
Abstract
Background
Deep vein thromboses (DVTs) are a significant cause of morbidity and mortality. Valvular destruction leads to the spectrum of disease called the post-thrombotic syndrome (PTS) with the sequelae of chronic venous ulceration and a reduced quality of life. Catheter-directed thrombolysis (CDT) may reduce the incidence of PTS following an acute proximal DVT and increases quality of life thereafter, but it is uncertain what proportion of patients diagnosed with a DVT would be suitable for CDT.
Methods
This study quantified the proportion of patients investigated for DVT that would have been suitable for CDT. A retrospective review was performed of all upper and lower limb duplex ultrasound scans for suspected DVTs in a contemporary one-year period in a major regional vascular institute. All positive scans for acute proximal lower limb DVTs were compared against strict inclusion and exclusion criteria for CDT, based on national guidelines and international randomized trials.
Results
A total of 2368 duplex ultrasound venous investigations were performed in a one-year period and 252 scans demonstrated DVT. Of these, 158 were acute proximal lower limb DVTs. Application of the inclusion and exclusion criteria for CDT suggested that 47/158 (30%) were potentially suitable for CDT using current criteria. The median age of the 158 patients was 58 years, meaning that more than half were of working age and 54% were men.
Conclusion
Using current eligibility criteria, only about 30% of patients with DVT appear to be suitable for CDT.
Background
Deep vein thrombosis (DVT) is a significant cause of morbidity and mortality in the general population and currently affects one in 1000 people in the UK each year. 1 It is the third most common cardiovascular pathology after coronary artery disease and stroke, 2 and its incidence is expected to rise over the next decade due to the rising elderly population and increased exposure to DVT risk factors such as hospital admission, oral contraceptives, pregnancy, obesity and long distance travel.
Prolonged exposure to an obstructive thrombus within a deep vein can cause valvular incompetence and venous reflux, which leads to venous hypertension. This sequence of events causes the post-thrombotic syndrome (PTS), which has important clinical implications in the form of significant pain and swelling in the affected limb, which impairs walking and perpetuates the initial disruption to venous flow. Recent research has shown that patients with PTS have a poorer quality of life than other patients of similar age with diabetes, arthritis or chronic lung disease, while patients with severe PTS report a quality of life similar to angina, cancer or congestive heart failure. 3,4 PTS ultimately leads to the development of chronic venous leg ulcers, which occur in up to 10% of DVT patients in two years 5 and are a source of considerable morbidity and financial burden within the UK, costing the English NHS £400 million per year to manage. 6
Proximal (above the knee) DVTs account for 80% of all symptomatic DVTs. Current best practice in the management of these cases involves a course of anticoagulation therapy in conjunction with graduated elastic compression stockings worn for two years post-thrombosis, which can reduce the incidence of PTS by up to 50%, although compliance with stockings and regulation of anticoagulation can be difficult to estimate. 7 Despite these therapies, the cumulative incidence of PTS at two years following a proximal DVT remains as high as 50% in large, contemporary cohort studies reporting to consensus-defined standards. 5,8
Alternative management strategies involve the local delivery of thrombolytic agents directly into the thrombus to achieve rapid local resolution of the thrombus and to restore venous patency, known as catheter-directed thrombolysis (CDT). A Cochrane review estimated that the use of CDT might improve valvular function and reduce the incidence of PTS by 34%. 9
A number of contraindications to CDT have been described, 10 some absolute and some relative, and thus if CDT is to be tested in a randomized trial, a pre-requisite is to estimate likely patient recruitment. The purpose of this study was to investigate the proportion of patients with ultrasound-diagnosed DVT who were potentially suitable for CDT.
