
Abstract
BACKGROUND:
Contrast-enhanced ultrasound (CEUS) and shear-wave elastography (SWE) are used for diagnostic purposes.
OBJECTIVE:
Investigate the diagnostic value of CEUS and SWE for breast lesions of sub-centimeter diameter.
METHODS:
Sixty-two patients (mean age: 49.3±12.1 years) with 66 lesions (mean diameter, 8.1±1.5 mm) were analyzed. Conventional ultrasound (US), CEUS and SWE were undertaken. Pathologic specimens were obtained through biopsy or surgery. Lesions were measured in kilopascals. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were analyzed.
RESULTS:
For conventional US, the sensitivity was 92.31%, specificity 28.30%, PPV 24.00%, NPV 93.75%, and accuracy 40.90%, whereas those for SWE were 61.54%, 98.11%, 88.89%, 91.23%, and 90.91% (p = 0.000) and CEUS were 92.31%, 60.38%, 36.37%, 96.97%, and 66.67% (p = 0.001), respectively. For SWE + CEUS, the sensitivity was 61.54%, specificity 100.00%, PPV 100.00%, NPV 91.38%, and accuracy 92.42% (p = 0.000). There was a significant difference between US and CEUS (p = 0.004), but not for SWE or SWE + CEUS (p = 0.568; p = 0.205). For SWE + CEUS, there was a significant difference with SWE alone and CEUS alone (p = 0.000; p = 0.008). Between SWE and CEUS, the difference was significant (p = 0.031).
CONCLUSIONS:
SWE and CEUS could help to differentiate between malignant and benign breast lesions <1 cm in diameter.
Introduction
Breast cancer (BC) is the second most prevalent cancer-related death in “developed countries”. In recent years, the incidence of BC has been increasing [1, 2]. Early detection and treatment can reduce mortality, as well as improve quality of life and survival.
Ultrasound (US) has become the main auxiliary modality because of its high sensitivity and low expense for imaging of breast lesions [3, 4]. Recurrence-free survival can be ≥20 years for >88% patients with lesion diameter ≤1 cm without lymph-node or distant metastases [5–8]. However, conventional US shows mainly the grayscale morphologic features of the lesion. Conventional US is not ideal for small lesions (especially those <1 cm in diameter) with atypical morphologic features.
Contrast-enhanced ultrasound (CEUS) can aid identification of benign and malignant breast lesions through visualization of the microcirculation within the lesion, and is less dependent on operators than conventional US [9]. Wan et al. [10] stated that the patterns and parameters of CEUS were important for identification of benign and malignant lesions as well for as the prognosis.
Shear-wave elastography (SWE) can reflect the “stiffness” of lesions by measuring the velocity through them by sound waves produced by acoustic radiation [11–14]. Several studies have shown that benign lesions tend to be “soft” and malignant lesions tend to be “hard” using SWE.
Some studies [15, 16] have focused on the diagnostic value of CEUS alone, SWE alone, and CEUS + SWE together for lesions of sub-centimeter diameter. However, few studies have focused on the influence of SWE and CEUS for such lesions. The purpose of the present study was to investigate the diagnostic value of CEUS and SWE for breast lesions of sub-centimeter diameter.
Materials and methods
Patients
Sixty-two patients (66 lesions) were selected from December 2015 to November 2016. Mean age of patients was 49.3±12.1 (range, 27–74; median, 49) years. Mean diameter of lesions was 8.1±1.5 (range, 3.6–10.0; median, 8.0) mm.
Patients were excluded if: (i) they did not undergo CEUS or SWE examinations; (ii) were pregnant or lactating; (iii) they had undergone chemotherapy previously or were undergoing chemotherapy currently; (iv) they were unwilling/unsuitable to undergo biopsy or surgery to obtain pathology data; (v) they had undergone biopsy previously; (vi) if the maximum diameter of their lesions was >10 mm. A flowchart depicting patient selection is shown in Fig. 1. The protocol for this retrospective study was approved by the ethics committee of our hospital. The requirement for informed consent was waived.
