
Abstract
Background
Recent reports indicate that numerical assessment of B-lines during transthoracic ultrasound may aid the differential diagnosis of acute diffuse pleuropulmonary disorders.
Purpose
To determine whether B-lines are different in normal and diseased lungs and whether they can be used to discriminate between different types of pulmonary disorders in acutely ill patients.
Material and Methods
In this multicenter study, transthoracic ultrasonography was performed on 193 patients with acute dyspnea, 193 healthy non-smokers, and 58 patients who had undergone pneumonectomy for lung cancer. Examinations were done with a low–medium frequency (3.5–5.0 MHz) convex probe and a high-frequency (8–12.5 MHz) linear probe. Video recordings were re-examined by a second set of examiners. In each participant, we measured the number of B-lines observed per scan.
Results
B-lines counts were higher in dyspnoic patients (means: 3.11 per scan per linear probe scan vs. 1.93 in healthy controls and 1.86 in pneumonectomized patients; P < 0.001 for all); all counts were higher when convex probes were used (5.4 in dyspnoic patients and 2 in healthy controls; P < 0.001 vs. the linear probe). Subgroups of dyspnoic patients defined by cause of dyspnea displayed no significant differences in the number of B-lines.
Conclusion
Our results demonstrate that there are a significant higher number of B-lines in the lungs of patients with dyspnea compared to healthy subjects and to pneumonectomized patients. Nevertheless, the quantification of B-lines does not make any significant contribution to the differential diagnosis of dyspnea.
Keywords
Diagnostic ultrasonography (US) is a valuable complementary technique for the study of pleuropulmonary diseases. It is widely available, low-cost, and has no significant biological effects. In addition, it allows real-time, multiplanar imaging that is highly portable and well suited for bedside assessments (1, 2). It has proved to be especially useful in emergency and critical care settings, where it is also used as a guide for percutaneous interventional procedures (1–5). On the other hand, the clinical applicability of this approach is strongly influenced by both anatomical factors, as well as by the physical properties of US. Its use in the study of pleural and pulmonary disease, for example, is limited by the presence of the bony rib cage, which markedly reduces the surface area of the lungs that can be visualized.
A basic understanding of the physical principles of ultrasound is essential for accurate, reliable interpretation of sonographic images of the chest cavity and its contents (as it is for other anatomical sites as well) (3, 6–10). Propagation of ultrasound within the human lung was first described by Dunn and Fry in 1961 (11–13) and it is now clear that substantial differences in the acoustic impedance of the chest wall structures and the air-filled lung parenchyma results in the reflection of over 96% of the US beam, a phenomenon that is responsible, along with cardiac and respiratory movements, for several types of potentially confusing reverberation artifacts (6, 10). These include the “ring-down”, defined B-lines, which appear as a solid streak of parallel bands radiating away from the air and differ in the pathophysiological mechanism of generation from the “comet-tail” artifacts. These latter consist of a trail of dense echoes that resembles a distally oriented comet-tail (14–19). There are also horizontal artifacts (i.e. “simple reverberation”) which consist of a series of evenly spaced, parallel echogenic lines situated below the pleural line. These are usually seen in the normal lung, but have been described as markedly increased in the lung of patients with severe pulmonary fibrosis (14). It is important to recall that the number of artifacts detected is highly dependent on the scanner settings used, particularly those regarding spatial resolution and the frequency of transmitted sound pulse and on the type of probe used.
Several recent reports indicate that assessment of the number of B-lines, commonly found in the lungs (including healthy ones and in pneumonectomy space), may be helpful in the differential diagnosis of acute diffuse pleuropulmonary disorders (16). Some authors define these vertical artifacts as “ring down”, but other times they are referred to as “comet tail” or “lines B” (17–21). In the present study, we always refer to “ring down” artifacts and name them as B-lines, in order to avoid any possible confounding definition.
The aim of this multicenter study was to determine whether B-lines numbers are indeed different in normal and diseased lungs and whether these numbers can be used to discriminate between different types of pulmonary disorders in acutely ill patients. Therefore, we investigated the B-lines observed on transthoracic US scans performed with both low–medium and high frequency US probes in a large series of patients with acute dyspnea and in control groups composed of healthy subjects and of patients who had undergone pneumonectomy.