Methods
A retrospective case-note review of all upper and lower limb duplex ultrasound scans for suspected DVT was performed in a one-year period in a major regional vascular unit: St George's Vascular Institute, London, UK. Case identification was through search of electronic radiological records using the Radiology Information System (RIS). Items searched for were the words or phrases ‘DVT’, ‘deep vein thrombosis’ or ‘venous duplex’ in any of the scan type or report fields. No ultrasound scans included in this study were performed outside of this institute. All scans were performed for the investigation of DVT, as venous studies performed in preparation for arterial bypass surgery were carried out in a different hospital location. All the scan requests were included along with the report and these were reviewed in tandem with the scan results.
Manual review of all duplex reports was performed to identify positive results occurring within the defined one-year period. All negative scans and duplicate entries were excluded, as were cases that reported chronic and subacute DVTs on follow-up investigations. All reports stating that a ‘high suspicion’ of DVT was present were excluded to preserve accurate reporting and quantification of this study. Upper limb and lower limb scans were reported separately.
In order to meet the objectives of this study, inclusion and exclusion criteria for CDT were retrospectively applied to the cases identified (Table 1). These were based on a recent review by this research group, 11 the American College of Chest Physicians guidelines 10 and the protocols of two RCTs currently running in the USA (NCT00790335) and Norway. 12 Patient age was taken at the time of the duplex investigation. Haematological results were obtained using electronic patient records from the hospital intranet together with documentation in their medical notes.
Study selection criteria

DVT, deep vein thrombosis; SBP, systolic blood pressure; DBP, diastolic blood pressure; ACKD, acquired cystic kidney disease
