
Abstract
BACKGROUND:
Recent studies have demonstrated that local application of corticosteroids reduces wound exudation following abdominoplasty and other reconstructive surgical procedures. On the other hand, corticosteroids might provoke wound healing disturbances due to their immunosuppressive effects.
OBJECTIVE:
The main objective of this study was to gain further information about the impact of the corticosteroid triamcinolone on cell migration in abdominoplasty patients.
METHODS:
An in-vitro scratch assay wound healing model was applied to observe cell migration of fibroblasts cultured with nutrient medium containing human seroma aspirate±triamcinolone.
RESULTS:
There were no significant differences regarding cell migration when fibroblasts were incubated with triamcinolone + seroma containing culture medium compared to seroma containing culture medium without triamcinolone.
CONCLUSIONS:
The performed in-vitro study suggests that triamcinolone does not decelerate fibroblast cell migration which is considered as a surrogate of wound healing.
Introduction
Abdominoplasty is one of the most commonly performed aesthetic procedures in the field of plastic surgery [1]. With an incidence ranging from 5 to 43%, seroma formation is the most prevalent complication of abdominoplasty [2, 3]. Seroma is hypothesized to accumulate due to an excessive local inflammatory response reactive to the applied surgical soft tissue trauma [4]. Interestingly, recent studies have demonstrated that local application of corticosteroids prevents seroma following abdominoplasty and other reconstructive procedures [4–6]. Besides their beneficial anti-inflammatory action, however, corticosteroids might impede the physiological wound healing cascade. Corticosteroids are believed to inhibit keratinocyte migration [5, 7]. In fact, there is particular evidence that cortisone affects collagen synthesis by reducing IGF-1 (insulin like growth factor-1), TGF-β (transforming growth factor-β) and procollagen I production [8]. Furthermore, corticosteroids act as immunosuppressants by the interference with cytokine signalling during the inflammatory phase of wound healing and hence might provoke wound healing disturbances and wound infection [5, 7–9].
This trial was designed to elucidate the impact of corticosteroids on wound healing in a cohort of abdominoplasty patients in greater detail. An in-vitro scratch assay wound healing model was applied to observe cell migration of fibroblasts cultured with human seroma aspirate.
Methods
Scratch assay wound healing model
In this experiment the effect of the corticosteroid triamcinolone on cell migration was investigated using an in-vitro scratch assay model. Primary human dermal fibroblasts were isolated from skin of the resected pannus following abdominoplasty. Briefly, the skin layers were separated from the subcutaneous fat tissue with a scalpel. Subsequently, the skin was incubated in 25 UI/mL Dispase II solution (Sigma-Aldrich, St. Louis, MO, USA) in Hank’s Balanced Salt Solution (HBSS, Sigma-Aldrich) at 4° Celsius overnight. Afterwards, the dermis could be separated from the epidermis and was digested enzymatically with 0.1% collagenase at 37°C for 60 minutes. The fibroblasts were cultured under standardized conditions according to the established laboratory protocol. Cells in passage 4 were seeded into 24-well plates with nutrient medium (α-MEM, PAN Biotech, Aidenbach, Germany) and incubated at a temperature of 37° Celsius and an atmosphere of 5% CO2 until confluency was reached. The confluent cell monolayer was scratched with a 100μl disposable pipette tip. Cultures were washed to remove any detached cells. Immediately after scratching the cell monolayer a micrograph photo of each well was taken (t0). Afterwards, cells were cultured with nutrient medium containing 5% seroma samples aspirated from patients who were intraoperatively treated with a single 80 mg dose of topical triamcinolone (A) or who were not treated with any triamcinolone (B). Regular culture medium served as a control (C). After 6–8 hours the cells were examined under the microscope and a second picture of each chamber was taken (t1). By measuring the cell-free scratch area at t0 and t1 fibroblast migration speed was calculated.
For each seroma sample three scratch assays were performed.
