol levels. 39 Nevertheless, this study failed to establish a causal connection between DHCR24 and AD or ADD among Europeans. Therefore, it is essential to conduct further research to uncover the contribution of DHCR24 to the progression of AD in patients. Furthermore, our focus was shifted to investigating the causal relationship between Rho GTPases (i.e., mimicking the cholesterol-independent effect of statins) and dementia. MR results demonstrated that RAC1 lowers the likelihood of the onset of AD, and RHOC mitigates the risk of dementia in AD patients. The mechanisms for RAC1 and RHOC's protective roles in AD are unclear. RAC1 is a highly researched member of Rho GTPases within the nervous system. The overactivity of RAC1 affects glutamatergic synapses in the hippocampus and cognitive function in mice. 40 According to Hoeppner et al., RHOC is essential for maintaining vascular homeostasis in endothelial cells. 41 These results lend credence to the protective roles of RAC1 and RHOC in AD that we observed in the current results. Taken together, the present findings provide insight into statins’ cholesterol-dependent gene-mimicking effect, mediated by DHCR24 and HMGCS1, which mainly impacts the development of DLB. In addition, their cholesterol-independent gene-mimicking effect, mediated by RAC1 and RHOC, predominantly affects the development of AD.
This study is pioneering in its efforts to comprehensively examine the causal links between statin medication, their genetically mimicked effects, plasma lipids, and several dementia subtypes through MR analysis, as well as to identify the mediators in the statin medication-dementias pathway. This design is considerably less vulnerable to confounders and reverse causation than conventional observational studies, addressing a key limitation of previous research. Unlike clinical trials that target single outcomes, our MR analysis simultaneously evaluates causal effects of statins across dementia subtypes, minimizing confounding from behavioral or environmental factors. Statins exhibited differential impacts across dementia subtypes, highlighting heterogeneous cognitive influences often masked by clinical trial heterogeneity. Mediation analysis identified TC as a key mediator, suggesting cholesterol metabolism as a potential intervention target. By leveraging genetic variants to simulate long-term statin exposure, we revealed sustained effects beyond the scope of conventional clinical trials.
This MR study highlights critical clinical considerations for statin use, especially in elderly and cognitively vulnerable individuals. While statins appear protective against AD, the suggested increased risks for ADD and DLB warrant caution. The identification of TC as a key mediator underscores the need for personalized statin prescriptions based on individual lipid profiles. A tailored approach, considering genetic predispositions and cognitive status, is crucial. Future research should prioritize targeted interventions addressing specific lipid pathways implicated in different dementia subtypes, thus allowing tailored therapeutic interventions with reduced side-effects and complications.
However, our study possessed certain limitations. First, our analysis was confined to European-ancestry cohorts, without accounting for demographic heterogeneity across datasets. Genetic and environmental differences among populations may alter causal inferences, limiting generalizability to other ethnic groups. Future studies should include diverse ancestries to validate and broaden the applicability of our findings. Second, sample overlap, primarily from UK Biobank inclusion in IEU Open GWAS, may introduce bias, though estimated overlap remained modest (≤8.6%). Based on simulation studies, this level of overlap likely biases odds ratios by <10%, which is unlikely to alter our primary conclusions given the larger effect sizes observed. Unquantified overlap in other datasets may still contribute residual bias. The shared genetic architecture among lipid traits suggests that the mediating role of TC may partly reflect contributions from correlated lipid phenotypes. Third, extensive sensitivity analyses were conducted to address potential violations of MR assumptions; however, residual horizontal pleiotropy cannot be fully excluded. This is especially pertinent for the LDL-C and LOAD association, where pleiotropic pathways or confounding by correlated lipid traits may contribute. These results highlight the need for further validation using approaches such as multivariable MR to better disentangle these relationships. Fourth, interpretation of the mediation analysis for TC should be cautious, given the wide confidence intervals that exceed 100%. This likely arises from the inherent statistical uncertainty in estimating ratio-based measures like the proportion mediated, particularly when the total effect is variable. Fifth, this study was designed to investigate total blood lipid levels and thus did not consider whether there are subtypes of these fractions (e.g., LDL subparticles) that might play different roles in dementia risk. Sixth, our analysis is constrained by the finite number of SNPs available, which represent only a fraction of the genome and may omit relevant genetic loci. Seventh, we cannot exclude the possibility that the absence of a causal link between statins and dementias is due to other pathways unrelated to Rho GTPases or HMGCR inhibition, which we could not investigate here because such pathways remain to be identified. Eighth, GWAS of diseases primarily assess disease risk rather than progression. Thus, the identified findings may serve as biomarkers for prediction or diagnosis, or as drug targets for prevention, but not necessarily for disease progression. Finally, despite MR's causal inference strengths, findings require validation in well-powered randomized controlled trials to confirm causality.
This MR study provides key evidence regarding the causal protective and deleterious effects of statin medication, plasma lipids, and their genetically mimicked effects on various types of cognitive impairment. TC may act as an intermediary in the pathway through which statins influence cognitive impairment, rather than directly modulating cholesterol-dependent or -independent pathways. Further investigation into the underlying causal pathways is warranted to inform prevention and intervention approaches.
Supplemental Material
sj-zip-1-alr-10.1177_25424823261440863 - Supplemental material for Exploring the role of statin interventions on cognitive function by Mendelian randomization study
Supplemental material, sj-zip-1-alr-10.1177_25424823261440863 for Exploring the role of statin interventions on cognitive function by Mendelian randomization study by Yan He, Heng Yang, Ting Pan, Fang Wang, Xiaofeng Zeng, Jiagui Huang and Qin Yang in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
We express our heartfelt gratitude to the studies and consortia that have been referenced and incorporated into this analysis for making public datasets available and managing summary statistics.
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the the Natural Science Foundation of Sichuan Province, the National Natural Science Foundation of China, Health Commission of Sichuan Province Medical Science and Technology Program, Medical Research Project of Sichuan Medical Association, (grant number 2025ZNSFSC0589, 82171456, 24QNMP024, 24WSXT075, S2024048).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available within the article and its supplemental material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.