
Abstract
Ultrasound elastography has been introduced into clinical practice for a decade and arisen continuous increasing attention worldwide. Shear wave elastography (SWE) is a further extension of ultrasound elastography on the basis of strain elastography, providing a two-dimensional distribution map of tissue stiffness and quantitative measurement of the tissue stiffness in Young’s modulus (kPa) and/or shear wave speed (m/s). The Society of Ultrasound in Medicine, Chinese Medical Association (CMA) has recently released a series of guidelines for the use of SWE, including the technique and principle of SWE, and use of SWE in liver fibrosis, breast, thyroid, and musculoskeletal system. Herein, a part of SWE in thyroid nodules is presented. In this guideline, the background, classification and technology of SWE, examination methods, diagnostic performance, prognosis evaluation, reproducibility, and limitations are discussed and recommendations are given. The recommendations are based on the published literatures with regard to SWE with different levels of evidence, particularly a mid-term result of the prospective multi-center clinical trial of SWE in thyroid, as well as the Society of Ultrasound in Medicine, CMA expert’s consensus. The document provides an overall analysis of SWE in thyroid from clinical perspective, which aimed to provide recommendations to the clinicians with regard to the management of thyroid nodules by the assistance of SWE.
Introduction
Thyroid nodule has become a common and frequent disease that attracts increasing attention by medical society and the public. According to epidemiological studies, in areas with sufficient iodine, about 1% of males and 5% of females have thyroid nodules, and the detection rate by high resolution ultrasound is as high as 19%–68% [2], out of which about 7%–15% are thyroid cancers. As the most common malignant tumor of the endocrine system, thyroid cancer accounts for 1%–2% of all malignant tumors, and its incidence shows a significant rising trend throughout the world. In the past three decades, the incidence of thyroid cancer in the USA had increased to 2.4 times more than the previous value, and the rising was even prominent in China, with the value reaching 300%–400%, making thyroid cancer a malignant tumor with the fastest rate of spreading [3]. Therefore, how to accurately distinguishing carcinoma from overall thyroid nodules, as well as how to formulate a rational treatment plan to avoid overtreatment, are clinical subjects to improve individuals’ life quality and patients’ survival rate.
High-resolution ultrasound imaging is often used as the favorable method for screening thyroid nodules, because it is simple to operate, non-invasive, highly repeatable, and with no radiation; moreover, fine needle aspiration (FNA) based on suspicious features of ultrasound is the golden standard recommended by many guidelines [4]. However, since benign and malignant nodules are with complicated ultrasound characteristics, and their image characteristics have certain overlaps on conventional ultrasound, the diagnostic efficiency of conventional ultrasound is thereby varied. Studies have reported that for differentiating benign or malignant nodules, the sensitivity of conventional ultrasound and the specificity ranged within 26%–87% and 53%–93%, respectively, which is unable to meet the requirements of clinical use, and new ultrasound imaging techniques are required as supplementary methods for diagnosis.
Elastography is a newly developed technology that could differentiate malignant or benign tumors by assessing the stiffness of tissues. It has been provided a new strategy for clinical identification of malignant or benign thyroid nodules, and has been recommended as an important approach for evaluation of thyroid nodule by the American Thyroid Association (ATA), American Association of Clinical Endocrinologists (AACE), American College of Endocrinology, and Italian Association of Clinical Endocrinologists (ACE) [5, 6]. The European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) and World Federation for Ultrasound in Medicine and Biology (WFUMB) sequentially published guidelines and recommendations on clinical use of elastography[7, 8], and affirmed the value of elastography in evaluating benign and malignant thyroid nodules. However, the guidelines also point out that elastography should not replace with conventional ultrasound, however, it can be used as a supplementary method in differentiating the nature of thyroid nodules. Meanwhile, due to particular anatomical structure of the neck, the influence of nodule locations on the results of elastography should be concerned as well.
According to the above-mentioned situation and the actual condition in China, the Society of Ultrasound in Medicine of Chinese Medical Association (SUM/CMA) carried out a prospective multi-center study in evaluating the efficiency of two-dimensional shear wave elastography (2D-SWE, hereinafter referred to as SWE) in diagnosing thyroid nodules in Chinese population. Based on the mid-term results, and in combination with the latest literatures, this paper has presented an extensive discussion on clinical application of elastography, and aimed to reach consensus and provide a reference for ultrasound practitioners, as well as clinical medical staffs.
Information included in this guideline is from (1) literatures on thyroid SWE extracted from PubMed (up to July 2018), and (2) expert opinion and experience (see Table 1 for statement of evidence level) [9]. This is also referred to the EFSUMB-WFUMB guideline for clinical use of elastography. The guideline has been discussed by the Expert Committee and agreed to be used as a navigator for clinical application of elastography. With continuous deepening of clinical practice and accumulation of literatures, the Expert Committee attempted to update the contents of the guideline. Eventually, it should be pointed out that in this guideline, the discussion and analysis was focused on SWE in thyroid nodules. Readers who are interested in strain elastography (SE) or diffuse thyroid diseases should refer to other clinical practice guidelines.
Evidence and grading of evidence-based medicine (GRADE system) [9]
Evidence and grading of evidence-based medicine (GRADE system) [9]
According to different imaging principles and methods, elastography can be classified as strain imaging and shear wave imaging. As a type of strain imaging, strain elastography (SE) utilizes a probe to create a distortion in the target tissue by pressure. The tissues with more deformation are relatively soft, while those with less deformation are hard. The image can be coded based on the extent of deformation, and thus SE can be realized as well. However, this is only a qualitative or semi-quantitative technique, and it cannot directly provide the Young’s modulus. Besides, shear wave elastography (SWE; Supersonic Imagine [SSI], Aix-en-Provence, France) is a type of shear wave imaging. It induces tissue displacement by emitting focused acoustic pulses from an ultrasonic transducer. The pulses can cause instantaneous micron-level displacement of the target tissue, which further generates transverse shear wave that can be captured by an ultra-high-speed imaging system for the calculation of shear wave speed or the Young’s modulus, thereby evaluating the stiffness of the target tissue [10]. The higher Young’s modulus is, the greater stiffness will be. This is a quantitative method (Fig. 1).
