
Abstract
BACKGROUND:
The Band Pull-Apart (BPA) exercise is used to strengthen the periscapular muscles. It was recently stated that the lower extremity and trunk movements should be included in the shoulder rehabilitation programs to optimize an effective energy transfer throughout the kinetic chain.
OBJECTIVE:
The aim of this study is to investigate the effects of kinetic chain based BPA exercise on the muscle activations of the sternocleidomasteideous (SCM) and the trapezius muscles in individuals with and without forward head posture (FHP).
METHODS:
Eighteen individuals with FHP and 18 individuals without FHP were included. Photographic measurements were made to identify individuals with FHP. The muscle activations of SCM, Upper Trapezius (UT), Middle Trapezius (MT), and Lower Trapezius (LT) were measured with surface EMG. BPA exercise was performed in the standing, unipedal standing, squat, unipedal squat, and Bulgarian split squat (BSS).
RESULTS:
There was no Group
CONCLUSION:
Performing the BPA exercise in the squat position is suggested in cases where lower SCM and UT muscle activation, lower UT/MT, and UT/LT ratios and higher MT and LT muscle activations are needed for individuals with and without FHP.
Introduction
Forward head posture (FHP) is described as the protrusion of the head in the sagittal plane, in positioning the head anterior to the trunk [1], and is considered a common postural deformity regarding musculoskeletal balance abnormalities [2]. Since the shoulder girdle and neck regions share many muscles, changes in head and neck alignment also result in changes in the activation of muscles of the shoulder girdle [3]. It is known that a very small change in the forward position of the head can increase the load on the musculoskeletal system, which in turn increases the activity of the upper extremity muscles [4]. It has been reported that the primary problem in FHP is shortening and hyperactivation of the sternocleideomasteideus (SCM) muscle [5]. It is also stated that the upper trapezius (UT) muscle becomes overactive to overcome the increased tension of the levator scapula due to FHP [6]. Furthermore, it is related to the weakness of the deep cervical flexor muscles and middle thoracic scapular retractor muscles (e.g., middle trapezius (MT), lower trapezius (LT), rhomboids and serratus anterior (SA)) [7]. Therapeutic exercises, including postural training, stretching of tight muscles, and strengthening of weak muscles, are crucial for treating FHP [8]. Elastic Band Pull-Apart (BPA) exercise is frequently used in rehabilitation to strengthen periscapular muscles such as trapezius and rhomboids [9, 10]. Fukunaga et al. found that when performed with a neutral grip, this exercise activated the UT (53%), the MT (55.8%), and LT (39.5%) muscles [9]. In addition, recent guidelines highlight the significance of integrating shoulder girdle exercises into a global functional kinetic chain for multiple reasons [11, 12]. The kinetic chain plays an important role in energy and force transfer from one part of the body to another [13]. Since the upper extremity performance relies not only on a single shoulder joint but also on the sequential activation of the kinetic chain from the bottom to top, clinicians suggest that the kinetic chain should be included in shoulder rehabilitation [14]. Shoulder rehabilitation using the kinetic chain instead of a strengthening exercise focused on a single shoulder joint can be more effective in restoring the normal movement of the scapula without an excessive load on the rotator cuff or periscapular muscles [13]. It is stated in previous studies that scapular muscle activation is altered when the upper body position [14], and lower body position/exercise position are changed [11, 14, 15, 16], or the trunk movements are included [17, 18, 19]. In a systematic review published in 2020 aiming to investigate the effects of the kinetic chain on shoulder rehabilitation, authors stated that integrating the kinetic chain into the shoulder exercises might increase axioscapular muscle recruitment, and leads to lower muscle ratios of the trapezius, and decrease the demand on the rotator cuff muscles [20]. De Mey et al. compared eight different lower extremity conditions and showed that trapezius muscle activity during squat on the contralateral leg was higher than in the traditional sitting position [11]. A challenge to the kinetic chain is often added to complicate the training program in the clinic [16]. With this study, we wanted to evaluate whether adding this difficulty affected the demand of the scapular muscles. Studies have mentioned the importance of the kinetic chain and it has been stated that the change in the demands of the muscles should be investigated when kinetic chain exercises are added to upper extremity exercises commonly used in the clinic. Therefore, this study aimed to determine whether the BPA exercise performed in different lower extremity positions affects the SCM and trapezius muscle activity in individuals with and without FHP. The effect of incorporating the kinetic chain on trapezius muscle activation during the BPA exercise, an exercise frequently used in the clinic, has not been investigated. The use of the lower extremity to encourage scapular movement has been stated to be ideal as it mimics the kinetic chain sequence [21]. We think that understanding the type of activation change that occurs in the scapular muscles with the addition of exercises in different lower extremity positions in individuals with and without FHP will guide us in exercise selection in the clinic. It was hypothesized that when there is a change in the demand of the kinetic chain, there will be a difference in scapular muscle activity during these exercises.
