
Abstract
Objectives/Hypothesis
Phleboliths in venous malformations (VM) of the head and neck are often observed and may cause significant symptoms. Only a few articles refer to the morphology and composition of the phleboliths in VM. The objective of this study was to analyse and to demonstrate their composition and morphology.
Methods
Patients with VM presenting to a vascular anomalies centre during a three-year period were identified. The incidence of phleboliths was analysed followed by morphological and structural analysis with cone beam tomography and X-ray diffraction.
Results
Phleboliths were identified in 28/98 patients with VM of the head and neck. Seven patients underwent conventional surgery to reduce the volume of the VM or to remove the phleboliths, which were localized in the cheek (3 cases), submandibular region (2 cases), infrahyoidal neck or upper eyelid (1 case each). The structural analysis showed that more advanced lamination and an increasing radiopacity of the cortex was observed in larger phleboliths. X-ray powder diffraction analysis revealed that the main constituent in the pulverized phleboliths was carbonate-fluorohydroxylapatite.
Conclusion
This study shows in a vivid way that phleboliths from VM of the head and neck area show a laminar structure and consist of apatite, without any indication of differences in their chemical composition. Treatment of localized intravascular coagulopathy in VM might be able to prevent the formation and the progression of phleboliths. Hypothetically, another option might be lithotripsy.
Keywords
Introduction
Phleboliths within venous malformations (VM) of the head and neck are often observed. Stagnation of blood flow and thrombosis in VM have been related to the cause of phlebolith formation.1,2 They may worsen symptoms of VM such as pain, stasis, swelling and foreign body sensation in the affected individuals.3,4 In many cases a complete elimination of the VM is not possible. 5 Conventional surgery, sclerotherapy or laser therapy may face limitations, depending on the location, the extent and the related symptoms of the VM. Sometimes it might be appropriate to achieve symptom relief, albeit temporarily, by removal of the phleboliths. 6 Even though the detection of phleboliths is considered as pathognomonic of VM,1,7,8 only a few articles refer to their morphology and composition. For better understanding of the etiopathogenesis of phleboliths, it will be important to analyse their composition and morphology besides the clinical manifestation, which is the objective of this study. More precise knowledge of the components and structure of the phleboliths would allow speculations and hypotheses on how to prevent their formation or their progress, or if other methods such as lithotripsy would be of potential interest in the context of VM management.
We have used X-ray powder diffraction analysis, which is a technique used mainly by mineralogists to characterize crystalline structures and to determine relative abundance of crystalline compounds. This technique has already been described for analysis of different human stones, e.g. sialoliths or renal stones.9,10 Clinical and mineralogical findings have been reported only in a very limited number of cases. Further, the stones were studied using cone beam tomography (CBT), allowing high-resolution imaging by volume rendering and thin panoramic slices. 11
Material and methods
Patients with VM
This is a three-year study of 98 patients who presented with VM of the head and neck from 1 July 2007 to 30 June 2010. Follow-up in outpatient settings was warranted for all patients who received surgical treatment and ranged from 13 to 43 months.
The collected essential medical data included demographic parameters, localization, clinical presentation, radiological reports and coagulation analysis with determination of D-dimers, fibrinogen and platelet count.
Ultrasound examination was performed using 7.5-MHz linear-array transducer (Sonoline G60 S; Siemens, Erlangen, Germany). Colour-coded duplex ultrasound was used routinely to detect the vascular flow of all lesions. The indication of other imaging studies, such as magnetic resonance imaging (MRI), CBT of the head (CBTHEAD), computerized tomography scan and plain X-ray (e.g. Orthopantomography), was based on the clinical findings of the affected patients. This was independent of the analysis of phleboliths. Patients who had conventional surgical therapy with removal of phleboliths were identified and enrolled in the present study.
Morphological studies with CBT
All phleboliths had been rinsed in distilled water, air dried and stored at room temperature, measured and weighed. For gross macroscopic evaluation, the stones were cut using a sharp scalpel.
