
Abstract
Endometriosis is one of the most common diseases that happen in reproductive women. The main symptoms include ovarian endometrial cyst, pelvic pain, and so on. We report a case of a 23-year-old woman with a refractory long-course ovarian endometrial cyst (OEC). The patient was previously identified to have a hypoechoic mass sized 9.7 cm in diameter on ultrasound (US) in the right ovary and was tentatively diagnosed as OEC in another tertiary hospital, who was then subjected to US-guided cyst sclerotherapy while the procedure was failed since only a very small amount of viscous and sticky fluid can be aspirated. The patient was then referred to our hospital for further treatment. Pretreat contrast-enhanced ultrasound (CEUS) showed non-enhancement of the mass with a thin cyst wall and a cyst-in-cyst pattern was observed. The possibility of ovarian malignancy was ruled out and the initial diagnosis of OEC was confirmed. The patient was then subjected to US-guided cyst sclerotherapy with lauromacrogol. The interventional procedure was eventful that no fluid was aspirated as what happened in the previous hospital. Thus urokinase was used to dissolve the old, viscious and sticky blood and finally, all the fluid was aspirated. The total consumption of urokinase was 60,000 U. Then lauromacrogol as a sclerosant was injected into the cyst cavity and the cyst wall was flushed repeatedly with lauromacrogol until the aspirated fluid became light red. Finally, 20 mL lauromacrogol was reserved in the cyst and the interventional procedure cost 2 hours. The post-procedure course was uneventful without any discomfort, and the volume reduction rate of the cyst was 54%at 3-month follow-up. The visual analogue scale for the pain decreased from 4 before treatment to 1 after treatment, indicating a successful and effective outcome for the refractory long-course OEC.
Introduction
Endometriosis is defined as the presence of functional endometrium-like tissue outside the uterus [1]. Among the protean physical manifestations, ovarian endometrial cyst (OEC) is one of the commonest symptoms. Women during their reproductive age are the most vulnerable people and treatments consist of surgical removal of lesions and hormonal medication [2]. Long-time drug therapy might cause different levels of adverse effects and laparoscopic surgery is inevitable to affect ovarian function [2]. Nowadays, ultrasound (US)-guided interventional procedure for OEC provides a novel alternative method with minimal invasiveness [3]. Pretreatment contrast-enhanced ultrasound (CEUS) has been proven to possess high clinical value in differential diagnosis between OEC and other ovarian lesions [4].
Lauromacrogol (Polidocanol) is a synthetic fatty alcohol, alkyl polyglycol ether of lauryl alcohol [5]. Lauromacrogol targets at the endothelial cell and causes protein denaturation and endothelial cell death [5]. Varicose veins and other vascular malformations are the main indications for lauromacrogol [6]. In recent years, applying lauromacrogol as an intracystic sclerosant to treat cystic lesions has been increasing [7–9] and fewer adverse effects like post-procedural pain are reported when compared with the traditional sclerosant of absolute ethanol [10].
In this article, we introduced the use of CEUS before treatment of OCE to establish its diagnosis and rule out the possibility of ovarian malignancy. We also suggested a method to treat refractory long-course OEC with ultrasound-guided administration of urokinase and lauromacrogol.
Case report
Patient
A 23-year-old female patient had a history of dysmenorrhea and occasional lower abdominal pain after menstrual period for 10 years, and the visual analogue scale (VAS) for the pain was about 4. Her menstrual colic suddenly aggravated in 2015 and the pain could be relieved only after taking ibuprofen orally. US examination in a local hospital revealed an ovarian cyst and the size of the cyst was not clear. The patient did not receive any other treatment until June 2020. The patient was tentatively diagnosed as OEC in another tertiary hospital and was then subjected to US-guided cyst sclerotherapy while the procedure was failed since only a very small amount of viscous and sticky fluid can be aspirated. The planned cyst sclerotherapy had to be terminated. The symptom of dysmenorrhea did not improve after the operation, thus the patitent was referred to our hospital for further treatment. The patient had neither abnormal vaginal bleeding nor an irregular menstrual period during the course. Laboratory test revealed CA 199 was slightly increased, measuring 40.67 U/ml.