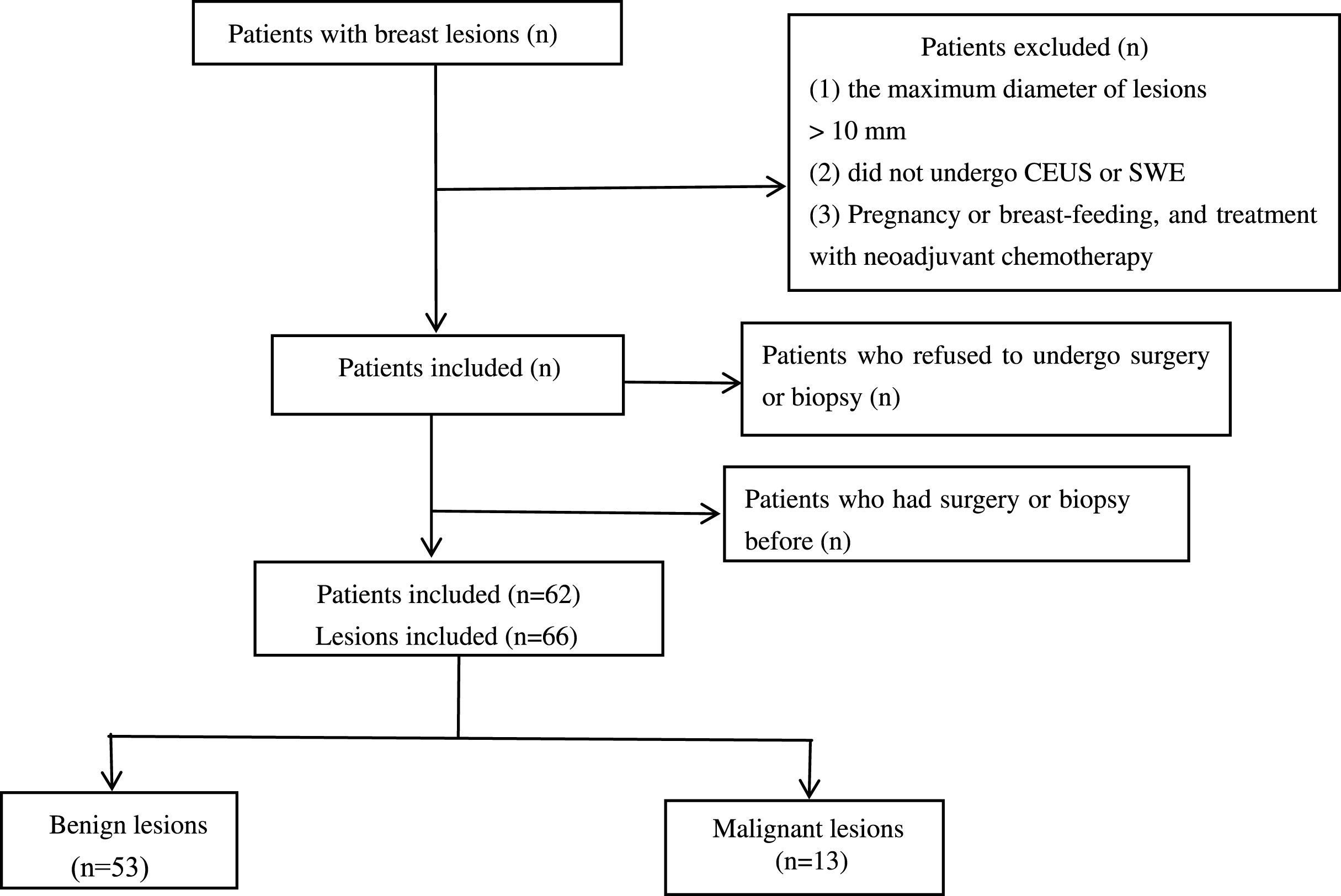
Flowchart showing inclusion of patients with breast lesions of sub-centimeter diameter.
Conventional US and CEUS
Conventional US and CEUS were done using a Logiq E9 system (General Electric Healthcare, Chicago, IL, USA) with a linear array probe (frequency, 4–9 MHz) for US and a linear array probe (frequency, 6–15 MHz) for CEUS. Examinations were carried out by one of two sonographers who had experience of US of the breast of >10 years and CEUS of the breast of >3 years.
Patients were positioned supine with their chest and axilla exposed fully. Morphologic characteristics of the lesion (location; size; echo; margin; calcification; posterior echo; acoustic halo surrounding the active region; internal/peripheral blood flow) were observed, and bilateral axillary lymph nodes were observed simultaneously. Then, we chose the breast lesion in maximum diameter and switched to CEUS. Parameters were adjusted for mechanical index (<0.1) and gain (100–120 dB) and remained identical for the entire process of CEUS. The contrast agent we used was SonoVue (Bracco, Milan, Italy). Physiologic (0.9%) saline (5 mL) was injected through a cubital vein (we did not choose a smaller vein so as to avoid a “burst” of contrast agent). Then, 2.4 mL SonoVue were injected in a bolus injection, followed immediately by flushing with 5 mL saline. The US probe was held very still and patients asked to breathe slowly. Recordings were taken every 3 min and images/video stored in the hard drive of a personal computer for further analyses.
SWE
SWE examinations were done using an Aixplorer® system (SuperSonic Imagine, Aix-en-Provence, France) equipped a linear array probe (frequency, 4–15 MHz). SWE was undertaken by a sonographer who had experience of carrying out elastography of the breast of >2 years.
Patients were positioned supine with their chest and axilla exposed fully. First, in the transaxial plane, the diameter of the lesion was measured and blood flow within it observed. The probe was adjusted to make the lesion in maximum size, and then we switched to SWE. The size of the sampling frame was adjusted so that the lesion and its surrounding normal breast tissue could be included. Then, patients were asked to hold their breath; three images were stored until the lesion and its surrounding normal tissues had an “even” color and were populated fully. Finally, we repeated the operation described above in the longitudinal plane of the lesion. Throughout all SWE examinations the probe was placed lightly on the skin to avoid excess pressure. All images were stored in the hard drive of a personal computer for further analyses.
