
Abstract
This case report describes a rare vascular tumor (epithelioid hemangioma) in the ulnar artery of a young male patient, treated by excision and bypass grafting.
Vascular tumors are rare. This report describes a rare tumor of the ulnar artery.
Case Report
A 21-year-old right-handed male presented with a lump on the right distal forearm that had been present for 6 months. Five years previously, he had suffered bilateral distal radial fractures following a bicycle accident. Clinically, there was a tender pulsatile mass proximal to the right wrist. An Allen test demonstrated that the ulnar artery was the dominant arterial supply to the hand. A duplex scan (Figure 1) reported an ulnar artery aneurysm. At operation, there was a mass associated with the ulnar artery (Figure 2) that appeared to have an inflamed, thick wall. The lesion was excised, and an interposition reversed saphenous vein graft (harvested from the ankle region) was performed using end-to-end anastomoses. Histology reported an epithelioid hemangioma (Figure 3). At the 1-year follow-up, there was no clinical recurrence and the vein graft was functioning well.
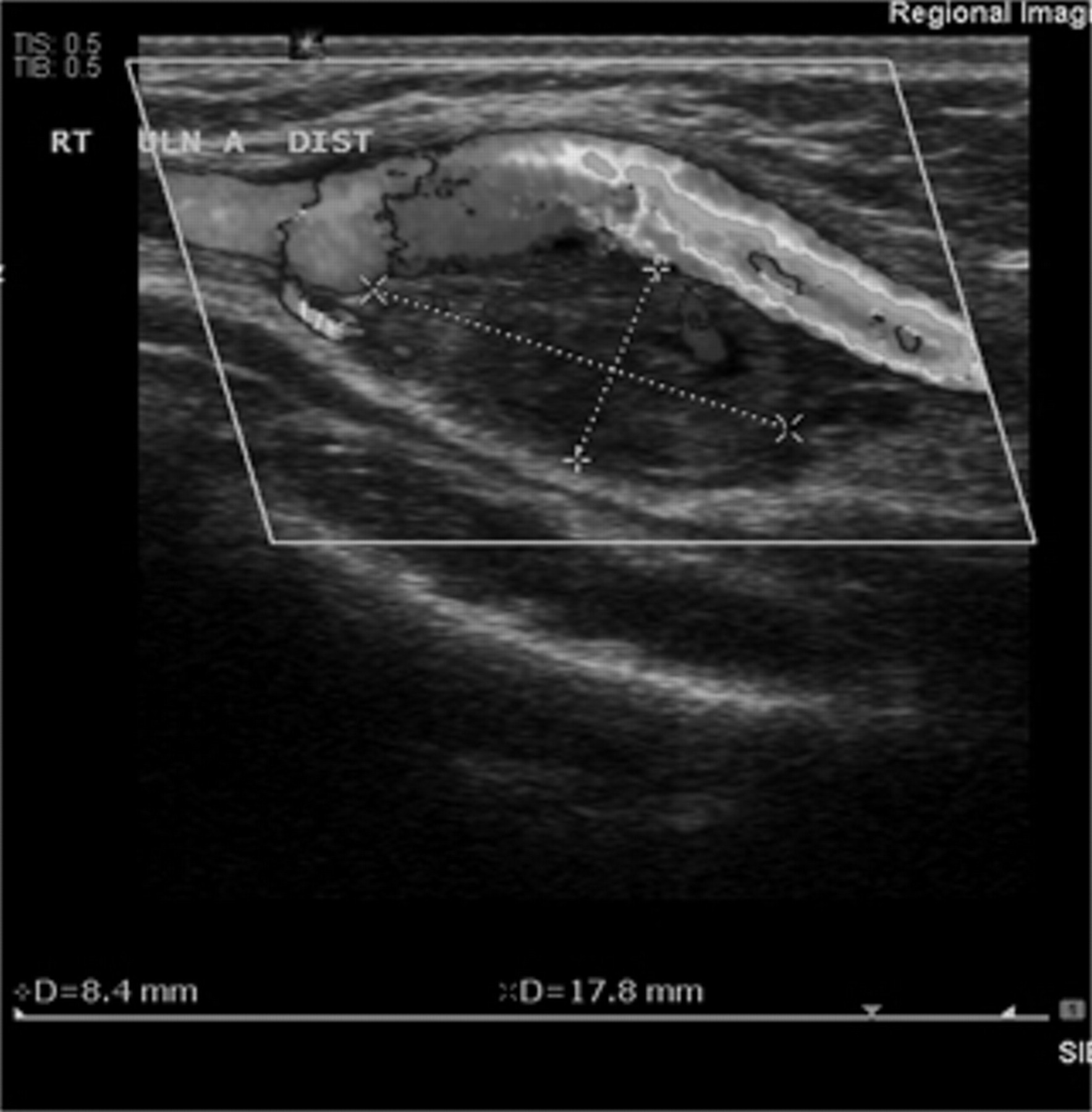
Ultrasound scan of wrist swelling reported as an ulnar artery aneurysm.

Operative photograph showing a mass arising from the right ulnar artery.
Histology slide of epithelioid hemangioma (hematoxylin-eosin stain).
Discussion
Epithelioid hemangioma is a benign vascular lesion with well-formed but often immature vessels, most of which are lined by epithelioid endothelial cells, which may protrude into the lumen. They are typically associated with a prominent inflammatory component. There is an abundant eosinophlic hyaline cytoplasm. Subcutaneous examples are usually associated with a muscular artery. They typically occur during early to midadult life (20–40 years) and affect women more than men. Most are found superficially in the head and neck, particularly around the ear. They usually start as a small, dull red, pruritic plaque that can crust, excoriate, bleed, and coalesce. Subcutaneous lesions present with a mass. Rare cases arise from a large vessel, as in this case. 1,2 Regional lymphadenopathy and blood esosinophilia can occur. This suggests an infective agent, but none has been identified. There is controversy as to whether these are reactive lesions or true neoplasia. The reactive process is supported by a predilection for superficial soft tissue sites that overlie bone, a history of trauma in 10% (as in this case), a tendency for subcutaneous examples to be well delineated and symmetric around a large vessel that may have evidence of damage, a pronounced inflammatory reaction, and some evidence supporting lesional maturation over time. Following excision, local recurrence occurs in 30%, and this suggests neoplasia as the pathology. They do not metastasize. Some lesions have been noted to regress spontaneously. 3
Given the rarity of this lesion when it involves large arteries, there is no clear consensus as to the optimal operative approach. In the case reported by Selvaraj and colleagues involving the subclavian artery, a polytetrafluoroethylene graft was used to reconstruct the artery following excision of the tumor, 1 and in the case reported by Bhat and colleagues involving the axillary artery, a reversed saphenous vein graft was used following tumor excision. 2
In retrospect, the solid component seen on the ultrasound scan (see Figure 1) is more suggestive of a vascular tumor rather than an aneurysm.
Conclusion
Although rare, vascular tumors should be considered in the differential diagnosis when a mass is associated with an artery.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.