Materials and methods
Study design
A case-control study design was used to evaluate muscle activation during kinetic chain based exercises in individuals with and without FHP. On the first day of the study, the craniovertebral angle (CVA) values of the participants were evaluated by using photographic posture analysis. After the analysis, participants were divided into two groups according to their CVA values. The BPA exercise was performed in five different lower extremity positions to determine the effects of the kinetic chain based exercises. Muscle activations of the participants during the kinetic chain based exercises were evaluated with surface electromyography (EMG). The 8-channel surface EMG Noraxon MiniDTS, which is a non-invasive method to measure muscle activation, was used to evaluate the activation of the SCM, UT, MT and LT muscles. The EMG data were normalized by using the maximal voluntary isometric contractions (MVIC) measurements for all muscles. EMG activity for each muscle was recorded while the participants were performing the MVIC. MVIC and muscle activations of the participants during exercises were measured on two different evaluation sessions. At the end of the first evaluation, the locations of the electrodes were marked with a permanent pen so that the electrodes could be placed at the same spot in the following evaluations.
Participants
The study was conducted at Gazi University, Faculty of Health Sciences, Department of Physiotherapy and Rehabilitation, Unit of Athlete Health. The required permission was granted from the Gazi University Ethical Commission (No. E-77082166-302.08.01-419695; Reference No. 2022-935; Date: 22.03.2022). All participants were informed about the study beforehand. All individuals who agreed to participate in the study signed informed consent forms.
Individuals between the ages of 18 and 35 who did not have any surgery, pain in the spine or the upper extremity and the lower extremity, fracture anamnesis of the related body parts, musculoskeletal system pathology in the upper extremity for the past 6 weeks, could perform the exercises properly, and agreed to participate in the study were included [3, 14, 19, 22]. Individuals who suffered from neck, shoulder, and knee pain for the last 6 weeks, had surgery on the related parts, had functional or structural scoliosis, had any neurological, rheumatological, or systemic disorder, had a body mass index (BMI) greater than 30 kg/m2 and participation in any sport activities were excluded [6, 11, 13]. For the non-FHP group, individuals who had a postural deformity regarding the neck and shoulder were also excluded. Undergraduate and graduate students and research assistants of the Gazi University, Physiotherapy and Rehabilitation Department were contacted through social media groups and the inclusion criteria were explained. They were invited to the clinic on the planned day and time to determine their eligibility for inclusion criteria and whether they had FHP. Initially, 62 asymptomatic individuals who agreed to participate were invited to determine their eligibility for inclusion. As a result, the study was performed with 18 participants each in the FHP and non-FHP group. The post hoc power analysis of the study was calculated using G*Power 3.1.9.7 program [23]. As a result of the calculation performed using the research data with a total sample size of 36, the partial eta squared value of the research was calculated as 0.041 (“Group
Assessment of forward head posture
Individuals were digitally imaged in the standing position from the lateral side to determine if they had FHP. The photogrammetry is considered the “gold standard” for assessing head position [24], and is reliable and valid compared to radiological measurements [25, 26]. A digital camera (Logitech c922 Pro Stream Webcam) was placed on a stable tripod without any rotation or tilt, at a 1.5-meter distance from the posture chart. The bottom of the camera was adjusted to the shoulder height of the participants [27, 28]. For the FHP evaluation, participants were asked to wear clothes with their neck region exposed to enable palpation of the spinous process of the 7th cervical vertebra and tragus, and two marker bands were placed at these anatomical locations. The marking tapes were placed on the 7th cervical vertebra and tragus following palpation by two experienced physiotherapists. Participants were guided to stand in a relaxed position with their feet shoulder-length apart, ensuring their lower extremities shared their body weight symmetrically [28]. Prior to taking a photo, participants were instructed to perform neck flexion and extension three times before positioning themselves in a resting period. Then, they were again instructed to look straight ahead in their natural relaxed position. Three measurements were performed by the same investigators. After the measurements, photographs were analyzed with the Image-J program [29]. The CVA, described as the angle between the horizontal line passing through the spinous process of the 7th cervical vertebra and the line extending from the tragus of the ear to the 7th vertical vertebra, was measured [27] (Fig. 1). The mean value of the three measurements was recorded as the CVA. A CVA of below 50∘ was considered as a FHP [1].