Positive scans were defined by their most proximal extent under the broad classification
of upper limb (internal jugular vein to brachial vein) and lower limb (inferior vena
cava [IVC] to calf veins). Lower limb thromboses were further subclassified as follows:
Iliofemoral in which the most proximal extent of the thrombus was between the
IVC and the common femoral vein; Above-knee where the most proximal extent of the thrombus was in the femoral or
popliteal veins; Distal – below the knee.
Only acute proximal lower limb DVTs (above-knee and iliofemoral) would be
considered for CDT under currently accepted inclusion criteria. These cases were
identified and subsequently limited to patients aged between 18 and 75 years old at the
time of thrombosis. The case-notes for these patients were withdrawn from the medical
record archives to allow the accurate application of inclusion and exclusion criteria
for CDT. The number of cases fitting these criteria in this one-year period was
quantified.
Results
The RIS system searches allowed the positive identification of 2368 DVT duplex ultrasound scans. Of these, 227 were duplicate reports and excluded, leaving 2141 duplex reports on individual patients in this one-year period. From this group, 252 patients had positive duplex scans for DVT (11.8%). These constituted 193 acute and 59 chronic DVTs occurring in both upper and lower limbs. Upper limb thromboses were identified in 13 patients. Acute lower limb DVTs were identified in 180 patients (Figure 1). Distal DVTs (limited to the calf veins) occurred in 22 patients and were excluded.
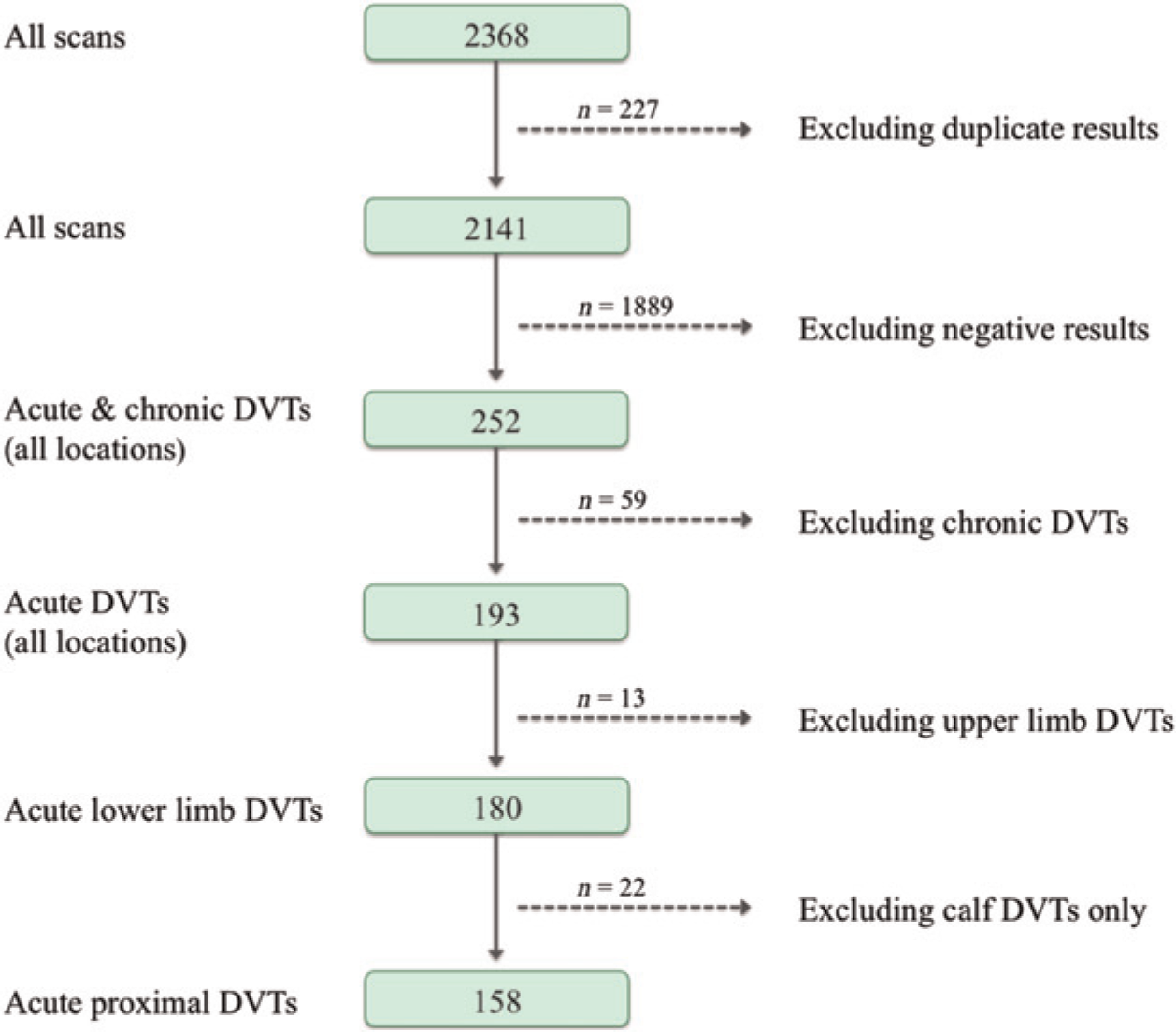
Flow chart showing filtering process for duplex ultrasound reports. DVT, deep vein thrombosis
First-time, acute, proximal lower limb DVTs (above the knee and iliofemoral) were identified in 158 patients (Figure 2). The anatomical distributions of the thromboses are shown in Figure 3a. The median age of this cohort was 58 years and 53.8% (85/158) were men.

