
Abstract
Introduction
Currently, with life pace accelerated, poor diet habits developed, psychological burden enhanced and many other factors, the incidence of coronary heart disease, atherosclerosis and other cardiovascular cerebrovascular diseases has been increased year by year, which are serious threat to human health. After the 1990s, minimally invasive treating vascular diseases technology began to be widely used, which had been recognized as one of the most effective means to treat cardiovascular and cerebrovascular diseases. In recent years, for vascular lesions and different requirements, researchers and clinicians are needed to jointly develop vascular stents with superior performance. Charles Dotter and Melvin Judkins [1] first proposed the concept of endovascular therapy in 1964. Gruentzig [2] conducted the first case of percutaneous transluminal coronary angioplasty in 1977. Then Sigwart et al. [3] first reported the self-expanding coronary metal stents and the first balloon-expandable stent was used in the human body in 1987. Then the clinical application has been widely developed. As an implant material, various properties of the stents are needed to meet high demands, especially the excellent blood compatibility and corrosion resistance. However, the latest achievements in this field are basically derived from abroad and involve less domestic. In order to provide references for the researchers, the metal stent materials were reviewed and prospected.
Vascular stent introduction
The vascular stent is a metal mesh, which can re-open the narrow lesion artery or vascular to support artery or blood vessel wall after implanted into the human arteries, thus reducing vascular recoil and remodeling, eliminating the clogging of blood vessels and achieving blood flow [4]. Such stents are mainly for the renal artery stent, coronary artery stent and aorta stent, shown in Fig. 1.
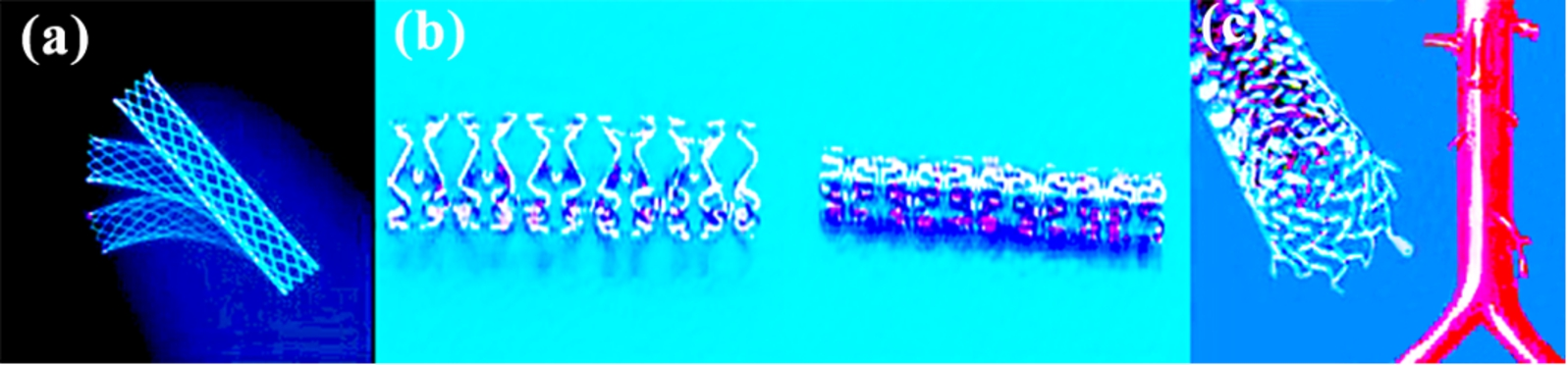
(a) Renal artery stent, (b) coronary artery stent, (c) aorta stent. (Colors are visible in the online version of the article;
The material of vascular stent must contain good biocompatibility because of its direct contact with the body, which does not cause adverse effects on human tissue, including tissue compatibility, blood compatibility and immune response. Of course, it must be ensured that the performance and longevity were not reduced because of its direct contact with biological systems.
Mechanical properties
The vascular stent must contain good mechanical properties after implanted into the body, because it needs to withstand the pressure from the blood vessels and blood, mainly including: (1) appropriate surface coverage; (2) good radial strength; (3) appropriate stretch; (4) suitable longitudinal shortening; (5) good flexibility; (6) radiopacity; (7) preventing restenosis [5].
Corrosion resistance
The main problem of metal materials in the biomedical aspects is the corrosion. Corrosion will not only reduce the mechanical properties of the metal stents and easily lead to breakage but also release the harmful metal ions which will affect the normal response of the cells after they enter into the body tissue. Meanwhile, corrosion products and corrosion currents can also cause the body metabolism disorder. Therefore, corrosion resistance to body fluids is critical in the medical application of metal material. Of course, the biodegradable metal stent is another matter due to its corrosion resistance to metals.