Measurement of craniovertebral angle.
Kinetic chain based exercises. A: Standing; B: Unipedal standing; C: Squat; D: Unipedal squat; E: Bulgarian split squat.
Descriptions of exercise positions
The BPA exercise was performed in; the standing, unipedal standing, squat, unipedal squat and in the Bulgarian split squat (BSS) position to identify the effects of kinetic chain based exercises (Fig. 2). In unipedal positions, the exercise was performed on the dominant leg. The dominant extremity was determined by questioning the leg they used to kick a ball [30]. These positions were chosen because they are the most used exercise positions in the clinic and in studies evaluating the effect of kinetic chain based exercises in the literature. An explanation of the lower extremity positions used during exercises is given in Table 1.
The feet positions of the participants were marked on the ground with chalk to make sure that the positions stayed the same throughout the trial. The knee angle during the exercises was measured with a goniometer. The angle of knee flexion during the exercises was adjusted with the help of a band placed between two parallel columns.
Exercises were performed with a resistance band. In order to standardize the resistance of the elastic band used in the exercises, the OMNI perceived exertion scale was used [31]. The instruction of the exercises and the amount of resistance of the elastic band were determined on a different day from the EMG measurement. In addition, all subjects were given time to practice the exercise before the test. The quality of exercise performance was checked and, if necessary, was corrected by an experienced physiotherapist. All subjects were instructed by the same researcher. The instructions were standardized with verbal cues to avoid variability between the instructions given to the subjects. The amount of the resistance was determined only in the standing position and not in other exercise positions separately due to the possibility of the occurrence of fatigue. Yellow, red, green, blue, black, silver, and gold elastic bands (Thera-Band®, Hygenic Corp., Akron, OH, USA) were used in this study. Participants were instructed to repeat the exercise 10 times with the lightest elastic band. Subsequently, they were asked to increase the resistance level of the band until the effort perceived by them was rated between the scores of 6 and 8 (somewhat hard and hard) on a scale of 0 to 10 (0: extremely easy; 10: extremely hard) [32].
