
Abstract
In this article we want to discuss the potential of lower extremity deep vein thrombosis (DVT) imaging and propose a systematic approach to DVT management based on a DVT classification of the lower extremity; the LET classification. Identifying and reporting DVT more systematically allows for accurate stratification for initial patient care, future clinical trials and appropriate descriptions for natural history studies.
Introduction
Acute deep vein thrombosis (DVT) of the lower extremity is a disease which has life-impairing consequences in the majority of those affected. It occurs in close to one person per 1000 population per year. Under the current standard treatment regimen (systemic anticoagulation), the outcome is far from optimal, with up to a 30% recurrence rate of DVT within five years and a 40% risk of post-thrombotic syndrome (PTS) within two years.1,2 This highlights the need for improvement of treatment outcomes, which can potentially be achieved with more invasive treatment modalities such as catheter-directed thrombolysis, 3 5 as has recently been confirmed by the Ca Vent trial. 6
The traditional classification of DVT offers two options: distal or proximal. The threshold location is the popliteal vein. Numerous observational studies have reported on outcome after ‘proximal’ or ‘distal’ DVT. Reviewing these studies, listing DVT extent, therapy and outcome, showed that there is a wide variety and inconsistency of reporting of DVT with regard to the location and extent of DVT. Therefore, the published data are not adequately comparable and the current medical reporting will not allow stratification to different therapy options.
With the current diagnostic imaging tools, including a range of new and updated imaging techniques, not only has identification of DVT become more easy but also visualization of the entire deep venous system is possible, allowing routine identification of potential underlying causes and accurate assessment of the location and extent of the disease. A combination of expanding the yield from clinical diagnostic imaging combined with standardized reporting will allow for an adequate comparison of published data and stratification to different treatment regimens.
Imaging
The described imaging techniques in the paragraphs below are not a complete review, but a summary of the key points of commonly used techniques to image DVT and their application in daily practice.
Over the past decade a wide variety of new imaging techniques to visualize DVT have been developed. Conventional phlebography, which is officially the gold standard, still has its uses, but as a routine diagnostic tool to identify DVT it has been surpassed by less invasive imaging alternatives. It is still the best imaging modality to visualize the extent of reflux in the deep venous system.
The last major change with regard to imaging of DVT was duplex ultrasound replacing conventional phlebography in the (routine) examination of patients suspected of DVT. The main reason for this is that the diagnostic question in the clinical setting is only the presence or absence of DVT. Thus the examination is often limited to verifying the compressibility and flow in the common femoral vein, the femoral vein and the popliteal vein. This also explains why there is such a wide variety and inconsistency on reporting DVT. Diagnostic imaging information, related to the extent of DVT, is scarce. Furthermore, there are also limitations to ultrasound imaging of DVT. In (morbidly) obese patients, compressibility and flow can be difficult to assess, making the examination either inconclusive or false-positive. The same applies in patients who present with recurrent DVT. Due to the changes in the vein wall (which becomes more rigid), ultrasound assessment of these veins becomes significantly less accurate. Additionally, no diagnostic information is available about the extent of the DVT. Questions such as: is it limited to one vein or more, does it involve not only the popliteal and/or femoral veins but also the iliac veins and are there signs of an underlying disease such as May–Thurner, atresia of the inferior vena cava, anatomical variants or a mass compressing the veins, remain unanswered. In the hands of a dedicated radiologist or technician, with enough time, duplex ultrasound can actually provide a lot of this additional diagnostic information in many cases. However, as mentioned before, in extensive or recurrent DVT there are other techniques that should be considered.
For example, with the current generation of computed tomography-scanners (CT-scanners), a contrast enhanced CT can visualize the abdominal and pelvic deep veins as well as the femoral and popliteal vein segments in great detail with a relatively low contrast and radiation dose. 7 Such a CT scan will provide an overview of the entire deep venous system from the inferior vena cava down to the groin or even the upper calf, depending on the extent of the scan. In acute DVT this examination will depict the location and extent of the thrombosis accurately 7 Unfortunately, a CT scan requires ionizing radiation (with the highest administered dose in the pelvic region) and in heavy and obese patients a significantly higher tube-voltage is generally required to acquire diagnostic images. There are no reports with regard to the accuracy of CT-venography in patients with recurrent or chronic DVT.
