
Abstract
To evaluate the effectiveness of high-resolution contrast-enhanced ultrasound (CEUS) to diagnose early post-operative complications in an interdisciplinary intensive care unit.
In 50 patients (male 32; female 18) 64 CEUS examinations were performed in an intensive care unit (ICU) setting to detect post-operative complications. Multi-frequency transducer (1–5 and/or 6–9 MHz) were used. All 64 examinations were performed by one experienced examiner. CEUS findings were compared with contrast-enhanced computed tomography (CECT) findings. CECT images were acquired within 1–24 hours after CEUS examination in arterial and portal-venous phases of the abdomen using either a 16-slice computed tomography scanner or a 128-dual slice computed tomography scanner.
In 56 out of 64 cases (88%) the CEUS-based diagnosis corresponded with the CECT diagnosis. Vascular stenosis in hepatic arteries and portal veins were recognised in both imaging modalities but were evaluated differently [5 cases]. In 3 cases (5%) small peripheral splenic infarction, retroperitoneal hematoma and fluid collection around the liver were not diagnosed by CEUS.
Introduction
Contrast-enhanced ultrasound (CEUS) allows the dynamic evaluation of the microcirculation up to capillary perfusion in internal organs by using a high-resolution multi-frequency transducer [1, 2]. The 2nd generation of ultrasound contrast agents, in particular sulfur hexafluoride microbubbles (SonoVue®; BRACCO, Italy) is used as an echo signal amplifier. This ultrasound contrast media consists of tiny gas-filled microbubbles in the range 2–10 μm and is a real blood-pool contrast agent allowing direct assessment of microvascularization of capillary perfusion. Sulfur hexafluoride is a nontoxic gas which is completely eliminated via the lungs within a few minutes after it application [1]. The phospholipid shell of the microbubbles is very flexible, allowing substantial oscillation even at the very low insonation power used in low mechanical index (<0.16) [1]. This allows continuous imaging of CEUS with an echo signal amplifier up to 20 dB.
CEUS enables the possibility of detection and characterization of liver tumors with comparable diagnostic accuracy as contrast-enhanced spiral computed tomography (CECT) or magnetic resonance imaging (CEMRI) [3–5] in daily clinical routine. CEUS visualizes dynamic changes of microcirculation in all parenchymal organs, thus organ infarction, organ injury, inflammation/infection, tumors, as well as vascular lesions such as stenosis, dissection or thrombus formation, can be detected [6–16].
The aim of this study was to examine whether CEUS at an intensive care unit allows for a comparable diagnostic effectiveness in acute changes of abdominal microvascularization as compared to CECT.
Material and methods
50 patients (18 female and 32 male) with a medium age of 56 [range: 24–88 years], were included in this study. In total 64 CEUS examinations were performed. All patients underwent CEUS at an interdisciplinary intensive care unit in the hospital between August 2013 and February 2015. Written informed consent for the contrast media application was obtained from all patients, as far as their general condition allowed it.
All examinations ware performed by the same experienced examiner using multi-frequency transducers (1–5 and 6–9 MHz, LOGIQ E9, GE, Milwaukee, WI, USA) with storage of digital images.
CEUS examinations were carried out with a reduced mechanical index. An intravenous bolus of 1–2.4 mL sulphur hexafluoride microbubbles (SonoVue®, Bracco, Italy [1]) followed by a bolus injection of 10 mL NaCl was applied via a peripheral cubital cannula or central venous catheter. The indication for CEUS was provided and documented by intensive care unit (ICU) physicians. Digital cine-loops were stored with sweep-technology in DICOM-format from the arterial phase (15–45 sec) to the late venous phase (3–5 min). If necessary, a second contrast media bolus followed. Acquisition of hemodynamical flow parameters through the color-coded Doppler sonography (CCDS) focused on the potential stenosis parameters like peak systolic velocity, end-diastolic velocity and resistive index.
