
Abstract
The number of elderly is increasing in recent years. According to the United Nations (UN), in 2050 there will be 2.1 billion people above 60 years of age worldwide. In addition, the World Health Organization (WHO) reported that more than 1 billion people live with some form of disability, the leading causes of which are chronic diseases and accidents. Thus, many opportunities for the application of smart environments to support ubiquitous healthcare are emerging, the benefits of which may be reflected in reduced medical costs and increased convenience of patients and families. This systematic mapping study aims to identify how smart environments have been applied to support ubiquitous healthcare, what techniques and technologies are being used, and what research gaps are still left unexplored. Eight scientific repositories were used to search for papers in the area of ubiquitous healthcare, and a filtering process was used to remove bias. Of an initial sample of 1706 studies, 49 were reviewed entirely, analyzed, and categorized. Among these, we highlight those oriented to monitoring, detection, notification, and action on situations that may cause illnesses or promote the improvement of people’s health and wellness. Technologies to support ubiquitous healthcare were categorized into three groups: ambient sensors, wearables, and social robotics. These technologies have been applied most frequently to support the elderly and disabled. The diseases most commonly cited were dementia, diabetes, Alzheimer’s, autism, obesity, mental stress, sleep disorders, asthma, epilepsy and chronic diseases. We found only three papers that used prediction models. Finally, we observed a trend of using social robotics to improve the intelligence of ambient, aggregating mobility, and acting.
Introduction
According to the United Nations (UN) [69], the world’s population is aging. Most countries in the world are experiencing rapid growth in the number and proportion of the elderly in their population. The number of the elderly is expected to more than double by 2050 and more than triple by 2100, rising globally from 962 million in 2017 to 2.1 billion in 2050 and 3.1 billion in 2100. Globally, the population aged 60 or over is growing faster than all younger age groups. People in this age group face problems with living independently and are more likely to suffer from chronic diseases [10].
The elderly also suffer from known causes of morbidity and mortality, such as accidental falls, forgetting to take medications, taking incorrect medications, amnesia, and Alzheimer’s. A large proportion of the global population, especially those aged 65+, is affected by multimorbidity [53]. There is also an increase in the number of people living alone, who do not give up their autonomy and independence. Therefore, older adults prefer to stay in their homes rather than enter a healthcare institution when they need specialized care [12,29].
The World Health Organization (WHO) reported that more than 1 billion people live with disabilities around the world [74]. The most common causes of disability include chronic diseases such as diabetes, cardiovascular diseases, and cancer, and injuries due to road traffic accidents, conflicts, falls, landmines, mental impairments, congenital disabilities, malnutrition, HIV/AIDS, and other communicable diseases [73]. Besides, according to the WHO, recent years have seen an increase in the rate of occurrence of some diseases, such as diabetes, obesity, and depression, which require continuous monitoring [75].
Weiser [72] described ubiquitous computing as the concept of computers weaving “themselves into the fabric of everyday life until they are indistinguishable from it”. He believed that ubiquity is the key to providing effective, flexible, and convenient ambient environments. In this sense, the use of smartphones, wearables, and IoT sensors is proliferating [6], mainly when applied to healthcare and wellness [71], as is the development of Wireless Sensor Networks (WSN) or Body Sensor Networks (BSN), which provide support for communication between these devices on the local network or the cloud [31].
The convergence of these technologies for healthcare has given rise to the term Ubiquitous Healthcare (U-Healthcare) [54]. According to the WHO [76]: “health is a state of complete physical, mental and social well-being, and it does not merely the absence of disease or infirmity”. Thus, U-Healthcare can act in the collection, monitoring, and support for diagnosis and prevention of diseases as well as in the promotion of well-being and quality of life [71].
The broadening of the ubiquitous approach is associated with cloud computing and artificial intelligence (AI) techniques. This background promotes a Smart Environments or Ambient Intelligence (AmI) paradigm [64] such as Smart Cities [63], which offer intelligent services to users in a city. AmI enables expansion of human capacities through environments, with a computational ability of sensing and actuation in an adaptive and responsive way, thus supporting the needs and preferences of users [64].
The AmI vision may be thought of as the convergence of at least three areas of computing: ubiquitous computing, sensor network technology, and artificial intelligence. It represents the vision of a future in which unobtrusive, interconnected, adaptable, dynamic, embedded, and intelligent environments support the people inhabiting them [2,64].