The phleboliths were positioned on an acrylic glass or on a sponge for the CBT examination (Accu-I-tomo F17; Morita, Kyoto, Japan). The emitter-detector unit of the CBT moved around the centre of the unit for about 18 seconds. During this time 570 single slices of X-ray images were produced. The extension of the X-ray beam was conical: the top of the cone was the emitter of radiation while the base was the detector. The exposed volume ranges from 4 to 10 cm in height and 4 up to 17 cm in transverse diameter. This was set to 4×4 cm for the purpose of the study to achieve the smallest accommodating volume of the unit. The tube voltage was set at 60 kV and the tube current at 1 mA, resulting in a computed-tomography-dose-index of 0.4 mGy. The special software (Idixel®, Morita, Kyoto, Japan) was used for image processing. Based on the registered isometric voxel of 0.08 mm, pictures with a slice-thickness of 0.125 mm and slice interval of 0.125 mm were reconstructed in all three orthogonal planes.
X-ray diffraction analysis
The largest phlebolith per patient was used for the analysis by X-ray powder diffraction. After CBT examination, the dried and cut phleboliths were pulverized in an achate mortar. X-ray diffraction analysis was performed on the pulverized specimen by an X-ray diffractometer (Siemens D500, Germany). The powder was placed in a holder and was then exposed to a continuous X-ray beam Cu Kα1.2 with a wave-length of 1.54 Å and X-ray tube voltage 50 kV, tube current 30 mA and scan speed 1° min−1 (2θ). The X-ray tube is equipped with copper anode and beryllium window. The intensity of the reflected radiation was then recorded using a goniometer. The presence of each phase was determined by the detection of their characteristic X-ray reflections. The X-ray diffraction pattern of each sample was matched with the standard data from crystalline minerals using powder diffraction files and validated by a mineralogist. The X-ray analytical identification of certain compounds is possible because every chemical substance will show a diffraction diagram which is characteristic for the substance.
Results
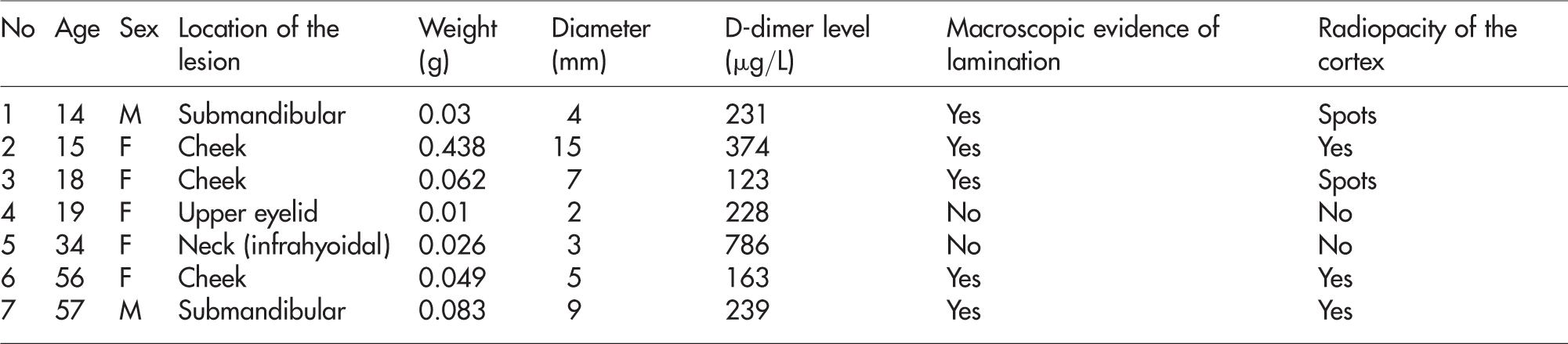
In 28 (28.6%) out of 98 patients (20 women and 8 men, median age 39 years, range 7–72 years) phleboliths were identified within VM. The diagnosis of phleboliths was made by palpation and radiographic imaging. A total of 18 (64.3%) out of 28 cases were detected by ultrasound, showing the typical sonographic feature of distal acoustic shadowing in B-mode ultrasound (Figure 1). Ten other cases of phleboliths were detected on either (or a combination of) MRI, CBTHEAD or plain X-ray. The management of patients was multimodal, as only seven (25%) patients underwent conventional surgery with removal of the phleboliths. Preoperative coagulation analysis in this group showed that the D-dimer level was elevated in 5/7 cases (Table 1; reference normal level 0–200 µg/L). Coincidence of other conditions explaining the elevation of D-dimer levels was excluded. Fibrinogen level and platelet count were within normal limits in these cases. The indication for surgery was aesthetic disfigurement and swelling conditions caused by the VM in five patients, and was excruciating local pain from the phleboliths in two other patients (case series nos. 2 and 6). These two patients suffered from chronic pain over several months despite previous treatment with low-molecular-weight heparin (LMWH) and anti-inflammatory drugs. The treatment modality of the remaining cases consisted of therapy with Nd:YAG laser in 12 patients, and sclerotherapy with bleomycin in four patients. The other five patients were only observed.