Evaluation of the muscle activation
The 8-channel surface EMG Noraxon MiniDTS system (Noraxon, USA, Inc, Scottsdale, AZ, USA), which is a non-invasive method to measure muscle activation, was used to evaluate the activation of the SCM, UT, MT and LT muscles. The device has a common-mode rejection ratio greater than 100 Db, a differential input impedance greater than 100 Mohm, and a 1500–3000 Hz sampling rate for each channel. Disposable and self-adhesive Ag/AgCl electrodes (3M Red Dot 2271) usable for only surface EMG applications were used to record the EMG signals. It was made sure that the distance between the centers of the two electrodes was not more than 2 cm. A synchronized video shooting at 50 frames per second was made to determine the different phases of the exercises. The skin was shaved, scrubbed with soft sandpaper, and cleaned with 70% isopropyl alcohol to minimize skin impedance. Following the skin preparation, electrodes were placed in a parallel orientation to the determined muscle fibers in accordance with the European Recommendations for Surface Electromyography (SENIAM) [33]. For the SCM; electrodes were located 1/3 on the distance between the sternal notch and the mastoid process [34]; for the UT, electrodes were located midway between the 7th cervical vertebra and the acromion (in the direction of C7 and the acromion); for the MT, electrodes were located midway between the medial border of the scapula and the 3rd thoracic vertebra (in the direction of the acromion and T5) and for the LT, electrodes were located 2/3 on the line from the trigonum spinae to the 8th thoracic vertebra (in the direction of acromion and T8) [35]. After the placement of the electrodes, the skin impedance was measured with an ohmmeter to make sure that it was
EMG Measurement during exercise
EMG data were collected from the dominant side of the participants. The dominant upper extremity was determined by questioning the hand they used for writing [37]. Participants performed the BPA exercise first without resistance and then with an elastic band resistance to get familiar with the exercise. The exercise order was assigned by the randomization made on
Normalizing EMG data
The EMG data were normalized by using the MVIC measurements for SCM, UT, MT and LT respectively. EMG activity for each muscle was recorded while the participants were performing the MVIC. All MVIC measurements were performed by the same investigator. After the familiarization trials of every MVIC test, three repetitions of the MVIC measurements, each lasting for 5 seconds, were performed. There were 30-second resting periods between every MVIC measurement and 1-minute resting periods between the repetitions [38, 39]. Throughout the measurements, participants were given the same standardized verbal stimulations by the same investigator to ensure that they displayed their maximum effort [39]. The MVIC measurement of the SCM muscle was performed in the supine position. Participants’ necks were flexed [34], and the resistance was applied with a stable belt over the forehead [40]. The MVIC measurements of the UT were performed in a sitting position in which the participants’ shoulders were 125∘ flexed, and the resistance was applied with a stable belt over the elbow. For the MT MVIC measurements, participants were asked to take the prone-T thumbs-up position. Resistance was applied vertically with a stable belt over the elbow joint while the shoulders were 90∘ horizontally abducted, and externally rotated. As for the MVIC measurements of the LT, participants were positioned in prone lying with their dominant arms 140∘ abducted and externally rotated. Resistance was applied over the elbow joint using a stable belt parallel to the LT fibers and against flexion [35].