Therefore, the application of the AmI paradigm to ubiquitous healthcare is one of the scenarios with the most significant potential for development, mainly because it offers the possibility of continuous support in healthcare with the aim of providing a better quality of life for people [64].
TrailCare [11] is an example of a smart environment model focused on the care of People With Disabilities (PWD). This model assists wheelchair users in an intelligent campus. This model aiming to avoid health risks. Besides this, Trailcare recommends services to promote accessibility and wellness for users. Abascal et al. [1] developed the AmbienNet as an intelligent and supportive environment model. The main purpose of this model is to examine in depth the advantages and disadvantages of pervasive supporting systems based on the paradigm of Ambient Intelligence for people with sensory, physical, cognitive limitations or older persons living independently. Vianna et al. [71] proposed a scalable model for noncommunicable diseases (NCD) prevention. The model recommends contextually and collaboratively actions to improve health users.
However, although there are several studies focused on ubiquitous care, most are specialized in data collection, monitoring, remote support, or health notification post-incident. Besides this, research gaps indicate that there are opportunities to study the prediction of health events [78].
The motivation of this paper is to understand the studies most relevant to the research area of U-Healthcare and smart environments. This work also focuses on discovering authors that are leading publications in this research area, the most relevant papers, the challenges and trends. This study presents the latest advances in the current theoretical landscape, serving to support future researches. Therefore, we present a systematic mapping study that is a compilation of filtered papers published in the last 11 years on smart environments applied to ubiquitous healthcare.
This paper is organized as follows. Section 2 presents related works and the differentials of this systematic mapping study. Section 3 describes how the mapping study was executed. The text selection process is presented in more detail in Section 3.3. Section 4 organizes the papers in the respective search questions. Section 5 exposes the threats to the validity of the work. Section 6 presents a discussion of the works found. Finally, the last section presents conclusions and future work.
Related works
This section covers existing work researching smart environments and healthcare through a search for surveys, mappings, and systematic reviews related to these themes before the beginning of systematic mapping.
The systematic literature review of IoT in healthcare, presented by [3], highlights the components of IoT architecture in healthcare, technologies in IoT, characteristics of cloud-based architecture, and challenges of IoT in healthcare. Besides this, they cited that security and interoperability issues in IoT architecture in health are still low in number. Concerning the most important effects of IoT in healthcare, these included the ability of information exchange, decreasing stay of hospitalization and healthcare costs. Ahmadi and colleagues [3] cited that the main challenges of IoT in healthcare were security and privacy issues. The related research covers only six years, between 2010 and 2016. They selected sixty papers and revealed that home healthcare service was one of the main application areas of IoT in healthcare, as mentioned in this paper. The related paper did not address population group, diseases, or predictive models for healthcare.
Liu and colleagues [48] address a systematic review related to smart homes and home health monitoring technologies for the elderly. The aim of this study was to conduct a systematic literature review to determine the levels of technology readiness among the elderly and evidence for smart homes and home-based health monitoring technologies that support aging in place for the elderly who have complex needs. An analysis of 48 of 1863 papers indicates that technology readiness for smart homes and home health monitoring technologies is low. The work focuses only on the elderly. Besides, it emphasizes the monitoring of the elderly. The related research also covers only six data sources between 2010 and 2014. However, one gap pointed by [48] is the same identified by this work: the lack of preventive and predictive works for healthcare, for example, fall prevention.
The survey on ambient intelligence in healthcare, presented by [2], cites AmI as a new paradigm in information technology aimed at empowering people’s capabilities by the means of digital environments that are sensitive, adaptive, and responsive to human needs, habits, gestures, and emotions. Acampora and colleagues [2] examine the infrastructure and technology required for achieving the vision of ambient intelligence, such as smart environments and wearable medical devices. The related work also discusses how AmI technology might support people affected by various physical or mental disabilities or chronic diseases. The work presents only qualitative analysis. Some successful case studies in the area as well as current and future challenges to draw upon possible future research paths were pointed. Acampora et al. [2] categorize technologies, algorithms, and applications related to ambient intelligence in healthcare as presented in this work.
The review of smart homes by [5] presents an overview of smart homes research as well as associated technologies. The paper describes aggregate information about sensors, multimedia devices, communication protocols, and systems that are widely used in the implementation of smart homes. Alam et al. [5] did not apply a rigorous methodology such as systematic mapping. The related paper did not present details of the criteria for the selection and classification of analyzed papers. The focus on healthcare in the related work is partial; it does not emphasize diseases supported by smart homes as presented in this work, although the taxonomy of technologies, protocols, and services presented in related work is similar to the approach used in this work.