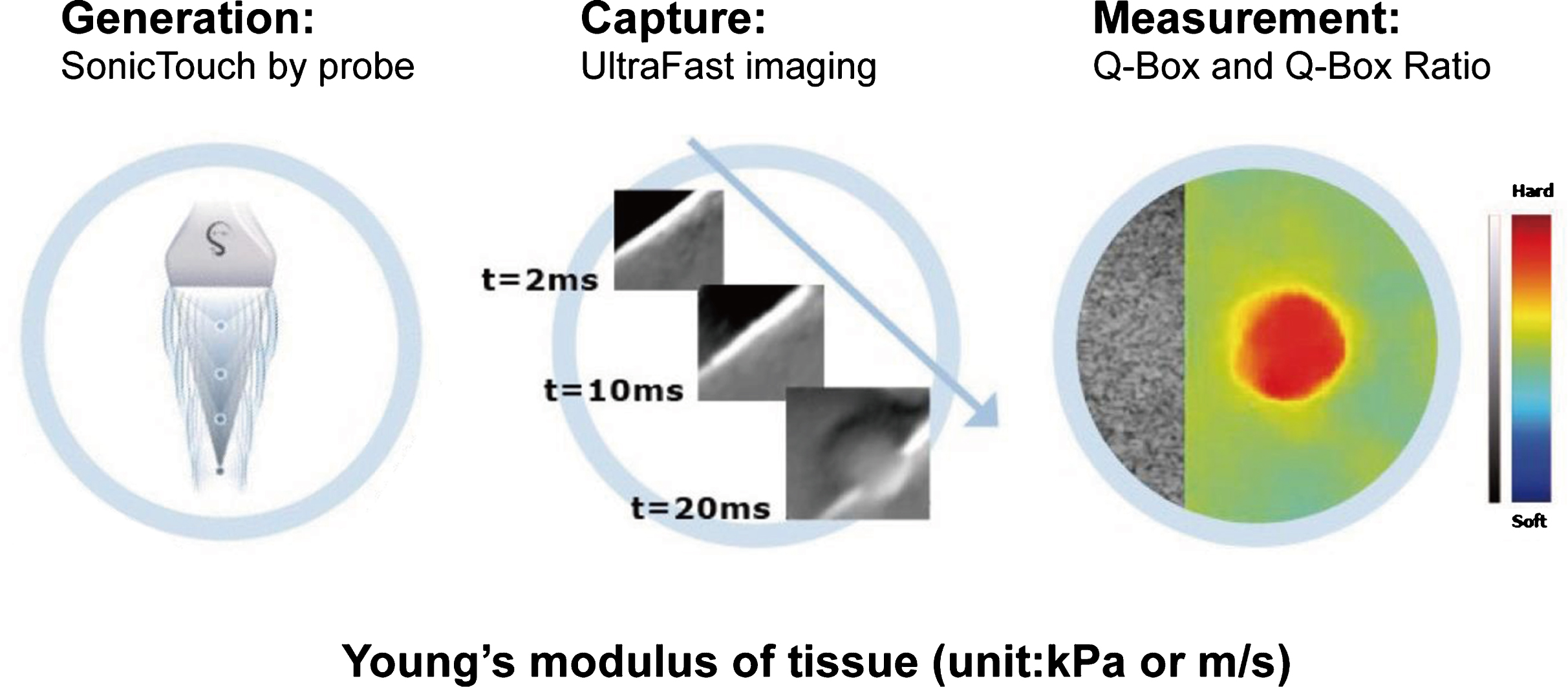
The principle of shear wave elastography (provided by Supersonic Imagine; Courtesy of People’s Medical Publishing House [1]).
As the most representative technique in SWE, 2D-SWE has several advantages when compared with other SE methods, including (1) it less depends on the operator’s subjective judgment and is therefore highly repeatable; (2) it can measure tissue stiffness in a quantifiable manner (shear wave speed or the Young’s modulus); (3) it is appropriate for the evaluation of relatively large or multiple nodules [11]; (4) it covers a wider range of Young’s modulus, and the value can be as high as 300 kPa for thyroid measurement; (5) it provides more quantitative parameters, such as the mean, maximum, minimum, and standard deviation (SD) values, and it can simultaneously measure the shear wave speed as well as the Young’s modulus. The disadvantages of this technique include: (1) pressure from the probe should be avoided during measurement, otherwise, the measured values of the target tissue might be increased [12, 13]; (2) training and experience are required from the operator [14]; (3) due to the influence of skin and hard trachea, the measurement of isthmus nodules might be difficult [8]; (4) false positive results might occur for cystic or coarse calcified nodules.
Preparation before examination
Patients need no special preparation before the examination [7]. They have to lie in a supine position, and the neck was fully exposed without excessive bending or stretching.
Training of operators
As previous studies have confirmed appropriate reproducibility of SWE, operators’ experience is still required to obtain reliable results [8]. Therefore, we suggest that providing SWE training is helpful to develop SWE reports for junior doctors with less experience, and they should complete the process of collecting SWE imaging data, as well as writing SWE reports for at least 5 cases under the supervision of experienced trainers, leading to improve the reliability of the measurement result.
Setting of device parameters
High-end ultrasound scanners with 2D-SWE function, such as the Aixplorer system (SSI, Aix-en-Provence, France), as well as high-frequency linear array transducer are used. It is recommended to use relatively high frequency linear probe L15-4 for conventional ultrasound examination, of which the frequency ranging 7.5–15 MHz for gray scale ultrasound and 5–9 MHz for Doppler ultrasound, and relatively low frequency linear probe L2-10 for SWE examination, of which the frequency ranging 2–10 MHz for gray scale ultrasound and 3.8–6.4 MHz for Doppler ultrasound. Device setting for SWE mainly includes adjustment of elastic gain, elastic range, region of interest (ROI), as well as the sampling box (Q-box) for stiffness measurement. Based on literature reports and our experience, we suggest to set the elastic gain within 70–80% and the elastic range within 0–100 kPa; the ROI should cover the whole nodule and peripheral normal thyroid tissues, and the Q-box should avoid cystic, coarse calcified areas, or areas with deficient SWE signal. Standard (STD) mode is recommended for routine measurement, and penetration (PEN) mode is recommended when the nodules are deeply located inside.
Examination methods
(1) Conventional ultrasound: During examination, the patient shall be asked to lie in a supine position and fully expose the neck. Conventional ultrasound (gray scale and color Doppler ultrasound) will be first performed to localize the target nodule. Then, the frequency, focus, depth, and gain shall be adjusted to optimize the image quality, and the target nodule should be placed in the center of the image with a proper size (Fig. 2A). The probe should be slightly placed on the thyroid, and enough couplant should be applied on the skin. The patient should keep his/her position, avoid over-turning to the back or side, and the breath shall be held as well.
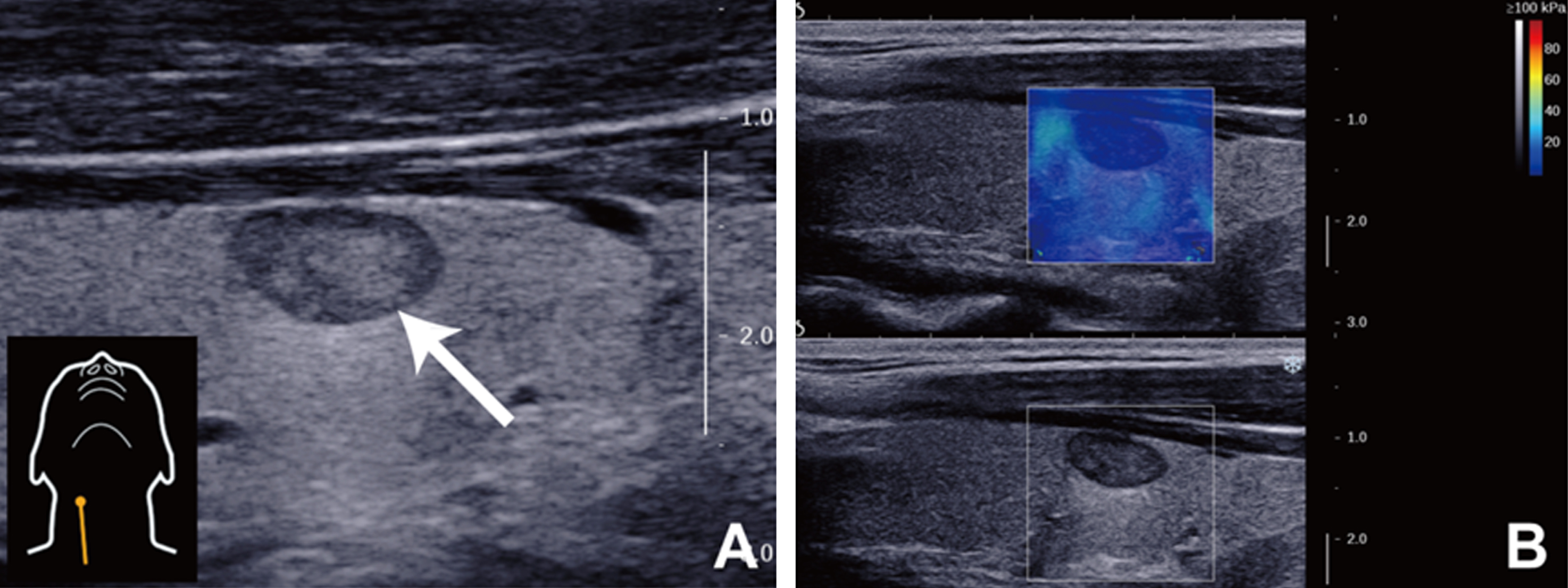
B-mode gray scale image (A) and SWE image (B) of thyroid (courtesy of People’s Medical Publishing House [1]).