Imaging findings
Conventional ultrasound
Conventional ultrasound was performed using a LOGIQ E9 scanner (GE Healthcare, Milwaukee, WI, USA) with a 1–5 MHz convex transducer. The gray-scale US showed that there was a homogeneous hypoechoic mass measuring 9.7×5.0×6.0 cm in length, width and height in the right ovary area (Fig. 1). No evident abnormalities were observed in the uterus and pelvic cavity. CDFI did not demonstrate obvious blood flow inside the mass (Fig. 1).
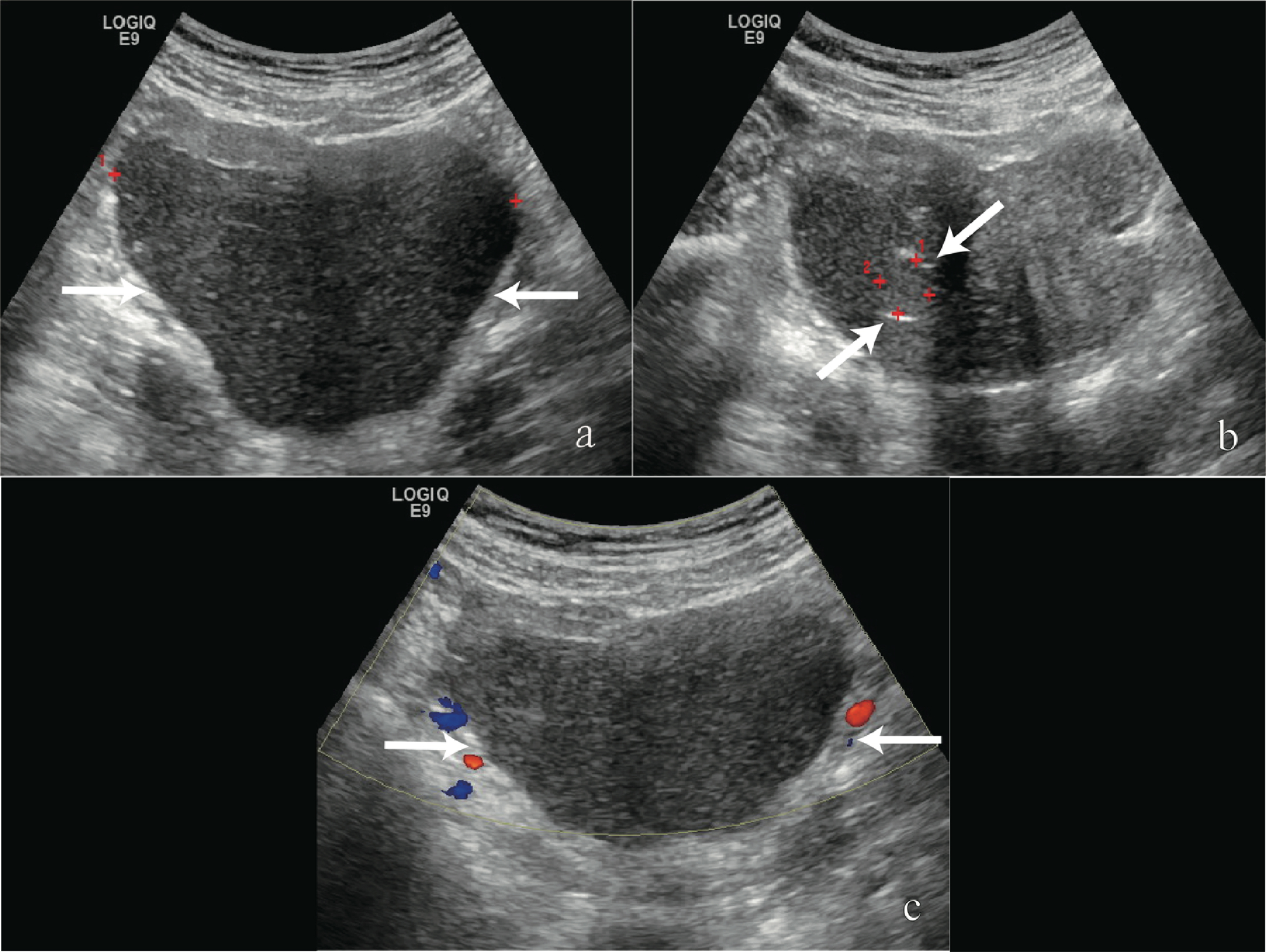
A 23-year-old female patient with an ovarian endometrial cyst in the right ovary area. (a) Conventional ultrasound showed an anechoic lesion measuring 9.7×5.0×6.0 cm in length, width and height in the right ovary area (arrows). (b) Conventional US demonstrated a small cyst inside the lesion (arrows). (c) Color Doppler flow imaging (CDFI) did not show blood flow signal inside the lesion (arrows).
To confirm the diagnosis of OEC and rule out the possibility of ovarian malignancy, CEUS was then performed with the same US scanner and transducer by the same