
Abstract
Objectives
Peripheral lymphocoele is a recognized complication after various forms of surgery. This is a case report of a calf lymphocoele after surgery for varicose veins by ambulatory phlebectomy.
Method
The reported incidence, pathology and possible treatment methods are discussed.
Conclusion
Phlebectomy practitioners need to be aware of the possibility of this complication.
Case report
Mr HS, aged 65, presented with a 10-year history of symptomatic bilateral varicose veins. His main concerns were their appearance and the likelihood of complications. There was a past history of a tri-malleolar fracture of the right ankle at the age of 28, which had left him with a swollen ankle and limited range of motion.
Examination revealed bilateral varicose veins in the zone of the great saphenous veins (GSV). There was bilateral pitting oedema at the lower shin area. The right ankle showed chronic synovitis and a reduced range of movements.
Investigation by duplex ultrasound scanning showed bilateral GSV reflux. On the right, there was GSV reflux from the saphenofemoral junction to the upper thigh extending into a large superficial tributary which extended to below knee. On the left, GSV reflux extended from the saphenofemoral junction to below knee.
Treatment of the right GSV was by endovenous laser therapy using the Diomed* 810 nm diode laser (Andover, Massachusetts, USA). The superficial tributary was surgically ligated at the epi-fascial escape point. Microblade ambulatory phlebectomy