
Abstract
Ulnar artery aneurysms are uncommon lesions. They are often caused by traumatic injury to the hand. Ulnar artery aneurysms have been reported in association with multiple sports-related activities, but never secondary to a basketball injury. The following is a case presentation of an ulnar artery aneurysm likely formed secondary to repetitive basketball slam dunking with accompanying review of diagnosis and surgical treatment of ulnar artery aneurysms.
Introduction
Ulnar artery aneurysms are uncommon lesions, but are the most frequent site of arterial aneurysm of the upper extremity. They are usually caused by blunt or penetrating trauma of the hypothenar region, often due to occupational or sports-related activities that involve using the palm as a hammer. 1–14 They have never, however, been associated with basketball-related injuries. Here, we present a case of an adult patient who likely developed an ulnar artery aneurysm after repetitive forceful slam dunking when playing basketball. Ulnar artery aneurysms, including their pathogenesis, diagnosis and treatment strategies are discussed.
Case presentation
A 33-year-old, right-handed man from Bermuda, with no significant medical history, was referred to our institution with a three-year history of a pulsatile mass in the right hypothenar region. He experienced occasional tenderness in the area with pain radiating to the little finger. Three years prior to presentation, he sustained trauma to his right palm while slam dunking a basketball, and he subsequently noted this mass. The patient also reported that for years he had been dunking with improper technique by hitting the base of his palm against the basketball rim rather than the distal palm and metacarpophalangeal joints. Thus, repetitive trauma may have played a role in the formation of the lesion. Of note, his occupation as a cameraman did not involve any trauma to the hand. Initially, the mass had been diagnosed as a ganglion, but later was identified as an aneurysm with an ultrasound performed in Bermuda.
Physical examination demonstrated an 8–10 mm pulsatile mobile mass of the right proximal palm in line with the ulnar artery. The Allen test was normal with excellent refill from the ulnar and radial circulations. There was no evidence of hemorrhage, and the patient denied any neurosensory symptoms in the digits.
Magnetic resonance angiography (MRA) of the right hand demonstrated a 15 mm lobulated saccular aneurysm arising from the anterior aspect of the ulnar artery at its junction with the deep palmar arch. The distal ulnar artery and the proximal aspects of both the third and fourth palmar metacarpal arteries showed some hypoperfused segments (Figures 1a and b). Prior to surgery, Doppler signals of the digital arteries were shown to be strong, except for a reduced signal from the small finger.
(a) Axial and (b) sagittal views from magnetic resonance angiography demonstrating a 17 mm saccular aneurysm of the ulnar artery (arrow)
Operative technique
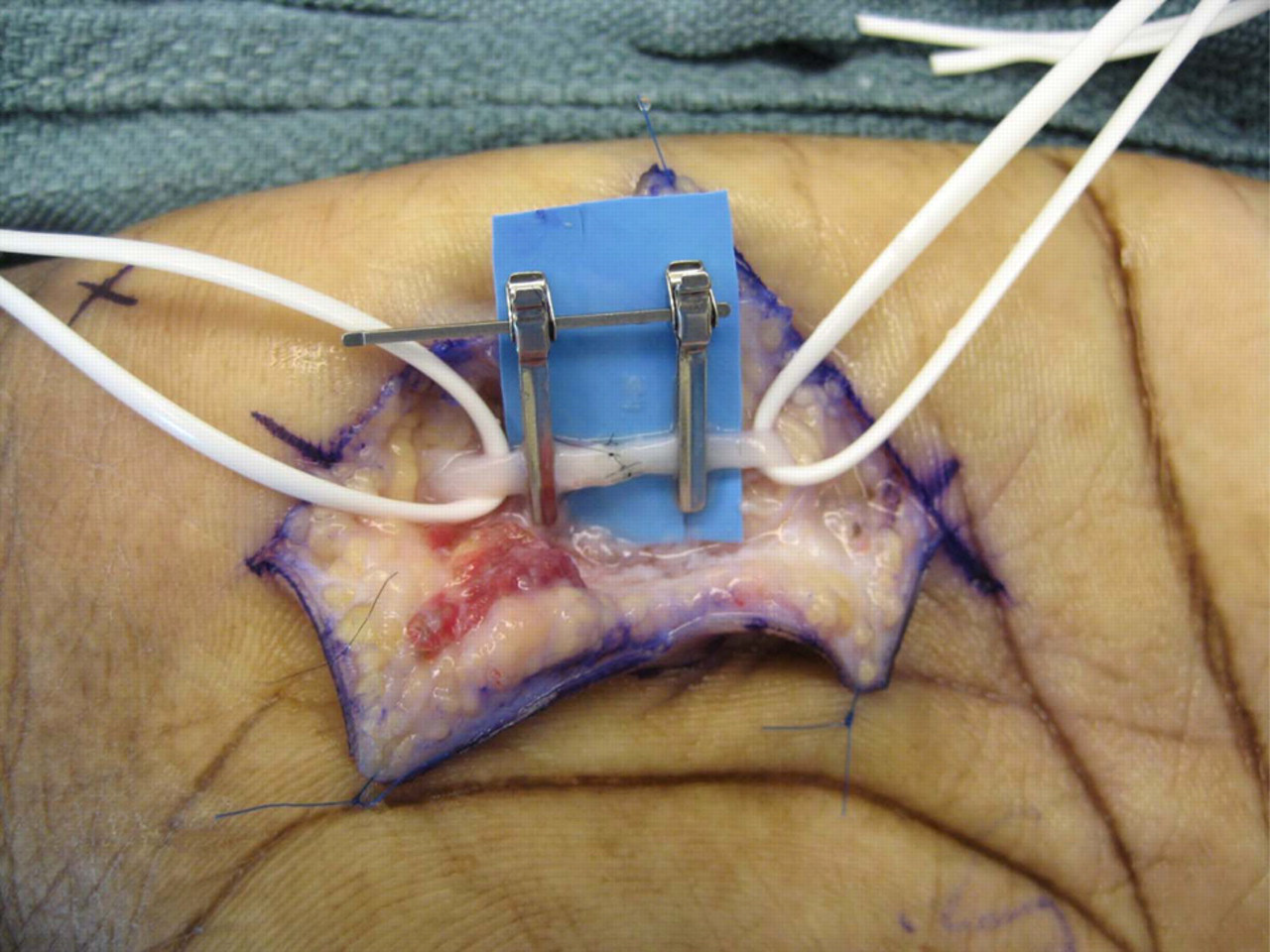
The hand and forearm were exsanguinated with an Esmarch and an arm tourniquet was inflated. This procedure may also be performed without a tourniquet by using direct arterial control instead. A zigzag incision was made over Guyon's canal, including the palpable ulnar artery aneurysm. Palmar fascia and the palmaris brevis were divided. A large ulnar artery aneurysm, 15 mm in diameter, was appreciated (Figure 2). The ulnar artery was dissected out. A double approximating clamp was placed, and the aneurysm was resected. The artery was repaired in an end-to-end fashion using interrupted 8-0 nylon using standard microsurgical technique (Figure 3). The tourniquet and vascular clamps were released and excellent flow through the anastomosis was noted. Doppler signals were exuberant in all fingers with a noted increase in the triphasic signal to the small finger.