Alternatively, there are a number of different magnetic resonance imaging (MRI) techniques available to image DVT, which can roughly be divided into two groups. The first group of techniques focuses on depicting the deep venous system and its attributes, in most cases with the use of an intravenous (IV) contrast agent. The second group focuses on depicting/detecting thrombi specifically. This second group uses the magnetic attributes of methaemoglobin in clot, allowing visualization of thrombus without using intravenous contrast. 8 This MR direct thrombus imaging technique (MRDTI) has shown promising results with regard to the visualization of thrombi, and thus is effective with regard to the clinical question of whether or not DVT is present. In addition, this technique is also capable of providing information with regard to the level and extent of thrombosis. However, it does not visualize the entire venous system and surrounding structures to identify underlying causes or identify anatomic variations. Furthermore, since this technique focuses on imaging new or recent thrombus (0–3 months), there is no or limited visualization of older thrombi or chronic (fibrotic) changes in the veins due to old DVT events.
This brings us to the first group, in which there are MR techniques that allow us to visualize the deep venous system completely. The aim of these contrast enhanced MR techniques is to accurately identify thrombosis, while providing a detailed anatomical overview of the veins, arteries and surrounding tissues. In addition, they might have the potential to visualize late and/or chronic changes in these veins, which still has to be investigated. There are a few variations of this contrast enhanced MR technique, but in order to be able to visualize the entire deep venous system from the calf up to the inferior vena cava, there are a few prerequisites, at the moment limiting the suitable protocols. In order to be able to scan such a volume (3–5 stations), 15–30 minutes of contrast enhanced scan time is required. Keeping the injected contrast volume within reasonable limits, this requires the use of a specific contrast agent, a so-called bloodpool contrast agent. The advantage of the use of a bloodpool contrast agent is that this greatly improves the contrast enhanced phase duration and thus increases the effective scan time. With a conventional MR contrast agent the contrast enhanced phase lasts only 5–10 minutes effectively, whereas with a bloodpool agent the contrast enhanced phase can last up to at least 30 minutes, allowing the high-resolution depiction of the entire venous system with the administration of a single dose of contrast. Furthermore, it requires dedicated equipment and technicians to be able to keep the scan times within a reasonable window (25–40 minutes).
In conclusion, there are a few (good) options to complement duplex ultrasound in the diagnostic imaging of patients with DVT. Depending on local expertise, equipment and available examination time, dedicated CT or MRI protocols are both capable of creating a broad overview of the deep venous system.
Classification
Description of the venous segments used in the LET classification

LET lower extremity thrombosis classification
LET class I: calf vein thrombosis
Patients with an isolated calf vein thrombosis usually do not have an outflow limitation of the deep venous system of the lower leg. It is important to differentiate this subgroup of patients as it is known that calf vein thrombosis can potentially extend into the popliteal vein, evolving into a DVT which can obstruct the deep venous system and place the patient at higher risk of pulmonary embolism and more severe post-thrombotic morbidity. Furthermore, there is evidence that suggests that the identification of involvement of axial (para-arterial tibial) veins versus deep-muscle veins in the calf is of clinical significance with regard to the success of systemic anticoagulant therapy in these groups of patients, 9 12 although recent observations challenge prior concepts. 13
LET class II: popliteal and femoral vein thrombosis
The second group is patients with thrombus in the popliteal and/or femoral vein. There is no occlusion of the common femoral vein. There can be impaired venous outflow due to an increased outflow resistance, but this is compensated for by increased venous return via superficial veins and a patent deep femoral vein system. This is the most likely explanation for why the majority of these patients do not develop severe PTS following an episode of DVT14,15 Persistent deep venous incompetence in the femoral vein might influence outcome, 16 18 but in these cases, the collateral pathways (superficial and deep femoral veins) reduce outflow obstruction for the lower extremity. Systemic anticoagulation prevents progressive thrombosis and may allow adequate physiological lysis of the thrombus in this segment leaving minimal residual obstruction of the deep venous axis and a relative low risk for the development of PTS. There is no evidence suggesting that invasive therapeutic options such as catheter-directed thrombolysis (CDT) provide an outcome benefit over systemic anticoagulation and compression therapy.