Image analyses
All images were reviewed by two sonographers who had experience of conventional US of >5 years and CEUS of 3 years. They were blinded to pathology findings and blinded to each other’s measurements. Disagreements were resolved by discussion of data. Lesions were classified mainly by morphologic features into categories 3–5 according to the Breast Imaging Reporting and Data System (BI-RADS) set by the American College of Radiology. Information about lesions was included in six images; the maximum and minimum values were excluded, and the values for the remaining four images were calculated. The cutoff value was obtained by the receiver operator characteristic (ROC) curve. If the mean value was more than the cutoff, the lesion was considered to be “malignant” and vice versa. CEUS features comprised the: pattern, degree, margin, and direction of the enhancement; perfusion defect; size of the discrepancy compared with conventional US. We adopted a five-point scoring system to differentiate a malignant lesion from a benign lesion [17–19]: 1 = no contrast agent in the lesion in the whole process and the lesion had a clear border with surrounding tissue; 2 = lesion and the surrounding breast tissue showed equal enhancement, and an obvious tumor outline was absent; 3 = the lesion showed homogeneous or heterogeneous enhancement, the margin was clear, and the extent of enhancement was similar to that of conventional US; 4 = the lesion showed homogeneous or heterogeneous enhancement, the margin was not clear, the extent of enhancement was greater than that of conventional US; 5 = heterogeneous enhancement, with or without a local perfusion defect, and the surrounding tissue had a “crab leg” appearance. If the score was >3, the lesion tended to be malignant. If the score was ≤3, the lesion tended to be benign.
Pathology
All patients underwent biopsy or surgery <1 week of the examinations described above, and the pathology results were used as the reference standard.
Statistical analyses
SPSS v22.0 (IBM, Armonk, NY, USA) was used for statistical analyses. Quantitative data (age, lesion diameter) are expressed as the mean±standard deviation. The shear-wave velocity is given as the mean value. ROC curves were constructed to determine the suitable shear-wave velocity and acceptable cutoff values, and applied for comparison of the different examination modes. Qualitative variables were compared with the x2 test. Examinations were employed to calculate the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy. p < 0.05 was considered significant.
Results
Sixty-six lesions in 62 patients were analyzed. There were 13 (19.70%) malignant lesions (ten were invasive ductal carcinoma, and the other three lesions were invasive lobular carcinoma, ductal carcinoma in situ and mucinous carcinoma). Of the 53 (80.30%) benign lesions, 25 were due to adenosis, 21 were fibroadenomas, five were intraductal papillomas, one was fibromatosis, and one was plasma-cell mastitis (Table 1).
Pathology
Pathology
Of the 66 lesions, 16 (24.24%) were category 3, four (6.01%) were category 3–4a, 40 (60.61%) were category 4a, one (1.52%) was category 4a–4b, three (4.55%) were category 4b, and two (3.03%) were category 4c using conventional US according to the BI-RADS, and were associated with a sensitivity of 92.31%, specificity of 28.30%, PPV of 24.00%, NPV of 93.75%, accuracy of 40.90% and an area under the ROC curve (AUC) of 0.603 (95% confidence interval (CI), 0.445–0.761) (p > 0.05).
Among the different values for shear-wave velocity, the maximum SWE (Emax), mean SWE (Emean), maximum difference in value between the lesion with surrounding normal tissues (Dmax), and mean difference in value between the lesion with surrounding normal tissues (Dmean) had a significant correlation with the differentiation of malignant and benign breast lesions (p < 0.05), whereas the minimum SWE (Emin) and minimum difference in value between the lesion with surrounding normal tissues (Dmin) had no significant correlation (p > 0.05). The AUC of the Emax, Emean, Dmean and Dmax were 0.852 (95% CI, 0.733–0.971) 0.768 (0.568–0.968), 0.692 (0.480–0.905), and 0.730 (0.548–0.912), respectively, and there was a significant difference among them (p < 0.005). The AUC of Emax was the highest and the cutoff value was 56 kPa, which was associated with a sensitivity of 61.54%, specificity of 98.11%, PPV of 88.89%, NPV of 91.23%, accuracy of 90.91% (p = 0.000) and an AUC of 0.798 (95% CI, 0.630–0.966). The different SWE values are shown in Fig. 2 and Table 2.