radiologist. Sulphur hexafluoride microbubbles(SonoVue®, Bracco, Italy) as the contrast agent was used in the case. A bolus injection with 2.4 mL of SonoVue® was conducted via the antecubital vein, followed immediately by a flush with 5 mL of saline solution (0.9%sodium chloride). CEUS showed a rim-like slight hyperenhancement around the mass after injection, indicating the cyst wall. No enhancement was observed within the mass, confirming the diagnosis of OEC. Another small cystic lesion measuring 1.4×1.2 cm was seen in the big cyst, that was, the cyst-in-cyst pattern was observed (Fig. 2).
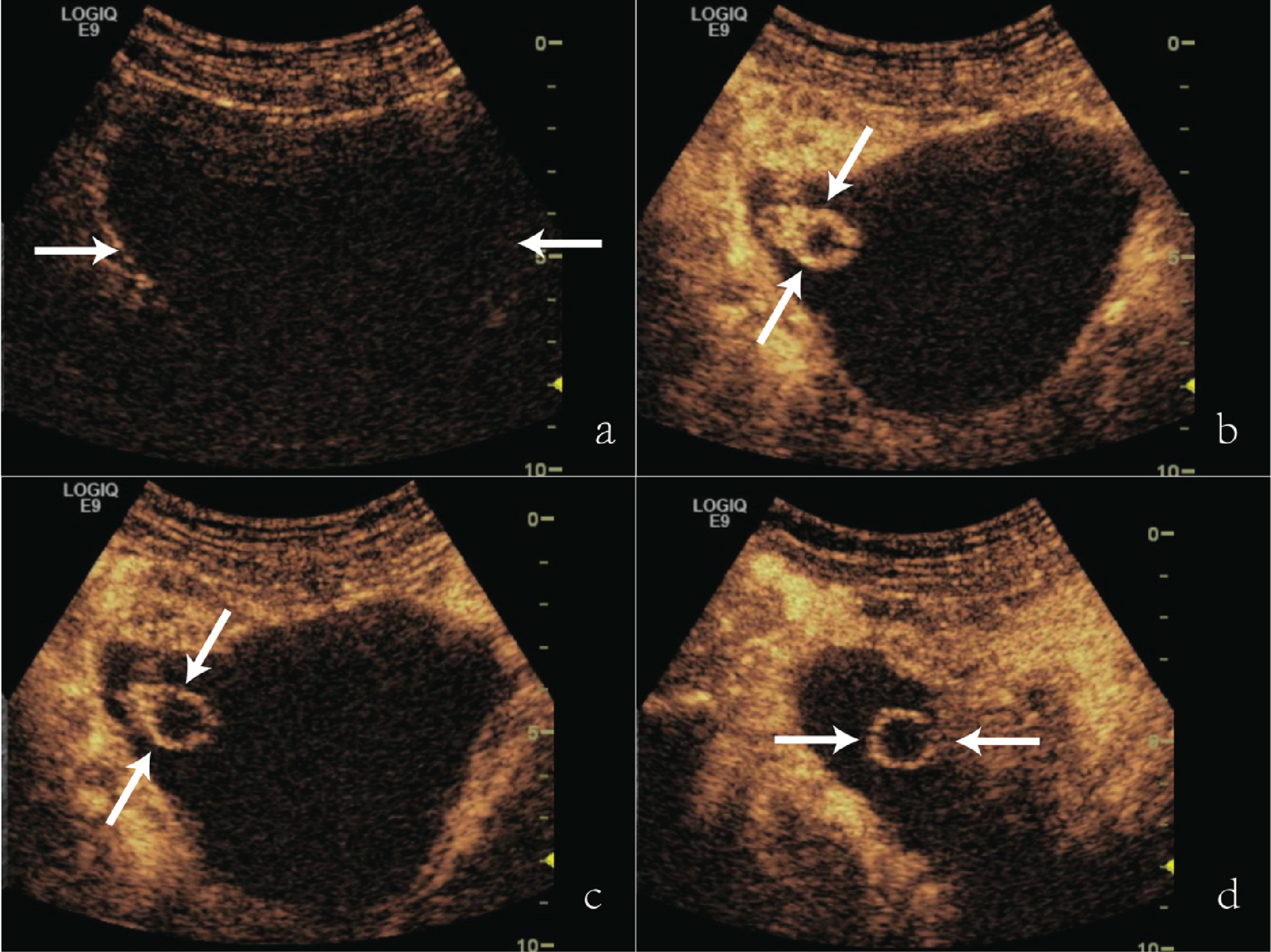
Contrast-enhanced ultrasound (CEUS) of the OEC. (a) Contrast agent is injected (0s after administration), the arrows pointed the cyst. (b) The early stage shows a slight hyperenhancement of the cyst wall after injection. No enhancement is observed inside the large cyst and there is another non-enhanced small cystic lesion measuring 2.0×1.5 cm (arrows) (30s) in the large cyst. (c) The enhancement of the small cyst wall (arrows) is slightly degraded during the late stage in cross section (3 min). (d) The late stage in vertical section also shows the iso-enhancement of the cyst wall (arrows).
The conventional T1 weighted imaging (WI) was obtained on a 3.0-T MRI scanner with a minimal slice thickness of 3 mm, a gradient strength of 40 mT/m, a gradient slew rate of 200 mT/ms (Magnetom Verio; Siemens; Germany). The enhanced contrast agent was gadopentetate dimeglumine (Magnevist; Bayer Schering; Germany). T1WI and enhanced fat-suppressed T1-weighted imaging were collected. All examinations were performed in a high-field-strength (1.5 94 Tesla) with phased array coils for signal reception.The magnetic resonance imaging (MRI) showed a cystic lesion measuring 9.5×7.5×6.3 cm in length, width and height with an intact cyst wall and mixed signals inside (Fig. 3), which showed high signal on T1WI. A patch of the abnormal signal was found in the cystic lesion and showed iso-signal and low signal on T1WI. No evident enhancement was seen in the lesion during enhanced fat-suppressed T1-weighted imaging.