Material and Methods
This multicenter study was conducted, with institutional ethics commission approval, between May 1, 2010 and June 31, 2011 in 10 acute healthcare facilities. Patients were recruited from the emergency and respiratory departments, intensive care units respiratory departments (ICUs), and intensive care cardiology, internal medicine, and gastroenterology wards on the basis of requests received in the radiology departments for chest radiography for “acute dyspnea”. Patients were contacted by the radiologist on duty at the time of the request and invited to take part in the study. Inclusion criteria were informed consent by patients and/or their proxies plus the attending physicians' authorization to perform transthoracic US.
For comparison purposes, we also examined two control groups. The first consisted of 193 healthy, non-smoking hospital employees (105 men, 87 women, aged 46 ± 1 years, range 19–58 years), who had recently (within 1 week of enrolment) undergone yearly physical examinations that included detailed medical histories, a complete physical examination, a chest X-ray, and an electrocardiogram. Candidates were excluded if the physical exam revealed any of the following: cardiac disease (any type), hypertension, pulmonary or pleural diseases, allergic diseases, chronic renal, or hepatic disease. The second control group was recruited from the Thoracic Surgery Outpatient Clinic of one of the participating hospitals. It included 58 patients (45 men, 13 women, aged 59 ± 8.9 years, range 48–68 years) who had undergone pneumonectomy for stage T1–2, N0 M0 lung tumors.
All three groups of participants underwent transthoracic ultrasonography performed at the bedside by (depending on the ward requesting the chest X-ray) cardiologists, internal medicine specialists, ICU physicians, pneumologists, or radiologists—all with a minimum of 5 (mean 7) years of experience in this technique. All patients with dyspnea were examined immediately after the execution for a chest X-ray. Each examination was done with two transducers: a low–medium frequency (3.5–5 MHz, depending on the physical characteristics of the subject) convex probe and a high-frequency (8–12.5 MHz) linear probe. The ultrasound scanners used in the different centers (Technos MPX, My Lab 25, and My Lab30 Gold [Esaote, Genoa, Italy]; Aplio XG and Xario XG [Toshiba, Tokyo, Japan]; HI Vision 6500 [Hitachi Medical Systems, Singapore]; Vivid 7 [GE Healthcare, (Waukesha, WI, USA)], were all used with the following settings for transthoracic study: depth of images (penetration): 7–14 cm; gain control: 50–60%; use of harmonic imaging; electronic focus: pleural line. The devices used had no more than 7 years of use and an annual maintenance was done.
Participants were examined in the sitting position, and scans were made bilaterally (except in the pneumonectomy patients, where only the pneumonectomy space was examined) through all ventral and latero-basal intercostal spaces. Ventral scans were made along the parasternal and mid-clavicular lines; the latero-basal scans were done along the posterior axillary line, and subcostal scans were also done with the convex probe. Each hemithorax was examined from apex to base, first with the convex probe, then with the linear probe. The complete examination lasted 10–15 min.
For each lung, the examiner recorded the presence and the number of B-lines detected with each probe at the second and fifth intercostal spaces in the anterior scans, in the seventh/eighth and 10th intercostals spaces in the latero-basal scans for a total of four observations per lung (eight in total) per probe. Results obtained for the right and left lungs were summed for healthy controls and patients with dyspnea, whereas the figures analyzed for pneumonectomy patients refer exclusively to the pneumonectomy space.
Video recordings of the examinations performed with each type of transducer (each lasting a minimum of 3 min) were later reviewed by a second group of examiners, all of whom were radiologists with 20 years of experience in transthoracic ultrasound. None of them had been involved in the original examinations, and all were blinded to the outcomes of those studies. These reviewers also recorded the presence and number of B-lines, as described above, and their findings were compared with those of the original examiners to assess interoperator variability.
The cause of each episode of dyspnea was definitively diagnosed by the physicians in charge of the patient on the basis of the laboratory tests and imaging studies they had ordered (including high-resolution computed tomography, as needed).
Statistical analysis
Intergroup differences in the number of detected B-lines were assessed with Poisson regression models for count data. Generalized estimating equations (GEE) (22) were used with a compound symmetry type matrix to account for repeated measurements within each patient. Group means with standard errors (SE) were calculated for the estimated number of vertical artifacts, and analyses were adjusted for participants' co-morbidities.