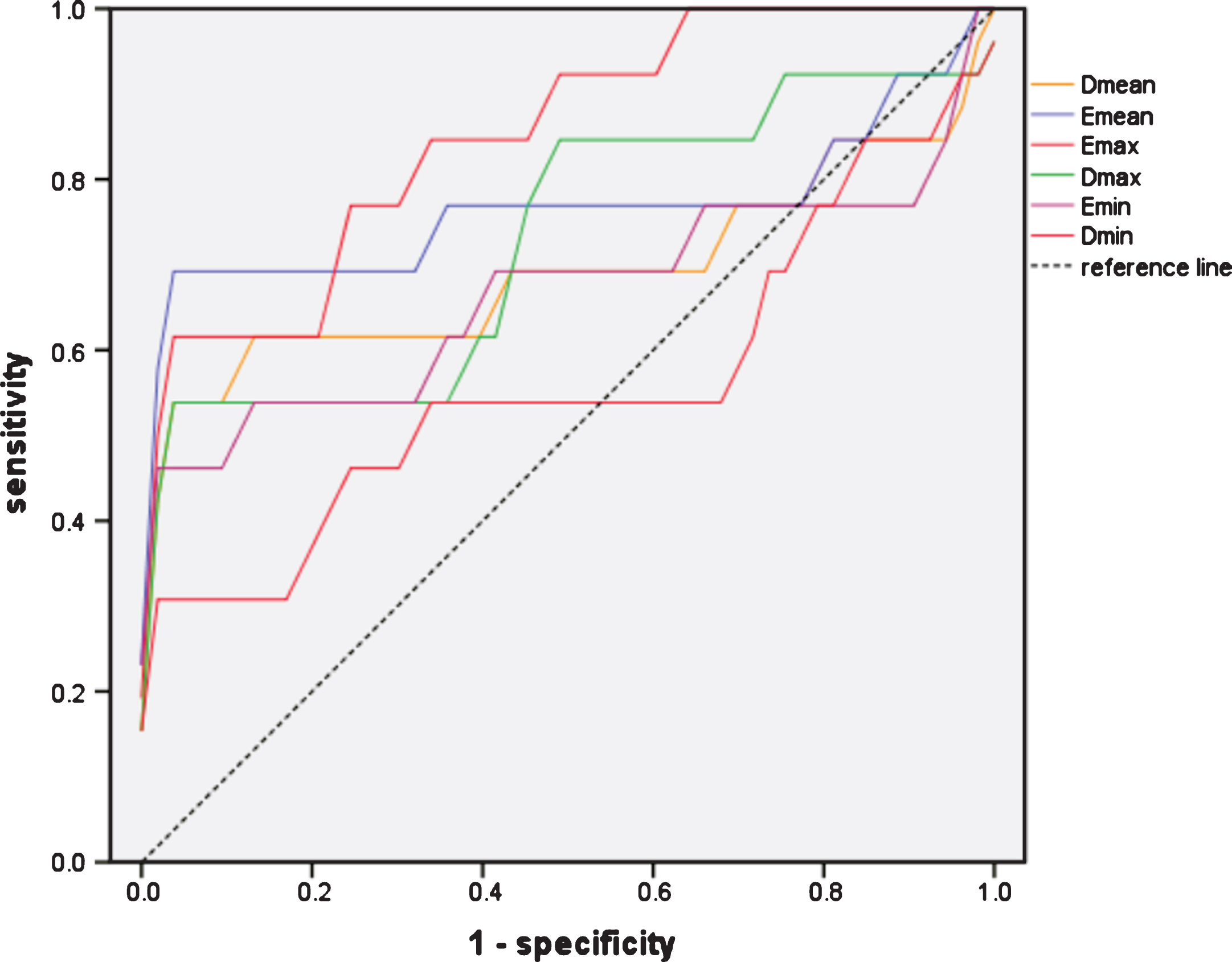
ROC curve of different shear-wave values; the maximum SWE has a higher AUC.
Area of the receiver-operating characteristic curves of different values of shear-wave velocity
Thirty-three lesions were considered to be malignant and 33 benign using CEUS. Of the 13 malignant lesions, 92.31% (12/13) were diagnosed correctly and 7.69% (1/13) were misdiagnosed as benign. Of the 53 benign lesions, 60.38% (32/53) were diagnosed correctly and 39.62% (21/53) were misdiagnosed as malignant. These data were associated with a sensitivity of 92.31%, specificity of 60.38%, PPV of 36.37%, NPV of 96.97%, and accuracy of 66.67%, respectively (p = 0.001). The AUC of CEUS was 0.763 (95% CI, 0.636–0.891).
With respect to SWE + CEUS, 61.54% (8/13) of malignant lesions were diagnosed correctly and 38.46% (5/13) were misdiagnosed as benign, whereas 100.00% (53/53) of benign lesions were diagnosed correctly. These data were associated with a sensitivity of 61.54%, specificity of 100.00%, PPV of 100.00%, NPV of 91.38%, and accuracy of 92.42%, respectively (p = 0.000). The AUC of CEUS was 0.808 (95% CI, 0.640–0.975).
A significant difference between SWE and US was not observed (p > 0.05). A significant difference was observed between CEUS and US (p < 0.05). A significant difference was observed between SWE and CEUS (p < 0.05). There was no significant difference for CEUS + SWE (p < 0.05) (Fig. 3, Table 3).