Flow chart showing filtering process for acute proximal DVT reports. DVT, deep vein thrombosis
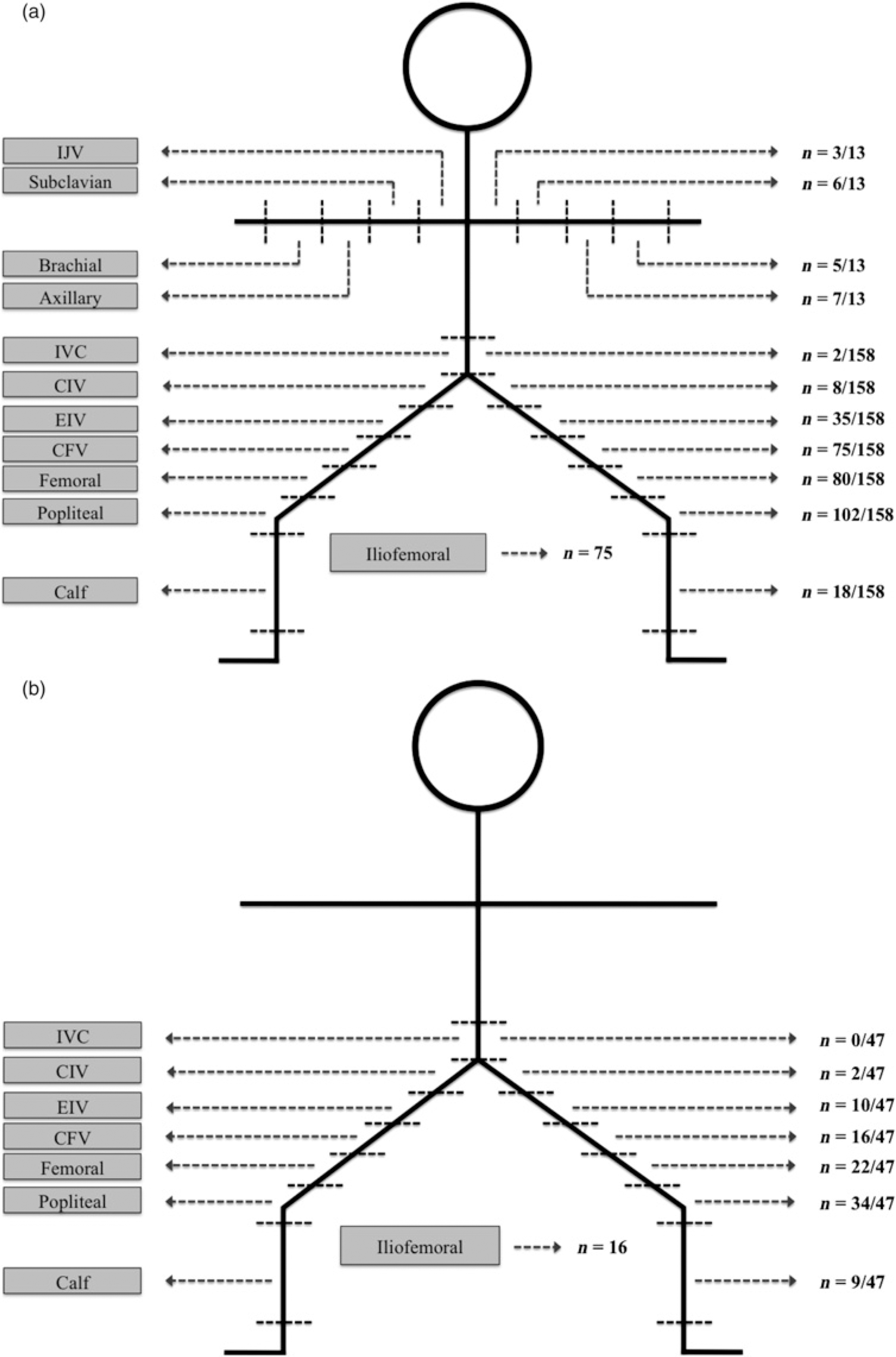
(a) Diagram showing anatomical sites of all acute proximal DVTs (n = 158) and upper limb DVTs (n = 13), excluding calf DVTs only (n = 22). (b) Diagram showing anatomical sites of all acute proximal DVTs using the exclusion criteria (n, 47). IJV, internal jugular vein; IVC, inferior vena cava; CIV, common iliac vein; EIV, external iliac vein; CFV, common femoral vein; DVTs, deep vein thromboses. Cumulative frequency of all DVTs in each anatomical location
Of the 158 patients with proximal DVTs, there were 36 positive scans in patients that fell outside the age criteria of 18–75 years and these cases were excluded, leaving 122 acute proximal DVTs available for consideration for CDT. A further 18 were excluded due to previous ipsilateral DVTs, eight cases were excluded due to the onset of symptoms present more than 14 days prior to presentation and four cases were excluded due to missing or incomplete medical notes. Seventy-five cases of iliofemoral DVT were identified.
