
Abstract
BACKGROUND:
Pancreatic ductal adenocarcinoma (PDAC) is highly malignant with a low 5-year survival rate. Blood biomarkers may be of value for the noninvasive diagnosis of pancreatic cancer.
OBJECTIVE:
This study assessed blood-based biomarkers and disturbances in red blood cell aggregation associated with pancreatic cancer.
METHODS:
We studied 61 patients who underwent pancreatic resection. Of these 61 patients, 46 patients had PDAC, and 15 patients had inflammatory tumours. Serum VEGF, hypoxia-inducible factor (HIF-1α), elastin-derived peptides (EDPs), total sialic acid (TSA) and resistin levels were measured. Red blood cell aggregation was assessed by a laser-assisted optical rotational cell analyser.
RESULTS:
VEGF (p < 0.000001), HIF-1α (p = 0.000002), resistin (p = 0.000349), EDP (p = 0.000089) and TSA (p = 0.000013) levels were significantly higher in the PDAC group than in the inflammatory tumour group. The aggregation index (AI), syllectogram amplitude (AMP) and threshold shear rate (γthr) were significantly higher in the PDAC group, whereas the aggregation half-time (t1/2) was lower than in the inflammatory tumour group. Multivariate analyses revealed that VEGF, TSA and EDP levels were variables that predicted PDAC. VEGF levels were the most powerful predictor of PDAC independent of CA 19-9 levels. The cut-off points for VEGF, TSA and EDP levels were 134.56 pg/ml, 109.11 mg/dl and 36.4 ng/ml, respectively, with sensitivities of 97.8%, 87% and 69.6%, respectively, and specificities of 86.7%, 86.7% and 93.3%, respectively.
CONCLUSION:
This study indicated that there are significant differences in blood-based biomarkers for differentiating between PDAC and inflammatory tumours of the pancreas. We also confirmed that PDAC is associated with the excessive aggregation of RBCs.
Introduction
Pancreatic carcinoma is highly malignant with a low 5-year survival rate because of high recurrence rates and low resection rates [1].
Pancreatic ductal adenocarcinoma (PDAC) is the most common pancreatic cancer, accounting for more than 85% of all malignancies of the exocrine pancreas [2]. Early-stage pancreatic cancer may be cured through surgical resection combined with chemoradiotherapy; however, there are no obvious symptoms when the cancer is still localized [3]. New strategies for screening high-risk patients to detect pancreatic carcinoma at earlier stages are desperately needed.
The diagnosis of pancreatic carcinoma at earlier stages is needed to improve its prognosis. There are currently no effective serum tumour markers for the early diagnosis of pancreatic cancer. Carbohydrate antigen 19-9 (CA19-9) is the only serum biomarker routinely used in clinical practice, but the sensitivity (80%, 95% CI: 72% –86%) and specificity (75%, 95% CI: 68% –80%) of this analysis are low [4]. Other tumour markers, such as CEA, CA125, and CA242, are also analysed together with CA 19-9, which leads to better sensitivity and specificity than the analysis of any single marker to diagnose pancreatic cancer [5]. Another important clinical problem is the differentiation between an inflammatory tumour and PDAC before surgery because pathological examination is not sufficient [6].
In healthy humans, vascular endothelial growth factor (VEGF) promotes endothelial cell proliferation and migration and angiogenesis. VEGF is the key mediator of angiogenesis in cancer, in which it is upregulated by oncogene expression, a variety of growth factors and hypoxia [7]. Hypoxia-inducible factor (HIF)-1 is a protein complex that plays an integral role in the body’s response to low oxygen concentrations or hypoxia. HIF-1 is involved in tumour immune escape under hypoxic conditions and during cancer invasion and metastasis [8]. Elastin is an important component of the extracellular matrix. Elastin-derived peptide (EDP) is a product of elastin degradation that has been shown to be biologically active in both physiological and pathological processes. EDPs have been shown to have various biological effects mediated through their interaction with their cognate receptor called the elastin receptor complex, eliciting the activation of several signal transduction pathways [9]. Sialic acid (TSA) is one of the main elements of the glycocalyx [10]. TSA is involved in a multitude of biological processes, and aberrant sialic acid levels are associated with several pathologies, such as cancer [11]. The differentiation between pancreatic cancer and an inflammatory tumour often causes substantial problems related to making decisions regarding surgical treatment and the scope of resection. Identifying and understanding the relationships between new predictive factors that differentiate pancreatic tumours would considerably improve preoperativediagnostics.