(2) SWE: In order to overcome the influence of carotid pulsation on shear wave measurement, longitudinal SWE should be performed for routine examination. When selecting and adjusting the ROI are conducted, the area should cover the whole lesion as well as peripheral normal thyroid tissues, and the diameter of ROI is suggested to be 2–3 times of the nodule. The upper edge of the ROI should be more than 1 cm from the skin, and the lower edge should be less than 4 cm in depth. The image shall be frozen and saved after 2–3 seconds of stabilization (Fig. 2B).
(3) Measurements: The Young’s modulus of the nodule can be calculated using the Q-Box tool; the Q-Box of measurement should cover the whole nodule, but not the peripheral tissue (Fig. 3A). The Young’s modulus could be calculated using the Q-Box ratio; when the diameter of Q-Box adjusted to 2 mm, the first Q-Box should be placed in the stiffest area within the nodule, and the second Q-Box should be placed in the peripheral normal tissue as a reference (normal thyroid tissues with the same depth are recommended) (Fig. 3B).
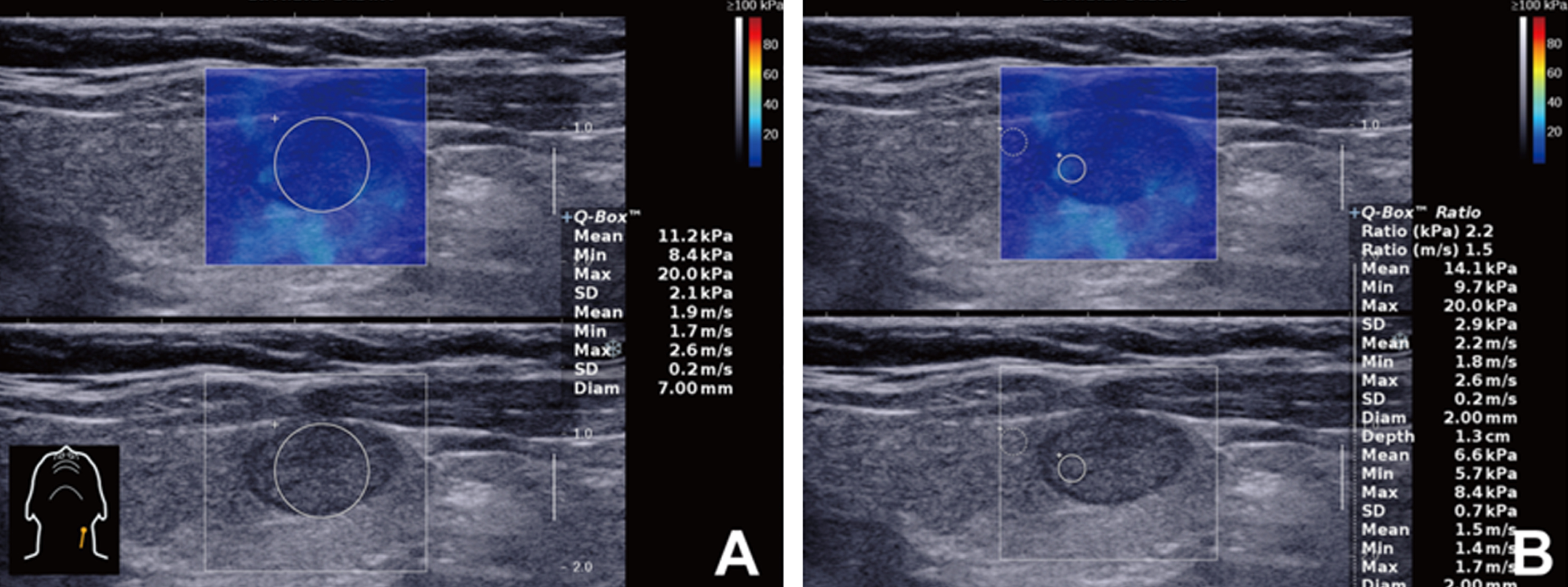
SWE measurement. A: nodule measurement (mean, max, min, and standard deviation (SD)), Q-Box is placed in the whole nodule. B: Q-Box Ratio measurement: the first Q-Box should be placed in the stiffest area within the nodule, and the second Q-Box should be placed in control thyroid tissues. (Courtesy of People’s Medical Publishing House [1]).
Based on the experience of several scholars, the median obtained from 10 measurements is more accurate. However, according to our multi-center study and a prospective DEGUM multi-center study for SE from Friedrich-Rust and Bojunga et al. [15], 5 measurements presented satisfactory results. Therefore, the measurement is recommended to be repeated for 5–10 times. Longitudinal imaging is suggested for routine examination, because this avoids the influence of carotid pulsation. Meanwhile, cross-sectional measurement can be performed as well.
Quality control
During SWE examination, enough couplant should be applied, and the probe should be carefully placed on the neck skin in front of the thyroid without compressing. Before freezing the image, patients are told to hold their breath, and the time required for image stabilization should be more than 2 seconds. After stabilizing for more than 2 seconds, the image could be captured if there is no obvious compression artifact or controllable external disturbance (Fig. 4). The image is regarded to be failed if there is no color within the ROI, or only variegated colors are being displayed. The operator should follow the operation protocol in order to acquire stable and reliable elastic images, but aside to improper operation or poor patient compliance; the image quality is also associated with many other factors, such as the properties of the nodule (malignant tumor), internal components (cystic changes and calcification), and location (deep or near the trachea) of the nodules.
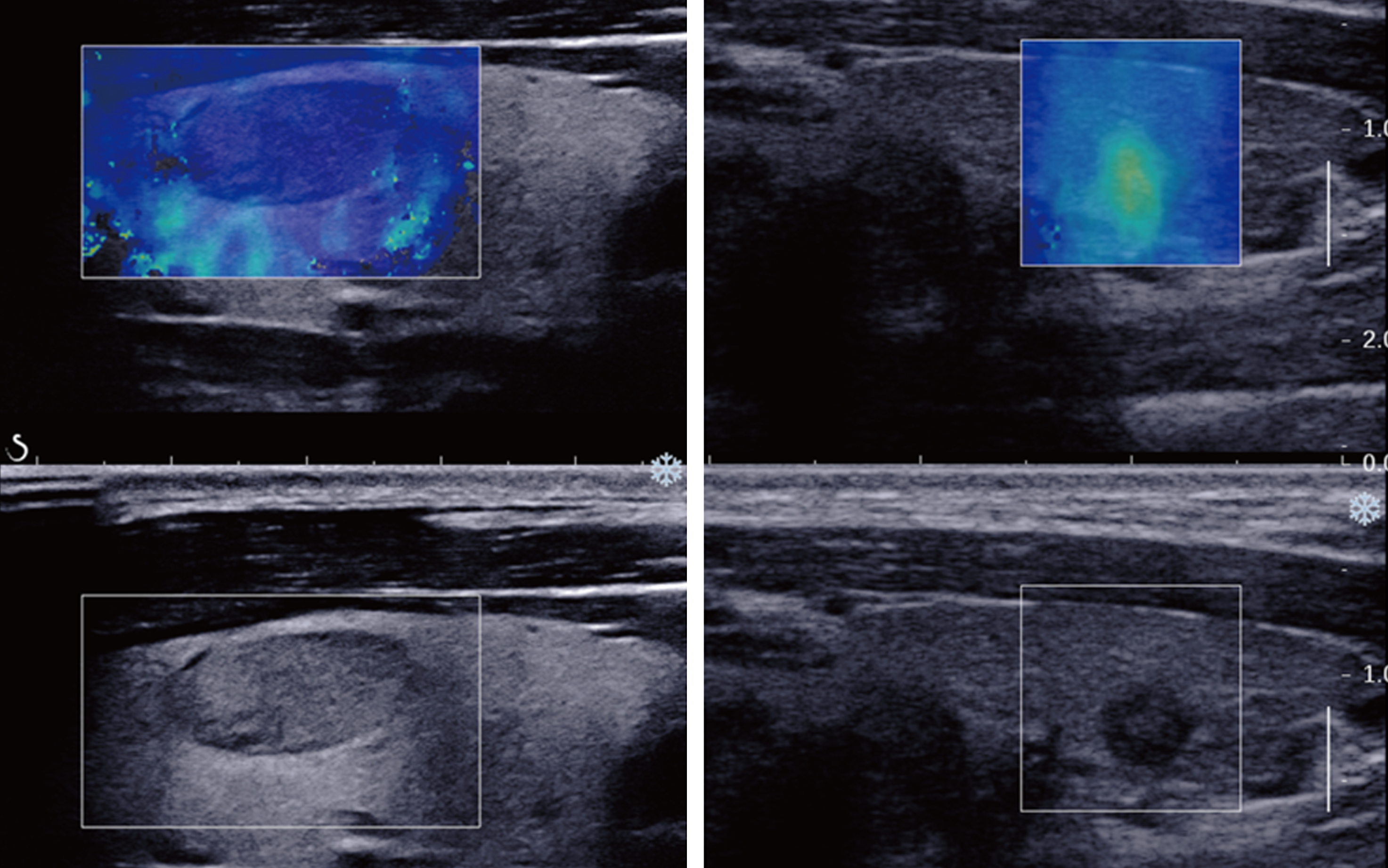
A qualified image (courtesy of People’s Medical Publishing House [1]).