was used to remove superficial varices in the thigh and calf using a BD beaver blade (Ref 376500) and Mueller phlebectomy hooks (Ref DV15000R) numbers 1 and 2. A four-layer bandage was applied for 48 hours, then 30–40 mmHg compression open toe thigh stockings were worn for two weeks. There were two later sessions of ultrasound-guided foam sclerotherapy for smaller residual varices.
Review at three weeks showed an asymptomatic, firm ‘golf ball’ like swelling in the right upper medial calf (Figure 1) and a provisional diagnosis of postsurgical lymphocoele was made. Initial treatment was 30–40 mmHg calf compression stockings. The cyst (Figure 2) was clinically unchanged after two months; it was aspirated on three occasions with continuing compression. Again, the cyst remained unchanged and 3% sodium tetradecyl sulphate was instilled on two occasions after aspiration. The lymphocoele remained unchanged at 18 months and surgical removal was undertaken (Figures 3 and 4).

Asymptomatic swelling in the right upper medial calf at three weeks after phlebectomy
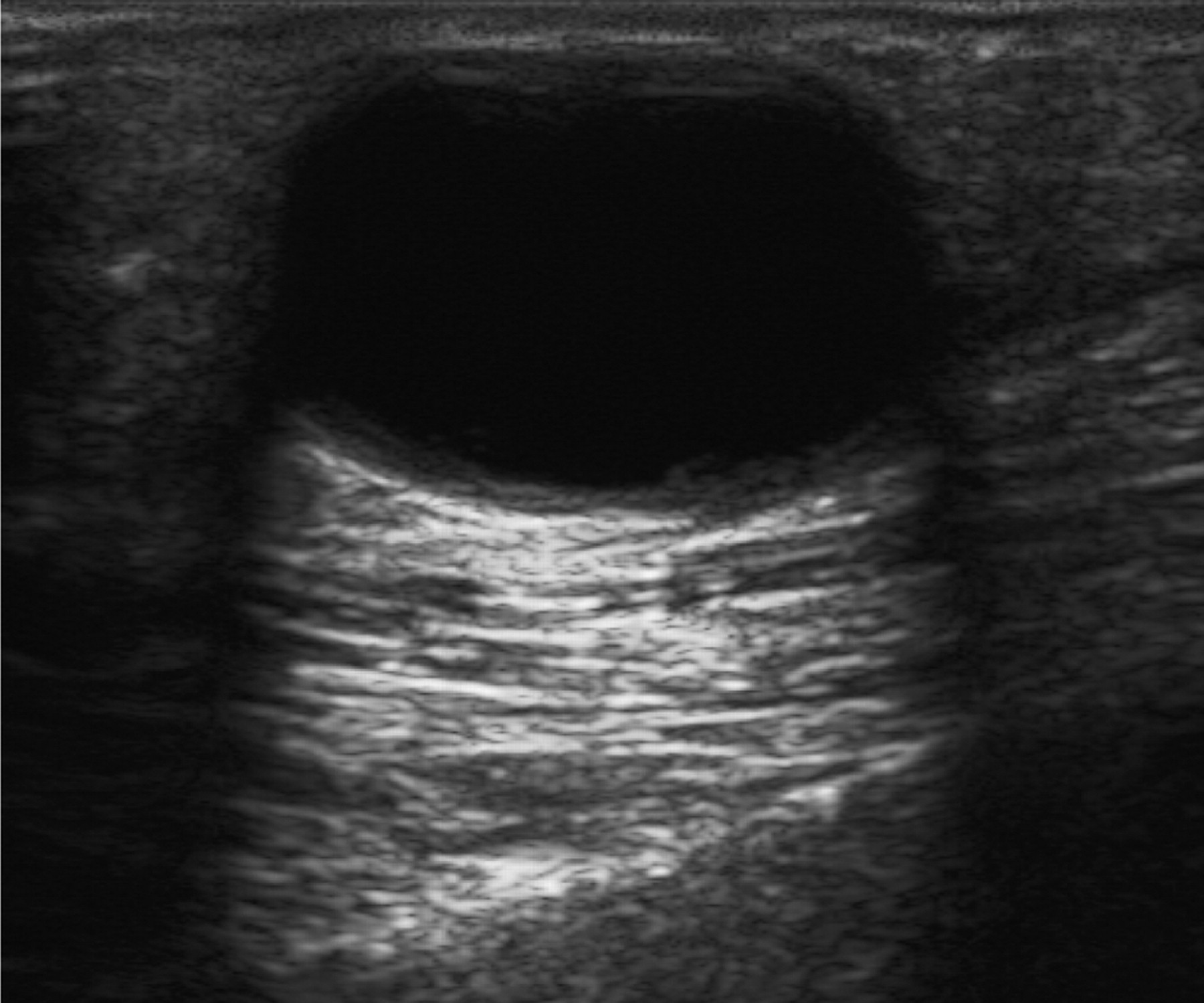
Lymphocoele. A B-mode ultrasound image showing the three criteria for classifying this lesion as a cyst 9 – acoustic enhancement, internally echo-free and a smooth wall
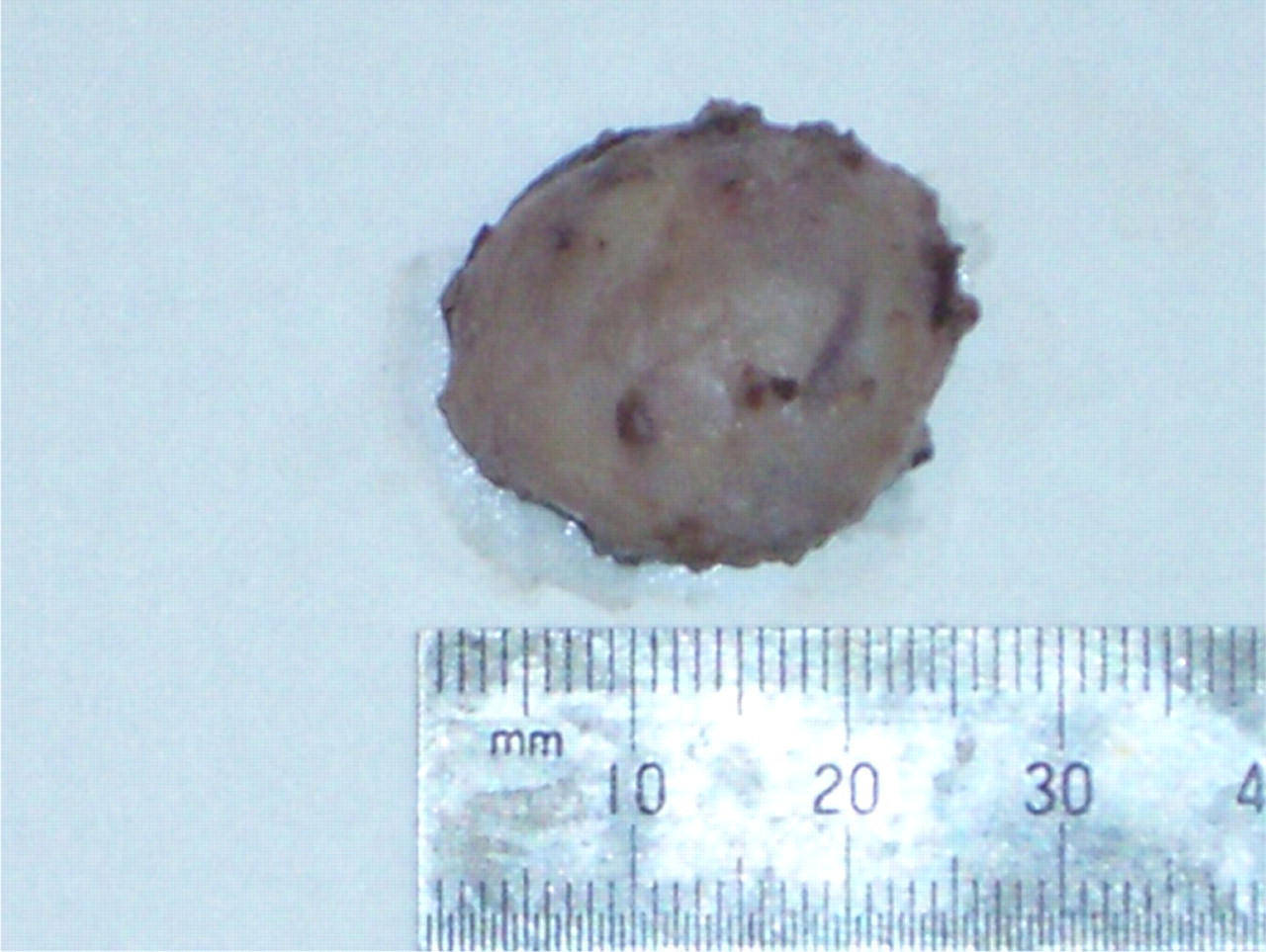
Excised lymphocoele
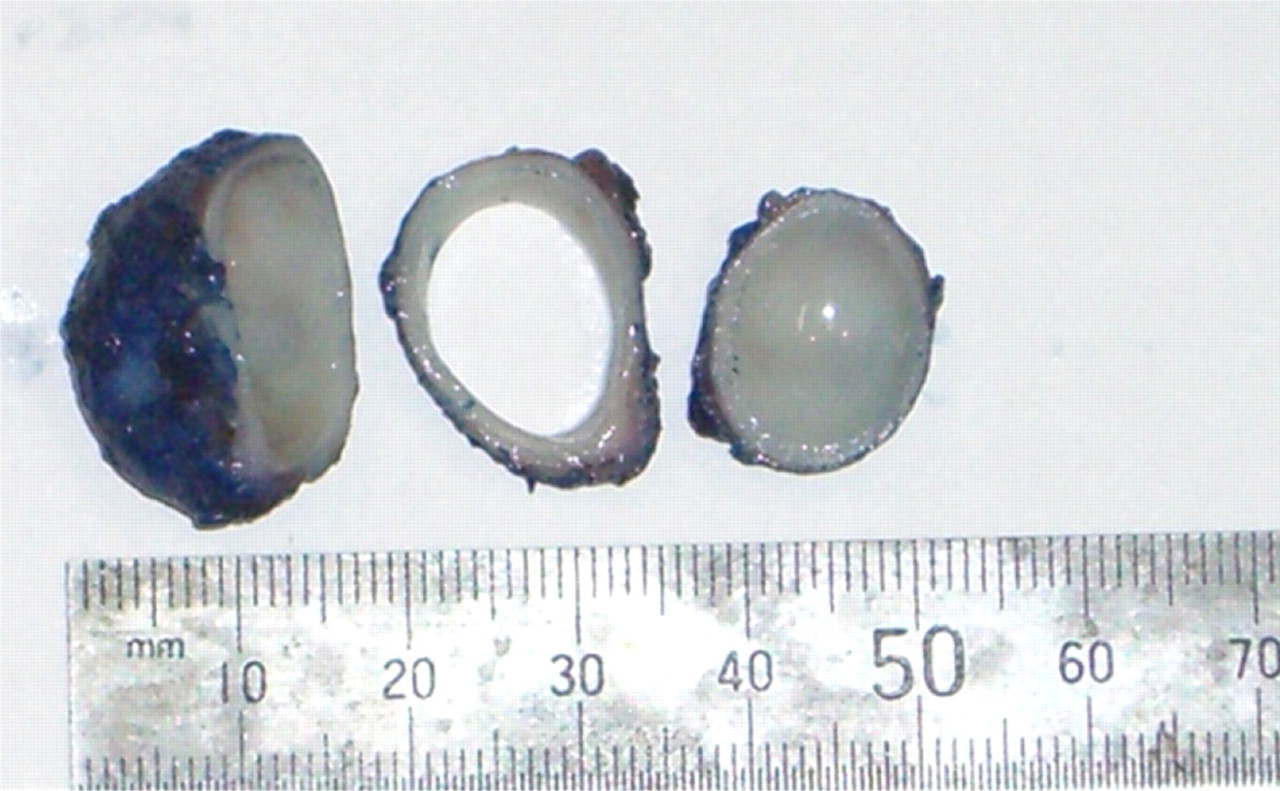