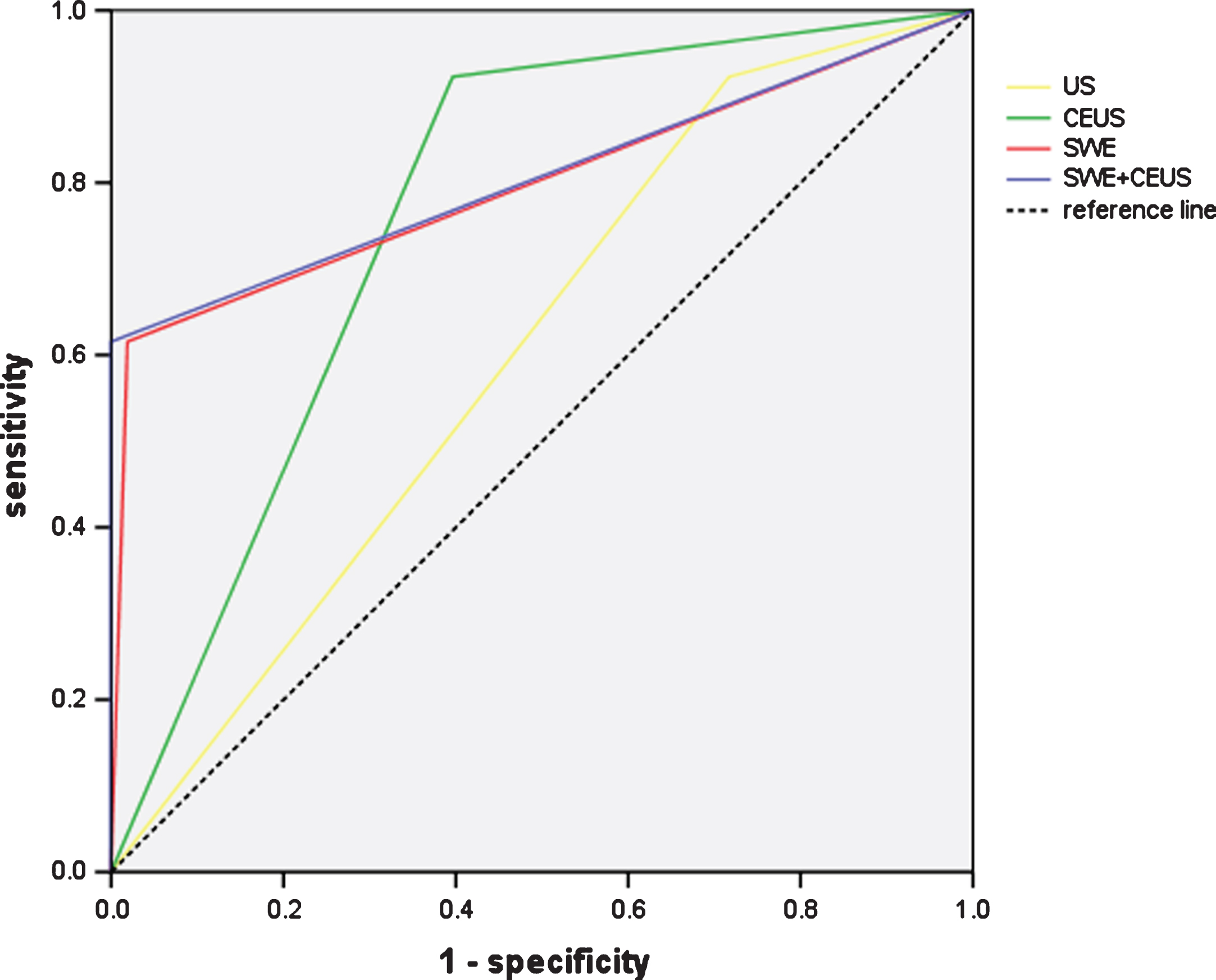
ROC curve of different modalities with area of: 0.642 (p = 0.116) for US; 0.763 (p = 0.003) for CEUS; 0.798 (p = 0.001) for SWE; 0.808 (p = 0.001) for SWE + CEUS.
Sensitivity, specificity, PPV, NPV, accuracy and P-values of different modalities
P-value 1: compared with pathology findings; P value 2: compared with US. P-value 3: compared with SWE + CEUS; P-value 4: comparison between SWE and CEUS.