Therefore, acquisition of qualified images needs us to: Set appropriate device parameters; Ask patients to hold their breath and stay when image is captured; Place the probe perpendicular to the neck without applying external pressure, and the hand should be kept during measurement (Fig. 5); Select a proper ROI that can cover the whole nodule and a part of the peripheral tissues. The ROI should be neither very deep or very shallow, and the transverse diameter of the nodule should expand 1/3–1/2 of the whole area (Fig. 6); Maintain uniformity of the proximal and distal fields, allow adequate image stabilization, and avoid pressure artifacts.
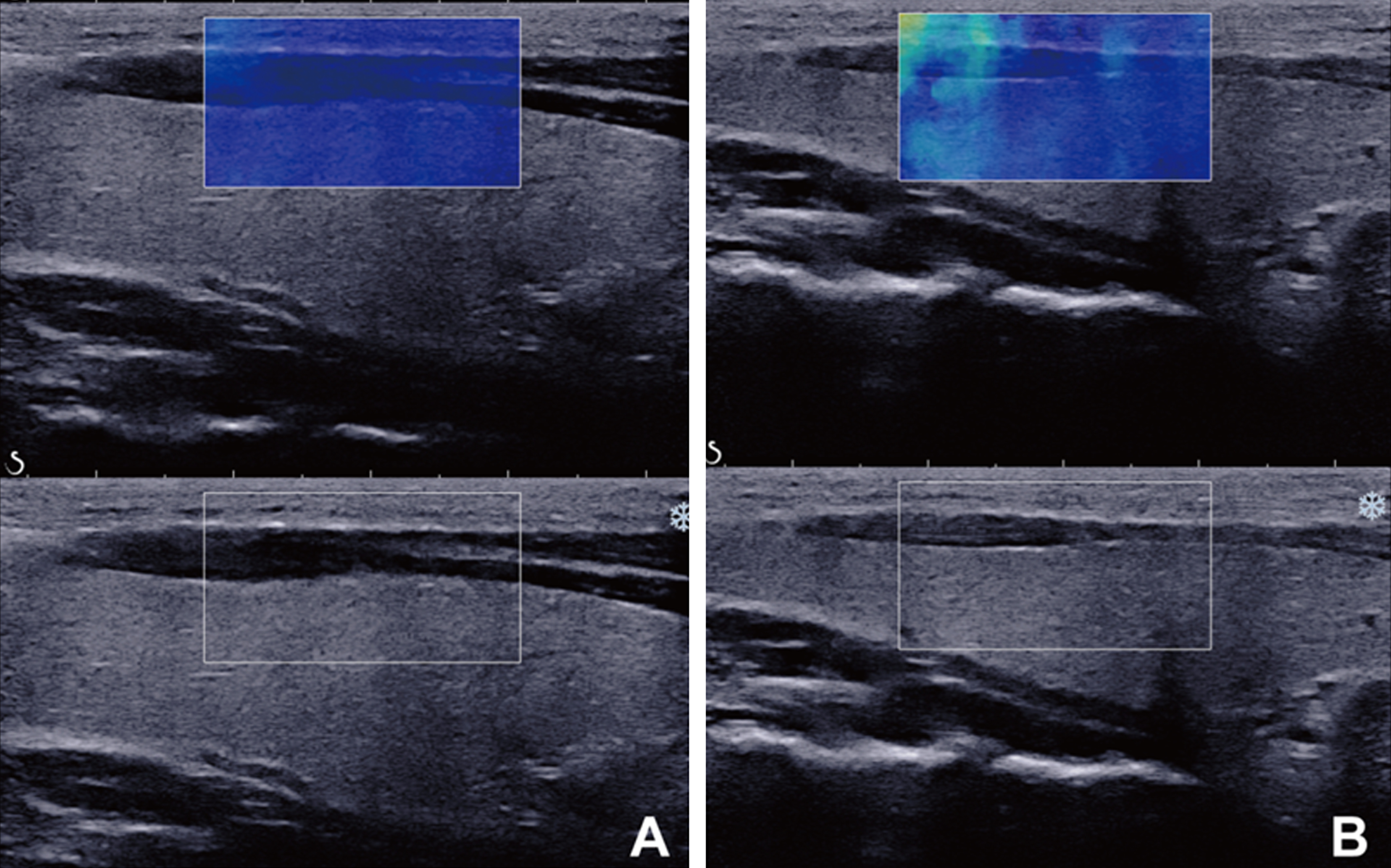
Influence of pressure on SWE examination. A: no pressure, the image is uniform. B: compression from probe and compression artifacts can be seen (Courtesy of People’s Medical Publishing House [1]).