B-mode sonographic image of a phlebolith with typical distal acoustic shadowing Demographic parameters, location of the venous malformations in the head and neck, weight, diameter and the mineral composition of the identified phleboliths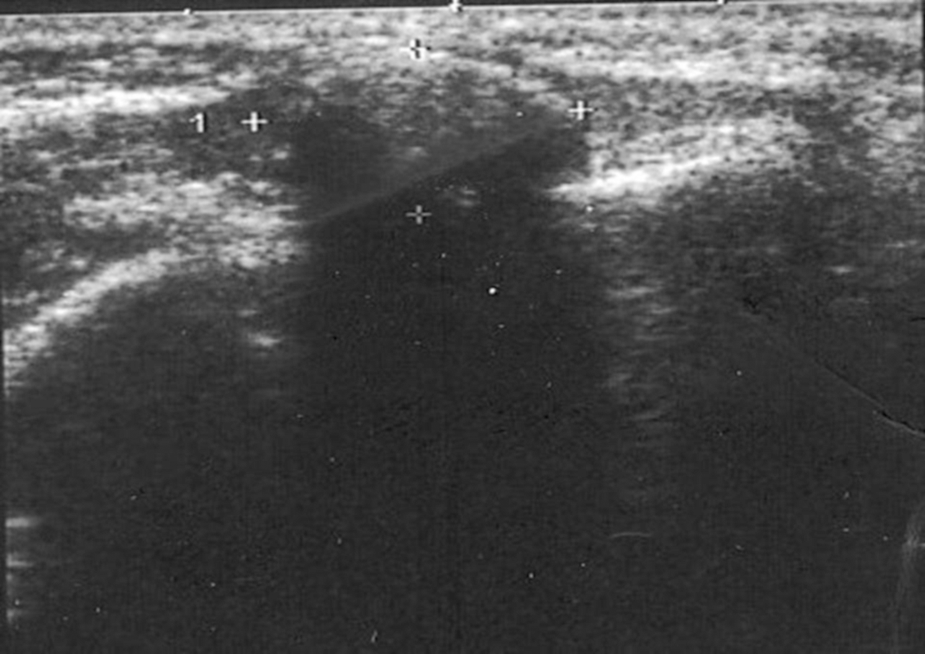
The surgical procedure consisted of open-neck surgery in three, removal of phleboliths of the cheek via intraoral approach in two; lateral parotidectomy and excision of a VM with blepharoplasty of the upper eyelid in one case each. Surgery of the parotid and buccal area included monitoring of the facial nerve. Haemostasis during surgery was achieved using conventional local measures such as coagulation and ligation. Haemodynamically significant intra- or postoperative bleedings did not occur. Symptom relief was reported by all patients after surgery. Remaining or recurrent phleboliths were evident in 3/7 cases in follow-up visits including ultrasound examination within a period of 10, 11 and 25 months, respectively. These patients were free from severe symptoms.
From these seven patients who underwent conventional surgical treatment, a total of 12 phleboliths were removed. Three phleboliths were removed in one case, two in three cases and one in each of the other three cases. As mentioned above, only one phlebolith in patients with multiple phleboliths was used for the analysis by X-ray powder diffraction analysis and CBT. The features of the studied phleboliths are presented in Table 1.