LET class III: common femoral/iliac vein obstruction
The third group is patients whose thrombus occludes the common femoral vein and/or iliac veins, thus obstructing the outflow of the entire venous drainage of the lower extremity. This poses an increased risk for the development of PTS and/or recurrence of DVT9,14-16
Persistently impaired outflow produces severe venous hypertension, especially ambulatory venous hypertension. Valves in and distal to the thrombotic segments might develop valvular incompetence. Valvular incompetence is caused by the destruction of valves and secondary to the venous dilation due to persistent obstruction caused by persistent proximal obstruction. This results in impaired outflow and increased valve incompetence, increasing the chance of developing recurrent DVT and/or PTS.
Based on available evidence, strategies of thrombus removal in patients with iliofemoral DVT offer patients an opportunity to restore patency, enjoy a better quality of life by avoiding PTS, and potentially reduce their risk of recurrence.
LET class IV: inferior vena cava
Thrombosis of the inferior vena cava (IVC) results in an outflow obstruction of the deep vein axis of both legs, which may or may not be associated with iliofemoral DVT of one or both legs. Similar to patients with iliofemoral DVT, restoring the outflow of the IVC to the heart can result in marked clinical improvement.
LET classification: imaging recommendations
Class I and Class II: Imaging can be limited to visualization of the popliteal and (common) femoral veins; crucial is the exclusion of involvement of the common femoral vein, reducing the probability of involvement of the inferior vena cava and/or iliac veins to less than 1%.
Class III and Class IV: Imaging should not only cover the popliteal and (common) femoral veins, but also the iliac veins and inferior vena cava. To effectively treat DVT involving the common femoral vein (and above), unobstructed outflow to the IVC and/or heart needs to be documented.
It is crucial to identify an underlying lesion which might have contributed to the initial venous thrombosis and may lead to recurrent thrombosis if left uncorrected (e.g. May–Thurner, IVC interruption or atresia). It is also essential to identify distal involved segments, because the total thrombus load influences outcome.9,16
Table 2 is a comprehensive overview of the classification described above. Figure 1 shows how the thrombosed segments translate into a LET class.
Scoring the LET classification. Encircle the segments involved Comprehensive overview of the LET classification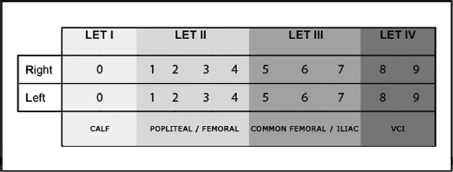

Discussion
These new definitions will clarify the benefits of new modalities of patient care, especially those designed to mechanically or pharmacologically clear the venous system of clot. The LET classification organizes the clinical heterogeneity of patients with DVT of the lower extremities in sharply demarcated subgroups. This new nomenclature will be helpful when describing DVT of the lower extremities in both a research setting, in clinical practice and when stratifying risk of patients. Additionally it will be helpful in the future when deciding on a more or less invasive treatment approach.
We acknowledge that there is currently limited study data to support our proposed classification. However, in our opinion this only strengthens the need for a consensus with regard to describing the location and extent of DVT accurately. The reason that we want to introduce a classification is that in regard of the current standards we are still treating very heterogeneous groups of DVT patients identically. Taking the results of recent DVT studies into consideration, it has been shown that there are significant subgroups within the ‘proximal’ and ‘distal’ standard groups. Not identifying these subgroups will hamper the outcomes of present and future studies. To make the next step in DVT research and future clinical treatment, it is required that we enable ourselves to properly compare future study results as they apply to different anatomical distributions of DVT. These anatomical subgroups identify patients that might develop PTS and recurrent DVT, and whether these post-thrombotic outcomes can be predicted and avoided.
Conclusion
In order to optimally treat DVT it is vital to accurately identify and describe the location and extent of the disease. Additionally, in extensive iliofemoral DVT it is crucial to identify or exclude underlying disease. A multimodality imaging approach combined with standardized reporting (e.g. the LET classification) is a simple and potentially meaningful approach to manage DVT treatment. Identifying and reporting DVT more systematically allows for accurate stratification for initial patient care, future clinical trials, and appropriate descriptions for natural history studies.