Four incomplete or missing cases were excluded for the following reasons: hospital notes for two patients were incomplete and did not provide enough information to allow hypothetical eligibility into prospective thrombolysis trials; one patient attended accident and emergency without admission, and no formal medical notes were generated; finally, one set of notes was missing from the hospital tracking system and therefore not feasible to locate.
The 92 patients who met the inclusion criteria underwent a detailed case-note review. The distribution of the thromboses is shown in Figure 3b. Compliance with the stated exclusion criteria led to a further reduction in case numbers of 45. The reasons for cases being excluded are shown along with the specific exclusion criteria (Table 2). This left 47 patients who were potentially suitable for CDT within a 12-month period at this hospital. The median age of these 47 cases was also 58 years. Overall, (47/158) 29.7% of all acute above-knee lower limb DVTs and (47/180) 26.1% of all acute lower limb DVTs were potentially suitable for CDT after application of strict inclusion and exclusion criteria. After further application of an age restriction, (47/122) 38.5% of all proximal lower limb DVTs were potentially suitable for CDT.
Results of the study selection criteria on the number of acute proximal DVTs meeting the inclusion criteria (n = 92)
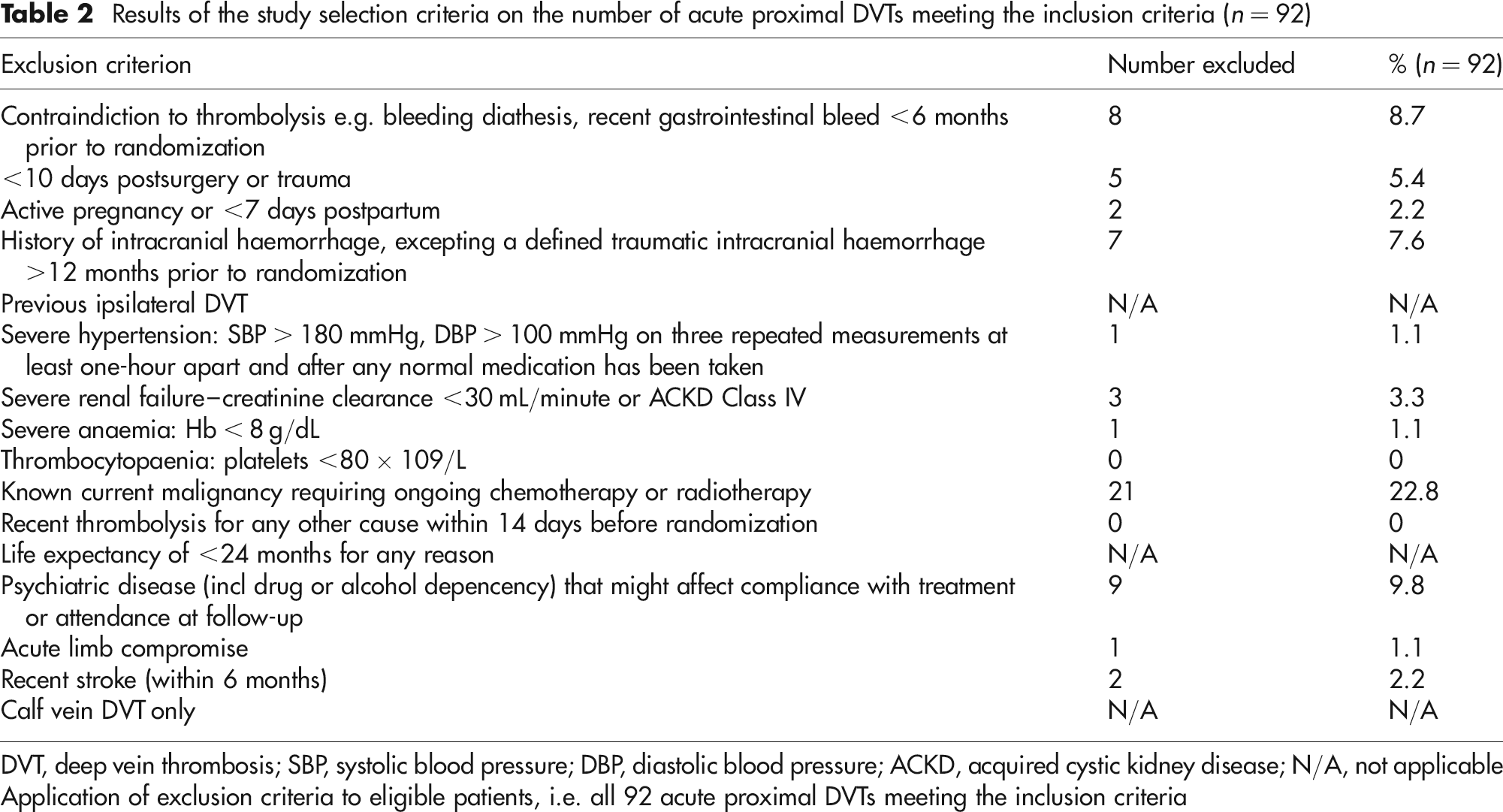
DVT, deep vein thrombosis; SBP, systolic blood pressure; DBP, diastolic blood pressure; ACKD, acquired cystic kidney disease; N/A, not applicable
Application of exclusion criteria to eligible patients, i.e. all 92 acute proximal DVTs meeting the inclusion criteria
Discussion
This retrospective audit of DVT diagnosis in a large London vascular institute has demonstrated that, after the application of strict inclusion and exclusion criteria, 30% of above-knee DVTs would have been suitable for CDT. This would significantly alter the management of DVT in this cohort of patients with anticipated gains in outcome. In particular the cumulative incidence of PTS and venous ulceration might be lower, with attendant gains in quality of life.
