
Abstract
Plasmablastic lymphoma of the oral cavity is a very rare and only recently recognized entity that has been identified almost exclusively in HIV-infected individuals. It has a predilection for the oral cavity, often exhibits very aggressive behavior and has a poor prognosis. The use of 18F-FDG PET/CT in the evaluation of HIV-associated lymphomas is a recent development, and its use in the staging of plasmablastic lymphoma of the oral cavity has not been previously reported. This rare report highlights the usefulness of 18F-FDG PET/CT in the staging of plasmablastic lymphoma of the oral cavity.
Plasmablastic lymphoma is a relatively new entity considered to be a subtype of diffuse large B-cell lymphoma that is seen almost exclusively in HIV patients. It has a predilection for the oral cavity, specifically the gingival and palate mucosa. It accounts for only 3% of all HIV-positive lymphomas, and only 60 cases have been reported in the literature. Epstein Barr virus (EBV) and human herpes virus 8 (HHV-8) infections have been implicated in its pathogenesis, and it generally has a poor prognosis (1-8). 18F-FDG PET/CT is very useful in the evaluation of some HIV-associated lymphomas, although the literature at this time is very limited (9-13). While 18F-FDG uptake in plasmablastic lymphoma of the skin, testes, and bone has been observed (14, 15), this is the first description of the use of 18F-FDG PET/CT to stage plasmablastic lymphoma of the oral cavity in an HIV-positive patient.
Case report
A 46-year-old woman from Uganda presented with a rapidly growing facial mass. She had a 13-year history of an untreated HIV infection. She was initially diagnosed with a dental abscess, and treated with dental extraction followed by two weeks of antibiotics; however, the right lower facial mass continued to grow in size. Three weeks after the dental extraction the patient presented again, this time complaining of dysphagia. The right lower facial mass was biopsied, and the patient was referred for a staging 18F-FDG PET/CT (Discovery ST, GE Healthcare, Montreal, Canada). Maximum intensity projection (MIP) images with anterior and left lateral views showed an extensive and intensely 18F-FDG positive mass involving the soft tissues of the right lower face, the right palate, right maxillary sinus, and inferior nasal concha (Fig. 1). There were also numerous 18F-FDG-avid lymph nodes scattered throughout the body (cervical, axillary, mediastinal, hilar, cardio-phrenic, celiac, peri-portal, para-aortic, splenic hilar, external iliac, and inguinal regions), representing HIV-related