The macroscopic examination revealed the evidence of comparatively loose cortex with a firm to hard core in four, and a hard cortex with presence of multiple lamellae in three cases (Figures 2 and 3, Table 1). The examination by CBT revealed a radiopaque nucleus with a radiolucent cortex in two (Figures 4a and b), evidence of some radiopaque spots in the cortex in another two (Figures 4c and d), and cortex consisting of radiopaque lamellae in three cases (Figures 4e–g). Absence of lamination and radiolucent cortex was observed in the two smallest phleboliths with a diameter of 2 and 3 mm, respectively, whereas the two largest phleboliths (diameter of 9 and 15 mm, respectively) consisted of several lamellae and showed relatively dense radiopacity of the cortex (Table 1; Figure 3).
Rinsed and dried phlebolith Showing multiple lamella of the cortex and the nucleus of a phlebolith after cutting

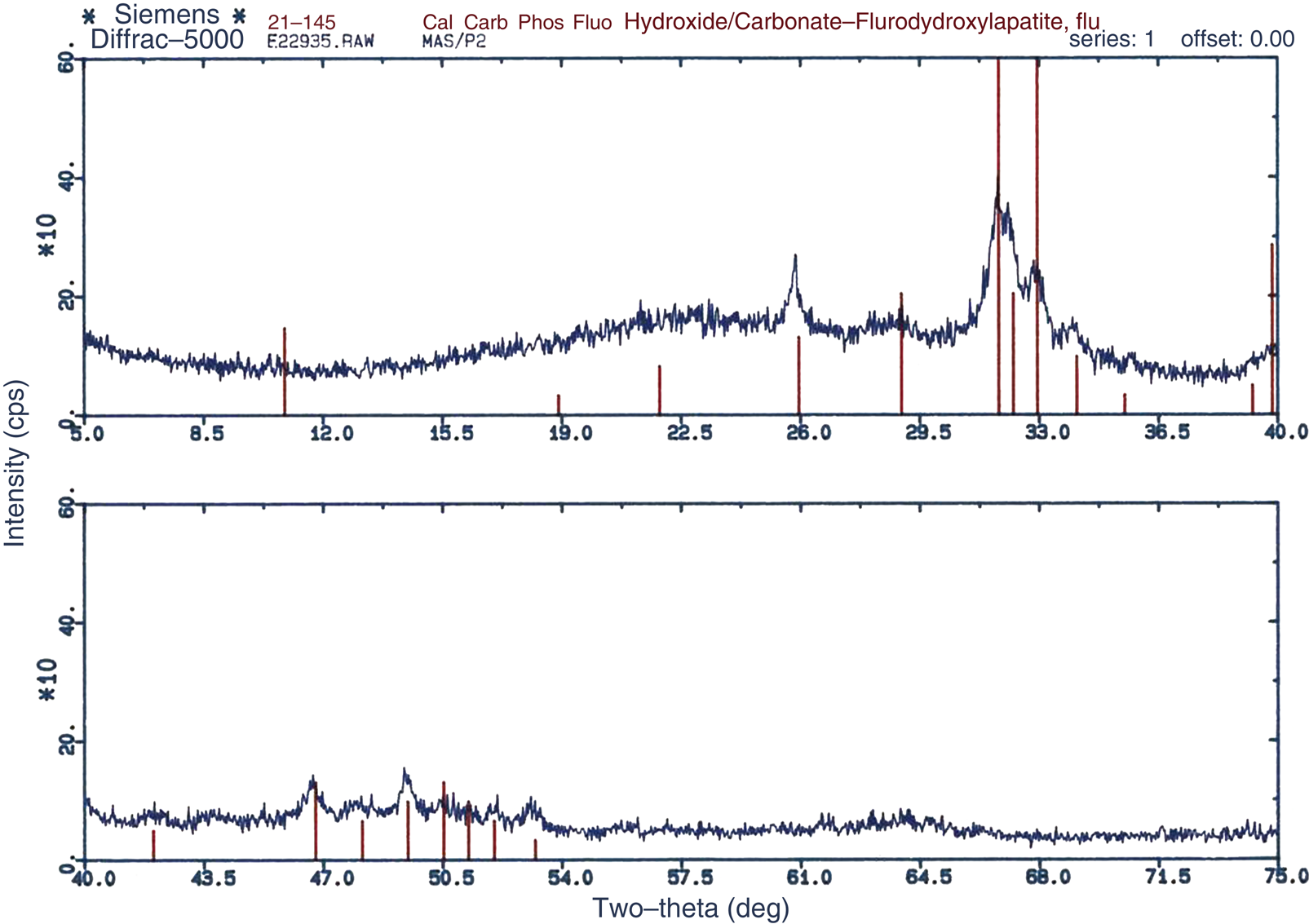
X-ray powder diffraction analysis revealed that the main constituent in the pulverized phleboliths was carbonate-fluorohydroxylapatite [Ca10 (PO4)5 CO3 (OH) F] (Figure 5). There was no observed difference in the difractograms of examined specimens, and thus differences in the mineral compositions were not found.