As for the diameter of breast lesions calculated by the US, SWE and CEUS, the malignant lesions tended to have a larger diameter while the benign lesions showed the similar diameter. (Table 4, Figs. 4, 5)
Evaluation of tumor diameter by US, SWE and CEUS
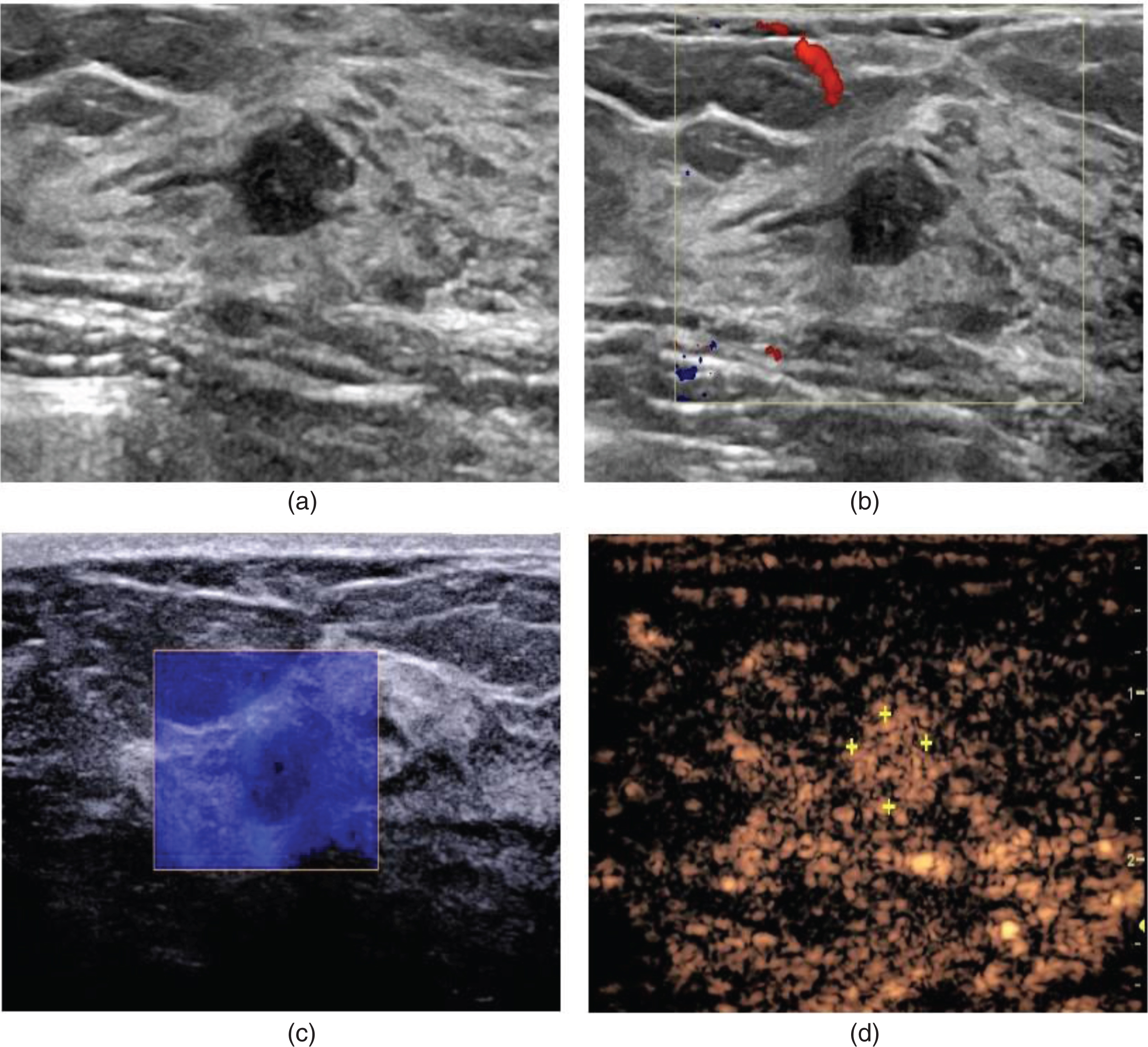
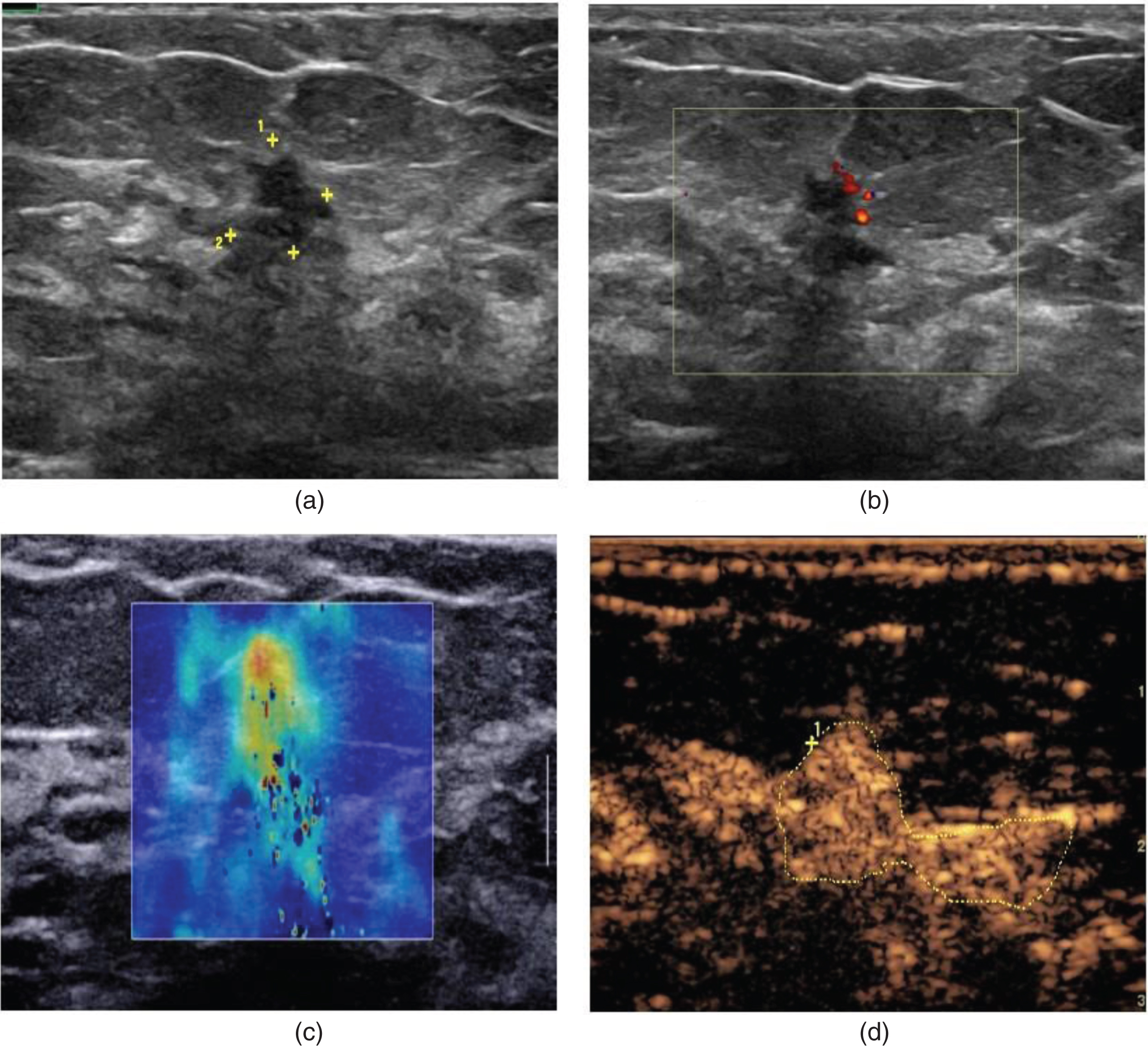
A 39-year-old female with fibroadenoma of the left breast. Conventional US image (a) and color Doppler image (b) and SWE image (c) indicate that the stiffness of the lesion is similar to surrounding normal tissue, and the CEUS image (d) demonstrates lesion with homogeneous iso-enhancement; the margin is clear and the size is similar to that obtained with conventional US.
A 53-year-old female with grade-III invasive ductal carcinoma of the left breast. The conventional US image (a), color Doppler image (b) and SWE image (c) indicate that the stiffness of the lesion is greater than that of surrounding normal tissue, and the CEUS image (d) demonstrates a lesion with homogeneous hyper-enhancement; the shape is irregular and the size larger than that obtained by conventional US.
Conventional US has high sensitivity, so we did not combine US with SWE or CEUS. Our study suggests that SWE and CEUS can be helpful, and that SWE + CEUS can improve the specificity of the imaging method.
In recent years, elastography (i.e., a medical imaging modality that “maps” the elastic properties of soft tissue) has advanced. Elastography can be divided mainly into conventional sonoelastography (SE) and acoustic radiation force impulse (ARFI) imaging. The latter can avoid dependence on the sonographer and the difference caused by different pressure than SE. Several studies [11–13, 21] have shown that benign and malignant lesions have different levels of stiffness, and that malignant lesions are usually harder than benign lesions. SE and ARFI imaging have value for identification of benign and malignant breast lesions. Lesions are analyzed and the related elastography values (Emax, Emean, Emin, Dmax, Dmean, Dmin) calculated.
