
Abstract
A survey of HIV testing practices among registrars of all admitting specialties within Sheffield Teaching Hospitals National Health Service Trust was performed in 2007. Respondents from most specialties tested patients for HIV infrequently and several barriers were identified, which prevented testing even when the diagnosis was considered.
BACKGROUND
There are an estimated 25,000 people with undiagnosed HIV infection in the UK. 1
Failure to diagnose HIV early places these individuals at risk of preventable morbidity and mortality from opportunistic infections and may attenuate their immunological response to antiretroviral therapy (ART). Ignorance of HIV status also contributes to a large proportion of onward transmissions. 2 Encouraging testing by specialties not usually involved in the care of HIV-infected patients is critical in the battle to reduce undiagnosed cases, a fact recognized in guidelines worldwide, 3 including the recently published UK National Guidelines for HIV Testing. 4
METHODS
In June 2007, we conducted a postal questionnaire-based survey of HIV testing practices of 281 registrars employed within Sheffield, where HIV seroprevalence is estimated at 1:1000. Paediatric and anaesthetic registrars were excluded and respondents had the option of remaining anonymous.
Respondents were asked to estimate the number of patients in whom they had considered and performed HIV testing over the preceding six months. Reasons for not testing patients in whom the diagnosis had been considered were explored and respondents were asked to rate their confidence in providing pretest counselling.
RESULTS
Of 124 (44%) registrars completing the questionnaire, 66% had considered and 51% had performed at least one HIV test over the preceding six months. Only 10% had performed more than five tests, a group consisting mainly of communicable diseases and obstetrics and gynaecology trainees. Medical registrars were significantly more likely to have performed a test than those training in surgical specialties (Figure 1) despite seeing similar numbers of patients from high-risk groups. None of the eight Accident and Emergency (A&E) respondents had performed a test.
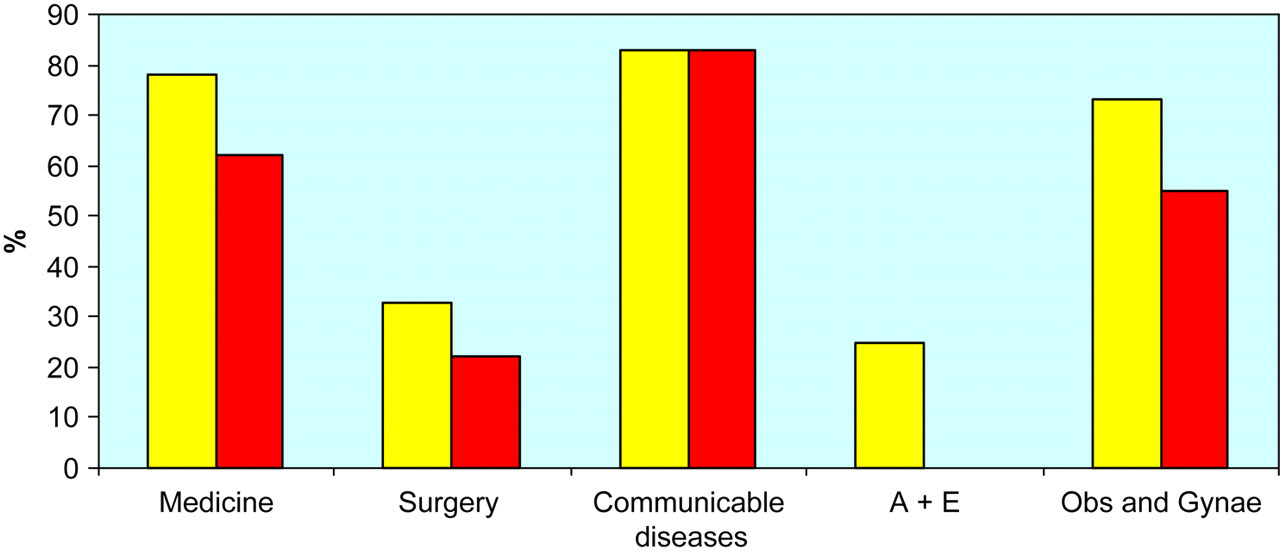
Percentage of respondents from individual specialty groups who had considered (light) and performed (dark) at least one HIV test over the preceding six months period. Medical registrars were significantly more likely to have performed a test than those training in surgical specialties (P < 0.001 consider, P < 0.01 perform)
Those registrars who qualified after 2000 were significantly more likely to have considered and performed at least one HIV test than those graduating prior to 1998 (Figure 2).
