
Abstract
We aimed to investigate whether patients with genital warts experience greater feelings of shame and lower self-esteem compared with controls. Sixty patients with genital warts were compared with 60 asymptomatic genitourinary (GU) medicine patients and 60 orthopaedic outpatients. The shame scores of those with warts (31.08) were significantly higher (P < 0.0001) than either control group (GU medicine controls 20.77; orthopaedic controls 19.00). The impact on health-related quality of life (HRQoL) by each of the individual emotional parameters of shame, low self-esteem, intrusive thoughts, avoidance behaviour and self-efficacy impact was examined in the wart sample group. Only internalized shame (P = 0.001) and intrusive thoughts (P < 0.0001) were significant in predicting HRQoL scores. There are emotional implications in having genital warts, which can have a profound effect on a patient's quality of life and these need addressing just as much as the physical warts.
INTRODUCTION
Genital warts are the most common viral sexually transmitted infection (STI) diagnosed at genitourinary (GU) medicine clinics. In 2007, 89,838 new cases of genital warts were diagnosed in the UK. 1 There have been relatively few studies that have examined the impact of genital warts on an individual's quality of life and emotional wellbeing. 2–7 The most recent study found that the quality of life of those with genital warts was significantly worse than population norms. 8
Several key emotions have been identified in people who have genital warts. These are anger, disgust, shame, embarrassment, depression, anxiety, worry and a feeling of being less desirable. 2–6 Very few studies have focused on individual emotions to discover their relative importance and impact on a patient's quality of life. One study, which focused on shame and stigma with warts, asked women to predict how they thought they would feel if they did develop genital warts. This demonstrated that awareness of the sexually transmitted nature of genital warts brought with it greater feelings of shame and stigma, and that a knowledge of the high prevalence of the infection reduced these feelings. 9
The initial aim of this study was to confirm whether patients with genital warts do experience feelings of shame and lower self-esteem. The study then examined the impact on quality of life produced by each of the individual parameters of shame, low self-esteem, intrusive thoughts, avoidance behaviour and low self-efficacy.
METHODS
Patients with a diagnosis of new or recurrent genital warts were recruited from the GU Medicine Department at Derriford Hospital in Plymouth. Those who consented were given five questionnaires to complete in an interview with the researcher; a demographic questionnaire, the internalized shame scale, the impact of events revised scale, the general perceived self-efficacy scale and the health-related quality of life (HRQoL) in AnoGenital Warts scale.
A control group of asymptomatic patients from the GU medicine clinic was recruited for the study. Those who consented were given the demographic questionnaire and the internalized shame scale.
A second control group of orthopaedic patients was recruited from the Orthopaedic Outpatients' Department of Derriford Hospital. Patients who consented completed the same two questionnaires; the demographic questionnaire and the internalized shame scale.
The demographic questionnaire asked about age, gender, nationality, relationship status and educational attainment.
The internalized shame scale 10 is a Likert scale (0–4). It has two subscales: an internalized shame subscale consisting of 24 items, which gives a shame score range of 0–96 (higher scores indicate more shame) and a self-esteem subscale, which gives a self-esteem score range of 0–24 (lower scores indicate lower self-esteem).
The Impact of Events Revised (IER) scale 11 measures current subjective distress related to a specific event to estimate the degree to which intrusive thoughts and avoidance behaviours are present. The IER scale consists of 15 items and has two subscales: intrusive thoughts and avoidance behaviour. Respondents are asked to rate the items on a four-point scale, giving a range of 7–28 for the level of intrusive thoughts and 8–35 for the level of avoidance behaviour (higher scores indicate a higher degree of distress).
The general perceived self-efficacy scale 12 aims to discover whether a person has a firm sense of one's own coping abilities when confronted with a variety of difficult and stressful situations. The scale has 10 items that are rated on a four-point scale, giving a range of 10–40 (lower scores indicate less self-efficacy).
The HRQoL in AnoGenital Warts questionnaire 13 was specifically formulated to address quality of life in patients with genital warts. The scale has 22 items and assesses emotional and sexual quality of life. Patients are asked to respond on a Likert scale (1–5) giving a range of 22–110 (higher scores signify worse HRQoL).
