
Abstract
The purpose of this study was to investigate whether a protocol for permissive hypotension was feasible for patients admitted with a ruptured abdominal aortic aneurysm (RAAA). It was aimed to limit prehospital intravenous fluid administration to 500 mL and to maintain systolic blood pressure at a range of 50 to 100 mm Hg following admission, using nitrates when indicated. The diagnosis of RAAA was confirmed with sonography, and all patients with uncontrolled hypovolemic shock immediately underwent open aneurysm repair (OAR). In all other cases, computed tomographic (CT) angiography was performed to determine the eligibility for endovascular aneurysm repair (EVAR). From January 1, 2004, to December 31, 2006, 95 patients with a suspected RAAA were admitted. In 77 patients, the diagnosis of RAAA was confirmed. Twenty-eight cases (36%) underwent OAR for uncontrolled hemodynamic instability. Following CT-angiographic evaluation, 25 of the remaining 49 cases were considered unsuitable for EVAR and subsequently underwent OAR. In 24 of 77 cases (31%), the RAAA was treated with EVAR. Preoperative systolic blood pressure recordings in EVAR patients showed median values (± SD) of 98 (± 34.7) mm Hg in the emergency department and 114 (± 26.2) mm Hg in the operating theater. The desired systolic blood pressure range of 50 to 100 mm Hg was reached in 11 of 24 cases (46%). In 13 of 24 cases (54%), a systolic blood pressure higher than 100 mm Hg was recorded for a period longer than 60 minutes. The 30-day mortality was 32 of 77 (42%), with 6 of 24 (25%) in the EVAR group and 26 of 53 (49%) in the OAR group. This is the first published series of RAAA in which a protocol of permissive hypotension has been adopted. The concept appeared to be feasible in the majority of cases. Protocol violations were sparse (n = 5). Uncontrolled hypotension occurred in 36% (28 of 77) of all patients, and the desired systolic blood pressure range was achieved in 46% (11 of 24) of the EVAR patients.
Keywords
Traditionally, the treatment of hemorrhagic shock is aimed at maintaining perfusion pressure by large-volume fluid replacement. This has been proven effective in animal models of controlled hemorrhage but may not be appropriate in situations of uncontrolled blood loss, such as a ruptured abdominal aortic aneurysm (RAAA). Large-volume fluid replacement leads to hemodilution with reduction of red cell and platelet counts, as well as a decrease in the concentration of clotting factors. As a result, oxygen delivery and coagulation are compromised. Moreover, restoration of a normal blood pressure may cause thrombus dislodgment or “clot popping,” with subsequent rebleeding and entry into a vicious circle. 1 This was recognized as early as 1918 by Cannon and colleagues during the First World War. 2
In trauma care, the concept of permissive hypotension has emerged, in which low blood pressures are accepted to the extent that oxygen delivery to the brain and the myocardium is maintained until hemorrhage control is achieved by surgical means. Multiple animal studies have compared hypotensive and normotensive resuscitation in uncontrolled hemorrhage. In a systematic review of these studies, the relative risk of death with hypotensive resuscitation was calculated to be 0.37 (95% confidence interval 0.27–0.50). 3 Several randomized controlled trials conducted in level I trauma centers indicate that survival of patients submitted with uncontrolled blood loss is improved with a permissive hypotension regimen. 4–8 The clinical experience with this regimen in RAAA is limited. Lawler and Crawford both reported promising results in uncontrolled series of open RAAA repair. 9,10 Clinical data on fluid resuscitation with endovascular repair (EVAR) of RAAA are lacking.
The purpose of the present study was to investigate whether a protocol for permissive hypotension in combination with preferential EVAR is feasible for patients admitted with RAAA.
Methods
Permissive Hypotension
The study was performed in a tertiary referral center for vascular surgery. A permissive hypotension protocol for patients with suspected RAAA transported and admitted to the emergency department was initiated in 2004. None of these patients were intubated and mechanically ventilated prior to admission. In this protocol, the prehospital fluid suppletion is limited to 500 mL. Following admission, it is aimed to maintain systolic blood pressure at a range of 50 to 100 mm Hg using nitroglycerine (Nitro Pohl, Pohl Boskamp, Hohenlockstedt, Germany) when indicated at a bolus dose of 4 to 5 μg/kg followed by a continuous intravenous infusion of 0.5 to 5 μg/kg/min. Intravenous bolus injections of 50 μg fentanyl citrate are used for analgesia. Blood pressure is recorded continuously and allowed to increase in cases of loss of consciousness or signs of myocardial ischemia on the electrocardiogram.