EMG data analysis
Raw EMG signals were visually checked for the possibility of electrocardiac artifact risk. EMG signals were 20 Hz high-pass and 450 Hz low-pass filtered. Then, the root mean square (RMS) of the signals in a 100-millisecond time period was filtered. The signals recorded during the MVIC measurements were analyzed, and the highest value among the three repetitions was recorded. Synchronized video recordings were watched for analysis, and the pull apart, stationary, and return phases of the exercises were identified. Only the stationary phase data were used for the analysis. Later on, EMG signals in the stationary phase of the exercises were divided by the mean MVIC values for normalization. The data were used as % MVIC for the statistical analysis. To simplify the interpretation of the EMG data, the muscle activations were categorized as low (
Flowchart of the study.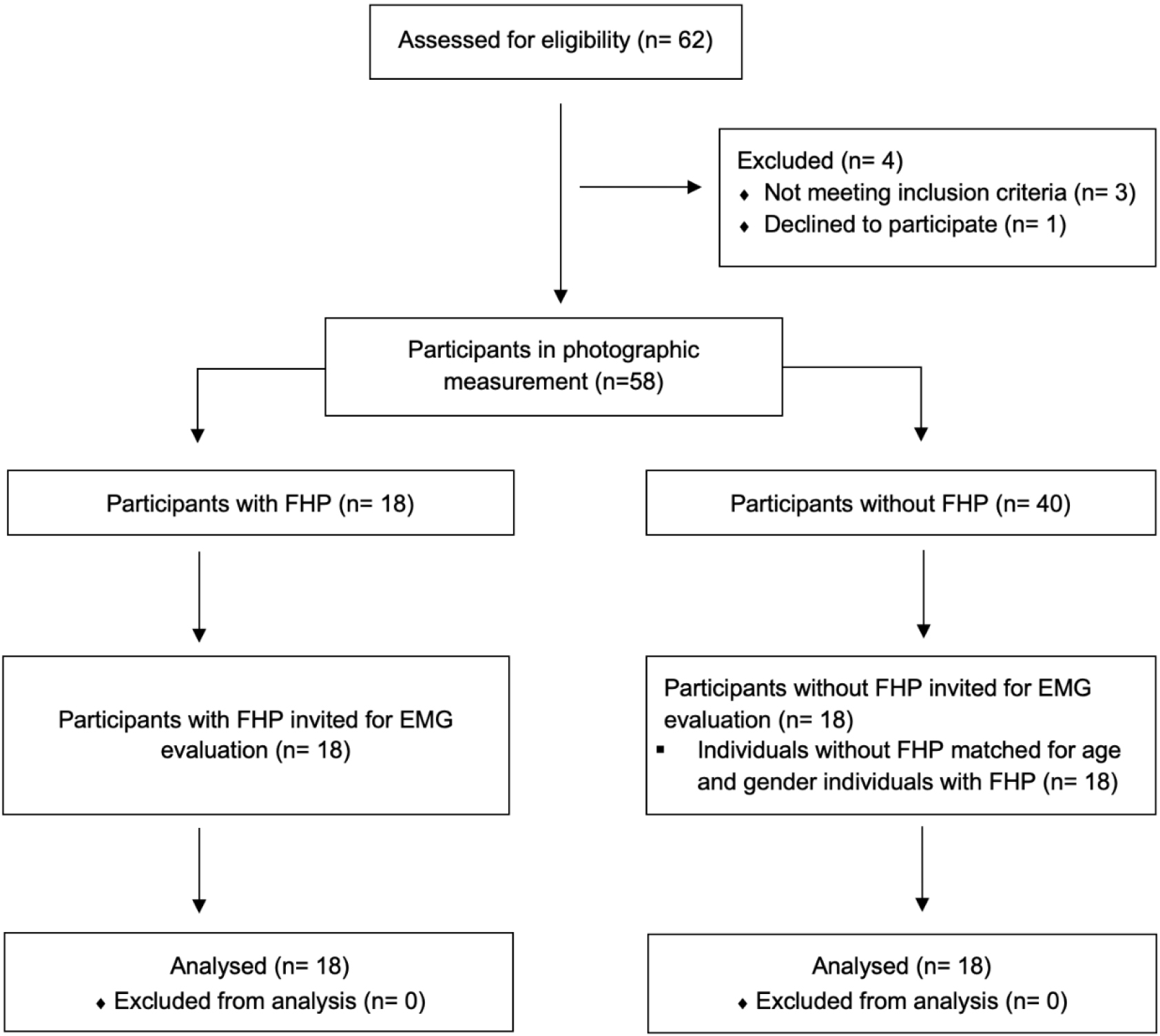
SPSS 22.0 program (IBM Corp., Armonk, NY, USA) was used for the statistical analysis. All outcome variables were normally distributed, as assessed using visual (histograms and probability plots) and analytical methods (Shapiro-Wilk tests). Participants characteristics and descriptive data for EMG were expressed as mean and standard deviation. Independent sample
Results
Initially, 62 individuals who were informed about the study and agreed to participate were invited to determine their compliance with the inclusion criteria. Four of the participants who underwent photographic measurement did not meet the inclusion criteria. Among the individuals who met the inclusion criteria, those with a CVA lesser than 50∘ were included in the FHP group [1, 44]. According to the results of the photographic evaluation, 18 participants were determined to have a FHP. Eighteen individuals who had similar demographic features (gender, age and BMI) with the participants in the FHP group, met the inclusion criteria and had a CVA greater than 50∘ were included in the non-FHP group. See Fig. 3 for the flowchart of the study.
There were no differences between the groups with and without FHP regarding age, height, body weight, and BMI (
Comparison of demographic information in individuals with and without FHP
Comparison of demographic information in individuals with and without FHP
FHP: Forward Head Posture, SD: Standard Deviation, BMI: Body Mass Index,
There were no significant “Group
Although the “Group
The exercise main effect was found to be statistically significant. There were significant differences observed among the exercises for the SCM muscle (F
No significant “Group
The effect of kinetic chain on muscle activation ratios during BPA exercise in individuals with and without FHP
BPA: Band Pull-Apart; FHP: Forward head posture, SD: Standard deviation, UT: Upper trapezius, MT: Middle trapezius, LT: Lower trapezius. aSignificantly lower UT/MT ratio compared to standing, unipedal standing and Bulgarian split squat. bSignificantly lower UT/LT ratio compared to unipedal squat and Bulgarian split squat.