Digitization and image processing
The plates were digitized using a calibrated microscope (Wilovert S microscope, Helmut Hund GmbH, Wetzlar, Germany) and the ScopeTec DCM 800 camera (using the Scope Photo 3.0 software) at a format of 3264×2448 pixels, with each chamber being imaged individually. To display the same image section after the incubation period, a part of the chamber wall was also captured at the left edge of the image to allow proper realignment.
Digital image analysis was performed using a self-developed macro for ImageJ freeware (Supplemental Material) [10]. To optimize the quality of the results, user-interactions were integrated to remove possible artifacts and to verify that the area was correctly recognized. The code has been implemented as batch processing (Supplemental Material, Automated Scratch Processing Code). First, the margins were removed, and the image was cropped to 1500×2448 pixels. Subsequently, the images were scaled and adjusted in terms of contrast and sharpness. Then a black and white image was created to select the cells. Now in several steps the cell area was homogenized to a surface. The user had the chance to correct artifacts or faulty connections and to select the cell-free area. The cell-free area was then calculated and an overlay image was created for proof. The relevant steps of the semi-automated image processing are shown in Fig. 1. The data was automatically saved.
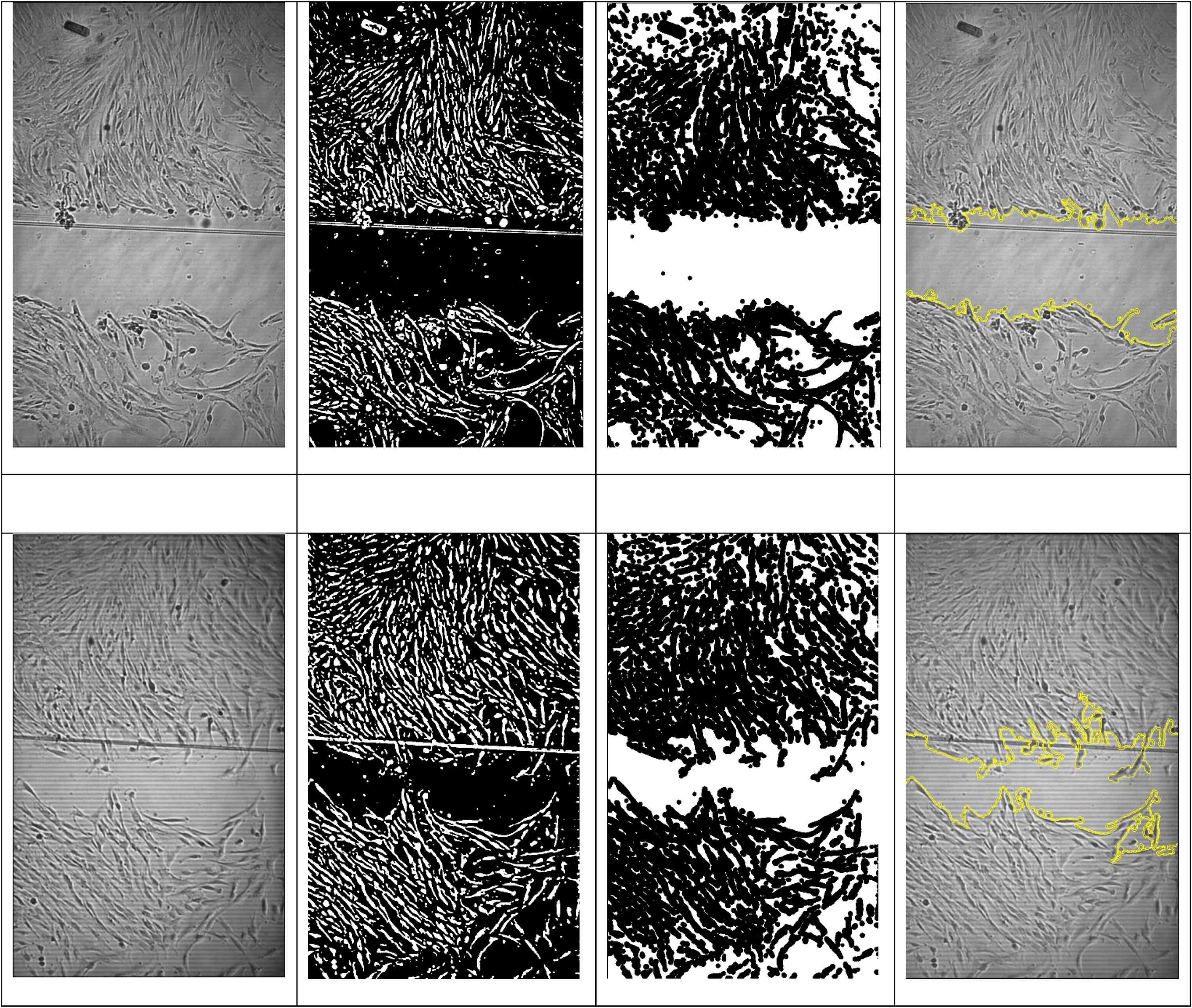
The four images at the top show a scratch-measurement by semi-automated image processing at t0, while the four images below show a measurement of the cell-free area at t1. First artifacts were removed, then cells were homogenized to a surface and finally the cell-free area was measured. It can be seen that the method worked well even with a diagonally running artifact (thin line in the area of the scratch).
In case a semi-automatic analysis was not feasible, e.g. when cell-cell distances were extensive or when there was too little contrast to recognize all cells automatically, a manual analysis with the ImageJ freeware was performed. According to the self-developed macro the margins were removed, and the image was cropped to 1500×2448 pixels. Then, images were adjusted in terms of contrast and sharpness and the cell-free area was selected manually (Fig. 2).