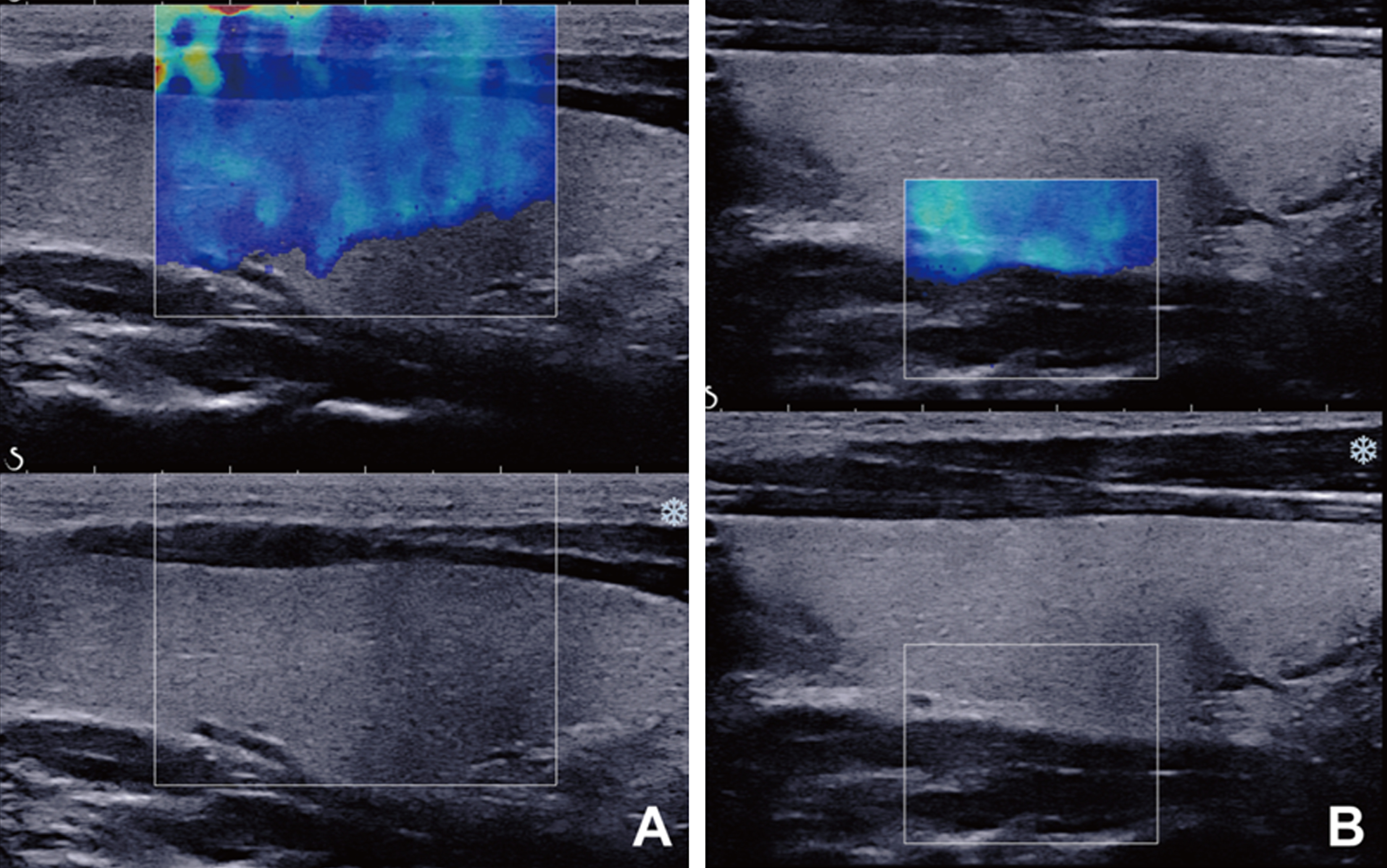
Other factors affecting the image quality. A: the ROI is very large. B: the ROI is very deep (Courtesy of People’s Medical Publishing House [1]).
Since SWE is performed on the basis of conventional ultrasound, the elasticity of shear wave is associated with the quality of gray-scale images. Therefore, in order to obtain high-quality SWE images, clear conventional ultrasound images are prerequisite. During operation, the probe should be perpendicular to the skin, as a tilted angle would cause slight movement on the probe, which further affects the image quality. Also, the site and depth of measurement, and carotid pulsation can all affect the accuracy of the results. In general, longitudinal scanning at sites less affected by carotid pulsation is recommended for SWE examination. In addition, when a high-frequency linear-array transducer is used for thyroid SWE, the maximum depth for an accurate measurement result should be less than 4–5 cm. The acoustic wave would be attenuated if the nodules are located very deep, and the transverse shear wave signal might be very weak to be accurately detected. Another noteworthy point is that, for all suppliers, the focus area in SWE cannot be adjusted by operators. The system will automatically focus on the ROI or observation, and display the signal for SWE.
Of the majority of SWE-associated studies use the max, mean, and other quantitative elasticity values to assess the hardness of nodules; some also take the peripheral thyroid or muscle tissues as the control and calculate the ratio of hardness. It should be noted that the ratios obtained from SWE might have different values with m/s or kPa as the units.
Clinical application of SWE in thyroid nodules
Differential diagnosis between benign and malignant nodules
Diagnostic efficiency
Literature search with keywords “shear wave elastography+thyroid” resulted a review of 6 meta-analyses [16–21]. These 6 meta-analyses included more than 10, 000 thyroid nodules, and there might be some overlapping studies. According to the results, the sensitivity and specificity of SWE in differentiating benign and malignant thyroid nodules are at the ranges of 0.79–0.86 and 0.84–0.90, respectively. All studies suggest that SWE can be used as a supplementary method for thyroid differential diagnosis, and it helps select patients for surgical treatment. However, in a recent meta-analysis conducted by Nattabi et al. [22] (including 2139 patients with 2851 nodules, out of which 1759 were benign and 1092 were malignant), the sensitivity, specificity, and area under curve (AUC) were only 0.66 (95% CI: 0.64–0.69), 0.78 (95% CI: 0.76–0.80), and 0.851, respectively, indicating that the value of SWE in thyroid diagnosis might be further discussed.
The reproducibility of SWE measurement
Many research teams have systemically evaluated the reproducibility of SWE in diagnosing thyroid diseases. Veyrieres et al. [23] analyzed the value of 102 lesions obtained from SWE, and obtained an inter-operator correlation coefficient of 0.97. Thus, the inter-operator and intra-operator reproducibility of SWE measurement is relatively high.
Diagnostic threshold
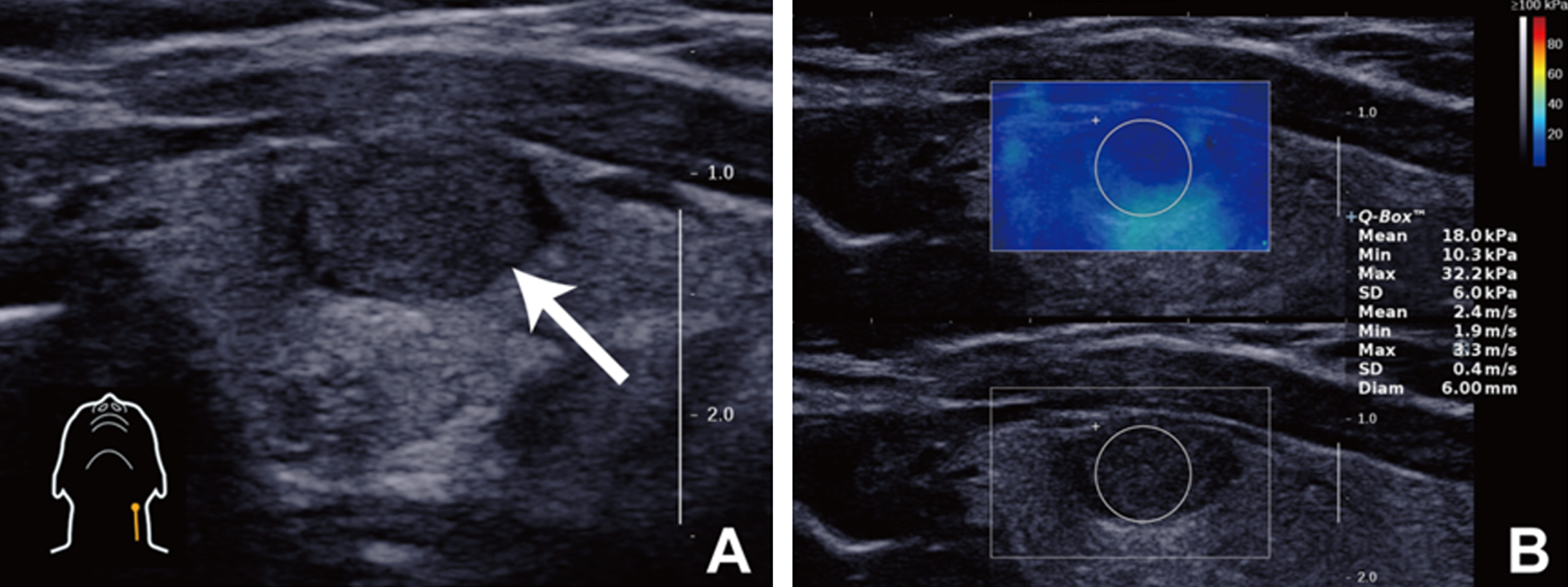
Generally, Young’s modulus and shear wave speed of malignant thyroid nodules are higher than benign ones (Figs. 7 and 8). Veyrieres et al. [23] suggested that the optimal cut-off value for SWE in diagnosing benign or malignant thyroid lesions was 66 kPa (4.70 m/s), and the corresponding sensitivity and specificity were 80% (95% CI: 62.5–90.9%) and 90.5% (95% CI: 86.1–93.6%), respectively. Park et al. [24] pointed out that Emean ≥85 kPa and Emax≥94 kPa were independent risk factors for malignant thyroid nodules, and combined application with conventional ultrasound could improve the sensitivity of diagnosis to 95.0% and 95.0%, respectively. Sebag et al. [25] compared the features of conventional ultrasound and SWE of 146 nodules from 93 patients, and reported that combined application of SWE increased the sensitivity of gray-scale ultrasound from 51.9% to 81.5%, and the specificity was 97.0% for both measurements. This indicates that SWE plays an important role in differentiating benign and malignant thyroid nodules. In a recent dual center study [26], Dobruch-Sobczak et al. suggested that Emax was an indicator with the most diagnostic significance. It had an OR value of 2.96, and when the cut-off value was 67 kPa, the sensitivity and specificity were 42.0% and 88.2%, respectively.