Clinical Evaluation
The presence of an abdominal aortic aneurysm (AAA) is confirmed with sonography immediately following admission. In case of uncontrolled hypovolemic shock, patients are transported to the operating theater and immediate open aneurysm repair (OAR) is carried out. In all other cases, computed tomographic (CT) angiography (Somaton Sensation 16, Siemens, Medical Solutions, Iselin, NJ) is performed in the emergency department to determine the eligibility for EVAR. The following scan protocol is used: collimation 0.75 mm, slice thickness 1 mm, 120 kV, caredose 4D, and reference 200 mA. Intravenously, 100 mL Xenetic (Guerbet, Bloomington, IN) contrast is injected at a rate of 4 mL/s followed by saline flush. The images are transferred to a dedicated Voxar 3D (Barco, Kortrijk, Belgium) workstation for three-dimensional, multiplanar, and central luminal line reconstructions. RAAAs with an infrarenal neck length of more than 12 mm and a diameter less than 35 mm with one or two patent iliac arteries and the possibility to preserve at least one internal iliac branch are considered suitable for EVAR.
Endovascular Aneurysm Repair
Patients are operated under local or general anesthesia. A carbon fiber imaging operating table (Orthopedic Systems Inc, Union City, CA) and a mobile C-arm (OEC 9800 plus, General Electric, Fairfield, CT) are used for fluoroscopy. Access is gained through bilateral 8 mm transverse groin incisions, and standard bifurcated Zenith endografts (Cook, Bloomington, IL) are employed. Aortic occlusion balloons are not used routinely. Following a completion angiogram, the arterial access sites are closed with Prostar suture devices (Abbott Laboratories, Redwood City, CA). No heparin is used, and patients are put on an antiplatelet agent from the first postoperative day.
Results
From January 1, 2004, until December 1, 2006, 95 patients with a suspected RAAA were admitted. In 18 patients, the diagnosis of RAAA was rejected following sonography, and in 77 patients, the diagnosis was confirmed during CT-angiography or laparotomy. Twenty-eight cases (36%) underwent OAR for uncontrolled hemodynamic instability. Of the remaining 49 cases, 25 were considered unsuitable for EVAR and subsequently underwent open repair. In 24 of 77 cases (31%), the RAAA was treated with EVAR (Table 1). In the same period, 83 of 117 (71%) asymptomatic AAAs and 23 of 38 (61%) symptomatic nonruptured AAAs were treated with EVAR at our institution.
Distribution of Open and Endovascular Aneurysm Repair in 77 Patients with a Ruptured Abdominal Aortic Aneurysm with or without Uncontrolled Hemodynamic Instability
EVAR = endovascular aneurysm repair; OAR = open aneurysm repair.
Preoperative systolic blood pressure recordings in EVAR patients showed median values (± SD) of 98 (± 34.7) mm Hg in the emergency department and 114 (± 26.2) in the operating theater (Figure 1). The desired systolic blood pressure range of 50 to 100 mm Hg was reached in 11 of 24 cases (46%). In 13 of 24 cases (54%), a systolic blood pressure higher than 100 mm Hg was recorded for a period longer than 60 minutes. Protocol violations occurred in five cases, in which fluids in excess of 500 mL were administered unindicated in the preadmission phase.