We identified five research gaps related to (1) what are the smart environment models that support U-Healthcare, (2) how predictive computing is being used in smart environments to support U-Healthcare, (3) what are the most common diseases addressed by smart environments applied to ubiquitous healthcare, (4) what are the most common population group supported by smart environments applied to U-Healthcare, and finally (5) which techniques and technologies have been most widely used. To overcome these gaps, we aim to answer eight research questions, which are presented in the following section.
Methodology
This section describes the experimental procedures adopted to plan and run the systematic mapping study. For this, we have adopted well-established guidelines [42–44,59,60]. Section 3.1 presents the objectives and research questions investigated. Section 3.2 introduces the search strategy and digital libraries used to retrieve representative studies. Finally, Section 3.3 outlines the inclusion and exclusion criteria used to filter the retrieved studies and all procedures used to extract data from these selected studies.
This paper uses a systematic mapping methodology. This approach eliminates or significantly reduces bias when compared to single reference reviews, thus getting more reliable results [24]. This type of methodology does not discuss just the final finding but all activities related to the finding. Thus, systematic mapping collects data about locations where activity occurs and media where it was published, thereby mapping that linkage. Mapping often focuses on published papers but can be used with other media like books, newspapers, and grant proposals. The methodology consists of the execution of the following steps: (1) elaborating the research questions; (2) designing the search process; and (3) defining the criteria for filtering results.
Research questions
The research questions led this study to discover works that could be linked with smart environments and ubiquitous healthcare.
This work addresses three General Questions (GQ), three Focused Questions (FQ), and two Statistical Questions (SQ). The purpose of GQs is to understand how smart environments are supporting ubiquitous healthcare. The FQs identify how specific models are used to predict events related to diseases and what are the main groups of people and diseases reported. Lastly, SQs find statistical data about the area being studied. Table 1 presents the research questions.
Research questions
Research questions
Through a well-defined research process [59], the study used three steps: specify the search string, choose the databases to apply the search string, and obtain the results.
The first step begins by identifying the major terms and their more relevant synonyms. Search strings consist of the concatenation of terms used in search engines to retrieve potentially relevant studies in current literature. In this study, Smart Environments and Ubiquitous Healthcare were chosen as major terms. The synonyms for Smart Environments were based on terms found in [64] and for Ubiquitous Healthcare were based on a search of synonyms in [54] (see Table 2).
Search string terms
Search string terms
These terms generated the following search string: ((smart environment OR ambient intelligence OR ami OR ambient assistive living OR aal) AND (ubiquitous healthcare OR pervasive healthcare OR u-healthcare OR u-health OR p-health)).
The definition of the search string allowed to define research parameters to be used in the databases. Thus, the second step was to select relevant databases for the area of study to apply the search string. Eight research databases were used, including the Journal of Medical Internet Research (JMIR), PubMed Central, ACM Digital Library, Google Scholar, IEEE Xplore Digital Library, Science Direct, Springer Library, and Wiley Online Library (see Table 3). The first two are references for research in the health area and the remaining are renowned research databases in computer science.
Research databases
The search in ACM Digital Library required the use of advanced search features, wherein the above search string was inserted into the Edit Query field. The search process in Google Scholar was done using the query string in advanced search considering just the title for the most relevant results. In IEEE Xplore, the Command Search from the Other Search Options menu was used. In the JMIR database, the search string was inserted in the criteria field. In PubMed Central, Advanced Search was used, and the search string was inserted in both abstract and title fields. In the Science Direct repository, the query string was applied to title, abstract, and keywords. In the Springer Library, in addition to using the search string as the search query, it was required to remove papers categorized as “Preview Only”. Finally, in the Wiley database, the abstract field, in the Advanced Search option, processed the search string.
This section aims at establishing inclusion criteria (IC) and exclusion criteria (EC) used to filter potentially relevant papers retrieved from the search engine used. The IC define what should be considered for including a particular work in the sample of representative papers. The EC define the requirements to remove works deemed inadequate to answer the research questions. Table 4 shows the IC and EC.
List of Inclusion Criteria (IC) and Exclusion Criteria (EC)
List of Inclusion Criteria (IC) and Exclusion Criteria (EC)
The inclusion and exclusion criteria help the process of filtering to get the most relevant studies and eliminating any noise generated in the search. The studies obtained from the search process were filtered, removing impurities that did not fit in the inclusion criteria IC1, IC2, and IC3. The remaining papers were stored in a spreadsheet, where the texts were organized in specific tags for each research database.