Macroscopic pathology showed a thin-walled cyst up to 25 mm diameter and the cut section revealed clear fluid inside. Microscopic histopathology showed that it was lined by a dense network of fibrin associated with a mild lymphocytic infiltrate. No endothelial lining was apparent. Concentric rings of fibrous tissue were present at the periphery of the cyst lining
Discussion
A lymphocoele is a lymph-filled space without a distinct endothelial lining. It is frequently seen following surgery where large amounts of lymphatic tissue are transected. Once injured, a lymphatic vessel is quite susceptible to continued leakage. Lymph contains a low concentration of clotting factors and has no platelets.
The incidence after ambulatory phlebectomy is uncertain. Sadick 1 quotes a 4% incidence in 50 patients. Ricci and Georgiev 2 reported a 1.6% incidence in 320 patients. Dr Robert Muller, regarded as the father of modern day ambulatory phlebectomy, 3 recorded a 1.8% incidence in 1000 patients treated between 1965 and 1975. 4 Olivencia et al. 5 reported a zero rate in 1000 cases of ambulatory phlebectomy. They are probably more common than reported as many are small, asymptomatic and mistaken for a slowly resolving haematoma.
The diagnosis of lymphocoele is straightforward once the possibility has been considered. A computed tomography scan or an ultrasound examination of the lesion will confirm the presence and location of cystic fluid collection; internal echoes and septations may be present. 6