Findings obtained by original examiners and reviewers were analyzed separately. Inter-examiner concordance involving the number of detected B-lines was assessed with a generalized linear mixed-effects model to account for the double-nested design of data, and inter-examiner variability was tested with the Roy approach (23). P values of <0.05 were considered significant. All analyses were performed using SAS® software, release 9.1 (2011 SAS Institute Inc, Cary, NC, USA).
Results
Causes of dyspnea in the 193 patients studied
B-line artifact means along with 95% CI
Estimated total B-line artifacts mean ratios
Compared with the linear probe findings, the total numbers of B-lines detected with the convex probe were significantly higher in the dyspnea patients (P < 0.001) and in healthy controls (P < 0.001). No significant differences were found between examiners A and B as far as probe-type specific counts of B-lines were concerned.
Discussion
In recent years, the use of transthoracic pleuropulmonary ultrasound has been increasing in clinical setting. It is simple to perform, more economical than other imaging modalities, and well-suited for bedside and point-of-care evaluations. However, these advantages are offset by two major limitations. First, the bony cage surrounding the lungs (ribs, spine, sternum, clavicles) markedly restricts visualization, and only about 70% of the total pleural surface can actually be explored (24). Second, the air content of the lung tissue limits the depth of visualization. Consequently, while transthoracic ultrasound displays good reproducibility in the assessment of lesions located right below the pleural surface and in the detection of changes in their size during follow-up (25), deeper areas of the lung parenchyma cannot be adequately explored.
Because of the limitations outlined above, transthoracic ultrasound has mainly been used to detect and characterize pleural effusions and as a guide for invasive percutaneous procedures (e.g. chest-tube insertion, sampling pleural fluid or subpleural, anterior-superior, mediastinal, and diaphragmatic lesions for cytology or histology) (1–7). The usefulness of this approach in the diagnosis of diffuse pulmonary diseases remains controversial. Nonetheless, several groups maintain that the analysis of B-lines can make an important contribution toward the differential diagnosis of dyspnea and in predicting the outcome of diffuse pulmonary diseases (16–18). In this context, it is also important to point up that there is an overall problem about the nomenclature used to define these types of artifacts. The artifacts generated at the boundary between soft tissue/liquid and air, as those in the present study, are named as “ring down” definite B line. Nevertheless, some authors referred to these artifacts as “lung comet tail”. Hence, we decided to refer to these artifacts as B line in order to avoid any possible confusion generating by incongruence in the definitions.