Statistical advice was sought regarding sample size. The data were analysed in Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL, USA). The assumptions and casewise diagnostics pertaining to multivariate analysis were examined. Due to non-normality, the variable shame was subjected to a square root transformation. Descriptive statistics were used to describe the demographic details of the sample. A one-way, between-subject analysis of variance (ANOVA) was used to compare internalized shame scores across the three groups. Correlations were carried out to determine whether any of the demographic variables were associated with HRQoL scores in the wart group. Hierarchical multiple regression was used to establish the extent to which internalized shame, self-esteem, intrusive thoughts, avoidance behaviour and self-efficacy scores predicted HRQoL for patients with genital warts. One outlier was detected during the exploration of diagnostics and subsequently removed for regression analyses. Statistical significance was considered when a P value was 0.05 or less.
RESULTS
Table 1 shows the demographics of the three groups; the wart sample group and the two control groups. All groups were Caucasian and had similar gender ratios. However, age, relationship status and educational attainment showed significant differences. The mean ages of those with warts (25.58 years) and the asymptomatic controls (24.63 years) were significantly lower (P < 0.0001) than the mean age of those in the orthopaedic control group (37.72 years). The categories of relationship status and education attainment were dichotomized into married/not married and degree level/below degree level, respectively. More participants in the orthopaedic control group were married than those in the two GUM groups (P < 0.0001). More participants had reached degree level in both control groups than in the wart group (P = 0.004).
Demographics of the wart sample group and control groups
GU medicine = genitourinary medicine
Figure 1 shows a scatter graph of the duration of infection for each patient in the wart sample group. The mean duration of infection was 12.46 months, the mode was less than one month and the range was 0.25–204 months. There was no association between duration of wart virus infection and HRQoL.
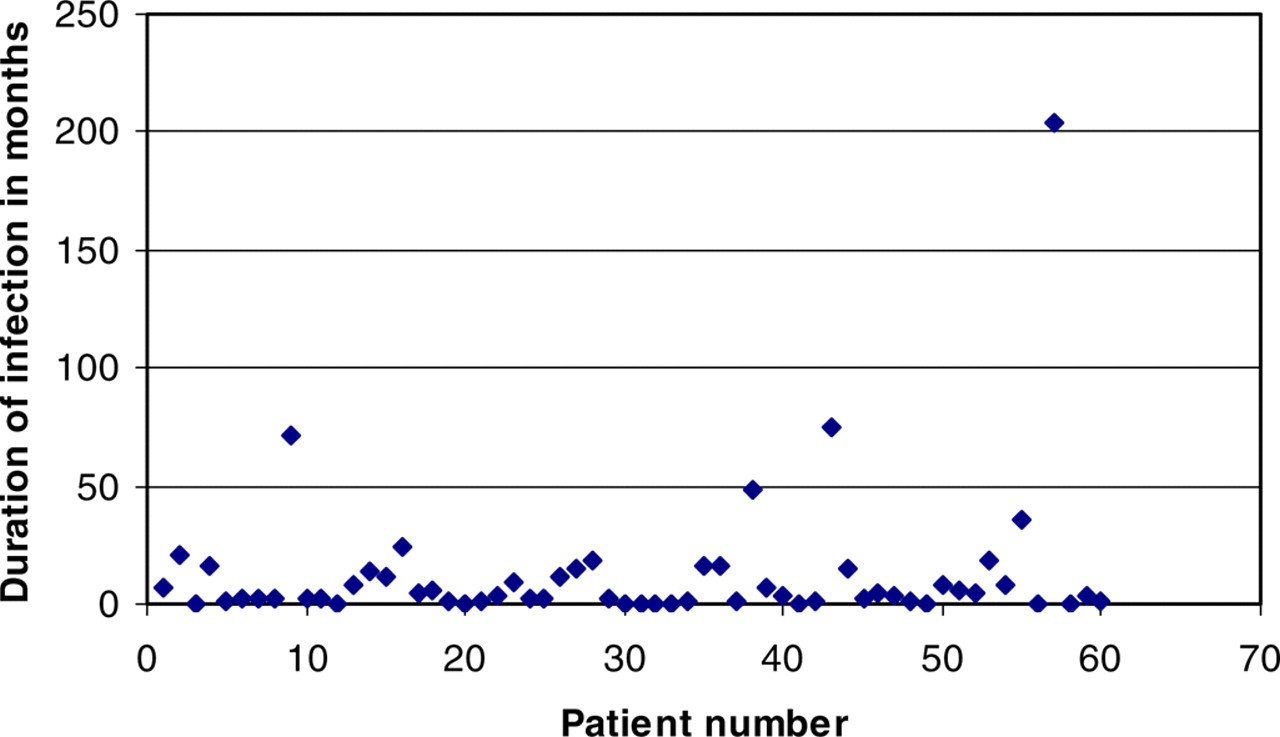
Scatter graph showing the duration of wart virus infection for each patient in the wart sample group
Figure 2 shows the mean shame scores and shame ranges for the three groups. An ANOVA demonstrated that the shame scores of those with warts were significantly higher than either control group (P < 0.0001). There was no significant difference between the two control groups.