Blood compatibility
Metal ions released amount in the blood before and after DLC films deposited in the stents
Metal ions released amount in the blood before and after DLC films deposited in the stents
Note: NC-no film, DLC-film unit: ng per 8 mL human plasma.
The properties of vascular stents depend on stent materials. In recent years, for many types of vascular lesions and requirements, researchers and clinicians are working together to develop vascular stents with superior performance. The stents made of different materials possess different efficacies in the animals and clinical trials and developing new stent materials has become a focus.
316L stainless steel stent
The main components of 316L stainless steel (Fe–18Cr–14Ni–2.5Mo) are iron, chromium, nickel, molybdenum and manganese, etc.; the microstructure is austenitic; the density is 7.75–8.9 g/cm3; the melting is 1385–1415°C. American ASTMF4 Committee confirmed 316L stainless steel as the standardization material of surgical implantation in 1960, which is currently the most common stent material. Currently, 316L stainless steel stents have been used in a wide range of clinical, mainly for coronary stents, aortic vascular stents and peripheral vascular stents.
Gutensohn et al. [6] deposited diamond-like carbon (DLC) film on the surface of 316L stainless steel stent by plasma induced cold deposition technique, forming DLC-316L stainless steel stent. Then they were placed in the blood and soaking time was 24 h, 96 h. The results showed that the amount of released Ni, Cr, Mn, Mo and other metal ions was significantly reduced, shown in Table 1. The dissolution amount of metal ions was reduced to almost unmeasured, which showed that DLC film could improve blood compatibility of metal stent. And Jones et al. [7] obtained similar results. Therefore, DLC, SiC, TiN, TiC, etc. films deposited on the surface of metal stents can greatly improve the corrosion resistance, reduce the surface free energy, reduce ion dissolution and improve their blood compatibility. However, whether the films are firmly adhered or not is needed for further research.
Super-elastic nickel–titanium alloy stent
Nitinol is an intermetal compound synthesized by 50% nickel and 50% titanium, which is also known as nickel–titanium shape memory alloy. Nitinol density is 6.45 g/cm3 and melting point is 1240–1310°C. There are austenitic and martensite in the crystal structure, and they can be transformed into each other in the certain conditions. Thus nitinol is able to show super-elasticity and shape memory effect. Because of the excellent performance, nickel–titanium alloy has been used on a large scale in clinical practice, especially in terms of vascular stents. According to the shapes, nitinol stents can be roughly divided into four categories: (A) spring-like nitinol stent (early product); (B) skirted Z-stent (single); (C) balloon-expandable stent (such as Palmaz Blue); (D) self-inflation stent (such as Wallstent).
In 1983, Dotter et al. and Cragg et al. first reported the use of thermal memory self-expanding stents made of nickel–titanium alloy and then used in human arteries [8,9]. After 1990, nitinol stents made a good therapeutic effect. Nitinol, currently, has been widely used in clinical practice, such as Precise carotid stent (Crodis company), Neuroforr intracranial stent (Boston company) and Memotherm peripheral vascular stent (Bard company), etc.
In recent years, nitinol stents have been studied very popularly abroad. Nitinol stents are mainly for the treatment of pipeline stenosis. First, the filamentous nickel–titanium alloy is made a mesh or a spiral shape at a certain high temperature. Then it is placed in a narrow place and prop up the blood vessels, achieving maintaining patency. Although TiO2 passivation layer on the stent surface made corrosion resistance of nitinol alloy superior than stainless steel, corrosion phenomenon still existed and nickel ions would still be dissoluted [10]. Even though the dissolution amount of nickel ions is less than stainless steel, the long-term presence of nickel ions is harmful to humans. Therefore, corrosion resistance to the blood of nitinol is still needed further improvement to reduce harmful ions such as nickel ion dissolution.
Cobalt-based alloy stent (Co–Cr–Ni–Mo–Mn)
In the biomedical field, cobalt-based alloy is mainly composed of cobalt, chromium, nickel, manganese, molybdenum, etc. Its density is 8.3–9.15 g/cm3 and melting point is 1290–1425°C. Now cobalt-based alloys mainly include Elgiloy, MP305 and L605, etc. Currently, cobalt-based alloys have been used in clinical practice, mainly including coronary stents, aortic vascular stents, carotid stents, peripheral vascular stents, thoracic and abdominal aortic stents, etc. And it may be the best choice of material in coronary drug-eluting stents.
