
Abstract
Objectives
Short saphenous vein (SSV) surgery carries a high risk of failure to identify the saphenopopliteal junction (SPJ). We assessed the impact of surgical expertise on anatomical outcome from SSV surgery and the role of preoperative duplex SPJ marking in improving outcome for vascular and non-vascular specialists.
Methods
A retrospective analysis identified patients (30 limbs) who had undergone SSV surgery. These were recalled for duplex scanning of the SPJ. In a prospective study, 187 limbs had preoperative duplex marking of SPJ and postoperative duplex to assess outcome. Grade of operating surgeon was recorded in both retrospective and prospective analysis.
Results
In both retrospective and prospective analysis, vascular specialists were significantly more likely than non-vascular specialists to correctly identify the SPJ (P < 0.0001). Preoperative SPJ marking did not improve outcome for the vascular specialist or the non-vascular specialist.
Conclusion
Preoperative SPJ marking is no substitute for surgical expertise. Competence in SSV surgery should be assessed prior to surgeons proceeding to independent practice.
Introduction
Short saphenous vein (SSV) operations are thought to carry a high risk of recurrence with one of the main causes being the failure to correctly identify the saphenopopliteal junction (SPJ). 1,2 Studies report a recurrence rate due to inaccurate surgery at 22–27%. 3–5 Difficulty in identifying the SPJ arises because of the variable anatomy in this region. 6–8 It has been suggested that preoperative determination of the anatomy and marking of the SPJ may improve surgical outcome; however, a study on 37 patients did not detect a significant reduction in inadequate surgery. 4
Accurate identification of the SPJ at operation may be influenced by the level of experience of the operating surgeon or subspecialty training. The aim of this study was to retrospectively determine the anatomical outcome from SSV surgery in our unit and to assess the effect of surgical expertise. We further aimed to prospectively investigate whether outcome could be improved through the use of preoperative duplex scanning for operations performed by vascular specialists or non-vascular specialists.
Methods
Retrospective analysis
Before 2004, all patients due to undergo varicose vein surgery in our unit had routine diagnostic duplex scanning. Duplex scanning was performed by an experienced vascular technician using a GE LOGIQ P5 scanner with a 9 MHz linear probe. Incompetence of the SPJ was defined as retrograde flow for more than one second following calf compression. If the SSV reflux was present, the level of the SPJ was recorded by measuring its distance from the heel and this measurement was recorded in the scan report and used as an anatomical guide at the time of surgery. Surgery for SPJ incompetence was performed in the prone position and involved dissecting down to the SSV to formally identify and ligate the SPJ. A minimum of 10 cm of SSV was resected or stripping as part of the surgical protocol.
Surgical notes were reviewed for patients who had undergone SPJ ligation between the years 2001 and 2003. Data collected included the date of surgery, type of surgery and grade of operating surgeon. Patients who had had such surgery were contacted by phone and letter and invited for a review outpatient consultation with duplex scanning in the clinic. At follow-up duplex, the absence or presence of an SPJ was recorded, as was reflux in residual SSV segments. To assess the effect of surgical expertise, the anatomical outcome was compared between limbs operated on by vascular specialists (consultant vascular surgeon or associate vascular specialist) and non-vascular specialists using the Fisher's exact test. Surgical outcome was recorded as ‘failed’ if there was an intact incompetent SPJ or residual reflux in the SSV. Outcome was recorded as ‘successful’ if no SPJ could be identified and there was no reflux in any residual SSV.
Prospective study
In January 2004, following analysis of the retrospective data, the policy for SPJ surgery was changed. Diagnostic duplex scanning and surgical technique remain unchanged but, wherever possible, any SSV surgery was carried out in the presence of a vascular specialist either of consultant or associate specialist grade. Furthermore, the position of the SPJ and the level of the fascial perforation of the SSV were marked on the skin on the day of operation in all cases. Any specific anatomical variances were also noted. Following surgery, all patients were invited to attend for out-patient follow-up with duplex scanning and the results were entered into a database. Fisher's exact test was used to test for differences between groups. To assess the effect of the new preoperative marking policy, rates of success were compared for procedures grouped by specialist input before and after policy change. To assess the effect of vascular expertise, the surgical success rates for vascular and non-vascular specialists were compared.