adenopathy (biopsy of a right inguinal node, and a bone marrow biopsy of the right iliac crest did not show any evidence of lymphoma, although this did not exclude the possibility of one or several of the lymph nodes being affected by lymphoma). Transaxial, coronal, and sagittal views (Fig. 2) showed intense 18F-FDG uptake in the large right facial soft tissue mass which was contiguous with the right palate measuring 5.3 × 5.3 × 6.9 cm in transverse, AP, and craniocaudal dimensions with a maximum standardized uptake value (SUVmax) of 39. There was extension into the right maxillary sinus and right inferior nasal concha.
18F-FDG PET/CT maximum intensity projection (MIP) images with anterior and left lateral views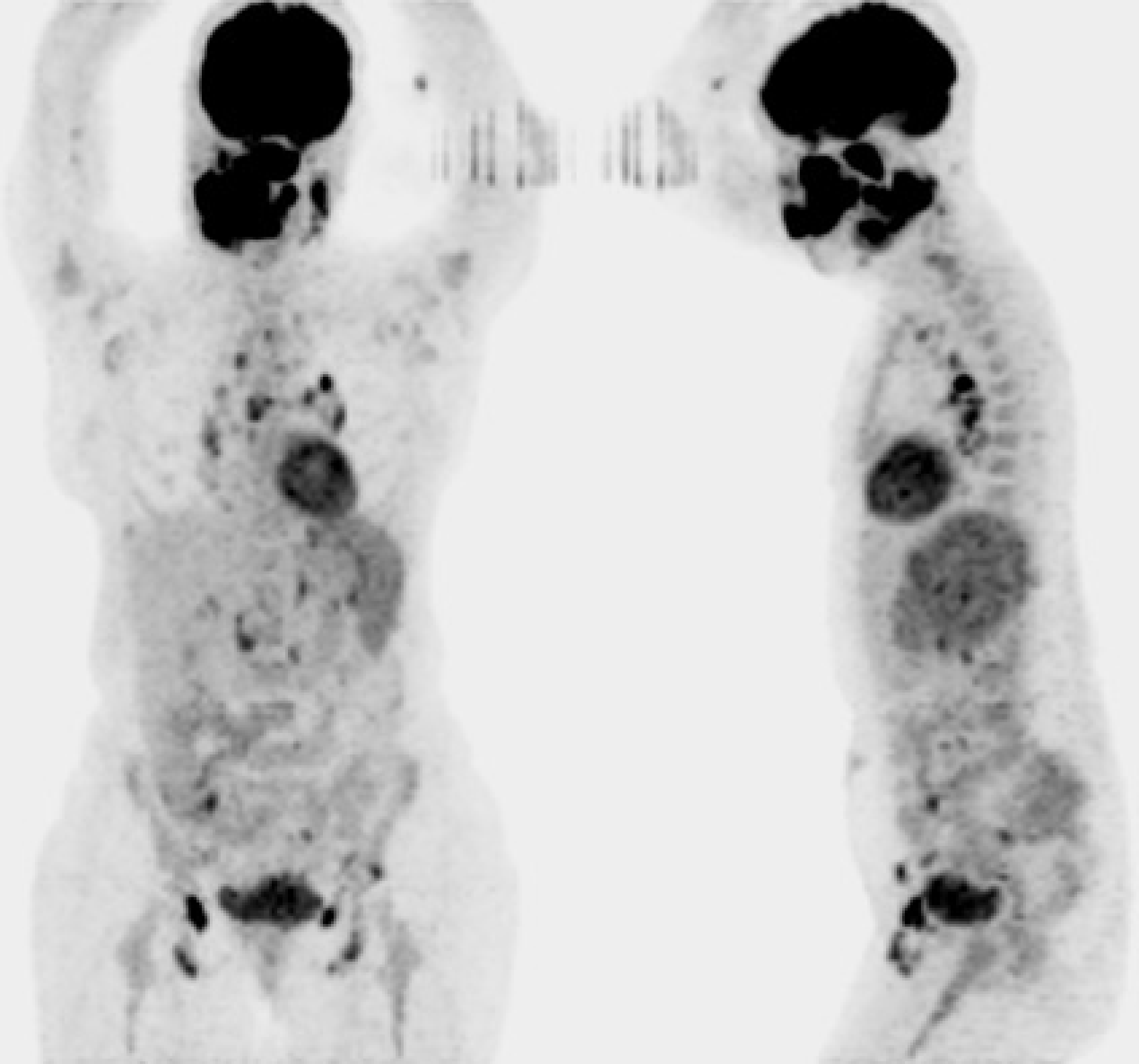
Transaxial, coronal, and sagittal views of the head and neck of the (a) CT portion of the PET/CT, (b) PET, and (c) PET/CT fusion images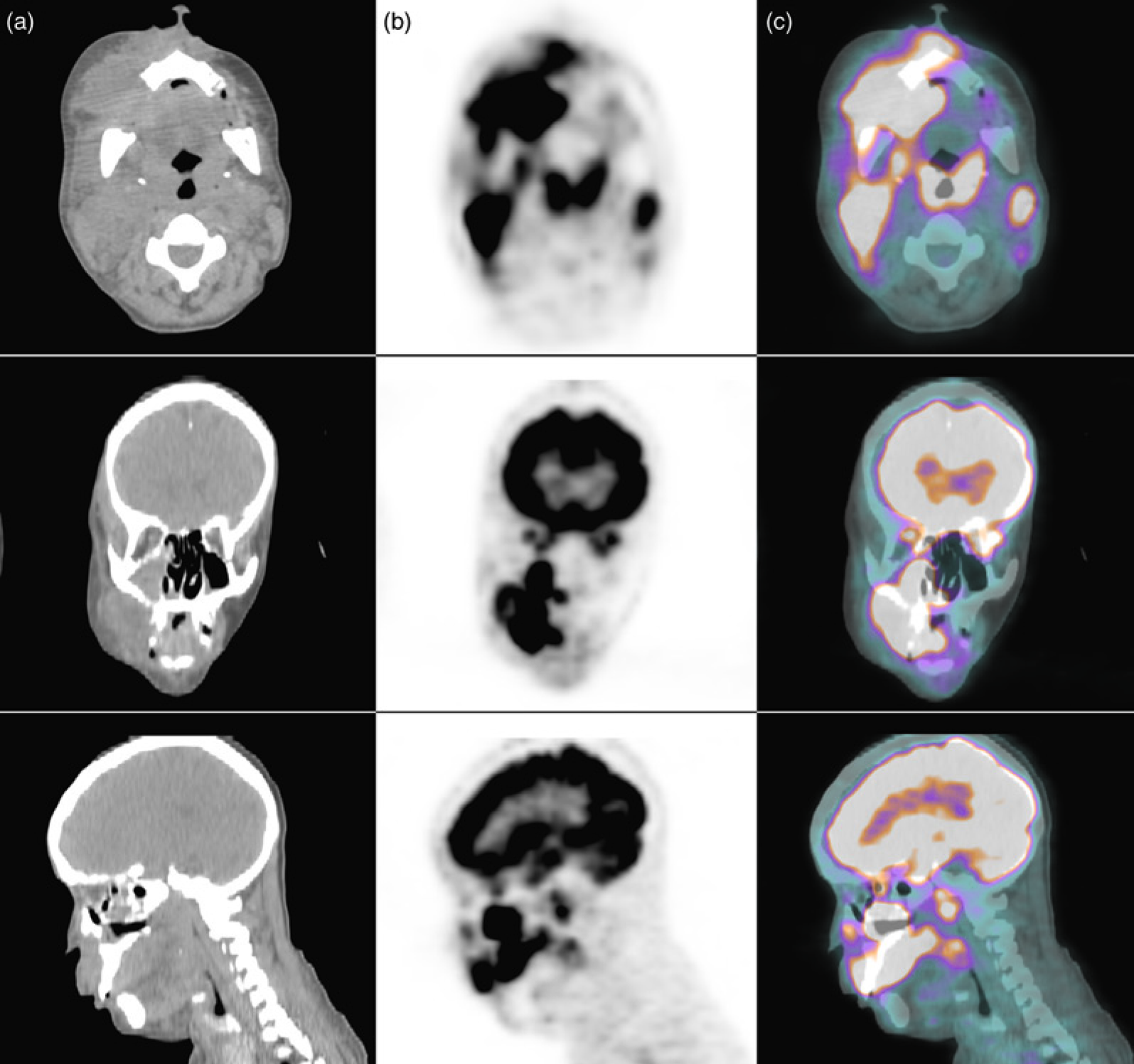
Biopsy of the right palate showed multiple fragments lined by squamous epithelium with focal areas of ulceration. The underlying stroma showed a diffuse lymphoid proliferation with a starry sky pattern. The vast majority of the cells were medium to large size with atypical irregular nuclei having a variably clumped chromatin, very prominent nucleoli, and moderately abundant cytoplasm. Immunohistochemistry showed: CD20 (+ in few cells), CD45 (+), Mum-1 (strong positive nuclear staining), CD38 (strongly positive in all tumor cells), CD79a (positive in moderate number of tumor cells), Kappa (positive in few plasma cells), Lambda (positive in rare plasma cells), Ki67 > 90%. Negative immunohistochemistry was seen for: Bcl2, Bcl6, CD10, CD23, CD30, CD43, CD45RO, CD56, CD138 (negative, except in a few plasma cells), TdT, EBV, HSV8, EMA, PAX-5, Keratin AE1/AE3, and S-100. Molecular studies showed a clonal population of B-cells for IgH, absence of a clonal population of T-cells, t(8;14), c-myc-IgG rearrangement, and clonal integration of EBV (detected by Southern blotting). These findings were diagnostic for plasmablastic subtype of diffuse large B-cell lymphoma. The patient's laboratory values included: HIV viral load 228603 copies, CD4 count 23 cells/ ul (normal 420-1980), CD8 count 311 cells/ul (normal 160- 990), CD4/CD8 ratio 0.1 (normal 0.9-5.5), CD3 absolute 344 cells/ul (normal 750-2650).
Following the PET/CT and biopsy results, the patient was started on highly active antiretroviral therapy (HAART) and CHOP chemotherapy (cyclophosphamide, doxorubicin, vincristine, prednisone), because the extent of metabolically active disease as determined by PET/CT precluded the possibility of surgical excision.