64 contrast-enhanced computed tomography (CECT) scans were performed in 50 patients after CEUS examinations within 1–24 hours post ultrasound examination in arterial and portal –venous phase of the abdomen. CECT images were obtained with either a 16 – slice computed tomography scanner (Sensation, Siemens, Erlangen, Germany, 16×1 mm collimation, 5 mm axial and coronal multi-planer images) or a 128 – dual slice computed tomography scanner (SOMATOM Definition Flash, Siemens, Erlangen, Germany, 128×0,5 mm collimation, 5 mm axial and coronal multi-planer images). An intravenous bolus nonionic iodinated contrast agent was administered with a power injector through cubital vein. 80–130 ml of Accupaque 300 (GE Healthcare, Munich Germany) was used for the CECT.
The images were archived in PACS and analyzed by two examiners with experience in computed tomography and ultrasound images. Concordance of CEUS results compared to CECT results was assessed using a spreadsheet (Excel, Microsoft, Richmond).
Results
Diagnostic results of CEUS and CECT examinations were compared in 64 cases. In 56 out of 64 cases (88%) the diagnosis from CEUS and CECT corresponded in both imaging modalities (Fig. 4).
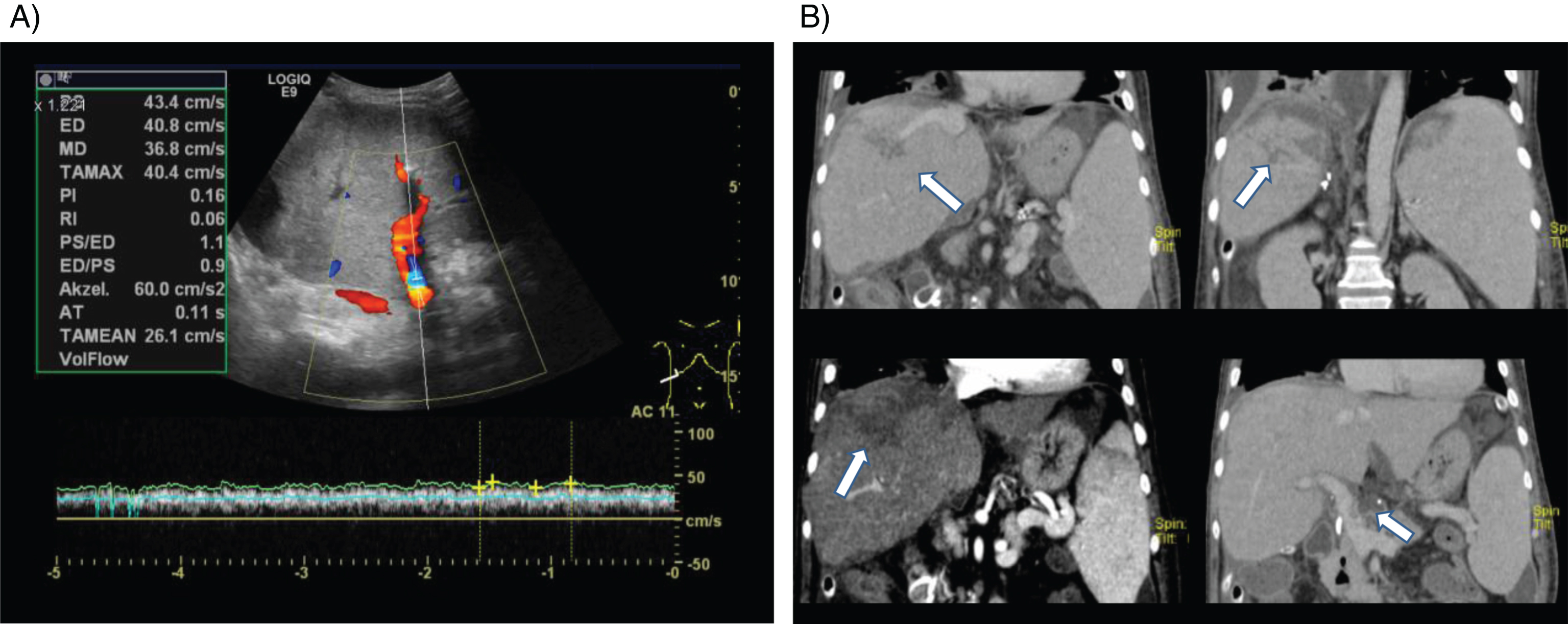
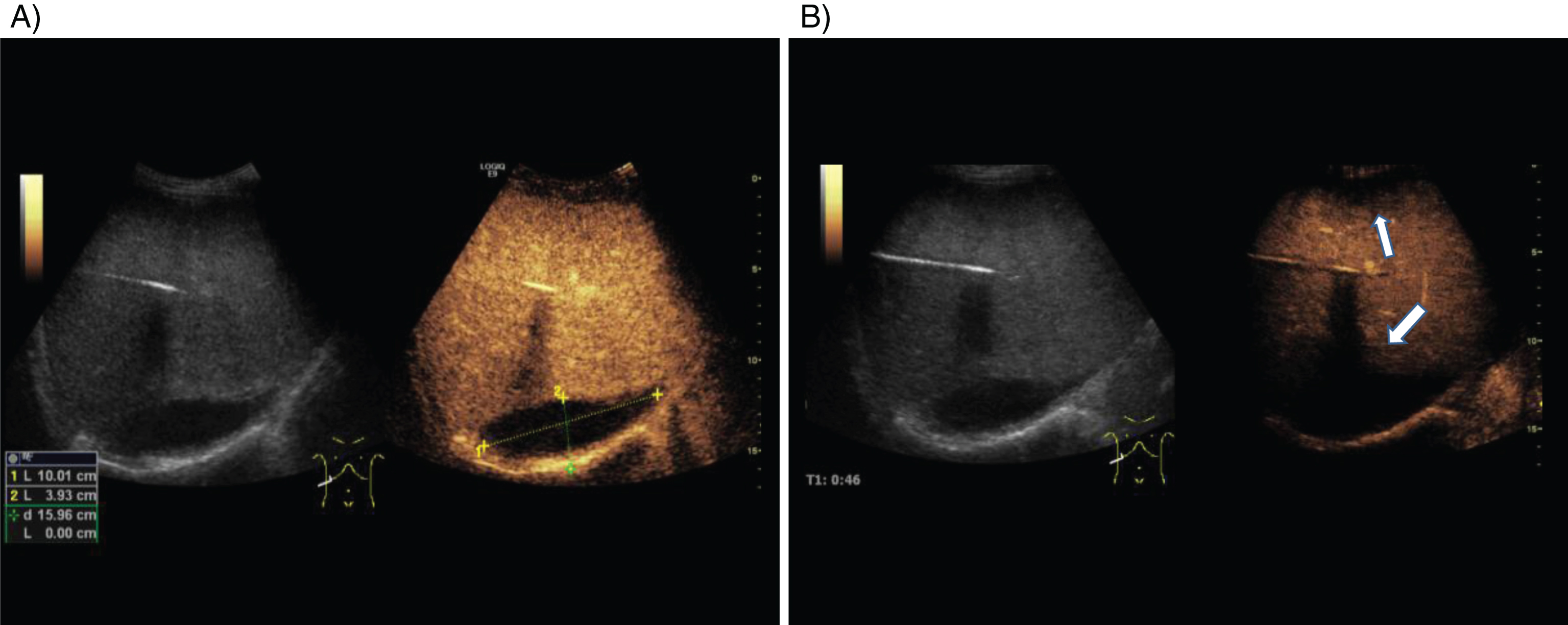
The following diagnoses were established by CEUS and CECT, respectively: Hypoperfusion of the liver after liver transplantation or vascular surgery [28 cases]. Reduced arterial, portal venous or venous vascularization and lumen reduction of hepatic artery or portal vein of more than 50% in combination with segmental reduced parenchymal microvascularization (Fig. 1). Thrombosis or stenosis of the portal vein [11 cases], with irregular lumen reduction (Fig. 2). Hypoperfusion of the kidney