The next step was to analyze the papers by title and abstract. Papers were combined in the same folder and any duplicate papers were removed. The papers [18] and [26] were added by heuristic, as they are relevant to this study even if not found through the search process. The next filter was based on the first two passes of a three-pass approach [41]. The first pass is a quick scan and consists of: (1) reading the title, abstract, and introduction; (2) reading just the section and subsection headings, but ignoring everything else; (3) glancing at the mathematical content (if any) to determine the underlying theoretical foundations; and (4) reading the conclusions.
The second pass consists of looking carefully at figures, diagrams, and other illustrations in the paper, paying particular attention to graphs. Finally, the remaining papers were filtered analyzing the full text and observing the exclusion criteria of EC4, EC5, and EC6. Figure 1 presents the filtering process, with IC and EC applied at each step.
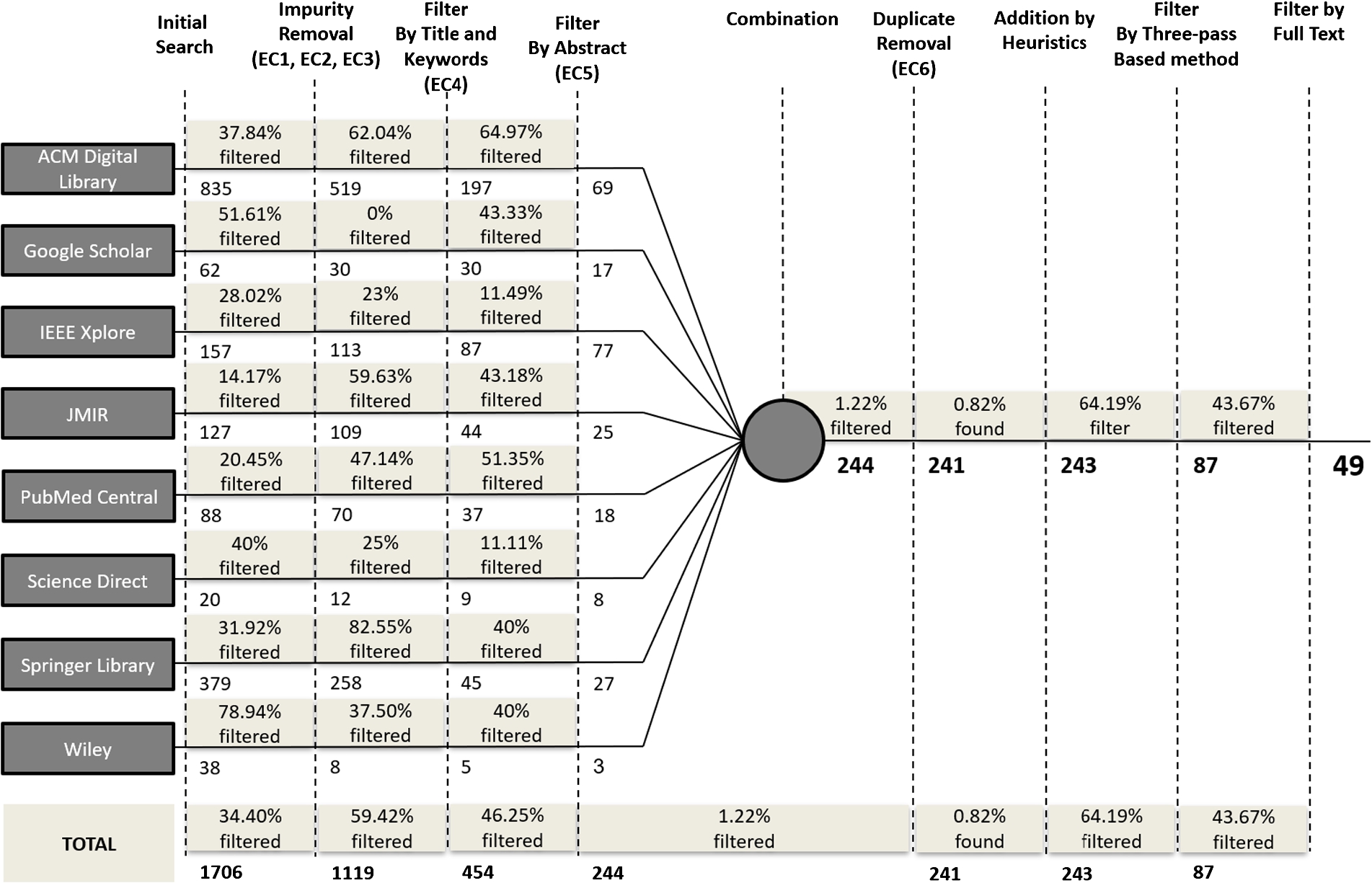
Steps of the filtering process.