The results of our study suggest that Emax, Emean, Dmax and Dmean had a correlation with identification of benign and malignant lesions of the breast (p < 0.05). Also, the diagnostic value of Emax was the best, and had a significant difference with Emean, Dmax and Dmean (p < 0.05). Our results are similar to those of other scholars [22, 23]. Ng et al. [24] found that, of the different values of elastography, Emax had the most significant correlation for differentiation between benign and malignant breast lesions, and provided a sensitivity of 100.0% and specificity of 97.6%. In our study, the cutoff of Emax was 56 kPa, and carried a sensitivity of 61.54%, specificity of 98.11%, PPV of 88.89%, NPV of 91.23% and AUC of 0.798. Our results were slightly different to those of Ng et al. [24], and could be because we only included breast lesions of diameter <1 cm whereas they focused on lesions regardless of diameter. Cho et al. [25] found that the lesion diameter influenced the Emax of lesions rather than the number of lesions. The results of our study were different to those of Yoon et al. [26] and Yao et al. [27], whose results suggested that the sensitivity of their method was ≈30%. This difference might have been caused by the different measurements taken: they used fixed sampling (virtual touch imaging quantification), whereas we focused on changes in SWE values. If the lesion was irregular, we undertook tracing to avoid inclusion of surrounding normal tissues, which may have reduced the elastography value. Irrespective of the measurement adopted, the Emax of lesions was identical but the Emean and Dmean differed, and the Emean has been used in previous studies. Our study demonstrated no significant difference between SWE and conventional US (p = 0.568), but it could have been due to the small number of lesions tested. However, most studies have demonstrated the diagnostic value of elastography. Therefore, we consider SWE to be more valuable than US for differentiation between benign and malignant breast lesions.