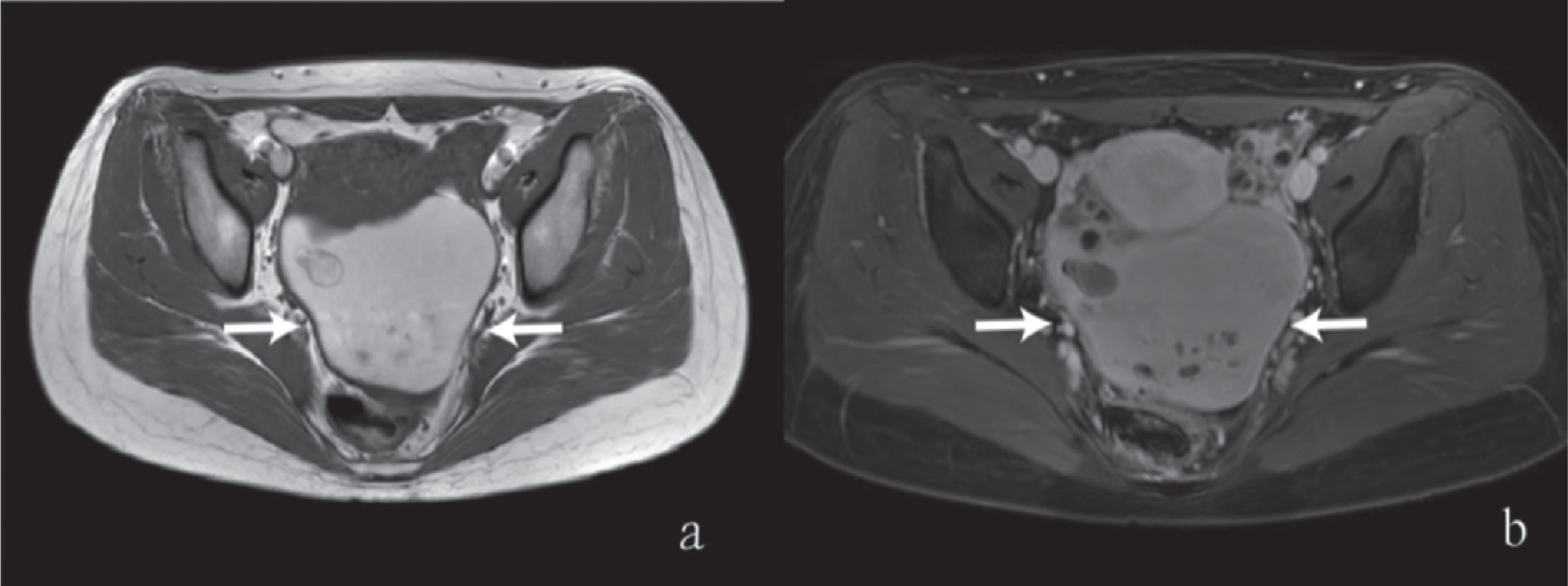
The magnetic resonance imaging (MRI) showed a cystic lesion measuring 9.5×7.5×6.3 cm in length, width and height with intact cyst wall and mixed-signal inside. (a) The mixed signal part showed high signal in TIWI (arrows). (b) Contrast enhanced fat-suppressed T1-weighted imaging showed no obvious enhancement inside the cyst (arrows).
Informed consent of the patient was obtained before US-guided cyst sclerotherapy. After the safe puncture path was confirmed, we applied local anesthesia with 2%lidocaine from the puncture site to the surface of the cyst. Meanwhile, 0.1 mg fentanyl citrate and midazolam were used for intravenous sedation. We selected a 16G PTC needle for puncturing since the previous procedure was failed in another tertiary hospital. After the PTC needle passed through the cyst wall and the tip approached the center of the cyst, a syringe was attached to draw out the fluid.