In this multicenter study, we evaluated the number of B-lines in ultrasound pulmonary examination in a large sample of patients with acute dyspnea and compared the results with those obtained in healthy lungs and in the pneumonectomized chest cavities. The latter were studied because, as previously described, in pneumonectomized chest cavities artifacts result from the difference in acoustic impedance between soft tissue and air or liquid/fibrosis (26) (Fig. 1). The same parameters were also analyzed in subgroups of the dyspnea patients defined by the cause of the dyspnea. On the whole, the dyspnea group had a significantly higher number of B-lines compared to both the healthy subjects and the patients who had undergone pneumonectomy.
Latero-basal transthoracic US scan with 3.5 MHz convex probe in a pneumectomy patient reveal pleural line (yellow arrows) and B-lines (“ring-down”) (white arrowhead)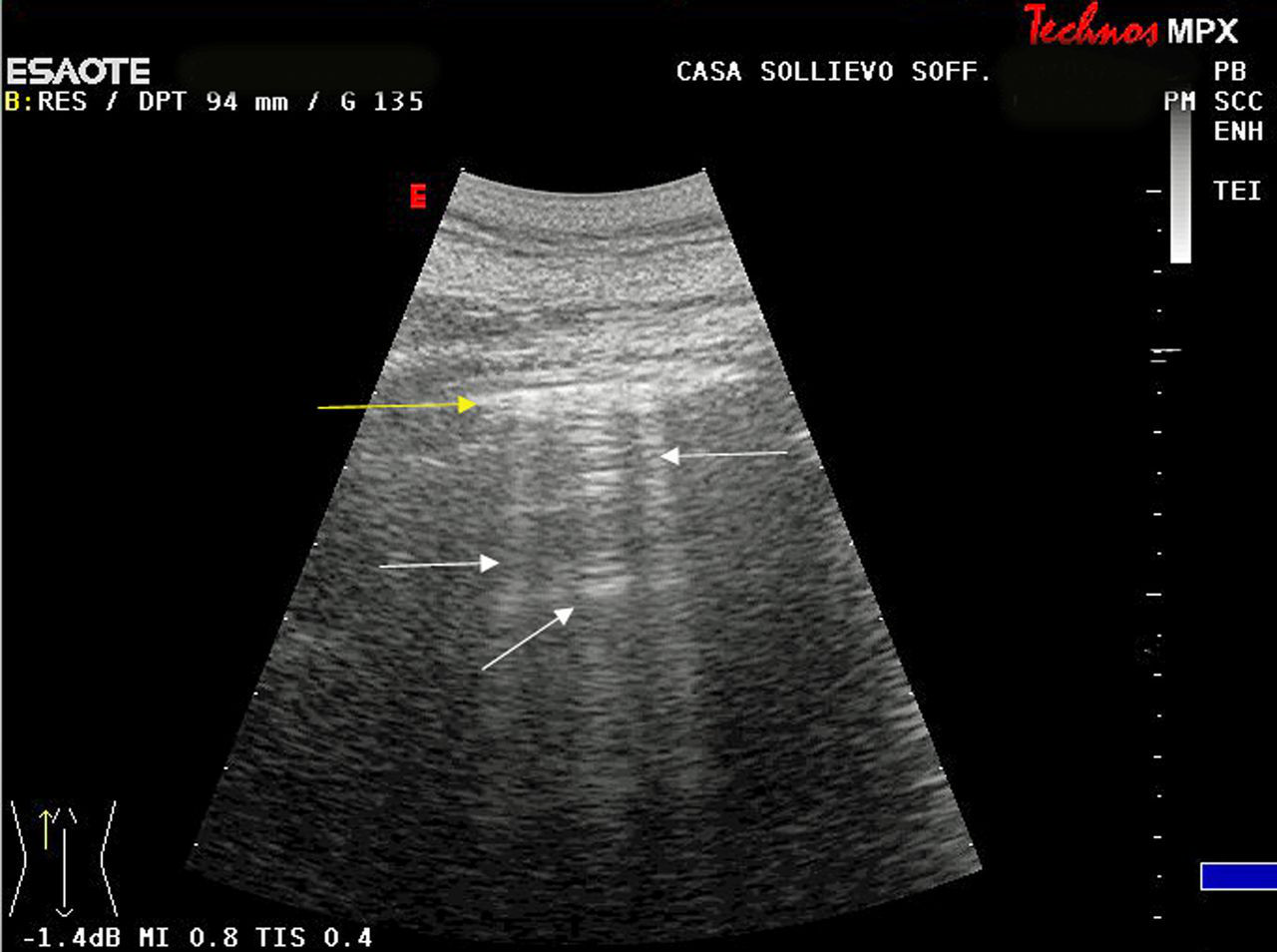
The B-lines were almost twice as numerous in the lungs of patients with dyspnea as in those of healthy subjects and in the chest cavities of patients who had undergone pneumonectomy (Tables 2 and 3). These findings are compatible with what we know about the physical behavior of ultrasound waves (27). Artifacts are commonly generated at interfaces between soft tissue and gas or between fluid and gas, zones characterized by substantial differences in acoustic impedance, which result in almost complete reflection of the incident beam (5). Interfaces of this type are likely to be more numerous in a number of pleuropulmonary diseases, including those considered in our study, because they are associated with increases in the fluid component of the lung or in the proportion of tissue that is fibrotic (Figs. 2–5). This mechanism would explain the increased number of B-lines observed in diseased lungs (5, 28). Furthermore, an increase in the number of these artifacts can also be detected in the abdomen and some authors maintain that these artifacts are generated when ultrasound waves cross intestinal areas where gas is mixed with fluid (28). This unequivocally confirms that these artifacts are generated by non-specific physical phenomena that are not indicative of any particular pulmonary disorder, and this conclusion is fully consistent with the absence of significant differences in the number of B-lines found in the eight subgroups of dyspnea patients we studied. On the basis of these findings, then, there does not appear to be any specific association between an increased number of B-lines and different types of diffuse pleuropulmonary disorders.