Sternocleideomasteideus, upper, middle and lower trapezius muscle activation levels during Band Pull-Apart exercises in individuals with and without FHP. Abbreviations: %MVIC: Percentage of maximum voluntary isometric contraction, FHP: Forward head posture.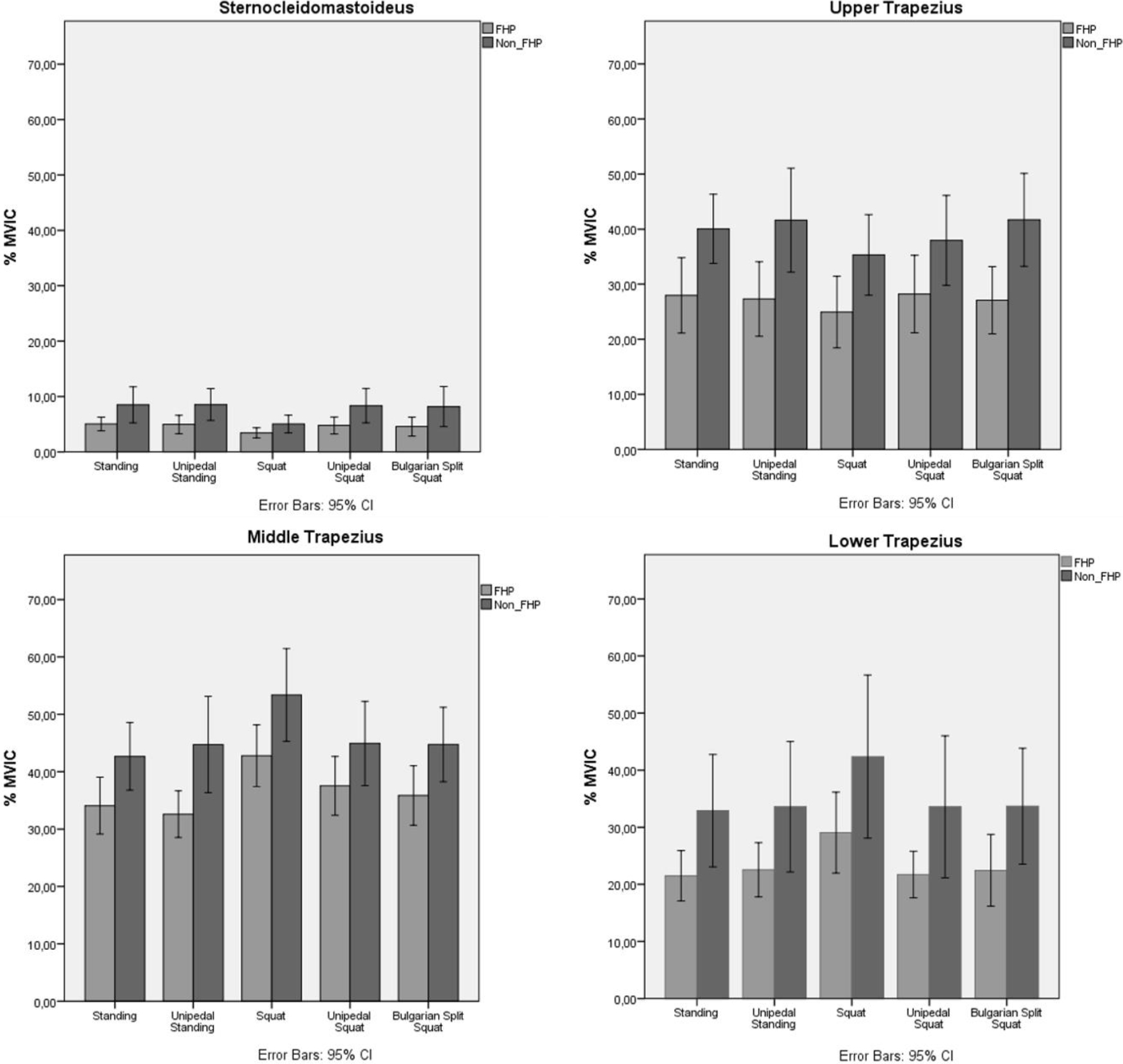
The exercise main effect was found to be statistically significant. It was observed among the exercises that there was a statistically significant difference for UT/MT (F(3.520,109.112)
The main purpose of this study was to investigate the effects of the kinetic chain during the BPA exercise in individuals with or without FHP. To the best of our knowledge, this study is the first to evaluate the effects of the kinetic chain during the BPA exercise. As a result of this study, SCM, UT, MT and LT muscle activations were found to be lower in the FHP group compared to the non-FHP group. However, UT/MT and UT/LT muscle activation ratios were similar between FHP and non-FHP groups. Considering the kinetic chain effect, it was observed that SCM muscle activation in the squat was lower compared to the activation in the standing and unipedal standing. Although there was no statistically significant difference in the amount of UT muscle activation, the activation during the exercise in the squat was lower compared to the other positions. MT muscle activation in the squat was higher compared to standing, unipedal standing, unipedal squat, and BSS positions. LT muscle activation in the squat was higher than the activation in the standing, and unipedal squat. UT/MT muscle activation ratio in the squat was lower compared to the ratio in the standing, unipedal standing, and BSS. UT/LT muscle activation ratio during the BPA exercise in the squat was lower compared to the one the unipedal squat and the BSS.