It is likely that these figures would be reflected in other major vascular centres, or exceeded in those that have a specific venous interest. Therefore, it would be expected that there would be a great number of DVT per annum that might be best treated by CDT, despite the strict criteria used in this retrospective study. These criteria are likely to be relaxed in the future, following a common pattern of the introduction of other novel treatments, if CDT is accepted as a first-line treatment for DVT. This would mean that this study has underestimated the potential of this treatment, as more patients would be considered suitable for CDT.
Modern management of acute DVT with oral anticoagulation and compression stockings 7 has been shown to significantly reduce the incidence of PTS, 9 venous thromboembolism and limit DVT recurrence, but does not treat the underlying pathology behind PTS (i.e. venous obstruction and hypertension and valvular reflux). Even, the imminent introduction of the fixed dose oral anticoagulant therapies into routine clinical practice, such as rivaroxaban and dobigatran, is unlikely to increase thrombus lysis despite other notable advantages over the use of warfarin.
One confounder to studies of the long-term outcome of DVT is that the true incidence of PTS is not known due to variations in treatment and the assessment of affected limbs. A number of recent large cohort studies have attempted to quantify this and have been aided by the introduction of reporting standards for both for the quality of life and incidence of PTS following DVT. 13–15 This would appear to make the more recent cohort studies on which these guidelines were based the most accurate estimates of PTS in the community. 8,16 If this is the case, then the reported rates of PTS may be as high as 50% despite medical therapy.