Parasternal transthoracic ultrasound scan (3.5 MHz convex probe) in patient with pulmonary edema reveal B-lines (“ring-down”) (white arrows) Parasternal transthoracic US scan with 3.5 MHz convex probe in patient with COPD exacerbation reveal B-lines (“ring down”) (white arrowhead) Parasternal transthoracic ultrasound scan with 3.5 MHz convex probe in patients with neoplastic lymphagitis reveal B-lines (“ring down”) (white arrowhead) Parasternal transthoracic ultrasound scan with 3.5 MHz convex probe in patients with pulmonary fibrosis reveal B-lines (“ring down”) (white arrows)



To our knowledge, only one other study (16) has looked at B-lines in the lungs of a large series of patients with different pulmonary disorders (250 consecutive patients with acute respiratory failure that was ultimately attributed to cardiogenic pulmonary edema, pneumonia, COPD, pulmonary embolism, asthma, or pneumothorax). It was found that the number of B-lines were useful in distinguishing between these conditions. The discrepancy between these findings and our own could perhaps be explained by the following considerations, many of which have not been addressed in previous reports. First of all, various methodological choices (e.g. the intercostal spaces and sitting position of the patient used for artifact counts, set-up equipment, frequency, type probe, time gain compensation setting, tissue harmonic and electronic focus [pleural line] used and the devices with less than 7 years of use) (29, 30) could influence the number and type of artifacts detected. Indeed, we used a greater number of acoustic windows, compared to previous studies. In particular, the intercostals latero-basal spaces considered in our study are physiologically wider and, consequently, allow us to detect a larger number of artifacts. Moreover, we studied the patients in the sitting position, compared to the supine position used by other studies (16). Indeed, a different decubitus could influence the intrapulmonary circulation and, therefore, the number of detected artifacts. At this regard, the possible clinical relevance of the location and of the pattern of distribution of the artifacts in the lung was not determined in the present study and requires further study.
It is also important to recall that transthoracic ultrasound is difficult to perform in acute settings. For example, in dyspneic patients with high respiratory rates, rapid movement of the pleural line can increase the perceived frequency of B-lines, and their number can easily be overestimated in these cases. Moreover, the accuracy and inter-operator reproducibility of any sonographic examination are highly dependent on the equipment used and the examiners' training, skill, and experience (28–30). A major strength of our study was that all of the scanners used were set up specifically for transthoracic examinations, and all the operators were adequately trained in pleuropulmonary ultrasound. It should also be stressed that the number of B-lines observed is inversely related to the spatial resolution of the image, which is determined by the frequency and duration of the ultrasound pulses transmitted (27). Higher frequencies are associated with higher resolution but also with limited penetration, whereas the use of low frequencies improves penetration but lowers resolution (30). For this reason, high frequencies are generally used for transthoracic studies of the pleural surface, and they are commonly associated with the generation of fewer artifacts. Low frequencies are employed to identify pleural effusions and subpleural lesions, and they are generally associated with the detection of a higher number of artifacts. In our study, patients were examined with a low-medium frequency convex probe (3.5–5 MHz) and also with a high-frequency linear probe (8–12.5 MHz) to explore the possibility that discrepancies reported in the literature regarding artifact numbers can be accounted for, at least in part, the use in different studies of probes with different frequencies. The number of B-lines detected with the convex and linear probes was significantly different in both the patients with dyspnea and the healthy controls, which confirms that this parameter is strongly dependent on the characteristics of the equipment used. The generation and perception of B-lines are also strongly conditioned by the time gain compensation setting, the ratio of probe curvature to the curvature of the lung surface, and whether or not movement artifact suppression and tissue harmonics are used.
In conclusion, our results reveal significant differences in the number of B-lines found during transthoracic ultrasound examinations of the lungs of patients with dyspnea and healthy subjects, and of the chest cavity in patients who have undergone pneumonectomy. However, this difference is common to several diffuse pleuropulmonary diseases. Consequently, in real-life clinical settings, the evaluation of B-lines offers no concrete benefits in terms of the differential diagnosis of dyspnea in diffuse pleuropulmonary diseases. Therefore, transthoracic ultrasound represents a potentially useful complementary tool in the study of pleuropulmonary diseases. Nevertheless, the quantification of B-lines alone does not make any significant contribution to the differential diagnosis or prognostic assessment of these diseases, especially in acute settings.
Footnotes
ACKNOWLEDGMENTS
The authors thank Marian E Kent for her contribution for the final draft of the manuscript.