The two images at the top show a scratch measurement by manual image processing at t0, while the two images below show the measurement of the cell-free area at t1. Due to the low cell density, the measurement had to be done manually.
Statistical analysis was performed with SPSS (IBM SPSS Statistics 26.0., Armonk, NY: IBM Corp.). For each sample (A) or (B), the relative reduction of the cell-free scratch area from t0 to t1 was normalized to the control sample (C) to obtain the mean relative scratch shrinkage ratio. A value greater than one indicated faster migration in the sample (A) or (B) compared to the control sample (C) and vice versa. For each case, the three performed assays were averaged. A subanalysis was performed to take into consideration when the seroma fluid used to cultivate the fibroblasts was aspirated (<10 d postoperatively, ≥10 d postoperatively). Continuous variables were summarized by mean and standard deviation, not normally distributed variables were expressed by median and range. Group comparisons were conducted by unpaired Student’s t-test and Mann-Whitney U test. Level of significance was p < 0.05.
Results
In total 15 seroma samples were analyzed. One seroma sample was from a male patient, the others were from female patients. Further patient characteristics are presented in Table 1.
Patient characteristics
Patient characteristics
*Median (Range) **Mean±SD.
Overall, there was no significant difference in fibroblast migration speed between group (A, triamcinolone) and group (B, no triamcinolone) samples (p = 0.364) (Table 2).
Mean relative scratch shrinkage of the analyzed seroma samples
**Mean±SD.
Further analysis showed that there was a tendency for the cells cultured with triamcinolone (group A), however, to migrate more slowly when seroma samples used to cultivate the fibroblasts were taken early (<10 d postoperatively) and vice versa more rapidly in the late aspirated samples (≥10 d postoperatively) (p = 0.014) (Fig. 3). The time of seroma aspiration did not affect cell migration velocity in group B (Fig. 3) (p = 0.697).

The two graphs (blue = group A, red = group B) show the mean relative scratch shrinkage in relation to the postoperative day of seroma sample aspiration. The cells cultured with triamcinolone (Group A) showed a positive linear correlation (R = 0.95, p = 0.014, n = 5). Group B demonstrated a negative correlation (R = –0.141, p = 0.697, n = 10).