A previous study detected the expression of VEGF, HIF-1, EDP and TSA in pancreatic tumour tissue. The results of these studies indicated that pancreatic tumour tissue in patients with PDAC exhibited overexpression of VEGF and HIF-1 [12, 13]. The authors also concluded that HIF-1 is the regulatory link between tumour hypoxia and VEGF production in pancreatic cancer, which contributes to angiogenesis and progression. Similar results were shown by Liang et al., who indicated a correlation between VEGF and TNM stage and metastasis of pancreatic cancer [14]. In contrast, Lim et al. suggested that VEGF is not associated with patient survival in PDAC but is potentially associated with p53 expression [15].
A recent study found overexpression of sialic acids in PDAC cells and highlighted their important role in controlling immune suppression [16]. In an animal model, some elastin degradation products increased PDAC progression through an increase in tumour vascularisation [17].
Studies have shown that disturbances of RBC aggregation are associated with medical conditions such as cardiovascular disease, metabolic disease, haematological disease or infection [18]. Studies have indicated disturbances in the blood’s rheological behaviour, such as blood hyperviscosity, enhanced RBC aggregation and evidence of a lower ability to disaggregate, in some cancers. To date, limited information is available on the interactions between pancreatic cancer and RBC rheological behaviour. Here, we address the hypothesis that PDAC may be associated with RBC rheological disturbances.
This study assessed the ability of blood-based protein biomarkers and the rheological behaviour of RBCs in blood to detect pancreatic cancer and investigated the added value of these analyses to the analysis of CA19-9, the common blood-based biomarker used clinically for pancreatic cancer. We hypothesize that some tissue markers are also overexpressed in blood and might be useful in the diagnosis of PDAC.
Material and methods
Patient characteristics
We studied 69 patients who underwent pancreatic resection for tumours. Of the 69 patients who were included in the study, 61 patients with confirmed PDAC or pancreatic inflammatory tumours were finally analysed. Patients with other postoperative histological diagnoses were excluded. Of the 61 patients, 46 patients (75.4%) had PDAC (Group I), and 15 patients (24.6%) had inflammatory tumours (Group II). There were 24 (52.2%) men and 22 (47.8%) women in Group I. Their mean age was 63.09±9.51 years, their mean weight was 73 (61–85) and their mean body mass index (BMI) was 25.89±4.84. There were 13 (86.7%) men and 2 (13.3%) women in group II. Their mean age, weight and BMI were 56.33±13.68, 65 (61–75) and 22.09±4.22, respectively. In the PDAC group, 16 patients also exhibited aggregation and kinetics of red blood cell aggregation.
This group included patients who did not exhibit factors that could potentially influence the observed rheological blood parameters, such as smoking, diabetes mellitus, chronic kidney disease, uncontrolled hypertension, history of leg vein thrombosis, and antithrombotic therapy. The control group for rheological measurements consisted of 16 healthy individuals with similar ages and weights without any of the above-listed features. There were no differences in age or weight between the groups. The study protocol was approved by the ethical committee of the Medical University of Silesia, and all participants provided written consent (KNW/0022/KB1/38/III/14/16/17).