Mean internalized shame scores and shame score ranges for each of the three groups: the wart sample group and the two control groups
All emotional scores for the three groups are shown in Table 2. None of the correlations between the demographic variables and HRQoL scores in the wart sample group were significant.
Emotional scores for the wart sample group and control groups
HRQoL= health-related quality of life
Regression analysis was used to determine which of the emotional parameters/personality variables contributed to the patient's HRQoL. Using casewise diagnostics one outlier was detected and removed from the analysis. The hierarchical multiple regression is shown in Table 3.
Hierarchical multiple regression for health-related quality of life (HRQoL)
Model 1
Internalized shame scores and self-esteem scores were entered into model 1. This showed that internalized shame alone explained a significant proportion of the variance in HRQoL (P < 0.0001). It explained approximately 50% (adjusted R 2 = 0.53) of the variance. Self-esteem did not contribute to the model.
Model 2
Intrusive thoughts and avoidance behaviour scores were entered into model 2. After controlling for the variables in model 1, model 2 significantly improved the prediction of HRQoL (P < 0.0001). The overall model 2 explained approximately 70% (adjusted R 2 = 0.69) of the variance. In this model, internalized shame (P = 0.001) and intrusive thoughts (P < 0.0001) had a significant contribution to predicting HRQoL. Self-esteem and avoidance behaviour did not influence HRQoL.
Model 3
Self-efficacy scores were entered into model 3. Having controlled for the variables; shame, self-esteem, intrusive thoughts and avoidance behaviour, model 3 did not significantly improve predictions of HRQoL. Therefore, of all the individual emotional parameters, only internalized shame and intrusive thoughts had a significant contribution to predicting HRQoL in patients with genital warts.
DISCUSSION
Our results supported the hypothesis that patients with genital warts do indeed feel more shame and that this is due to the infection itself rather than attending a GU medicine clinic. The outcome of this study joins a growing body of evidence, which suggests that infection with genital warts not only has an effect on the patient's physical wellbeing but also a potentially damaging effect on the patient's emotions. 2–6,9 Our results were consistent with previous findings that genital wart infection is associated with a negative effect on HRQoL. 7,8 Higher feelings of shame and high levels of intrusive thoughts contributed to this detrimental effect.
The implications of feeling ashamed and enduring intrusive thoughts can be profound. Fortenberry 14 found that adolescents who are experiencing stigma and shame related to having an STI delay in seeking treatment and shame has been linked to other psychological problems such as low self-esteem and depression. 15 This may be exacerbated if the patient hides their diagnosis from others as they may not receive the social support they need in coming to terms with the infection and its impact on their life.
Intrusive thoughts are involuntary and appear without warning. Often the patient has no idea when or where these thoughts will intrude into their daily life and as such, they may feel as if they have no control over the way they think and feel. Ireland et al. 6 found that illnesses that are perceived as being out of the patient's control tend to produce feelings of depression and anxiety.
Medical professionals should be aware that many patients do feel embarrassed and ashamed. If the patient is confused or distressed about their diagnosis, an opportunity to discuss their diagnosis with a health adviser may be helpful. Providing further information may help deliver control of the illness back into the patient's hands, which may in turn result in a reduction in the frequency of intrusive thoughts. It may be helpful to educate the patient regarding the high prevalence of the condition. Waller et al. 9 found that informing university students about the common occurrence of genital warts reduced feelings of shame and stigma. One possible reason for this is that it reduced feelings of isolation and helped to ‘normalize’ the condition.
However, it is important to acknowledge that certain factors, which were not examined in this study, may have an effect on the shame and stigma experienced. Further research might focus on discovering the underlying cause of the greater feelings of shame and the higher volume of intrusive thoughts. While filling out the questionnaires, one patient with warts stated ‘I'm quite a laid back person, so this wouldn't really affect me anyway’. It is likely that personality characteristics such as a tendency toward anxiety or neuroticism would be important factors in determining the extent of the negative emotional impact on HRQoL.
At present many medical professionals still work within the biomedical model, focusing solely on the physical wellbeing of the patient. 16 But, it is clear that there are emotional implications in having genital warts, which can have a profound effect on a patient's quality of life and these need addressing as much as the physical warts.
Footnotes
ACKNOWLEDGEMENT
Ethical approval for the study was given by the Plymouth and Cornwall Local Research Ethics Committee.