FHP alignment places the center of gravity of the head anterior to the vertical axis, thus increasing the load on the posterior neck. These postural changes alter scapular mechanics and muscle activity related to the shoulder complex, resulting in altered force couples and scapular movement [45]. To investigate the effect of FHP on muscle activation, we evaluated muscle activation during BPA exercise. As a result of this study, SCM, UT, MT and LT muscle activations were lower in the FHP group than in the non-FHP group. Similar to our study, Lee et al. stated that the activation of splenii and SCM muscles was found to be reduced in the group with FHP during neck protraction exercise compared to the group without FHP, while OT muscle activation decreased during retraction exercise. The authors also found that UT muscle activation was similar during both protraction and retraction exercises. They stated that the reduced activation was due to changes in muscle length due to FHP and was associated with decreased ability to produce force [46]. In contrast, Khan et al. observed that the EMG activity of the SCM and UT muscles significantly increased in individuals with FHP compared to the group without FHP, both at rest and during shoulder abduction [47]. Kiatkulanusorn et al. investigated the differences in muscle activation while resting in the side lying position in individuals FHP and non-FHP and found that FHP might cause excessive activation in the UT and LT muscles, and that the activations in the SCM and MT were similar in those with FHP and without FHP [48]. When the present study and literature is examined, it is seen that the muscle activations in individuals with FHP are contradictory. The reason for the different results in the studies may be the different exercises used in the studies.