A case of nodular goiter. A: The nodule is solid, regular and hypoechoic on B-mode gray scale ultrasound. B: The nodule is homogeneous blue (soft) on SWE map, Emax = 17.0 kPa and Emean = 10.4 kPa.
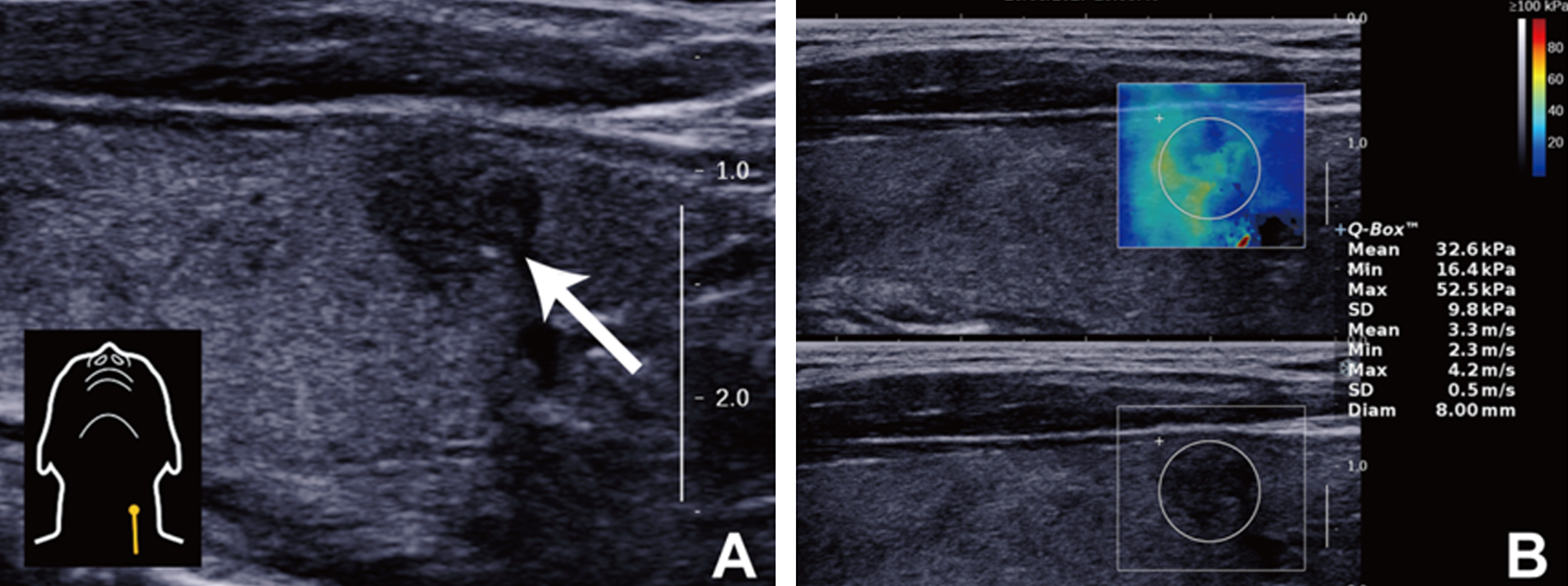
A case of papillary thyroid carcinoma. A: The nodule is solid, hypoechoic and micro-calcification on B-mode gray scale ultrasound. B: The nodule is heterogeneous colorful (hard) on SWE map, Emax = 52.5 kPa and Emean = 32.6 kPa.
It should be emphasized that there are currently no results from prospective multi-center studies, thus the above-mentioned results need to be carefully considered. Based on mid-term results of our multi-center research for thyroid SWE (including 844 thyroid nodules with 435 benign and 409 malignant), when Emax was used, the cut-off value, sensitivity, and specificity were 46.1 kPa, 66.3%, and 74.0%, respectively; when Emean was used, the cut-off value, sensitivity, and specificity were 27.7 kPa, 51.8%, and 82.5%, respectively; when ESD was used, the cut-off value, sensitivity, and specificity were 5.8 kPa, 79.0%, and 57.5% respectively. Our suggestions for the above-mentioned results are as follows: first, the diagnostic efficiency of SWE is not prominent when it is merely used, thus, the results must be analyzed in combination with conventional ultrasound and SWE; second, different quantitative indexes might present varying levels of sensitivity or specificity, therefore, these indexes should be appropriately selected according to different needs instead of using just one (Table 2).
The diagnostic performance and threshold of SWE
Note: SWE, shear wave elastography; SEN, sensitivity; SPE, specificity; AUC, area under ROC receiver operating characteristic curve.
The Bethesda system is recommended for classification of FNAC results. Bethesda category 3 includes atypia of undetermined significance or follicular lesion of undetermined significance (AUS/FULS), and category 4 includes follicular neoplasm or suspicious for a follicular neoplasm (FN/SFN). Nodules of the two categories are defined as indeterminate nodules. A certain part of indeterminate nodules is malignant, and its malignancy significantly varies in different centers, imposing huge difficulty for clinical practice. Repeated FNAC, molecular test, and diagnostic surgery are often performed for such nodules, however, the outcome is far from satisfaction. Samir et al. [32] used SWE to analyze 35 indeterminate nodules (16 AUS/FLUS and 19 FN/SFN), which obtained 22.3 kPa as the cut-off value, and the AUS, sensitivity, and specificity were 0.81, 82%, and 88% respectively, thus, they suggested that SWE is accompanied with high diagnostic value for nodules with indeterminate FNAC. Recently, Bardet et al. [33] conducted a prospective dual-center study including 131 nodules with diameter >15 mm with indeterminate FNAC results (classified as Bethesda category 3 and 4), and found that the Young’s modulus of malignant and benign nodules were no statistically significance (Emean: 20.2 vs. 19.6 kPa; Emax: 34.3 vs. 32.5 kPa; Eratio: 1.57 vs. 1.38; all P > 0.05). Thus, further studies are still required to determine the diagnostic efficiency of SWE in thyroid nodules with indeterminate FNAC results (Figs. 9 and 10).
A case of nodular goiter with Bethesda category III on FNA. A: The nodule is solid and hypoechoic on B-mode gray scale ultrasound. B: The nodule is homogeneous blue (soft) on SWE map, Emax = 32.3 kPa and Emean = 18.0 kPa.

A case of papillary thyroid carcinoma with Bethesda category III on FNA and positive BRAF mutation. A: The nodule is solid, irregular, and hypoechoic on B-mode gray scale ultrasound. B: The nodule is heterogeneous colorful (hard) on SWE map, Emax = 77.0 kPa and Emean = 54.8 kPa.