Discussion
Infection with the human immunodeficiency virus (HIV) dramatically increases the risk of development of lymphoma (about 25-30% of all patients with AIDS will develop lymphoma). About 95% are B-cell lymphomas and 60% are considered to be high grade. Typically, HIV-related lymphomas present with widespread disease with a predilection for extranodal sites (1-4).
Plasmablastic lymphoma (PBL) is a relatively new entity considered to be a subtype of diffuse large B-cell lymphoma with a unique immunophenotype, with an estimated prevalence of 3% of all lymphomas in the HIV population (5). Approximately 60 cases fulfilling the clinico-pathological characteristics of PBL have been reported in the literature (6). Epstein Barr virus (EBV), as well as human herpes virus-8, are often found present in patients with PBL, implying that these viruses may play a role in its pathogenesis (7, 8). Recent genetic studies have also shown Ig/myc rearrangements as the main cytogenetic alteration in PBL (9, 10), and a c-myc-IgG rearrangement was identified in our patient. PBL has a predilection for the oral cavity, specifically for gingival and palatal mucosa; it effaces the mucosal architecture with infiltration of the submucosa and extension to the mucosal surface with ulceration, and has the propensity to infiltrate adjacent bone. The prognosis is poor with death occurring between 1-24 months after diagnosis, with average survival time of 6 months (1-4).
Although the use of 18F-FDG PET/CT in differentiating central nervous system (CNS) toxoplasmosis infection from lymphoma in HIV-infected patients is well known (11, 12), the role of PET/CT in the evaluation of HIV-associated lymphomas is less clear and currently under active investigation (13-15). 18F-FDG uptake in metastatic lesions of PBL affecting the skin, testis, and bone, has been described in a few case reports (16, 17), however, the use of 18F-FDG PET/CT in the staging of PBL of the oral cavity in HIV-infected patients has not been previously described in the literature. In this case, the PET/CT was very useful in determining the local extent of metabolically active disease, which guided the therapeutic management toward chemotherapy rather than surgical excision.
In conclusion, surgeons and oncologists should be aware of the usefulness of 18F-FDG PET/CT in the evaluation of plasmablastic lymphoma of the oral cavity in HIV positive patients. PET/CT can define the extent of metabolically active disease and help guide biopsy location as well as therapeutic management.
Footnotes
None.