CEUS is also a relatively new technology. Several studies [28–31] have shown that CEUS can be helpful for differentiation between benign and malignant breast lesions. A malignant tumor can produce interrelated factors to stimulate angiogenesis (e.g., vascular endothelial growth factor) to supply its own growth, which causes the lesion to have a richer blood than that of normal tissue [32]. A malignant tumor has vascular contortions because a lesion with a rich blood supply cannot maintain its rapid growth. Also, a malignant lesion can be irregular, with no clear boundary separating the lesion with surrounding normal tissues. Our five-point scoring system for CEUS was based on such features for identification of benign and malignant breast lesions. Zhao et al. [33] found that for different diameters of lesions, the diagnostic value of CEUS was different. Wang et al. [34] suggested that qualitative assessment of the enhancement pattern was better for differentiation between benign and malignant lesions than quantitative assessment of the enhancement pattern. Related studies [17–19] have shown the diagnostic value of the five-point scoring system. In our study, CEUS was correlated with a sensitivity of 92.31%, specificity of 60.38%, PPV of 36.37%, NPV of 96.97%, and had a significant difference with conventional US (p = 0.004). Our results are similar to those of previous studies, and demonstrate the helpful role of CEUS for differentiation between benign and malignant breast lesions of diameter <1 cm.
When SWE and CEUS were combined, lesions were considered to be malignant only if SWE and CEUS both indicated malignancy. This combination showed a sensitivity of 61.54%, specificity of 100.00% and AUC of 0.808, which was slightly different to the data of a previous study [15, 17]. There was a significant difference between SWE + CEUS with CEUS alone and SWE alone (p = 0.008, p = 0.000) whereas there was no significant with conventional US (p = 0.205). There was a significant difference between CEUS and SWE (p = 0.031). Our results demonstrated that the specificity of SWE + CEUS was 100.00%. Thus, SWE + CEUS could reduce the need for biopsy or surgery to avoid unnecessary injury to patients. Our study is the first to analyze the impact of SWE and CEUS for breast lesions of diameter ≤1 cm.
Our study showed the specificity of CEUS to be 60.38%, lower than that recorded previously [11, 27]. Several lesions were shown to be due to adenosis. The reason may be that lesions affected by adenosis have a rich blood supply, the margin is indistinct, the shape is irregular, and some lesions may be like nodules whereas others are not. Thus, estimation of the diameter of lesions was greater than that for conventional US, and such lesions were considered to be malignant using CEUS. SWE can avoid such situations. Wang et al. [18] and Choi et al. [21] found SWE to be helpful for the diagnosis of non-mass-like breast lesions. Our study also showed that many of the benign lesions, especially adenosis, diagnosed as malignant by CEUS could be diagnosed correctly using SWE. This finding confirmed the necessity of combination of SWE with CEUS.
Zhou et al. [35] demonstrated that the “stiff rim sign” might be caused by desmoplastic reactions, and that the low amplitude of the shear wave within a malignant lesion might be caused by attenuation of the energy of the shear wave in the peritumoral region. In our study, most of the malignant lesions had the stiff rim sign. One explanation may be that the stromal reaction was not parallel to the angiogenesis within lesions. Our study suggested that lesions with a rich blood supply might have no stromal reaction in surrounding tissue. Whether angiogenesis is more likely than desmoplastic reactions merits further study.
Our study had three main limitations. First, the number of lesions included was 66 because patients always had more than one lesion and the diameters of other lesions were >1 cm, so usually the lesion with the larger diameter underwent CEUS or SWE. Hence, the small number of samples would affect the statistical robustness of our study. Second, penetration of shear waves for deeper lesions was weak, and the “coloring” could not be filled completely for some lesions. Third, we did not analyze the pathologic types and histologic grades of lesions. Wan et al. [10] found that different histologic grades had different enhancement patterns. Also, Evans et al. [36] demonstrated that different pathologic types had different elastography values.
Conclusions
SWE and CEUS can be helpful for differentiation between benign and malignant breast lesions of sub-centimeter diameter. The Emax of SWE might be more important compared with other elastography values. Combination of SWE and CEUS can increase the specificity of imaging, thereby reducing the need for unnecessary biopsy or surgery.
Conflicts of interest
The authors had no conflict of interests to declare in relation to this paper.
Footnotes
Acknowledgments
This work was supported in part by Grant SHDC12016233 from Shanghai Hospital Development Center, Grant 124119a3201 from Science and Technology Commission of Shanghai Municipality, Grants 81471673 and 81671699 from the National Natural Science Foundation of China.