Science Direct database gave fewer, only 20 papers, but assertive papers related to the search string, constituting 40% of the filtered results. The IEEE database results constituted 49.04% of the filtered results; although it gave more results when compared to the other databases using this search string, it included many unrelated papers. After filtering the results, the best papers of Google Scholar were contained in the other databases used. The filtering process showed many papers studying only telemedicine or apps for patient interaction; these were removed from the study.
This section presents the results obtained from the primary studies. Table 5 lists the reviewed papers and shows their characteristics, presenting an overview of the data gathered. The specific tables also are used to provide particular approaches. Each table focuses on presenting data about a particular research question. The findings of each research question are presented in the subsequent subsections.
How are smart environments being applied to ubiquitous healthcare? (GQ1)
This question investigates the practical application of smart environments to U-Healthcare. Figure 2 shows the frequency of application of smart environments to U-Healthcare from three perspectives: scope, type of classification, and technology. As can be seen on the left side of Fig. 2, the status awareness of situations based on the detection of objects, people, or activities are the most frequent application of selected papers. Besides this, the right side of Fig. 2 shows that Ambient Sensor (AS) for monitoring is the primary use of technologies according to selected papers.
Selected papers
Selected papers

Application of smart environments in U-healthcare.
Table 6 shows the distribution of primary studies by type of classification. The data indicate that status awareness is the most used, being present in 17 primary studies (34.69%, 17/49). Support system is the second most used, corresponding to 28.57% (14/49) of primary studies. Other applications were adopted by different studies, such as robotic assistance (18.36%, 9/49) and activity recognition system (18.36%, 9/49).
Monitoring is considered a fundamental part of the smart environment [4]; this feature is present as a base requirement in all primary papers. This feature realizes data collection from environmental sensors, wearables (by biosignals reading) or via social robot sensing. In some cases, in addition to monitoring, the selected paper also addresses detection, notification, or actuation in the environment, favoring the user in their healthcare needs. We classified the papers researched as follows: (1) monitoring only: some cases where data is only collected from the user’s body or the environment; (2) detection: projects that approach the activity recognition system, detecting the occurrence or change of patterns of user behavior in the environment. Some works cited Activity Daily Living (ADL), a general term to daily events, such as sleeping, feeding, and watching TV; (3) notification: most common situation, where messages or alerts are sent to the user, their family or caregivers, such as for elderly falls or risky situations. We have identified some works that act as a persuasive system (Deen, 2015); (4) notification/acting: in papers selected in this scope, in addition to the notification also perform some action in a smart environment, modifying variables of ambient. For example, some of these works implemented reminders to alert the user about the consumption of medicine or water; (5) acting: generally associated with a robot that acts in the environment supporting the user or actively modifying the ambient.
Table 7 shows the distribution of primary studies by scope. The data indicate that detection is the most used, being present in 15 primary studies (30.61%, 15/49). The results indicate that most of the researches focus on monitoring, detection, and notification of health incidents and health events, such as, a system that sends an automatic alert to the elderly that forgot some task in their daily routine.
Distribution of primary studies by type of classification
Distribution of primary studies by scope
This general question aims to discuss the main technologies employed in the primary papers to provide smart environments that support U-Healthcare. We classified these technologies into three macro groups: ambient sensors, wearables, and service robots. Table 8 displays the data obtained in the research on technologies and techniques used. The results show that a significant part of the primary studies adopts only the ambient sensor (36.73%, 18/49) to support U-Healthcare in smart environments. Furthermore, only two works used technology fully, i.e., ambient sensor + wearable + service robot (4.08%, 2/49).