SWE can also be used to predict extra-thyroidal extension and cervical lymph node metastasis. Park et al. [34] studied the Young’s modulus of 208 papillary thyroid carcinomas, and attempted to use SWE to determine extra-thyroidal extension. A multi-factor analysis revealed that extra-thyroidal extension is associated with Emean, Emax, and Emin, and the authors believed that SWE could be used as a supplementary method for determining extra-thyroidal extension. Another study [35] used SWE to predict cervical lymph node metastasis in 363 cases with papillary thyroid carcinomas, and the results showed that Emean and Emax were associated with central lymph node metastasis, whereas Emin was associated with lateral neck metastasis. Taking Emean≥124 kPa and Emax≥138 kPa as the cut-off values for diagnosing lymph node metastasis, the AUC was 0.659 and 0.667, which indicates that SWE helps predict cervical lymph node metastasis of papillary thyroid carcinoma (Fig. 11).

A case of papillary thyroid carcinoma with cervical lymph node metastasis. A: The nodule is mostly solid, lobulated margin, and multi-micro-calcification on B-mode gray scale ultrasound. B: The nodule is heterogeneous colorful (hard) on SWE map.
The signal intensity of elastography determines the quality of SWE image. If the signal would be very weak, the shear wave speed could not be measured. Therefore, during SWE examination, the operator should be careful to avoid pressing the probe, leading to remove the human’s influence on the accuracy of detection shear wave properties [36, 37]. Lam et al. [38] found that, the hardness of papillary thyroid carcinoma detected by SWE was increased at a higher rate, when compared to benign nodules with the increase of probe compression. Thus, the influence of probe compression should not be ignored, and it might cause lack of comparability of results obtained from different centers or different operators. In addition, Wang et al. [39] reported that the size of thyroid nodules may also affect the results of SWE.
The size of ROI is negatively correlated with SD. The elastic map of SWE is superimposed with 2D anatomical image by pseudo-color coding, thereby achieving real-time speed of the shear wave. The ROI can be placed within the hardest area of the lesion, or in peripheral thyroid tissues, or neck muscles, leading to acquire quantitative data and calculate the ratio. If the ROI covers cystic or calcified areas, wrong results might be obtained as well.
The influence of thyroid background on thyroid SWE
Clinically, thyroid diffuse diseases mainly include hyperthyroidism, Hashimoto’s thyroiditis, subacute thyroiditis, and nodular goiter. Generally, these four diseases are diagnosed by clinical symptoms, laboratory examinations, and ultrasound imaging. As thyroid diffuse disease tends to develop into extensive sclerosis of the whole gland, glandular inflammation and different degrees of scarification would lead to varying levels of thyroid stiffness. Magri et al. [40] performed SWE on 75 patients with benign thyroid nodules diagnosed by cytology. Among them, 33 cases were combined with Hashimoto’s thyroiditis (HT), and 42 were with single or multiple goiters (non-HT). According to the results, the stiffness of thyroid tissues outside the nodule of HT patients was greater than that of non-HT patients, however, the difference was not statistically significant. On the other hand, Menzilcioglu et al.’s study [41] on subacute thyroiditis reported that the hardness of inflammatory tissues would increase, thus any focal inflammatory lesion needs to be differentiated from thyroid carcinoma.
Liu et al. [42] found that SWE could differentiate thyroid nodules in patients accompanied with autoimmune thyroiditis. The study included a total of 243 patients with 286 thyroid nodules confirmed by surgical pathology, and patients were divided into the HT and non-HT groups according to the presence of chronic lymphocytic thyroiditis. The results showed that for the 117 nodules in HT group and 169 nodules in non-HT group, no statistically different Young’s modulus was identified between the two groups, no matter compared for malignant or benign nodules, whereas the extra-nodular thyroid tissue of the HT group was greater than that of the non-HT group, and the difference was of statistical significance. Vlad et al. [43] also found that the stiffness of thyroid parenchyma would significantly increase when patients are accompanied with autoimmune thyroid disease. Thus, by quantitatively evaluating tissue stiffness in patients with diffuse thyroid disease, SWE helps assess the level of thyroid fibrosis for patients with HT, thereby providing reference data for clinical diagnosis.
Different pathological types
When SWE is used to determine benign or malignant thyroid nodules, the operator should be aware that not all thyroid carcinomas are hard; some of them may also be soft or heterogeneous (Figs. 12 and 13). For example, some follicular thyroid carcinoma are accompanied with low stiffness, because it is composed of follicles with different degrees of differentiation. As numerous studies reported that SWE has provided a better diagnostic outcome, follicular thyroid carcinoma is still difficult to be differentiated from benign thyroid nodules. In addition, elastogryphy overlapps broadly for adenoma and carcinoma. In such cases, additional diagnostics such as contrast-enhanced ultrasound (CEUS), B-mode US, Duplex US, and scintigraphy, are needed [44, 45]. Samir et al. [46] retrospectively analyzed cases whose FNAC results were follicular neoplasm or suspicious for follicular neoplasm, and compared their preoperative conventional ultrasound and SWE results with postoperative pathological results, who eventually aimed to evaluate the accuracy of preoperative SWE in diagnosing follicular thyroid carcinoma. The results showed that by taking the mean Young’s modulus of 22.3 kPa as the cut-off value (lower than the Young’s modulus reported by previous studies), the sensitivity, specificity, and positive and negative predictive values were 82%, 88%, 75%, and 91%, respectively. To date, studies on thyroid medullary carcinoma only involved SE [46], and few researches have reported the use of SWE for evaluation. Another study also suggested that the hardness of typical papillary thyroid carcinoma is greater than that of atypical papillary thyroid carcinoma or other types of thyroidcarcinomas [33].

A case of follicular thyroid carcinoma. A: The nodule is solid, regular, and isoechoic on B-mode gray scale ultrasound. B: The nodule is homogeneous blue (soft) on SWE map, Emax = 21.8 kPa and Emean = 9.8 kPa.

A case of medullary carcinoma. A: The nodule is solid, regular, and hypoechoic on B-mode gray scale ultrasound. B: The nodule is heterogeneous blue (moderate soft) on SWE map, Emax = 44.8 kPa and Emean = 16.1 kPa.
Sometimes, SWE imaging might fail when nodules are accompanied with cystic or calcified components [47]. Bhatia et al. [48] performed pathological analysis on 21 papillary thyroid carcinomas, out of which 18 immeasurable specimens contained heterogeneous pathological components, and 9 contained calcified components. Besides, nodules containing either or both of the features accounted for 95%. On the other hand, out of the 29 samples with detectable data, 25 were with homogeneous pathological composition, and only one contained coarse calcification. The results of this study are in accordance with the hypothesis. Bhatia et al. [48] also found that for benign nodules, no significant differences in SWE imaging were identified between solid nodules and cystic components, or between calcified nodules and non-calcified nodules. However, Vorlander et al. [49] reported that compared with non-calcified thyroid nodules, the rate of misdiagnosis was significantly higher for calcified thyroid nodules.
Comparison of SWE with other ultrasound elastography methods
The ultrasound elastography guidelines published by EFSUMB, WFUMB, and many others studies all point out that [7–8] SWE is an effective supplementary method for gray-scale and color Doppler ultrasound. In order to obtain reliable SWE results, both appropriate equipment and experienced operation are required. Generally, it is suggested to avoid pre-compression of the tissue, and the probe should be placed perpendicular to the target area. Moreover, the size and location of ROI should be concerned; sites of accessories, calcified or cystic areas within the nodules should be avoided. Additionally, the quality of imaging also depends on high patient cooperation. In the future, technological innovation might reduce the variability of SWE, and this would hopefully improve the accuracy of examination.