The aspirate fluid was chocolate-like dark and viscious (Fig. 5),and it was hard to be drained smoothly (Fig. 4). To dissolve the thick and solid contents within the old, viscious and sticky blood fluid, urokinase was firstly injected into the cystic cavity. Then normal saline was injected to dilute the fluid in the cystic cavity (Fig. 4). The content inside the cyst became thinner and thinner after flushing urokinase and normal saline alternatively. In total, 165 mL chocolate-colored and viscous fluid were extracted from the cavity after consuming 60,000 U urokinase. The cystic cavity was then flushed with normal saline continuously until the rinse solution became clear. All the normal saline was extracted and 20 ml 1%lauromacrogol was injected into the cyst. The cyst wall was rinsed repeatedly 30–40 times with lauromacrogol (Fig. 4). Finally, we extracted the previously injected sclerosant until the fluid became light red and another 20 ml lauromacrogol was injected into the cavity and was preserved in the cyst (Fig. 4). In total, the interventional procedure cost 2 hours.

The dark chocolate-like viscous and sticky cyst fluid which was difficult to be aspirated.
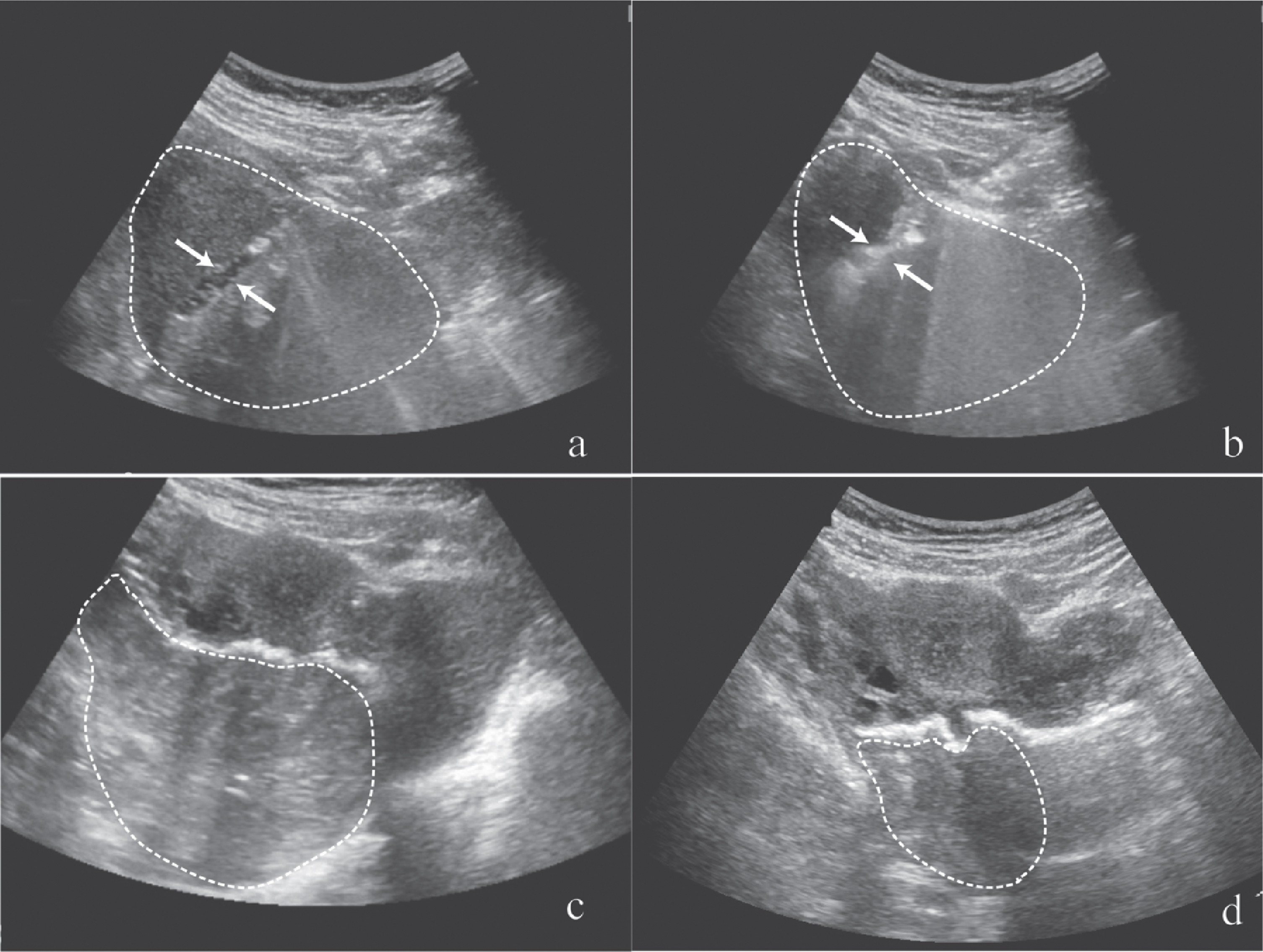
Ultrasound-guided intervention procedure: aspiration and sclerotherapy. A 16G PTC was punctured into the cyst (outline), but the thick, viscous bloody content in the OEC couldn’t be extracted (arrows). (b) Urokinase (arrows) was injected into the cyst (outline) to dissolve the viscous cyst fluid which had condensed into solid-like substance. (c) 20 ml 1%lauromacrogol was injected into the cyst as sclerotherapy and the cyst wall was flushed rapidly with lauromacrogol. Arrows showed the enlarged cyst with lauromacrogol inside. (d) 20 ml lauromacrogol was reserved in the cyst at the end of the procedure (arrows).
The minor complication of mild fever (highest temperature up to 38°C) was developed and was relieved 3 days after the procedure without additional treatment. The efficacy was assessed three months later with conventional US and laboratory tests. The US revealed that the size of the remained cyst was 7.2×4.6×4.0 cm in length, width and height. The volume reduction rate was 54%. Laboratory test revealed the serum CA 199 returned to normal level. The VAS for the pain decreased from 4 before treatment to 1 after treatment.