Results
In the retrospective review, 35 patients were identified of which 28 (16 male and 12 female) with 30 operated limbs agreed to attend for review. The follow-up duplex scan showed an intact SPJ in seven out of 30 limbs (23%) and one patient had continued superficial vein reflux via an incompetent perforator. In 22 limbs the SPJ had been successfully ligated (Figure 1). The majority (73%) of the operations were performed with vascular specialist input (21 with vascular consultant as main surgeon, 1 with vascular consultant assisting). One of these operations had a failed outcome (4.5%). Two operations were carried out by a specialist registrar unassisted, both of which had a failed result at follow-up duplex. Four operations were carried out by staff-grade doctors without specialist vascular training. Three of these had failed results. Two operations were carried out on a waiting list initiative by consultant surgeons in another unit. Both had a failed result on duplex scanning. Overall, eight out of 30 operations were carried out without the input of a vascular specialist and of these seven (88%) had a failed result (Figure 1). There was a significant difference in the success rate between limbs operated on by a vascular specialist and those operated on by non-vascular specialists (P < 0.0001).

Number of patients recalled for follow-up duplex scanning after SSV operation in the retrospective study and the number of patients/limbs who attended for duplex scanning. The number of limbs operated on by vascular specialists and non-vascular specialists is illustrated as well as the percentage outcome of successful or unsuccessful surgery
Following the policy change in 2004, the outcome from SPJ surgery was prospectively studied until June 2008. During this time period our unit experienced an increase in workload due to the development of a ‘one-stop’ varicose vein clinic. A total of 166 patients (female 115/male 51; age range 24–77 years) with 187 limbs (95 left side; 92 right side) underwent SSV surgery in this time period and were followed up with a duplex scan 6–8 weeks after the operation (Figure 2). A proportion of patients (55 limbs) had SSV surgery only; however, the majority had synchronous additional procedures. The additional procedures comprised: long saphenous vein (LSV), high tie and strip (48 limbs), venectomies (42 limbs) and VNUS closure of LSV (27 limbs). Other synchronous ipsilateral procedures included re-do LSV high tie, perforator, and giacomini vein ligation and subfascial endoscopic perforator vein ligation in the remaining patients. Out of 187 limbs, 179 were operated on either by a consultant vascular surgeon (including operations performed by a trainee supervised by a consultant vascular surgeon) or an associate vascular specialist (96%). Of these, 174 had a successful result recorded with no SPJ, no proximal SSV and no residual superficial vein reflux. The SPJ was missed in five limbs in four patients; an overall failure rate of 2.7%. Of sixteen limbs operated on by a higher surgical trainee with a vascular consultant assisting all had successful SPJ ligation (failure rate 0%). A total of seven limbs were treated by an associate vascular specialist. All had successful SPJ ligation (failure rate 0%). Non-vascular specialists performed eight SSV operations and two of these were performed by unsupervised higher surgical trainees. All showed patent SPJs on follow-up duplex (failure rate 100%) (Figure 2). Twelve procedures were re-do procedures, all of which were performed by a consultant vascular surgeon. None of these operations exhibited failure on review, although one SPJ ligation was not flush and showed a 5 mm stump. There were no significant differences between the success rate of SSV surgery before and after the introduction of more accurate preoperative SPJ marking for both operations performed with or without vascular expertise (P = 0.51 and 0.50, respectively). However, the overall success rate following the policy change in 2004 was significantly improved (pre-P = 0.009). There was a significant difference in the surgical success rate between vascular and non-vascular specialist in the prospective study (P < 0.0001).
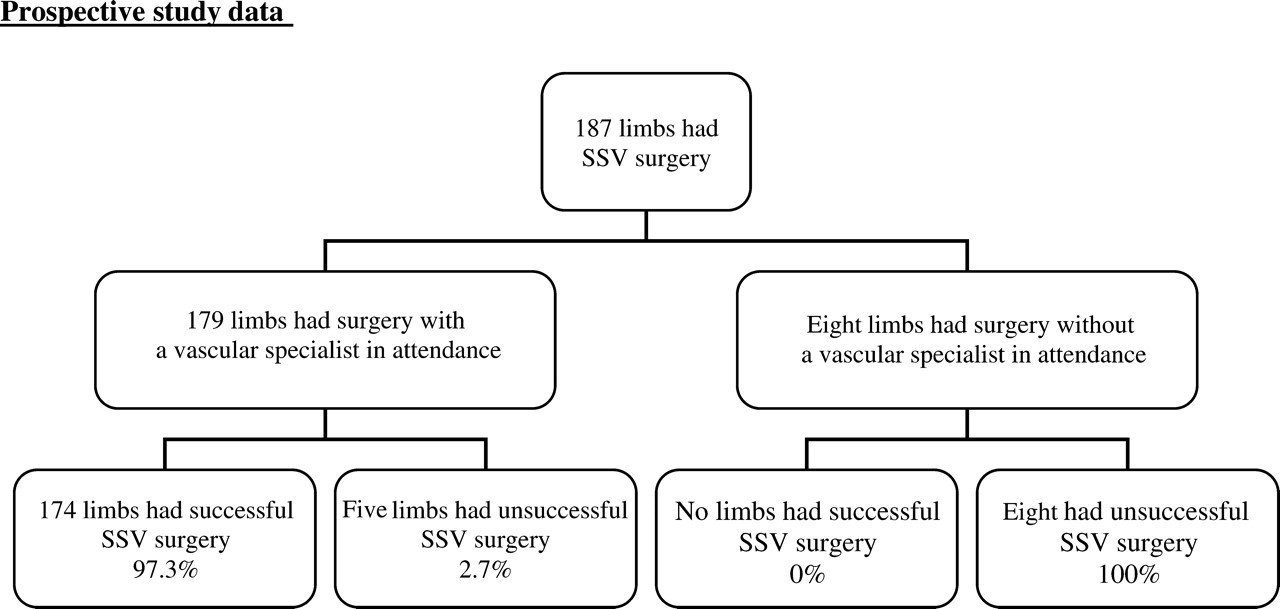
Number of limbs operated on by vascular specialists and non-vascular specialists in the prospective study group. Percentage outcome of successful or unsuccessful surgery is illustrated