Distribution of primary studies by technology
Distribution of primary studies by technology
Ambient sensors are devices and sensors installed in an environment that collect data such as luminosity, temperature, presence, pressure, and humidity. In this sense, AmI uses a set of domotic sensors for monitoring of environmental conditions. Additionally, we found works that encompass a smart toilet [35], a smart kitchen [56], and a smart bed [36]. Moreover, we identified a proposal using a set of infrared sensors that detect a person’s presence in a given portion of a home, their posture, and also their movement [51]. The technologies applied were PIR, RFID, beacons, pressure sensor, temperature sensor, luminosity sensor, humidity sensor, Kinect sensors, smart TV, acoustic sensor, voice recognition, cameras for image recognition, IP camera, projectors, smartphone/tablet, desktop computer, laptop, embedded sensors on smartphone/tablet such as accelerator, nurse sticker, shower sensor, toilet sensor, bed sensor, and room sensor. For communication, we found that mainly the protocols used were Bluetooth (BT), Bluetooth Low Energy (BLE), WiFi, 3G/4G, and ZigBee.
Wearables are IoT devices that can measure physiological data like pulse heart rate, detect posture, fall of equipped person, and their activity rate. Sensors used are electroencephalography (EEG), electrocardiography (ECG), electromyography (EMG), blood temperature, skin temperature, body temperature, pulse rate, respiration, blood pressure, etc. The primary papers cited the followed gadgets and healthcare devices that work isolated or via BSN/BAN [23]: smart garment/smartwatch [61] and smart wheelchair [38].
Service robots are service, assistive, or social robots that collaborate with a smart environment, providing additional services to the user. The robots typically aggregate actions to the ambient, besides sensing, making them more intelligent. Primary papers showed an arm-robotic manipulator to support object collection [38], specialized service robots with visual-based human motion detection, voice recognition, and dialogue management [51], assistant robots for walking support and in the bathroom [57], and KuBo [49].
Table 9 presents the distribution of technologies of primary papers grouped by their respective impact factor (IF). The table shows five groups of impact factors. The results indicate that 40.8% of selected papers were published in vehicles with IF score lower than 1. Furthermore, more than 40% had IF indicators higher than 2. Service robots and wearable are the predominant technology in venues with a higher impact factor, resulting in 8.16% of selected papers which IF score is higher than 4.
Distribution of technologies in % of primary papers by group of impact factor (IF)
The analysis of related works allowed understanding the modeling strategies used in AmI. Table 10 shows that 46.94% (23/49) of papers approach models to support U-Healthcare. The other 53.06% (26/49) did not cite the use of a model to address U-Healthcare in a smart environment.
Distribution of primary studies by the citation of model
Distribution of primary studies by the citation of model
This question aimed to identify the diseases mostly cited. As presented in Table 11, dementia, Alzheimer’s, and diabetes were the most cited. Chronic diseases in general, sleep disorders, mental stress, obesity, asthma, epilepsy and autism also were cited at least once. Approximately 67% of primary papers did not name one specific disease.
Distribution of primary studies by disease
Distribution of primary studies by disease
This question aimed to identify the target users of the systematic review conducted. Table 12 shows that the elderly were the most mentioned age group. People With Disabilities (PWD) and children are also treated in some papers due to their vulnerability.
Distribution of primary studies by age group
Distribution of primary studies by age group
This question investigates what papers used a predictive model. The aim is to identify projects that not only monitor but also notify especially anticipated risks and events favorable to healthcare. Among the 49 primary papers, only 3 (6.12%) focus on some predictive aspects of U-Healthcare in smart environments.
Alkhomsan et al. [8] addressed that the success of providing smart healthcare services in Ambient Assisted Living (AAL) mostly depends on a useful prediction of situations in the environment. They concluded that situation awareness in AAL is used to determine environment smartness by perceiving information related to the surroundings and human behavioral changes. In the AAL environment, there are plenty of ways to collect data about its inhabitants, such as through cameras, microphones, and other sensors. According to Alkhomsan and colleagues [8], the collected data are complicated enough to go for efficient processing in perceiving the situation. Their paper gives an overview of the current research results using multimodal data analysis in the AAL environment to improve the living environment of the elderly and attempts to bring efficiency in complex event processing for real-time situational awareness. Finally, the paper considers multimodal sensing for the detection of current situations as well as to predict future situations using decision tree and association analysis algorithms. To illustrate the proposed approach, they considered elderly activity recognition in the AAL environment.
Jung and Yoon [39] published a paper that measures human physiological changes from different body parts to quantify human mental stress levels by using multimodal biosensors. By integrating these physiological responses, they generate bio-index and rules for the prediction of mental statuses, such as tension, healthy, and relaxed. They also develop an inspection service middleware for analyzing health parameters such as EEG, ECG, oxygen saturation (SpO2), blood pressure (BP), and respiration rate (RR). In this service middleware, they use a multi-level assessment model for analyzing mental stress level that consists of three steps: classification, reasoning, and decision making. The classification of datasets from biosensors is enabled by fuzzy logic and a support vector machine (SVM) algorithm. The reasoning uses the decision tree model and a random forest algorithm to classify the mental stress level from the health parameters. Finally, they propose a prediction model to make a decision for the wellness contents by using Expectation-Maximization (EM).