Intraoperative ulnar artery aneurysm Repair of the ulnar artery aneurysm
The histopathology on the resected specimen showed a thrombosed aneurysm with recanalization. The patient had an uneventful postoperative course and returned to Bermuda the day after surgery. At three-year follow-up, an Allen test demonstrated fill of the ulnar and radial arteries within two seconds. The patient was asymptomatic concerning the ulnar artery repair.
Discussion
Aneurysm of the ulnar artery was first described by Guattani in 1772. 15 Distal ulnar artery aneurysms form most frequently secondary to repeated blunt trauma at the level of the hypothenar eminence in patients who use their palm for pounding, manipulating or hammering objects, or by using power tools. Ulnar artery aneurysm can be a component of hypothenar hammer syndrome (HHS), which is the formation of a traumatic lesion in the ulnar artery, either stenosis, aneurysm or arterial spasm, which produces secondary symptoms of ischemia in the fingers, usually by emboli to the digital arteries. The first case of HHS was identified by Von Rosen in 1934 in a factory worker who slammed the hypothenar aspect of his right hand against a metal bar while using a screwdriver. 1 Ulnar artery aneurysm and HHS have been seen in various sports as well, but have never been cited in a basketball player. They have been reported in hockey, 2 golf, 3 baseball, 4 badminton, 5 handball, 4 football, 6 frisbee, 4 softball, 7 weight-lifting, 8 karate, 9 hockey, 10 soccer, 1 mountain biking, 11 snowboarding 12 and tennis. 13 Single episodes of severe trauma to the palm leading to ulnar artery aneurysm have been reported in the setting of a bicycle accident 15 and a powerful hockey slapshot. 12
Ulnar artery aneurysms have also been noted to form secondary to atherosclerosis, 16 Kaposi sarcoma 17 or in the setting of a hypoplastic radial artery, with subsequent increase in blood flow through the ulnar artery. 18 Ulnar artery aneurysm formation is usually seen in adults, although cases have been reported in children, including a one-year-old boy who most likely had a congenital aneurysm. 19 It has been proposed that HHS can occur as a result of repetitive trauma to pre-existing diseased distal ulnar arteries, such as with fibromuscular dysplasia. 20
The superficial branch of the ulnar artery is particularly vulnerable after it exits Guyon's canal and before it continues deep to the palmar fascia. The short segment of the artery that runs over the hamate bone is only protected by fibers of the palmaris brevis muscle, thin fibers derived from the tendon of the flexor carpi ulnaris muscle, subcutaneous tissue and skin. 2 Classically, it has been thought that injury to the tunica media results in aneurysmal dilation, whereas injury to the intima promotes thrombus formation. 1 True aneurysms, commonly caused by blunt trauma, include all three layers of the vessel wall (intima, media, adventitia) and histologically may show a hyperplastic intimal layer and fragmentation of elastin fibers in the media. 21 Pseudoaneurysms are seen typically following penetrating trauma, and consist of fibrous tissue encapsulating a post-traumatic hematoma, which remains in continuity with arterial flow. 22