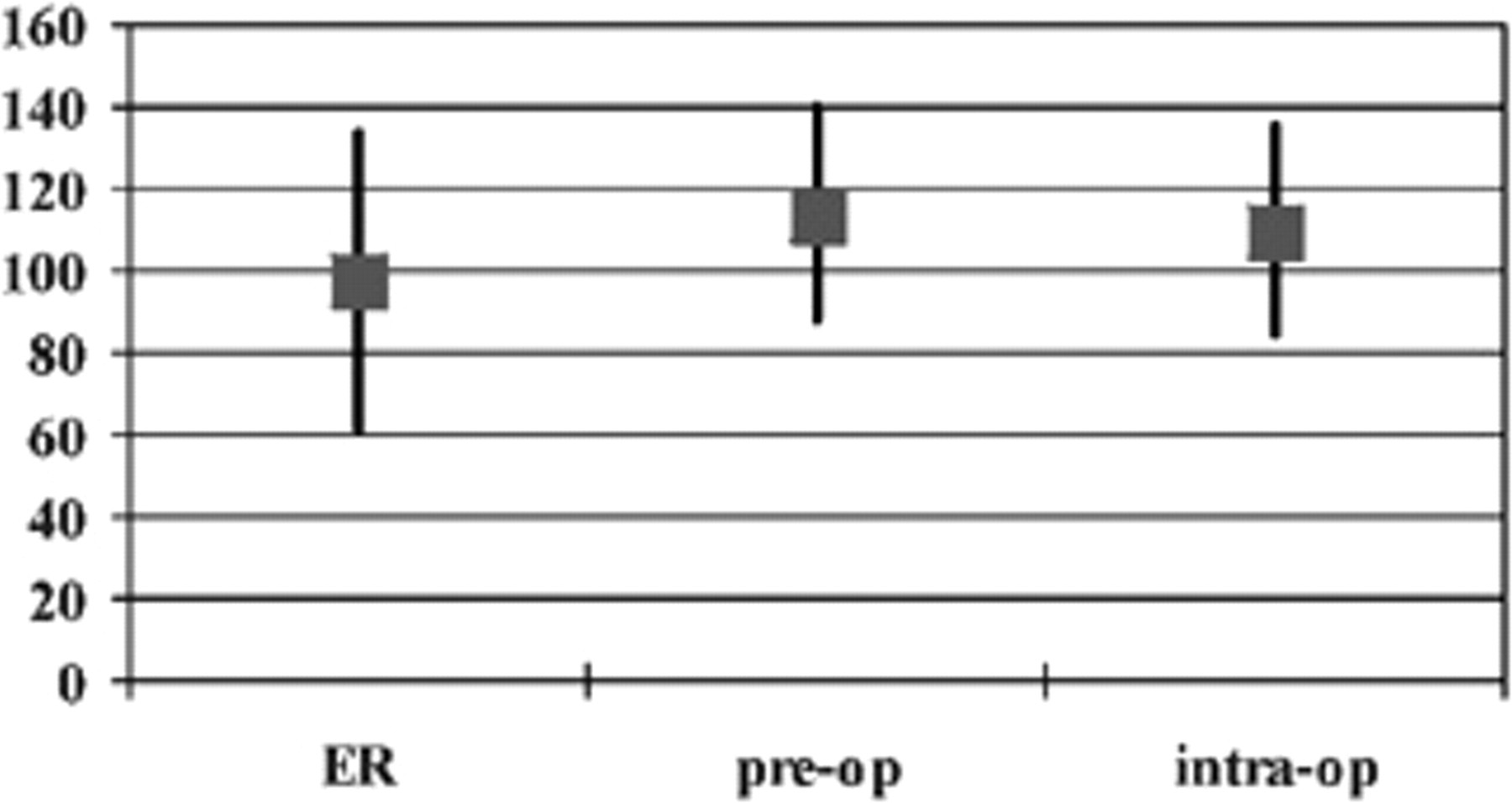
Median (± standard deviation) of systolic blood pressure (mm Hg) recordings in 24 patients with endovascular repair for ruptured abdominal aortic aneurysm. ER = during the emergency department stay; intra-op = intraoperatively; pre-op = during the preoperative phase in the operating theater.
The 30-day mortality was 32 of 77 (42%), with 6 of 24 (25%) in the EVAR group and 26 of 53 (49%) in the OAR group. In the EVAR group, intraoperative blood transfusion was required in 6 of 18 survivors and 5 of 6 nonsurvivors, with a median transfusion requirement of 2 and 7 units of packed red cells, respectively. There were no differences in preoperative systolic blood pressure between survivors and nonsurvivors in the EVAR group. In three (13%) cases, endovascular reinterventions were performed for one type 3 and two type 1 endoleaks, respectively.
Discussion
Although the application of the concept of permissive hypotension in patients with RAAA has not been investigated in a controlled, randomized fashion, this observational study shows encouraging results. With a 30-day mortality rate of 25%, it compares well with several other series of EVAR for RAAA. 11–17 Peppelenbosch and colleagues reported on a series of 49 patients with RAAA who were treated with a Talent (Medtronic, Santa Rosa, CA) aortouni-iliac device, with a 30-day mortality rate of 35%. 13 Mehta and colleagues reported an 18% 30-day mortality rate in a series of 40 EVARs for RAAA in which bifurcated and aortouni-iliac devices were used. 14 Coppi and colleagues used a variety of mostly aortouni-iliac devices and recorded a 30-day mortality rate of 30% in 33 patients treated with EVAR and 46% in 91 patients treated with OAR. 17 In the present series, only bifurcated stent grafts were employed as it was felt that the emergency procedure should mimic the standard practice as closely as possible. The decision to use a routine percutaneous access with arterial closure devices was for the same reasons. No time is gained or lost with this approach, as in our experience, the amount of time needed for a femoral cutdown equals that of the percutaneous access with installation of closure devices.
From the present data, one cannot determine whether the outcome of patients with uncontrolled hypovolemic shock is influenced by prehospital fluid restriction. Exclusion from EVAR may have had a detrimental effect on their chances of survival. With a more aggressive approach using intraoperative aortic balloon occlusion, it may be possible to avoid open repair in a number of these patients, with subsequent prognostic improvement.
Ours is the first series in which a protocol of permissive hypotension has been adopted. The concept appeared to be feasible in the majority of cases. Uncontrolled hypotension occurred in 36% (28 of 77) of the patients with RAAA. Protocol violations were sparse (n = 5), and the desired systolic blood pressure range was achieved in 46% (11 of 24) of the EVAR patients. These preliminary observations warrant further study.
Footnotes
Presented at the VEITHsymposium, New York, NY, November 19, 2006.