To investigate the effect of the kinetic chain, we evaluated SCM, UT, MT and LT muscle activation during BPA exercise in five different lower extremity positions. The most important finding of this study was that BPA exercise performed in squat position showed decreased SCM, UT and increased MT and LT muscle activation. As a result of the present study, SCM muscle activation in the squat was lower compared to the activation in the standing and the unipedal standing. Although there was no statistically significant difference (
Regardless of group, when normalised EMG values during different variations of BPA exercise are investigated, SCM muscle activation produced low activation (
Restoring muscle control and balanced coactivation is challenging for clinicians. Maintaining minimal activity in the overactive muscles, and the selective activation of the weak muscles is important to reduce the imbalance in patients with scapular muscle imbalance. Since the lack of MT, LT and SA muscle activity is considered to be related to the excessive recruitment of the UT, it is especially important to keep the UT/MT, UT/LT, and UT/SA ratios balanced [43]. In a systematic review, the authors stated that integrating the kinetic chain into shoulder exercises may produce lower muscle ratios of trapezius and reduce the demands on the rotator cuff muscles [20]. Considering the kinetic chain effect, UT/MT muscle activation ratio in the squat was lower compared to the ratio in the standing, unipedal standing, and BSS. Regardless of groups, the squat position showed a good UT/OT ratio (0.6–0.8), while the other four positions showed a moderate ratio (0.8–1.0). These findings suggest that performing the BPA exercise in the squat may be more beneficial for rehabilitation regarding the trapezius muscle balance. UT/LT muscle activation ratio during the BPA exercise in the squat was lower compared to the one the unipedal squat and BSS. The ratios in all positions were above 1. However, during BPA exercise performed in squat, the ratio was very close to 1. Since a ratio
When the kinetic chain was included during BPA exercise, decreased SCM and UT and increased MT and LT muscle activations were observed. Furthermore, the incorporation of the kinetic chain decreased muscle activation ratios. It is recommended to perform BPA exercise in the squat position when lower SCM and UT muscle activation, muscle activation ratios, and higher MT and LT muscle activations are requested in individuals with or without FHP. We think that our findings regarding changes in muscle activation by performing the BPA exercise in the squat position will contribute to the literature. To our knowledge, this is the first study to investigate the effect of the kinetic chain in BPA exercise, which is a frequently used exercise in clinics. It is also important because it is the first study investigating the effectiveness of the kinetic chain in individuals with FHP.
This study has several limitations. Firstly, muscles that are important for scapular control during rehabilitation such as pectoralis minor, rhomboids, levator scapula and SA could not be evaluated due to the impossibility of accessing them with surface EMG. Secondly, surface EMG can cause possible crosstalk between superficial and deeper scapulothoracic muscles (such as UT, MT and LT) and artifacts from movement during the test. However, small size surface electrodes and inter-electrode distance, proposed electrode placement are extensively standardized to ensure the reliability of the tests, so errors were minimized. Thirdly, this study was conducted with young, sedentary individuals who did not have any shoulder pathology. Therefore, the results of our study may not be generalizable to different age groups, individuals with different pathologies, or athletes.
Conclusion
To our knowledge, this is the first study to examine the influence of the kinetic chain during the BPA exercise. It is also the first study to investigate the effect of the kinetic chain in individuals with FHP. Understanding the muscle activations during exercises can be useful for clinicians and trainers to choose the appropriate exercises. The influence of the kinetic chain on muscle activation and muscle activation ratios should be considered while giving exercises to individuals with and without FHP. The most important finding of this study is that BPA exercise during squat causes decreased SCM and UT and increased MT and LT activation. Moreover, it was found that the involvement of the kinetic chain contributes to the scapular muscle balance by reducing muscle activation ratios. In shoulder rehabilitation, clinicians should consider using BPA exercise in the squat position if lower SCM and UT muscle activation, lower UT/MT and UT/LT ratios, and higher MT and LT muscle activations are desired in individuals with or without FHP. Future studies are needed to investigate the effect of different exercises on the kinetic chain in different age groups, individuals with different shoulder pathologies, and athletes. It may be also intriguing to investigate the effects of the kinetic chain variations on core muscle activity.
Author contributions
GC: Study Design, Data Collection, Statistical Analysis, Data Interpretation, Manuscript Preparation, Literature Search. NAG: Study Design, Data Interpretation, Reviewing. ZBE: Study Design, Data Collection, Literature Search. MYD: Data Collection, Statistical Analysis, Data Interpretation, Manuscript Preparation.
Data availability
Data is available from the corresponding author upon reasonable request.
Ethical approval
The study was approved by the Gazi University Ethical Commission (No. E-77082166-302.08.01-419695; Reference No. 2022 – 935; Date: 22.03.2022).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Informed consent
Informed consent was obtained from the participants prior to the start of the study.
Footnotes
Acknowledgments
The authors would like to thank Nihan Kafa and İrem Düzgün for their contributions in the thesis committee. They would also like to thank Zeynep Hazar, Çağla Özkul, Gökhan Yazıcı, Melek Volkan Yazıcı and Ebrar Bardakçı for their support throughout the thesis process.
Conflict of interest
The authors report no conflict of interest.