The prompt and effective removal of an acute thrombosis has been shown to effectively preserve venous valvular function, reduce reflux and removes venous obstruction. This also reduces the risk of thrombus recurrence, which is a strong predictor of a poor long-term outcome from DVT and severe PTS. 17 Successful clot lysis has been demonstrated in up to 85% of patients undergoing CDT, with the majority of these being grade III (complete) lysis and the remainder being grade II (50–90%) lysis. 18–21 In so doing, CDT prevents the subsequent development of PTS. As well as reducing the cumulative incidence of PTS, CDT may also reduce the severity of PTS, which is correlated with impaired QoL in graded fashion. 3
Clot-burden change also predicts long-term outcome from DVT, providing clinically relevant, patient-specific prognostic findings and also predicts DVT recurrence. 22,23 CDT provides a safe and effective way of performing rapid local thrombus removal, in addition to current medical treatment strategy of anticoagulation and elastic compression stockings. 9,18 The mid-term outcomes from the Norwegian CaVenT trial suggested that CDT increased iliofemoral patency from 36% to 64%, which was statistically significant. The resultant preservation of venous patency without reflux, and subsequent prevention of PTS, is associated with improvements in quality of life and so is likely to have associated economic gains over traditional treatment methods. 19
Haemorrhagic complications are an anticipated complication associated with a lysis strategy, and may be minimized with careful catheter placement under ultrasound guidance to avoid multiple vessel puncture. Infrequent bleeding complications were reported by a national multiregistry study in the USA, 21 which mainly involved catheter insertion sites (4%), together with musculoskeletal, gastrointestinal, and genitourinary bleeds (3%), retroperitoneal haematoma (1%), and intracranial haemorrhage (<1%). The reported rate of mortality associated with CDT was less than 1%, which may become less frequent with routine practice.
CDT can be viewed as a new horizon in the management of DVT, which eliminates the root of long-term morbidity including DVT recurrence, rather than simply preventing thrombus propagation and clinical deterioration, or relapse. Therefore, CDT represents an attractive therapeutic adjunct in the management of acute DVT in defined patient subgroups.
However, this treatment remains poorly adopted in clinical practice due to a lack of level 1 evidence. One aim of this study was to assess the feasibility of implementing a major, multicentre RCT on CDT in England to address this knowledge gap and clinical equipoise. The results of this study suggest that a major randomized trial involving CDT would indeed be feasible for acute proximal lower limb DVT, as long as key stakeholders can be effectively engaged to ensure adequate recruitment. This is especially important in light of the fact that only 30% of patients with acute lower limb DVT might be candidates for CDT based on these results and inclusion criteria.
The cost of implementing CDT may present one barrier to its introduction as a primary therapy for acute DVT, as each case has significant procedure costs which are in addition to the costs of medical therapy. CDT also requires an inpatient stay whereas currently most DVTs are managed as outpatients. Sufficient evidence will have to be produced through clinical trials to quantify the long-term socioeconomic benefits in terms of quality-adjusted life-years and incremental cost-effectiveness ratios to justify the generalized uptake of this procedure. These benefits have been illustrated in a number of previous studies on the basis that PTS is lifelong, irreversible and costly via medical care and through work disability. 8,19 Consequently, it is expected that there will be demonstrable benefits in terms of reduced hospital and community health-care needs and in terms of fewer missed workdays leading opportunity cost advantages with CDT. 9,19 This is all the more relevant when considering that well over 50% of cases suitable for CDT would be in people of working age, from both this and previous studies.
Given the current costs and potential risks of CDT, it is suggested that case selection should conform to strict guidelines at the current time, and the decision to perform CDT should be through the working of a multidisciplinary care team involving haematologists, interventional radiologists and vascular surgeons.
As a final comment, it was interesting to note that only 252 or 2141 (11.8%) of DVT investigations were positive. This would suggest that the clinical diagnosis of DVT is not straightforward. In order to save on costly scanning time, these results might suggest that further research efforts should be focused on the development of accurate (sensitive and specific) and cheap point of care diagnostic tests for DVT.
Conclusions
DVT is a common condition that affects a large number of people of working age. Current treatment strategies do not optimize thrombus removal and leave patients at risk of long-term complications including DVT recurrence, PTS and venous ulceration. CDT provides a more effective method of treatment for acute proximal lower limb DVTs than medical treatment alone, although only 30% of patients would appear realistic candidates based on these results. Despite this, it would appear that there are a large number of patients missing out on a potentially beneficial therapy at present due to a poor uptake of CDT.