Biomarker measurements
Blood from the basilic vein was collected on an empty stomach in the morning between 7.30 and 8.00 for biochemical tests. Blood samples were collected into Vacutainer tubes. Blood was collected on the clot (dry tube) in a volume of 10 ml of whole blood. Each sample was immediately centrifuged at 3000×g for 30 min at 4 °C. After separation of the morphotic elements, the obtained sera were frozen at –85 °C until use. Test samples and control samples were simultaneously processed. Serum VEGF-A and HIF-1α levels were measured by an enzyme-linked immunosorbent assay (ELISA) method using commercial kits (VEGF-A R&D System ELISA Minneapolis USA; HIF-1α ELISA Kit, Mybiosource San Diego USA). Serum total sialic acid (TSA) levels were measured using an enzymatic method purchased from Boehringer Mannheim (Mannheim Germany). This method uses a coupled enzyme assay reaction incorporating neuraminidase, N-acetylneuraminic acid aldolase and pyruvate oxidase linked to a peroxidase dye system. EDP (elastin-derived peptide) concentrations in the serum were measured using an immunoenzymatic method with a kit (Cloud-Clone Corp., Houston, USA) according to the manufacturer’s instructions. To measure the concentrations of the tested markers, calibration curves were prepared using the standards included in the kits. Absorbance readings were obtained using the Universal Microplate Spectrophotometer-μQUANT apparatus by BIO-TEK INC (Bio-Tek World Headquarters, California, USA) at a wavelength of 450 nm, and the results were processed using the computer program KCJunior (Bio-Tek, USA). Serum concentrations of resistin were measured using a commercially available enzyme-linked immunosorbent assay kit (DRG International, Inc., Marburg, Germany) according to the manufacturer’sinstructions.
Biochemical measurements
Serum basic preoperative biochemical parameters and CRP levels were measured using an automatic analyser COBAS INTEGRA 400 PLUS (Roche Diagnostic, USA). The levels of neoplasm markers such as α-fetoprotein (AFP), carcinoembryonic antigen (CEA) and carbohydrate antigen (CA 19-9) were measured using the automatic analyser COBAS e411 (Roche Diagnostic, USA).
Haemorheological measurements
Blood samples were collected for rheological measurements from the cubital vein and then anticoagulated with K3EDTA (1.5 mg/ml). Blood withdrawal was performed after a 10-minute resting period after a 12-hour overnight fast between 8 and 9 a.m. The rheological tests were performed at a stable temperature of 37 °C within two hours after the blood was collected. In patients with RBC aggregation measurements, Ht was measured with a microhaematometer, and we did not use an automatic analyser. Haematocrit was adjusted to a standard Htc of 45% before determining EA.
RBC aggregation and kinetics of the red blood cell aggregation were determined by the Laser-assisted Optical Rotational Cell Analyser (LORCA; Mechatronics, Zwaag, the Netherlands). In erythrocyte aggregation measurements, laser backscatter light was used, where the intensity of reflection depended on whether erythrocytes formed rouleaux at rest or if they were disaggregated and deformed with high shear rates. The computer program analysed the aggregation parameters of RBCs according to the syllectogram, the curve of the relationship between laser backscatter intensity and time. The following parameters specific to the aggregation process were estimated: aggregation index (AI), syllectogram amplitude (AMP), aggregation half-time (t1/2) and threshold shear rate (γthr).
Statistical analysis
Continuous variables are presented as the mean±SD or the median with the interquartile range if the data were not normally distributed. Categorical variables are presented as absolute numbers and percentages. The Shapiro-Wilk test was used for all continuous variables to test for a normal distribution. Statistical comparisons were achieved using the unpaired Student’s t test and the Mann-Whitney U test for nonnormally distributed data. Chi2 or Fisher’s exact test (in the case of expected numbers smaller than 5) was performed to compare the differences in the categorical data. Independent blood-based protein biomarker predictors of PDAC were determined with a multivariate regression model using the stepwise selection of biochemical parameters, with an entry criterion of P < 0.2. Variables considered to be potential predictors for multivariate modelling were identified with univariate analyses and subsequently selected with stepwise backwards selection. A regression analysis was performed for the following covariates: age, CA19-9, CEA, AFP, VEGF, HIF-1α, resistin, EDP and TSA levels. Three multivariate models were used for the following covariates: VEGF, HIF-1α, resistin, EDP and TSA levels (Model I), CA 19-9 levels (Model II) and age (Model III). Receiver operating characteristic (ROC) curves were generated for the estimated models. To assess the accuracy of the model, the area under the receiver operating characteristic (ROC) curve (AUC - area under the ROC curve) was used. After determining the optimal cut-off point, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated. Results with a P value < 0.05 were considered to be significant. The statistical analysis was performed using Statistica 12 (StatSoft, Inc., Tulsa, OK, USA).
