
Abstract
In July 2004, British Association of Sexual Health and HIV (BASHH) published guidelines for post-exposure prophylaxis following sexual exposure (PEPSE) and the Terence Higgins Trust (THT) launched a campaign promoting PEPSE among men who have sex with men (MSM). We evaluated subsequent changes in PEPSE attendances. Individuals requesting PEPSE in 2004 were identified from clinic databases. Comparisons of clinical data, exposure characteristics and follow-up were made pre and post campaign. Data were available for 197/216 (91%) PEP attendances. The proportion requesting PEP following sexual exposure increased significantly following the campaign. The majority commencing PEPSE were MSM, with the proportion of MSM increasing significantly from 36/46 (78%) pre to 76/80 (95%) following the campaign. Most prescriptions were in high-risk groups and within guidelines. Times to initiation and completion rates were unchanged. Access to PEPSE following the THT campaign and introduction of BASHH guidelines increased. Promotion of earlier initiation of PEPSE and improvement of completion and follow-up is required.
Introduction
Demand for post-exposure prophylaxis (PEP) following sexual exposure to HIV (PEPSE) is increasing, although availability and awareness varies widely.1,2 Current UK guidelines 3 recommend a combination of three antiretroviral agents as soon as possible after an HIV exposure for 28 days, based on a case-control study of exposed health-care workers (HCW). 4 Delays in initiating PEP or shortening the course of PEP reduced efficacy in an animal model 5 and in a study of humans exposed sexually to HIV, the time to initiation of PEP was greater among seroconverters compared with non-seroconverters. 6 When compared with HCWs, individuals present later for PEPSE, with poor completion rates in both groups. 7
In July 2004, the British Association of Sexual Health and HIV (BASHH) published guidelines for PEPSE 8 and the Terence Higgins Trust (THT) launched a publicity campaign promoting PEPSE 9 among men who have sex with men (MSM), providing information to facilitate access. We evaluated the subsequent changes in PEPSE requests and provision on two services, the Mortimer Market Centre (MMC), London and the Claude Nicol Centre, Brighton.
Methods
Individuals requesting PEPSE in 2004 were identified from clinic databases. Comparisons of clinical data, exposure characteristics, follow-up and awareness of PEPSE were made between the pre and post-campaign periods. Analysis was performed using STATA 9 (STATA Corp, College Station, TX, USA).
Results
We identified 216 individuals who requested PEP in 2004; 165 MMC and 51 Brighton. Data were available for 197/216 (91%). The proportion requesting PEPSE increased significantly following the campaign from 49/80 (61%) to 90/117 (77%), P = 0.025. The majority of those 139 following sexual exposure commenced PEP, 46/49 (94%) before and 80/90 (89%) after the campaign. Exposure characteristics were considered low risk in the majority of those 58/197 (29%) individuals not commencing PEP (as defined by medical staff and BASHH guidelines). Of these, 12/29 (41%) were MSM prior to the campaign and 14/29 (48%) following the campaign.
The majority commencing PEPSE were MSM (112/126), with the proportion of MSM increasing significantly from 36/46 (78%) pre to 76/80 (95%) following the campaign, P = 0.007. As the campaign targeted MSM, subsequent analysis is restricted to this group of 112, subject to missing data across items.
Of MSM presenting after July for which data were available on the source of their awareness of PEPSE, 17/63 (27%) cited the THT campaign. Comparing those citing the THT campaign and those who did not, there was no significant difference in the median time to initiation of PEP, 22 h (range 12–64), compared with 31 h (range 6–76), P = 0.81 (Mann-Whitney test). Completion rates for PEPSE in both groups were similar, 7/8 (88%) and 28/31 (90%) respectively, P = 1.00, Fisher's exact test. The proportion having a follow-up HIV test among individuals citing and not citing the campaign were similar: 9/17 (53%) and 16/43 (37%), respectively, P = 0.38, Fisher's exact test.
Overall, MSM reported similar numbers of sexual partners in the preceding three months and similar exposure characteristics pre and post campaign (Table 1). Comparing MSM taking PEPSE before and after the campaign there was little change in the median time to initiation of PEPSE (21.5 and 23 h, respectively) or the proportions commencing PEPSE via Accident and Emergency (17% and 24%, respectively, P = 0.62). Completion rates of PEPSE among MSM were similar pre and post campaign; 56% and 60%, respectively. Among individuals completing four-weeks of PEPSE, 100% adherence was reported by 72% pre and 85% post campaign. Follow-up testing for HIV at three and/or six months was poor (<50%) in both groups.
A comparison of MSM commencing PEPSE before and after the THT campaign
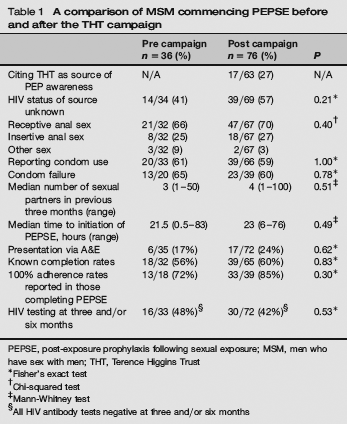
PEPSE, post-exposure prophylaxis following sexual exposure; MSM, men who have sex with men; THT, Terence Higgins Trust
Fisher's exact test
Chi-squared test
Mann-Whitney test
All HIV antibody tests negative at three and/or six months
Discussion
Our data suggest an increase in access to PEPSE following the THT media campaign and introduction of BASHH guidelines. Nearly 1/3 of MSM attending following the campaign cited it as the source of their awareness of PEPSE. However, this may be an underestimation, as a good campaign will ‘get people talking’ and those who do not cite the campaign may still have been indirectly influenced by it.
The apparent changes seen following the campaign and introduction of guidelines may be coincidental. We may have underestimated the number of individuals influenced by the THT campaign as data regarding the source of knowledge of PEPSE was not always recorded. Other limitations include the potential underestimation of numbers requesting but not commencing PEPSE due to clinic coding procedures and that not all data were available for a proportion of individuals.
The majority of prescriptions for PEPSE were in high-risk groups and within BASHH guidelines. Increased attendance to request PEPSE is an opportunity to offer testing for sexually transmitted infections and behavioural interventions, even if PEPSE is not dispensed.
Given that time to initiation and completion of therapy may influence efficacy of PEPSE, it is disappointing that we found no improvement following the THT campaign, despite promotional literature advising this. Particular focus to promote earlier initiation of PEPSE including 24-hour access and providing support to improve completion and follow-up is required.
Ethical approval
This is a retrospective case note review for which ethical approval was not required.