Phlebolith imaging on cone beam tomography showing increasing lamination and radiopacity of the cortex with increasing size X-ray diffraction pattern of a study sample containing carbonate-fluorohydroxylapatite
Discussion
Most VM in the head and neck are asymptomatic or cause only mild symptoms. Advanced cases may be associated with severe cosmetic problems, obstructions within the upper aerodigestive tract, painful inflammation and stasis, thrombosis or even bleeding.2,5,6 Phleboliths in VM of the head and neck may cause or worsen existing symptoms such as pain, swelling, tenderness and foreign body sensation.
Whenever thromboses are formed within VM they may also become calcified. 12 It is stated that 40% of VM are located in the head and neck region, of which a significant portion may be associated with phleboliths. 12 The presence of elevated D-dimers with or without decreased fibrinogen levels in patients with advanced VM is well described and gives rise to the condition known as localized intravascular coagulopathy (LIC).2,13–15 LMWH, beside anti-inflammatory drugs, are appropriate for the treatment of symptoms related to LIC, 15 but removal of phleboliths might be indicated for symptom relief in chronic cases.4,6
While severe LIC along with a strong increase in D-dimer and fibrinogen consumption is observed in large and deep VM, especially in extremities and the presence of palpable phleboliths, 14 we observed elevated D-dimer levels in 5/7 patients in whom conventional surgery was indicated; fibrinogen levels were within normal limits. This is in concordance with the results of Dompmartin and coworkers, who showed that severe LIC is more frequently observed in VM of the trunk or extremities. 14
There are individual differences in the observed size and structure of phleboliths, where the core and the cortex of a phlebolith may be made up of varied grades of calcification. This observation was demonstrated very clearly in the present study.
The pathogenesis of phleboliths, which evolved from the theory of Ribbert, is that phleboliths begin with marginal intravascular thrombus formation and later fibrosis formed around it in a lamellar fashion. His works at the beginning of the 20th century contributed siginificantly to today's understanding of the pathogenesis and morphology of phleboliths. 16 He demonstrated, that phleboliths initially arise from thrombi which are attached to the vascular walls and successively become mineralized and organized during further development under the influence of fibroblasts. The calcification progresses from the inner to the outer layers forming the multiple laminar pattern of the cortex as it increases in size. Only at a later stage of their development do external factors, such as mechanical manipulation of the lesion, cause the release of the phleboliths into the vascular lumen. Microscopically, phleboliths consist of calculi with characteristic concentric lamination.16,17 However, fibrosis in a laminar pattern develops progressively on the surface of this mineralized thrombus and also undergoes secondary calcification, and, hence, a phlebolith is formed. Calcium phosphate and calcium carbonate are deposited at the centre of the thrombus, with successive mineralization to the periphery. The repetition of this process leads to the enlargement of the phlebolith which may eventually cause symptoms in cases of persistent blood stasis as in vascular malformations.