or renal artery stenosis [7 cases], and segmental reduced microvascularization. Postoperative hematoma [3 cases] (Fig. 3). Others, for example splenic infarction, ascites, cholestasis, lymphocele, flow changes in visceral vessels (for example SMA) [12 cases]. Arterial stenosis after liver transplantation. A) Color-coded Doppler sonography (CCDS) shows lumen reduction of the hepatic artery with elevated systolic and end-diastolic flow velocity and reduced resistance (RI), less than 0.5. B) Contrast enhanced ultrasound (CEUS, right) shows a high grade stenosis of the hepatic artery (arrow) without infarctions of the liver after transplantation. B-Mode (left) shows echo-inhomogeneous liver parenchyma. A) Color-coded duplex sonography (CCDS) image of the liver. Portal hepatic vein stenosis with flow increase up to 43.4 cm/s. B) Coronal computed tomographic scans of liver a few weeks later with hypodensic infarct area and portal hepatic vein stenosis with thrombus (arrows). B-mode (each left) and contrast-enhanced ultrasound (CEUS, each right) images of the liver parenchyma after transplantation. A) 10×4 cm anechoic, strictly delimited area in right lobe of liver at the lower edge compatible with hematoma. B) Another smaller hypoechogenic area at the upper edge of the liver corresponds to reduced organ perfusion. Representation of the diagnoses of 64 cases in 50 patients classified as hypoperfusion of liver (1), portal vein stenosis or thrombosis (2), hypoperfusion of kidney or renal artery stenosis (3), postoperative complications (such as hematoma) (4), Other (5) compared to contrast-enhanced CT.

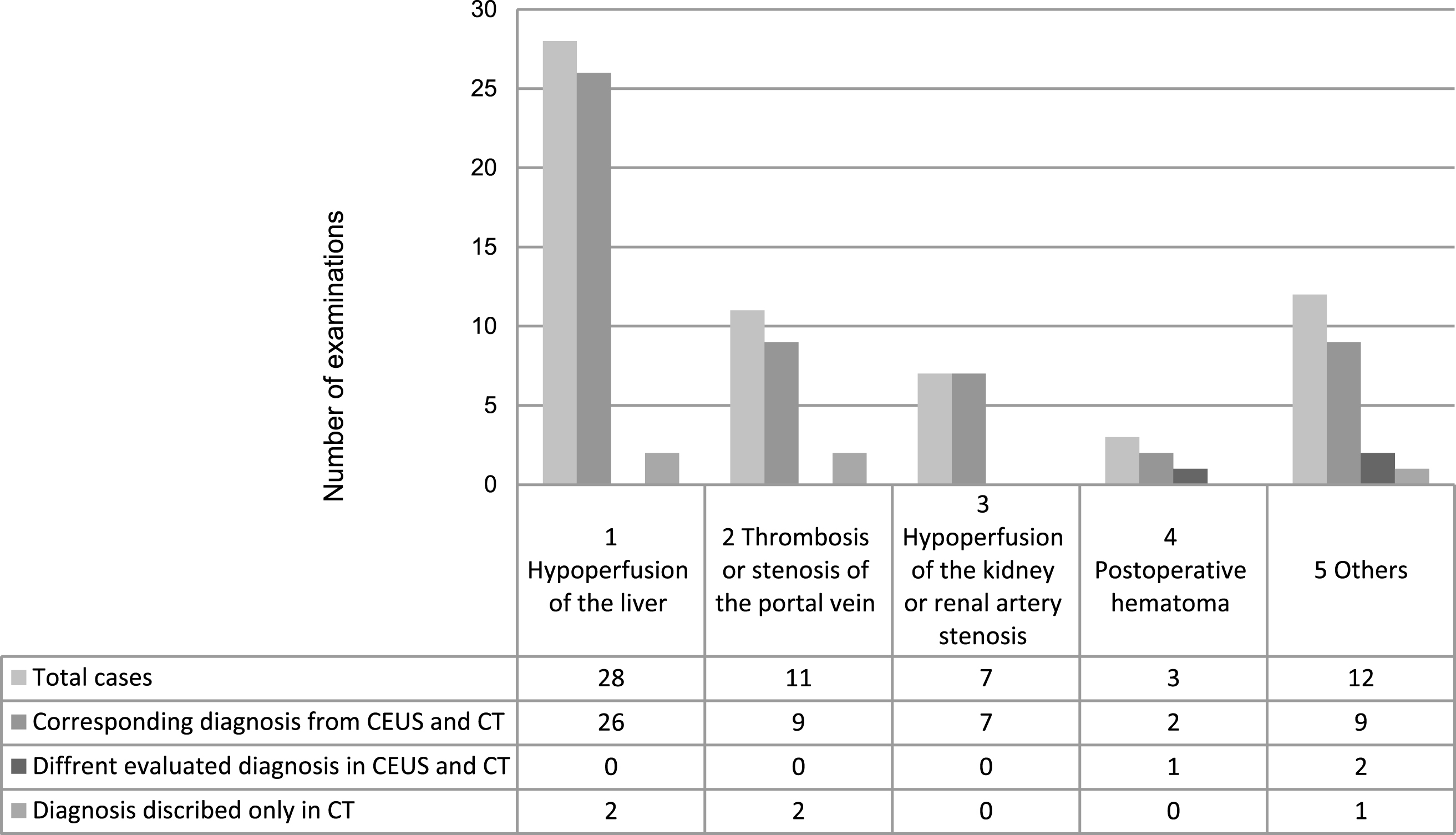