In early 1937, cobalt-based alloy was first used as the clinical material of implant human, which is now widely used as a stent material in clinical practice, such as new Wallstent self-expanding stents and covered self-expanding stents. In 2002, Driver, a employee of Medtronic, first used cobalt-based balloon-expandable stent for coronary blood vessels. Therefore, cobalt-based alloy is considered to be a better platform for the future stent, because it is superior to conventional 316L stainless steel in term of some significant performance.
Magnesium alloy stent
The clinic application of magnesium stents
The clinic application of magnesium stents
Magnesium alloy coronary stent was first successfully applied to human clinical trials in 2004. Erbel et al. [15] put 71 magnesium alloy stents into 63 patients. The stents were degraded after four months, indicating the success of magnesium alloys as biodegradable stents. However, the density of magnesium alloy is too small, resulting in poor developing effect. It will be guided to locate by ultrasound during the surgery, causing surgery difficulty and expense increase. Shanghai Jiao Tong University has developed a new bio-medical magnesium alloy JDBM (Mg–Nd–Zn–Zr) [16], with deformation up to 20–35% at room temperature. Its corrosion resistance and mechanical properties can satisfy the degradation requirement so as to be used for biodegradable cardiovascular stents.

Different states with the times of magnesium alloy stents implanted in the animals.
However, in the application, the rapid degradation of magnesium alloy stents will lead stents themselves to collapse, blocking blood vessels, making serious consequences. Figure 2 shows the biodegradable characteristics of magnesium alloy in different periods. How to improve corrosion resistance and increase service time in the blood vessels became a serious problem. Currently, a small amount of magnesium alloy coronary stent clinical trials have been conducted, but it has been not widely used in clinical practice.
Animal experiment of pure iron stents
Animal experiment of pure iron stents
Hermawan et al. [19] prepared Fe–35Mn alloy by powder metallurgy. Because of the excellent mechanical properties, corrosion resistance and magnetic properties, this alloy has promising prospects as biodegradable stents. In 2006, Peuster et al. [20] made cardiovascular stent using 99.5% iron and did animal experiments (pig) for 1–12 months. Compared with 316L stainless steel stent, iron-based alloy stent was demonstrated with good biocompatibility and safety. In 2008, Waksman et al. [18] implanted iron-based alloy stent into porcine coronary artery. 28 days later, the iron-based alloy stent begun to corrode compared with the cobalt–chromium alloy stent. But there was no obstruction, thrombosis and inflammation. Although iron-based alloy stents have many advantages, there are still some disadvantages, such as pitting slowing degradation speed and poor compatibility. Therefore, the key of new iron-based alloy stent development is to find new corrosion ways to obtain suitable degradation rate and improve clinical value.
Tantalum has high corrosion resistance. Its density is 16.65 g/cm3 and melting point is 1996°C. According to the hardness, tantalum can be divided into soft state, semi-soft state and hard state. Currently, tantalum metal is mainly used in coronary stents, peripheral vascular stents and esophageal stents. However, it is rarely used alone in clinical practice, but to participate in the composition of other stents.
In 1988, the Strecker balloon expandable stent woven by tantalum wire was used in clinical practice. Then there were different designs of tantalum wire stents, such as Fontaine stents and Wiktor stents, etc. But because of its radial strength limit, currently, tantalum has been not widely used in clinical practice [21].
Other metal stents
Currently, there are also other metals which have been used as stents, including gold, platinum, iridium, palladium and other precious metals. Since these metal stents mostly exhibit alkaline, they can be magnetized in a magnetic field. Researchers use this feature to research and manufacture magnetic metal stents. Animal experiments showed that the magnetic field can be anti-oxidation, anti-inflammatory, promote endothelial repair and inhibit vascular smooth muscle cell proliferation. Therefore, these advantages make magnetic metal stents have entered vigorous development stage.
Conclusion
With the rapid development of stent materials and preparation techniques, the functions of the stents have been gradually improved. Although metal stents have been widely used in clinical practice, there are still many problems to be solved, especially to improve mechanical properties and biological activity. Strong immune rejection is also a problem and vascular tissue engineering has been committed to immunogenicity processing of vessels for a long time. Therefore, it will be a significant direction for future material research to treat surface modification, further improve the biocompatibility, reduce the thrombosis and completely eliminate the rejection and vascular restenosis. In addition, the stent materials should be developed toward controllable degradation and special features in the future.
Footnotes
Acknowledgements
The author would like to acknowledge National Natural Science Foundation (50830106) for the financial support for the study. Special thanks to Prof. Dr. Dezeng Fan and Xiaolu Pang on his valuable comments on the study.