Comparing with other elastography techniques, SWE, from the theoretical perspective, has the advantage of less dependency on an operator. However, strain elastography has a shorter learning curve [50], and it can rapidly provide high-quality images by real-time feedback of the operator. It is believed that SWE is a technique with low dependency of operator and high repeatability, however, due to the lack of relevant studies, its efficiency needs to be verified by multi-center researches in the future [51]. Liu et al. [27] compared SWE with SE; their study included 49 patients with 64 thyroid nodules confirmed by surgical pathology, out of which 19 were papillary thyroid carcinomas and 45 were benign nodules, and the results showed that taking Emean≥3 8.3 kPa and elasticity score ≥4 as the cut-off value, the sensitivity and specificity were 68.4% and 79.0% for SWE, and 86.7% and 84.4% for SE, respectively. Hence, Liu et al. believe that in comparison with real-time elastography, SWE is accompanied with low sensitivity, but with high specificity, thus it could be used in differential diagnosis of thyroid nodules. Hu et al. [21] conducted a meta-analysis to compare the diagnostic efficiency of SE with SWE. The study included a total of 2106 benign nodules and 613 malignant nodules, and revealed that the sensitivity of these two techniques was similar (84% and 79%, respectively, P > 0.05), however, SE had a higher specificity (90% vs. 87%, P < 0.05). Besides, the overall diagnostic efficiency of SE was higher than SWE (AUC 0.94 vs. 0.83, P < 0.01). Friedrich-Rust et al. [15] performed a prospective multicenter study for differentiation of thyroid nodules using SE, including 567 benign nodules and 90 malignant nodules from 7 centers. The sensitivity, specificity and accuracy were 21%, 73%, 71%, respectively. Xu et al. [52] prospectively studied 441 thyroid nodules (116 malignant and 325 benign) by using point shear wave elastography (p-SWE) from Siemens, and found that shear wave speed was an independent predictor for thyroid carcinoma, with a sensitivity, specificity, and AUC of 71.6%, 83.4%, and 0.86, respectively, which was similar to the diagnostic efficiency of SWE [16–21]. In addition, ARFI-induced SE and p-SWE could predict cervical lymph node metastasis in patients with papillary thyroid cancer when combined with conventional US [53].
Zhang et al. [15, 48–55] suggested that p-SWE possesses good efficiency, and combined application could improve doctor’s confidence in diagnosis. Since both SWE and other elastography techniques have their own advantages, they can be jointly used in promoting the application of ultrasound elastography in diagnosing thyroid diseases (Fig. 14).

Pointed SWE of virtual touch tissue quantification (Siemens S2000, Germany). A: The nodule is solid, hypoechoic and micro-calcification on B-mode gray scale ultrasound. B: The shear wave speed is 6.59 m/s.
Even for shear wave imaging, different principles or modes will result in different image assessments or elasticity measurements (Figs. 15 and 16).

2D SWE of virtual touch tissue imaging quantification (Siemens S3000, Germany). A: The nodule is solid, hypoechoic and micro-calcification on B-mode gray scale ultrasound. B: Multiple ROI is placed in the SWE map.

2D SWE (Toshiba Aplio500, Japan). A: The nodule is solid and hypoechoic on B-mode gray scale ultrasound. B: SWE map and shear wave spread image.
He et al. [30] for the first time compared two SWE techniques (T-SWE from Toshiba and S-SWE from Supersonic) in imaging 140 thyroid nodules (93 benign and 47 malignant). The results showed that for both techniques, Emax had the highest diagnostic efficiency, with a cut-off value, sensitivity, specificity, and AUC were Emax≥26.6 kPa, 83.0%, 68.8%, and 0.816 for T-SWE, respectively, and Emax≥42.9 kPa, 63.8%, 88.2%, and 0.799 for S-SWE. Wang et al. [56] for the first time compared SWE techniques (p-SWE from Siemens and S-SWE from Supersonic) in imaging 332 thyroid nodules (216 benign and 106 malignant). For the two techniques, the hardness of thyroid carcinomas was significantly higher than benign modules (61.3 kPa vs. 21.2 kPa, 4.45 m/s vs. 2.98 m/s), and the AUC (Emax) for p-SWE and S-SWE techniques in diagnosing thyroid carcinoma was 0.813 and 0.796, respectively. Therefore, different SWE techniques should be judged objectively and selected carefully.
Zhao et al. [57] further compared the ability of 3D-SWE and 2D-SWE in diagnosing thyroid nodules. They performed both 2D-SWE and 3D-SWE for 176 patients with 176 thyroid nodules (63 malignant and 113 benign), and identified a AUC of 0.836 and 0.839, respectively, (P > 0.05), and a specificity of 82.3% and 88.5% (P = 0.039), respectively for 2D-SWE and 3D-SWE techniques. This indicates that 3D-SWE has a higher specificity than 2D-SWE. Also, for 35 cases suspicious for benign nodules on gray-scale ultrasound, 3D-SWE helps reduce unnecessary FNAC results when compared with 2D-SWE (31 cases vs. 27 cases) (Fig. 17).

A case of three-dimensional 3D SWE. A: B-mode gray scale image of transverse and longitudinal plane. B: 3D SWE from Supersonic.
To date, almost all guidelines or studies suggested that SWE should be used in combination with conventional ultrasound for diagnosing thyroid nodules. Thus, a standard SWE report should first describe features of thyroid nodule on conventional ultrasound, including nodule location, size, echo, internal component, presence of calcification, margin, internal blood supply, extra-thyroidal extension, and whether there are cervical lymph node enlargement or abnormal echoes.
Apart from these, risk stratification should be given based on ultrasound features of the nodule. Methods for stratification can be referred to the latest ATA guidelines, AACE/ACE/AME guidelines, the thyroid imaging reporting and data system (TI-RADS) proposed by Kwak et al, or TI-RADS by American College of Radiology (ACR). Each center can use different methods according to actual situations; this guideline does not make special recommendation.
It is also suggested to describe the qualitative and quantitative characteristics of nodules on SWE images; quantitative parameters could include either or both of the Young’s modulus and the shear wave speed.
At the end, a report should provide advice on the management of nodules, such as follow-up, close observation, FNA, or surgery.
Conclusions
SWE is a non-invasive technique that enables quantitative and convenient assessment of tissue stiffness. Its unique imaging principle broadens the connotation of ultrasound diagnosis and expands the field of conventional ultrasound, and it provides enriched information, as well as more objective basis for evaluating thyroid diseases. However, as a newly-developed technology, SWE still has some disadvantages, and can be affected by multiple factors. Standardized operation in combination with unified criteria would better promote the application of SWE in clinical practice. As there is no technical standard for the SWE and no comparable standards for the different companies, the recommendation level of A1 might be bold in some cases and might be challenged in the future. Moreover, exploring specific scenarios for SWE application would help maximize its clinical value. In conclusion, the SWE used in diagnosing thyroid diseases can be summarized asfollowing: SWE evaluates thyroid stiffness by detecting the Young’s modulus or the shear wave speed; the stiffness is associated with the nature of nodules. Despite simple operation and proper reproducibility of SWE, a standard operation is required to guarantee the image quality. SWE is a supplementary method that cannot replace routine ultrasound or FNA in determining thyroid nodules. SWE is of certain diagnostic value in differentiating benign and malignant thyroid nodules, however, the cut-off values and diagnostic efficiencies vary significantly in literatures. The use of SWE in solving clinical problems is a research hotspot (e.g., further stratification of nodules of indeterminate FNA cytology, or prediction of cervical lymph node metastasis). It is hopeful that new emerged technologies, such as artificial intelligence might have potentials to solve the limitations of SWE in diagnosing thyroid nodules.
Disclosure
We disclose that the Chinese version of these guidelines “Chinese Guidelines and Recommendations on the Clinical Use of Ultrasound Elastography” (Section 5: Thyroid) [1] has been published by People’s Medical Publishing House and we have been authorized to publish the English version here.
Conflicts of interest
The authors declare that there are no conflicts of interest regarding the publication of this article.
Footnotes
Acknowledgments
This work was supported by National Natural Science Foundation of China (Grant Nos. 81671695, 81371570, and 81725008), Shanghai Hospital Development Center (Grant Nos. 16CR3061B and SHDC12014229), and the Science and Technology Commission of Shanghai Municipality (Grant Nos. 16411971100 and 14441900900), and Capital Health Research and Development of Special (Grant No. 2016-2-2153), and Fundamental Research Funds for the Central Universities (Grant No. 22120170097).