In 5 cases (7.8 %) vascular stenoses were recognized in both modalities but they were described differently: high-grade stenoses in CEUS and moderate/mild in computed tomography angiography (3 x portal hepatic vein and 2 x hepatic artery). In 3 cases (5 %), small peripheral splenic infarction, small retroperitoneal hematoma and -fluid collection around the liver, were not diagnosed by CEUS.
CEUS offers decisive advantages in the postoperative phase after tumor resection or organ transplantation to reliably assess reduced organ perfusion, bleeding or leakage [4, 17–19].
The ease of use of CEUS is an advantageous especially in an intensive care unit (ICU) environment, potentially allowing to overcome the need for patient transport to the computed tomography scanner. However there is only limited data regarding diagnostic effectiveness of CEUS compared to CECT for ICU patients with acute postoperative complications. In our study a few vascular stenoses were evaluated differently, but these stenoses were recognised in both modalities and only 3 cases, partial splenic infarction and small retroperitoneal hematoma and -fluid collections around the liver are not described using CEUS technology. These conditions may have arisen in the time period between CEUS and CECT or due to the severe postoperative condition, for example gas collection, so that they couldn’t be detected by CEUS.
The high diagnostic value of CEUS in the detection of organ hematoma, infarcts, but also vascular changes such as stenosis, dissection and pseudoaneurysm are documented in the literature [4, 18]. We report similar results with a very high degree of concordance regarding such diagnosis for CEUS and CECT. Ultrasound examinations in the ICU require a particularly high experience of the examiner. The limiting factor being a very small acoustic window due to postoperative dressing