Wound irrigation of the abdominal cavity with triamcinolone has been shown to have a reductive effect on the formation of postoperative seroma in abdominoplasty patients [4]. Seroma is presumed as an inflammatory secretion which accumulates due to the applied surgical soft tissue trauma [4]. With regard to their mechanism of action, it is hypothesized that corticosteroids lead to seroma reduction as a consequence of their immunosuppressive effect [4, 11]. On the other hand, corticosteroids are discussed to increase the risk of wound infections and to provoke wound healing disturbances [8, 9]. Due to this contrast, the main objective of this trial was to gain further information about the impact of cortisone on cell migration in seroma patients. Seroma samples of 15 patients were analysed in a scratch assay wound healing model and compared to regular culture medium. Scratch assays are a well-established standard in-vitro technique to study the migration of divergent cell populations [12–14]. In this trial, there was no significant difference in the cell migration speed between the triamcinolone group A and the non-triamcinolone group B. Accordingly, this in-vitro study suggests that steroids do not have any negative consequences on cell migration which is considered as a surrogate of wound healing. This supports the findings of a recent randomised controlled clinical trial showing no significant increase in wound healing disorder and wound infection rates after irrigating the abdominoplasty wound cavity with triamcinolone in a cohort of 60 patients [4].
However, the wound healing cascade is complex, and it is affected by various biochemical pathways [15]. Lee et al. found that steroids can interfere with skin healing by decelerating keratinocyte migration mediated by EGF [7]. EGF, IL-1 and TNFα are the main signalling molecules for cell-mobility that activate keratinocytes to migrate and proliferate by targeting the cytoskeletal components K6 and K16 [16–18]. The authors discovered that glucocorticoid application prevents the expression of K6 and K16 mediated by a repressosome complex [7]. This might be reflected by our data showing a tendency for delayed fibroblast migration when the cells where incubated with early aspirated (<10 d postoperatively) group A samples still containing higher concentrations of triamcinolone.
Correspondingly, we detected an increased migration rate of cells incubated with late triamcinolone seroma samples (aspirated ≥10 d postoperatively) containing corticosteroid residuals only (Fig. 3).
The process of cutaneous wound repair includes different overlapping stages. First, a blood clot forms, followed by angiogenesis and the phases of inflammation. Finally, formation of granulation tissue and reepithelialization takes place. Importantly, the stage of inflammation is transient in the physiologic wound healing cascade and resolves as the healing process moves on. A disturbance of this cascade may cause chronic inflammation and impaired wound healing [8, 19].
Hofman et al. have noticed a remarkably positive effect of cortisone on chronic wounds resulting in accelerated healing and significant pain relief. They postulated that chronic skin-lesions and delayed wound healing are characterised by chronic inflammation and persistent elevation of cytokine levels, e. g. tumor necrosis factor alpha and interleukin-1 [8]. Corticosteroids work as antagonists for these molecules and decrease the amount of inflammatory mediators by formation of the phospholipase inhibitor lipocortin [6, 20]. This might be one explanation why steroids have beneficial effects on chronic wounds.
The performed study is not without caveats. Even if scratch assays represent established wound healing models, their in-vitro design obviously does not allow a direct transmission of findings into clinical medicine. However, the presented experimental results mirror recently published clinical data that showed no relevant increase of wound complications when triamcinolone is used to treat abdominoplasty patients for reasons of seroma reduction [4].
Conclusion
In summary, the performed scratch assay wound healing models did not show statistically significant differences regarding cell migration / mean scratch shrinkage speed when fibroblasts were incubated with triamcinolone containing seroma sample culture medium compared to triamcinolone-free seroma medium. These in vitro results suggest that corticosteroids might not have a relevant impact on wound healing when used for wound irrigation in abdominoplasty patients. While the presented data allows speculations only, it reflects the results of recent clinical trials showing that the fear of corticosteroid associated wound healing disturbances is unreasonable at least in the context of topical application of standard doses in abdominoplasty wound cavities. In conclusion, wound healing and its modulators depict a complex framework that so far has not been fully understood.