Discussion
In both the retrospective and the prospective study, there was a significant difference in the success rate between vascular and non-vascular specialists. The rate of unsuccessful SSV surgery recorded in the retrospective analysis was similar to that reported in other studies. 4 Before January 2004, almost a third of operations were performed without the input of a vascular specialist; however, after this time a unit protocol was developed to prevent SSV surgery being put on to non-vascular lists, resulting in 91% of operations having vascular specialist input. The failure rate of SSV surgery dropped from 23% to 9% in this time period. Some SSV operations still took place outside the protocol but in an era of National Health Service waiting list targets, this type of non-urgent surgery may be assigned to ‘waiting list initiative lists’ or contracted out to other units. The surgeons who perform these lists will have varicose vein experience but, in practice, this may be confined largely to experience of groin dissection. Outside the vascular specialist unit, the details of SPJ anatomy and its variables may be lacking. Our improvement in the success rate seems to be mainly due to the increased involvement of vascular specialists. The introduction of detailed preoperative marking of the SPJ did not improve the outcome either for the vascular specialist or non-vascular specialist group. This suggests that preoperative duplex marking is unnecessary. A survey in June 2003 suggested that 59.8% of consultant members of the Vascular Society of Great Britain and Ireland use preoperative marking of SSV/SPJ. 9 It is now widely regarded that duplex imaging to confirm the presence of SPJ reflux is mandatory as SPJ incompetence is difficult to diagnose clinically. 9,10 Distance from heel measurement to the SPJ would, therefore, not add significantly to the time or cost of the management of these patients, although assessing its value requires further investigation.
However, our subsequent (and continuing) method of marking the SSV and SPJ immediately preoperatively provides more anatomical information than SPJ level alone and allows for a smaller surgical incision. As more portable scanners become available and intraoperative ultrasound scanning becomes more routine, this method allows for on-table marking of the SPJ. The immediate anatomical image available to the surgeon shows size, angulation and branch anatomy, which provides greater confidence during dissection.
Due to difficulty in identifying the SPJ correctly, some have argued that uncomplicated SSV varicosities should be treated with repeat multiple phlebectomies and sclerotherapy alone. 3 In practice, less than 1% of surgeons use this approach. 9 Our study is against this argument and supports the practice of formal SPJ ligation practised by most surgeons. 3,9 It demonstrates that, in the hands of a surgeon with vascular expertise, successful SPJ ligation can be achieved in 95% of cases.
The advent of endovascular techniques such as foam sclerotherapy, endovenous laser treatment and radiofrequency ablation may in the future absolve us from the need to dissect the SPJ in most patients. 11–17 A number of patients will, however, still require surgical exploration, e.g. due to unfavourable anatomy or patient choice. There is after-all no randomized controlled trial to date comparing conventional surgery with endovascular ablation. The decision between the techniques therefore relies on availability of technique and patients preference. Unfortunately, endovascular techniques will reduce training opportunities to familiarize trainees with the anatomy of the popliteal fossa and make it more difficult to achieve the expertise needed to dissect the SPJ.
Conclusion
SPJ exploration is technically demanding. A major factor ensuring correct ligation of the SPJ is the level of vascular expertise of the operating surgeon. Accurate anatomical data provided by duplex scanning immediately prior to operation is helpful but does not protect the inexperienced surgeon from failing to identify the SPJ correctly. Interpretation of duplex findings and exploration of the SSV and popliteal fossa should, therefore, be an exercise subject to satisfactory assessment before proceeding to independent practice.