Lin et al. [47] wrote a paper that shows an assistive environment like a smart domestic space based on pervasive computing to support the elderly and disabled. They highlight that, unlike sensors, which can only provide passive monitoring, a robot can be an active element to improve the quality of life for humans. An active service robot in an assistive environment was proposed to help humans in case of an emergency. It works on a hierarchical, partially observable Markov decision process (POMDP). The multimodal observation series are used in the decision and evaluation process. This proposal is used in an emergency response system (ERS) to deal with emergencies, such as elderly falls or diseases. The purpose of multimodal observations is to guarantee the precision of the report for emergencies. Four observation sources were introduced in the paper: vision recognition, voice recognition, physical input devices, and external systems. According to Lin and colleagues [47], for each observation source, there are two observation series. Multiple information sources give the agent more opportunities to learn from the real world and to make more reasonable predictions, evaluations, and decisions.
Where have the researches been published? (SQ1)
This question seeks to reveal where the primary studies have been published, which may be taken as a basis for future submissions. Table 13 shows the distribution of primary papers by venue. There is a predominance of publications in a journal (59.18%, 29/49). The remaining studies have been published in conferences (20/49, 40.82%). Researchers have chosen PETRA as the main venue to publish their research results.
Conferences (C) and Journals (J) where papers have been published
Conferences (C) and Journals (J) where papers have been published
The publications were grouped according to the year of publication. Figure 3 presents the distribution of papers.
In the past decade, an average of 4.6 papers on AmI applied to U-Healthcare have been published per year. We can highlight PETRA as the conference with the most significant number of publications in 2009 (14.28%, 7/49). In 2010, the number of papers published fell from 8 to 0, representing a significant drop. Only two papers were published in 2013, whereas no papers were published in either 2008 or 2010. We observed a growing trend during 2010-2012, 2013-2015, and 2016-2019. Most studies (83.67%, 41/49) were published from 2011 to August of 2019. A peak of 8 papers in 2009 and 2018 was observed.
Threats to validity
Like any other systematic mapping study, this work has some shortcomings that could be affected by the results found. Shortcomings can occur as a result of decisions made during systematic mapping. Eight databases which are known in the academic world for their relevance in the areas of computer science and healthcare were selected to guarantee better research results, thus mitigating the shortcomings of the databases.
There is a risk of the filtering process restricting the papers in such a way that relevant works may get removed. To mitigate this risk, the filtering process was based on Petersen technique [59]. Papers were analyzed and selected without a reviewer, which may have affected the filtering results. To mitigate this risk, we used revision processes already used by other authors [33].
Papers dealing with the following themes were excluded: (1) apps that focus only on individual monitoring; (2) apps for monitoring or control of diabetes, depression, and insomnia; (3) passive telemonitoring/telemedicine, without a smart environment approach; (4) smartphones/tablets used only as reminder assistants; (5) papers that focus in HCI/UX issues only; (6) projects related to education; (7) papers that approach cloud computing view only; (8) projects that deal with security or surveillance; and (9) papers that feature gadgets and IoT solutions isolated.
Discussion
This paper focused on the application of smart environments to U-Healthcare and can guide future works about the use of technology in improving people’s health and in promoting wellness.
The analysis of the 49 filtered papers concluded that technologies such as wearables, environment sensors, and robots are used to aid in healthcare. Some works used smartphones and tablets as an integrated resource because of the variety of sensors and their integration with wearables. Smartphones generally were used to record biological data from users or to communicate with the cloud.
This mapping study presented the many ways that technology is being used to support healthcare, such as monitoring only, detection, notification, notification, and acting, or acting only. Papers in which actions were the main scope were associated with the use of social robots that interact with the environment, helping people in case of an emergency, as presented by [51] or improving user experience and wellness as presented by [38] and [57]. However, we observed a default healthcare flow that follows the path of monitoring, detection, and notification.
Although the studies did not indicate any specific disease as the most frequently cited in the 49 papers researched, we categorized eleven of the works under known illness, such as dementia, diabetes, Alzheimer’s, autism, obesity, mental stress, sleep disorders, and chronic diseases. AmI has proven to be an adequate solution to monitor and assist in the treatment of diseases that require continuous monitoring.