Discussion
Conventional treatment of OEC
Endometriosis is a gynecologic disorder primarily affecting reproductive women. Its pathological character is the growth and periodic bleeding of ectopic endometrial tissue outside the uterus [11]. Among the numerous symptoms, OEC is the most common one. The oral contraceptive pill, both combined or progestin-only, is widely used as the first-line treatment for dysmenorrhea or chronic pelvic pain, particularly in primary care [12]. However, drug therapy has a limited curative effect on the existing OEC, especially on a huge cyst with a long-process. Meanwhile, a significant number of patients complain of intolerable side-effect in the medical treatment [13]. On the other hand, almost every surgical procedure aimed eliminating at an endometrioma is bound to impair ovarian function and recurrence cannot be avoided.
Evaluation of OEC by US
With the development of US technology and improvement of the resolution of US gray scale imaging, the detection rate of ovarian cysts increases gradually. Innovative technology like CEUS plays an important role in diagnosing malignancy and monitoring intervention procedures [14]. While EFSUMB guildelines do not recommend gynecological clinical indications for the use of CEUS, findings suggest that the absence of any enhancement in adnexal masses corresponds to benign lesions [15]. Rennert J et al. demonstrate that CEUS is a valuable tool for post-interventional succuss control following thermal ablation [16]. Similarly, CEUS and other US technology like elastography plays an important role as an additional imaging vascular malformations treatments [17, 18]. In this case, CEUS was applied to confirm the diagnosis of OEC and rule out the possibility of ovarian malignancy, which was of particular importance since the OEC showed homogeneous hypoechoic at grayscale US and previous interventional procedure was failed in another hospital. Besides, features and quantitative parameters for the ovarian endometrial cysts differed before and after US-guided interventional treatment can be evaluated by CEUS which indirectly reflected sclerosis of capillaries in the endometrial cyst wall [19]. Therefore, CEUS is used as a routine for the OEC patients subjected to sclerotherapy in our hospital and becomes an indispensable component during the whole procedure.