Phleboliths in the head and neck region have been found in both children and adults.17–19 In the head and neck region, the localization of phleboliths is more common in the cheek.17–19 This is supported by the finding in this study that 42.9% of the removed phleboliths were located in the cheek. A rare location of phleboliths, in the eyelid, is also reported in this study. Most phleboliths in the VM of the head and neck region are asymptomatic, and hence require no treatment. However, stone removal may be justified when phleboliths would contribute to the exacerbation of symptoms such as pain, stasis or inflammation of the surrounding tissue. Certainly, the removal of phleboliths alone does not cure the VM. This measure should be considered alongside other options such as treatment with LMWH, sclerotherapy, laser therapy and surgical volume reduction of VM as a possible intervention.
Phlebolith has been reported as a characteristic feature of VM especially in the so-called ‘intramuscular haemangiomas’.18–21 However, the true incidence of phleboliths in the head and neck is not known as they rarely cause symptoms. Sometimes, they may cause pain, but more often are accidentally discovered on radiographic investigations.17–19 Typically, most of these phleboliths are seen on plain radiographs. 22 In particular, the distinction between phleboliths and sialoliths can be challenging.3,17,23
Phleboliths are much more commonly observed in the pelvis even without the coincidence of VM. 16 The increased stasis of blood within the lumen of vessels within the pelvis more than in the head and neck region might have accounted for this observation.
In the present study, we reported on phleboliths in 28 cases of VM of the head and neck. These were discovered on radiological imaging and accounted for 28.6% of all VM in this cohort. Only 30.4% of those cases presented with chronic pain and had surgical therapy with removal of the phleboliths. All have varied sizes, numbers, weights and differential thickness ratios of the nucleus to cortex of the phlebolith. Phleboliths are usually of varied sizes and the ratio of their core or nucleus to the cortex is different from one phlebolith to another. When they are wet, their cores are only distinguishable from the periphery by colour and texture. However, when they are dried, their cores usually have holes and appear yellowish to greyish in colour. The phleboliths, which had a diameter between 2 and 15 mm, were light yellowish to grey in colour with a hard consistency, and their shapes ranged from oval to round.
The histopathological description of the decalcified stone was published by Anneroth et al. 24 They found small and large needle-shaped spaces in the matrix that contained some erythrocytes and fibroblasts. We did not set out to find out the histopathological make-up of phleboliths in this study as we do not expect a deviation from the known and published literature. The structural analysis by CBT showed that increasing radiopacity of the cortex of the phleboliths was observed in larger specimens. The powder X-ray microdiffraction of all specimens exhibited only a mineral pattern Carbonate-fluorohydroxylapatite [Ca10 (PO4)5 CO3 (OH) F]. Our confirmation of the existence of calcium carbonate and calcium phosphate in this study was similar to the findings from previous reports.12,17 Similar pure apatite of the same size and orientation as crystals found in many other human hard tissues like bones, dentin and salivary calculi had been previously documented. 9 However, unlike in phleboliths, the lamination of alternating high and low mineral content is well accentuated in sialoliths. 9 In contrast to phleboliths, sialoliths also consist of other minerals such whitlockite and brushite, which is attributed to a different chemical composition of saliva. 9 The occurrence of different mineralogical compositions is also well known from renal or biliary calculi.25,26 The evidence that apatite is the main component of phleboliths leads to the assumption that mechanical destruction of these stones in vivo might be a theoretical option to achieve symptom relief. While lithotripsy is used to treat sialoliths among other human stones, 27 we could not find any reference to a clinical or experimental trial of lithotripsy of phleboliths in the head and neck.
Conclusion
Surgical removal of phleboliths might be indicated in patients with VM of the head and neck to achieve symptom relief. This measure is only one option besides other modalities such as treatment with LMWH, sclerotherapy, laser therapy and surgical resection. Phleboliths consist of apatite without any indication of differences in their chemical composition. The aetiology can therefore be attributed specifically to the underlying coagulopathy in VM (LIC). Transcutaneous lithotripsy, as applied for other apatite-containing human stones like sialoliths, might be theoretically a less invasive alternative method to treat phleboliths of the head and neck. Furthermore, this study shows in a vivid way that phleboliths show a laminar structure. Lamination and calcification progress with the increasing size of the stones. A consequent treatment of LIC with LMWH might therefore be able to prevent the formation of new and the progressive lamination and calcification of existing phleboliths. Both hypotheses must be objects of upcoming experimental and clinical investigations.