The most studied population group was that of the elderly; about 53% of cases researched focus on this age range. Doukas et al. [27,28] proposed a model to assist the elderly in case of accidental falls. Valero et al. [70] discussed a proposal that helps the elderly in ordinary activities of day to day living. The second most cited group was of PWD. AAL was proposed to reduce the difficulties faced by PWD in everyday life. For example, Papageorgiou et al. [57] presented a model to support people with motor impairment in bathroom use. Huang et al. [35] studied the reading of physiological data for health monitoring. Finally, children also were reported by Tentori et al. [68] as an aided group with the application of smart homes that supports the monitoring of children’s healthcare indicators.
Analyzing the filtering process presented in Fig. 1 and the SQ1 presented in Fig. 3, the most accurate database performing the query string was ACM, and the less accurate databases were JMIR and Wiley. Also, the ACM, Springer, PMC, and IEEE libraries contributed to around 83,65% of papers selected.

Distribution of primary studies over the past years.
We identified some technical characteristics as the use of video monitoring with image recognition. This feature generally was used for recognition of falls in indoor environments. Another reality is the use of sensors embedded in smartphones due to their low cost and widespread immediate use. In the environment, use of non-contact sensors or non-invasive sensors (“sensitiveness”) are recommended. The use of Digital Reminder Systems (DRS) are cited for functionality, especially activity reminders.
In the perspective of general opportunities involving economic and technical motivations, the following are seven reasons to use the approach of smart environments applied to U-Healthcare: (1) the accelerated aging of the global population; (2) the increased and multiplicity of chronic diseases; (3) the growing demand for health services; (4) the possibility of delivery of continuous support services; (5) the support of specialized and personalized U-Healthcare services; (6) the interconnection between hospitals, emergency services, caregivers, and robots; (7) and reducing hospitalization and medical costs.
General and technical criteria indicate ten challenges: (1) data fusion from multimodal sensing is still a significant challenge that needs to be overcome; (2) the methods of detection and classification of events have gaps that need to be supplanted; (3) the HCI needs to be improved in many aspects to be more natural and non-intrusive; (4) many aspects of security must be addressed to reduce security vulnerabilities; (5) preventive and predictive models, predicting routines and habits, are approaches that could improve effectively smart environments; (6) detection of generic human activities and behaviors continues to be a challenge; (7) many strategies of indoor location have evolved, such as image, acoustics, magnetic field, and wireless signal, but are not fully satisfactory; (8) dealing with large data volumes (big data) and real-time processing capacity continue to be another significant challenge; (9) artificial intelligence techniques need to be enhanced; (10) and ethical and social issues, as well as human factors and their particularities, need to be addressed.
The main trend identified for smart environments was the aggregation of assistive robots for support in AmI. These social robots can act to prevent or support people in specific circumstances or in case of an emergency. Additionally, we identified an opportunity to implement self-learning in systems, in addition to alerts/notifications as currently proposed. Finally, the use of physiological data in addition to default data could contribute to the development of more accurate preventive and predictive solutions for U-Healthcare.
This systematic mapping study presented the latest in the application of smart environments to U-Healthcare. The paper also presented the different ways in which technology is used to support many diseases and population groups. The review of the works published in the last decade may provide initial insights into interventions based on smart environments applied to U-Healthcare and help identify the shortcomings in this area of study.
The primary aim of researchers in the application of smart environments was to find models related to U-Healthcare, especially predictive models. However, only three of the reviewed papers documented that AmI effectively supports people’s U-Healthcare with a predictive approach. The most frequent scope of projects includes monitoring, detection, and notification. We observed that the development of predictive models, as a step forward to context-sensitive computing, presents itself as a great opportunity in the AmI fields for U-Healthcare.
This study contributed to the analysis of journals and conferences for potential future publication of papers resulting from further studies in AmI. In the industrial context, there are several opportunities for companies to produce technologies applied to disease prevention and maintenance or improvement of people’s health using devices and resources that are increasingly present in daily life.
The main gap found during the evaluation of works was the application of the paradigm of actuation in smart environments, in addition to monitoring and detection events only. A proactive view could improve the support of healthcare. Some papers presented as a solution, according to this placement, the use of service robots. Finally, this paper serves as a reference source for AmI models for U-Healthcare, to support decision making and to inform future research.
Footnotes
Acknowledgements
The authors wish to acknowledge that this work was supported by FAPERGS (Foundation for the Supporting of Research in the State of Rio Grande do Sul –