Interventional treatment of OEC and related literatures
US-guided aspiration and sclerotherapy is a minimally invasive treatment for OEC, with less adverse effect than other approaches. In 1997, Chang et al. [20] performed transvaginal US-guided aspiration of the cyst and tetracycline installation on 32 patients with an encouraging clinical pregnancy rate of 34%. Similar efficacy was reported using ethanol sclerotherapy [21]. Up to date, the most common applied sclerosant is ethanol while we used lauromacrogol in this case. The scientific name of lauromacrogol (also called polidocanol) is polyoxyethylene 10 lauryl ether which is a new type of detergent blood vessel hardener and is commonly applied in sclerotherapy of varicose vein [6]. Compared to ethanol, lauromacrogol achieves the same curative effect with fewer adverse events [10]. Pathologically, lauromacrogol functions by damaging the endothelial cells of target vessels to expose the underlying collagen with the ultimate aim of inducing endovascular fibrosis and aseptic inflammation [22]. The cyst wall consists of glandular epithelium, stroma, and the fibrotic layer, scattering by ectopic endometrial lesion [23]. Lauromacrogol induces a similar chemical effect on the ectopic endometrial lesion and causes fibrosis of the cyst wall ultimately.
From our clinical experience, cyst contents are multitudinous including rheumy blood, viscous chocolate fluid, or clay-like substance. Chang et al. [24] used saline with heparin to dissolve the hemosiderin-rich fluid during flush of the cyst. In this case, the patient underwent an unsuccessful interventional procedure without any special medicine used previously. Small bulks in the cyst blocked the puncture needle probably were the reason for the failure. In this case, we provided a novel solution for patients with sticky fluid in the cyst by urokinase flushing. Urokinase is an enzyme protein isolated from the urine of healthy people or obtained from human kidney tissue culture. It acts directly on the endogenous fibrinolytic system and is widely used for treating thrombolysis [25]. Though complications of urokinase include bleeding and gastrointestinal reaction, intracystic rinse is relatively safe and risks of bleeding are also reduced by subsequent use of lauromacrogol.
Previous literatures related to ultrasound-guided sclerotherapy
TV: transvaginal; TA:transabdominal; NM: no mention.
US-guided aspiration and sclerotherapy is not a conventional therapy for OEC now but a widely accepted intervention before in vitro fertilization (IVF) [26]. Koike et al. [27] demonstrated that US-guided transvaginal ethanol sclerotherapy appeared no adverse effect on reproductive performance in subfertile women with ovarian endometriotic cysts through a retrospective research. Zhu et al revealed that there was a linear regression relationship between the change of times of aspirations and the chance of recurrence of cysts [28]. A multicenter trial in Spain showed that ethanol sclerotherapy for endometrioma treatment seems to reduce healthcare costs and could reduce complications as well versus laparoscopic surgery [29]. A higher detectable rate of OEC makes it a dilemma for young patients to choose the treatment modality, which might lead to long-term anxiety [30]. While the transvaginal and transabdominal intervention approach is both feasible for aspiration [31, 32], US-guided aspiration and sclerotherapy have similar clinical efficacy with surgery and are more acceptable for young women without sexual life.
In conclusion, CEUS is useful for confirming the diagnosis of OEC and ruling out the possibility of ovarian malignancy for those refractory long-term OEC patients, particularly when the lesion looks solid and shows hypoechoic on the conventional US. The application of urokinase is useful in the aspiration of OEC for those patients with a long course and those who had an unsucessful treatment before. Lauromacrogol sclerotherapy is an effective, minimally invasive method for the ovarian endometrial cyst.
Footnotes
Acknowledgments
This work was supported in part by the National Natural Science Foundation of China (Grants 81671695, 81725008 and 81927801), Fundamental Research Funds for the Central Universities (Grants 22120190213), Shanghai Municipal Health Commission (Grants 2019LJ21 and SHSLCZDZK03502), and the Science and Technology Commission of Shanghai Municipality (Grant 19DZ2251100).
Conflict of interest
The authors declare that there are no conflicts of interest regarding the publication of this article.