material, limited positioning options of the patient and mechanical ventilation. Breath-hold maneuvers are usually not feasible in an ICU environment. Particularly after liver transplantation, the assessment of the hepatic artery, celiac trunk and SMA may be difficult.
The benefit of CEUS is the dynamic evaluation up to the capillary level of hypoperfusion, inflammation/infection, stenosis as well as emergency diagnosis of active bleeding, but also to assess the microvascularization of tumors and the sonographic visualization of tumoral characteristics[11, 20]. CEUS can provide additional, clinically relevant information in patients with acute and subacute complications following pancreas and renal transplantation [4, 6]. Early diagnosis of such complications is essential for urgent therapy, like re-operation, vessel dilatation or embolization before development of severe organ failure, bleeding or sepsis. CEUS might be helpful to improve early diagnosis of diabetic nephropathies by quantitative evaluation of renal cortex perfusion [13].
There are several limitations to the study: the most important one is inherent in the study design –as all patients that were included in the study had to have CEUS and CECT examinations within a given timeframe, we could not asses patients that only underwent CEUS examination during their ICU stay. Furthermore all CEUS examinations were carried out by a single physician, thus limiting the generalizability of our results. Another limiting factor is that the patient cohort was mixed and diagnostic effectiveness was assed retrospectively.
In conclusion, our data suggests that CEUS in an ICU setting is a promising tool for intensive care patients in the assessment of post-operative abdominal complications.