Ulnar artery aneurysm may present as an asymptomatic palpable mass at the hypothenar eminence. The mass may be tender, pulsatile and a thrill or bruit may be appreciated. 12,13,21 Neurosensory symptoms can result from compression and irritation of sensory fibers of the ulnar nerve which run deep to the artery, leading to numbness, paresthesia or pain. 13,23 Embolization of aneurysmal thrombus to the digital arteries can cause ischemia in the fingers including pain, pallor and skin ulcerations. 24,25 The Allen test may be performed preoperatively to assess ulnar and radial artery patency in the setting of ulnar artery aneurysm. 11 Frequently, the ulnar circulation is compromised. Even when the Allen test is normal, more sophisticated testing can reveal a drop in finger pressures with occlusion of the radial circulation. 21
Duplex ultrasound and color flow Doppler are useful in assessing the size of the aneurysm, and to detect the presence of a mural thrombus. 21 Conventional catheter arteriography is the diagnostic gold standard, and may demonstrate a fusiform aneurysm, obstruction of the ulnar artery, disruptions in deep and superficial palmar arches, occlusions of digital arteries and spiral corkscrew deformities. 2 However, it has a morbidity of 1–2%, and is being employed infrequently. 26 The use of multidetector computed tomography with peripheral angiography has been reported in several cases, and allows good visualization of the arterial wall and surrounding soft tissue structures. 18 There have been a few previous reports of using MRA as an additional minimally invasive modality to assess ulnar artery aneurysm. 14,26,27 MRA allows detailed information about morphology and extent of vessel injury in the ulnar artery, palmar arches and digital arteries. A drawback of MRA is that it cannot provide the flow data that the more invasive conventional catheter angiography provides. 27
The treatment of ulnar artery aneurysm most frequently involves surgical resection with or without microsurgical reconstruction of the ulnar circulation. The decision to reconstruct is largely based on the strength of the radial circulation as demonstrated by the Allen test, finger pressures during compression of the ulnar artery and intraoperative Doppler signals or digital plethysmography after exclusion of the aneurysm from the circulation. 21,22,28 Intraoperative digital plethysmography is an excellent means of demonstrating whether collateral flow from the radial circulation is adequate after aneurysm resection. If the pulse volume recording waveform is normal, resection alone may be sufficient. However, if there is blunting or flattening of the waveform, then reconstruction can be performed with primary end-to-end anastomosis. 22 The absence of back bleeding after aneurysm resection has also been used to determine whether or not to perform microsurgical reconstruction. 28 Venous interpolation can be used if there is unacceptable tension or if the defect is too large. 21 Reversed saphenous vein interposition graft 29 or ipsilateral dorsal hand vein interposition grafts 30 have been employed with success.
Follow-up for graft patency and maintenance of palmar circulation can be assessed by duplex ultrasound or color flow Doppler in the hand and fingers 2 or by MRA. 14 After resection, patients may complain of intolerance of cold temperatures. 2 Distal embolization after revascularization has also been reported. 31
In summary, we present a case of ulnar artery aneurysm which very likely formed secondary to repetitive trauma related to basketball dunking. It is crucial that ulnar artery aneurysm be part of the differential diagnosis when assessing a patient who has suffered a basketball-related hand injury. Additionally, practitioners must be prepared to counsel patients on proper basketball dunking technique that does not place the ulnar artery at risk. By bringing the distal palm and metacarpophalangeal joints against the rim in a dunk follow-through instead of the proximal hypothenar area, injury to the ulnar artery can potentially be avoided.