There is little information in the literature regarding the best treatment for a small peripheral lymphocoele following ambulatory phlebectomy. In contrast, a medline search revealed multiple case reports on the treatment of large proximal lymphocoeles following arterial, abdominal and renal transplant surgery by surgery, drainage and sclerotherapy. 7
Ricci and Georgiev suggest that lymphocoeles can sometimes be broken down by digital pressure or can be aspirated with local pressure applied until the lesion disappears. The anterior lateral tibial area is the most prone to develop lymphatic disruption as the lymph vessels are very superficial in this region. 8 Ramelet stated that ‘lymphatic pseudocyst may complicate phlebectomy of the ankle, pretibial, or popliteal areas. 9 The lymph collection may be punctured and drained. The best treatment is compression in addition to gentle circular massage and, in resistant cases, to manual lymphatic drainage. Excision is rarely indicated’.
Conclusion
Although chronic peripheral lymphocoele appears to be uncommon, it is likely that most phlebectomy practitioners will occasionally come across the condition. As there is no report of late complications in these lesions, small relatively asymptomatic lymphocoeles can be left untreated.
Peripheral lymphocoeles that cause cosmetic concern or are symptomatic should be treated. Options include compression, aspiration, sclerotherapy and excision. If there is concern that surgical excision could cause further lymphatic damage, it may be reasonable to open the cyst and ‘marsupialize’ the lymphocoele, packing the cavity to allow healing by secondary intention.