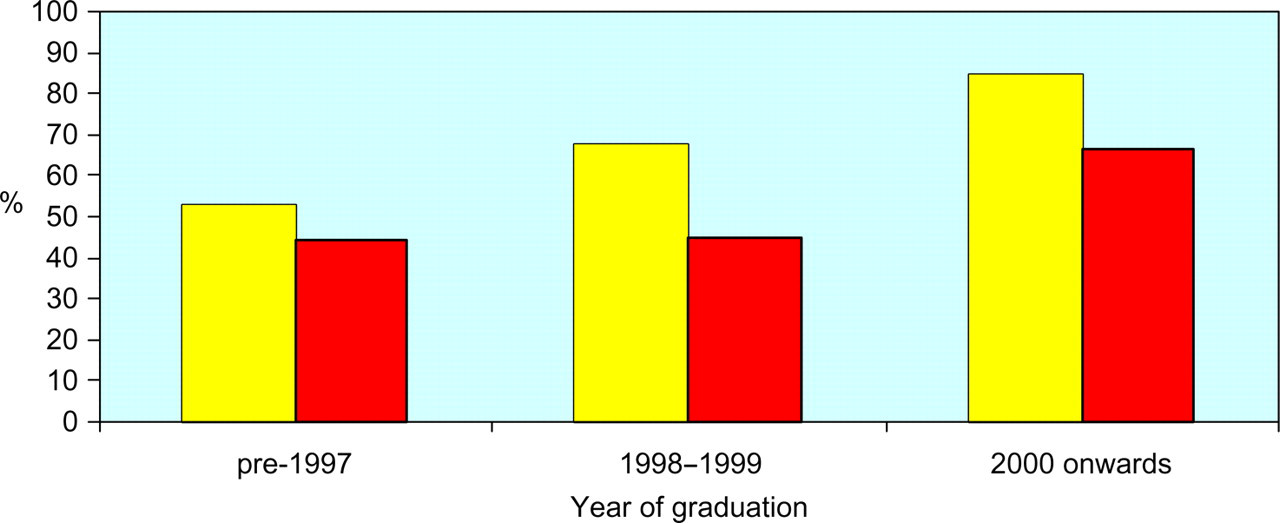
Relationship between year of graduation and percentage of respondents considering (light) and performing (dark) at least one HIV test over the preceding six months period. Those who qualified after 2000 were significantly more likely to have considered (85% versus 50%, P < 0.01) and performed (67% versus 42%, P = 0.03) a HIV test than those graduating prior to 1998. This difference persisted when communicable diseases and obstetric trainees were excluded
Forty-nine (40%) respondents reported not performing a HIV test on a patient whom they had considered testing and, in 29% of these cases, uncertainty about counselling the patient was recorded as a contributory factor. Registrars who felt confident to counsel alone or after verbal advice only were significantly more likely to have performed an HIV test than those who felt they would require the presence of someone with experience (63% versus 33%, P < 0.005).
Other reasons cited for considering but not performing a HIV test included: belief that local policy or General Medical Council guidance discouraged respondents from testing; concern about distressing patients and harming the doctor–patient relationship; lack of suitable location for counselling and anxiety on the part of the doctor about how to manage a positive result.
DISCUSSION
Only half of registrars responding to this survey had performed a HIV test over the preceding six months. Patients may fail to be HIV tested because the diagnosis is not considered or because systemic or personal barriers prevent a test from being performed. In this survey, a third of respondents had not considered testing any patients but a further 40% had not performed a test in a patient despite considering the possibility of HIV infection.
Organizational barriers to testing must be addressed to minimize missed opportunities for diagnosis. In this survey, a perception that testing was discouraged by certain departments, a lack of suitable environments for counselling, and inadequate systems for providing results and post-test counselling for patients discharged from A&E were highlighted. Lack of testing in A&E is of particular concern as some of the patient groups in whom HIV is most prevalent, especially new immigrants and intravenous drug users, are also those least likely to be engaged with primary care services and instead to visit A&E or walk-in centres with any medical problems. It is particularly important that opportunities to discuss HIV testing with these patients are not missed and testing practices within these areas should draw particular attention. 5
Education of staff is vital to ensure that HIV is considered in relevant patients and to overcome personal barriers including anxiety over patient counselling. It is noteworthy that doctors training more recently were more likely to feel confident in counselling and to have tested patients. This may relate to improvements in the undergraduate curriculum or be a function of these registrars having trained in an era of effective ART.
The publication of guidelines rarely results in an instant paradigm shift in behaviour, especially where their implications fall upon a broad range of specialties. Instead, they encourage a more gradual evolution of individual practice over time. For the new HIV testing guidelines to have their desired effect, trusts need to address the institutional and personal barriers to HIV testing identified by this survey.