Results
Patient characteristics
The baseline characteristics of the study population are presented in Table 1. There were no significant differences between the groups in the sex distribution (P = 0.374), mean body mass (p = 0.194) or BMI (p = 0.08). Patents with PDAC were older than those with inflammatory tumours (p = 0.037). Significant differences were observed for some biochemical parameters between both groups. Glucose levels, MPV levels and the levels of hepatic parameters were significantly higher in the PDAC group, whereas amylase, creatinine and white blood cell levels were significantly higher in the inflammatory tumour group (Table 1). Levels of the CA 19-9 antigen were significantly higher in the PDAC group than in the patients with inflammatory tumours. There were no differences in CEA or AFP levels between the groups.
Baseline characteristics of the study group
Baseline characteristics of the study group
RBCs, red blood cells; Hb, haemoglobin; Hct, haematocrit; WBC, white blood cells; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALP, alkaline phosphatase; GGT, gamma-glutamyl transpeptidase.
The levels of all measured blood-based protein biomarkers were significantly different between the two groups of patients (Table 2). VEGF (p < 0.000001), HIF-1α (p = 0.000002), resistin (p = 0.000349), EDP (p = 0.000089) and TSA (p = 0.000013) levels were significantly higher in the PDAC group than in the inflammatory tumour group. The median VEGF level was four times higher in the PDAC group than in the inflammatory tumour group; the HIF-1α level was three and a half times higher; and the levels of resistin, EDP and TSA were each two times higher in the PDAC group than in the inflammatory group.
Statistical analysis of differences in the levels of novel blood biomarkers and CA 19-9 between patients with pancreatic cancer and inflammatory tumours
Statistical analysis of differences in the levels of novel blood biomarkers and CA 19-9 between patients with pancreatic cancer and inflammatory tumours
CEA, carcinoembryonic antigen; CA 19-9 carbohydrate antigen 19-9; AFP, α-fetoprotein, HIF-1α, hypoxia-induced factor 1α; VEGF, vascular endothelial growth factor; EDP, elastin-derived peptide; TSA, total sialic acid.
Univariate analyses revealed potential predictors of PDAC. These predictors included age (OR = 1.058; 95% CI: 1.001–1.118; p = 0.044), BMI (OR = 1.231; 95% CI: 1.042–1.453; p = 0.014), VEGF levels (OR = 1.018; 95% CI: 1.008–1.028; p < 0.001), HIF-1α levels (OR = 1.018; 95% CI: 1.006–1.030; p = 0.002), resistin levels (OR = 2.389; 95% CI: 1.448–3.940; p = 0,001), EDP levels (OR = 1.182; 95% CI: 1.079–1.294; p < 0.001) and TSA levels (OR = 1.098; 95% CI: 1.050–1.149; p < 0.001). Multivariate analyses revealed that VEGF, TSA and EDP levels were variables that predicted PDAC (Table 4). Independent of these models, the VEGF level was the most powerful independent predictor of PDAC. After accounting for CA 19-9 antigen levels (model II) and CA 19-9 antigen levels and the patient’s age (model III), additional independent predictors of PDAC were TSA and EDP levels. Based on the ROC curve, the cut-off point for VEGF levels in serum in PDAC patients was 134.56 pg/m. With this value, the sensitivity of VEGF analysis was 97.8%, the specificity was 86.7%, the positive predictive value (PPV) was 95.7%, and the negative predictive value (NPV) was 92.9% (Fig. 1A). The cut-off point for TSA levels was 109.11 mg/dl, with a sensitivity of 87%, a specificity of 86.7%, a PPV of 95.2%, and an NPV of 68.4% (Fig. 1B). The cut-off point for EDP levels was 36.4 ng/ml, with a sensitivity of 69.6%, a specificity of 93.3%, a PPV of 97%, and an NPV of 50% (Fig. 1 C).
Multivariate regression analysis of serum biomarkers as independent predictors in patients with PDAC
Model I: VEGF, HIF-1α, resistin, EDP and TSA. Model II: VEGF, HIF-1α, resistin, EDP, TSA and CA 19-9. Model III: VEGF, HIF-1α, resistin, EDP, TSA, CA 19-9 and age.
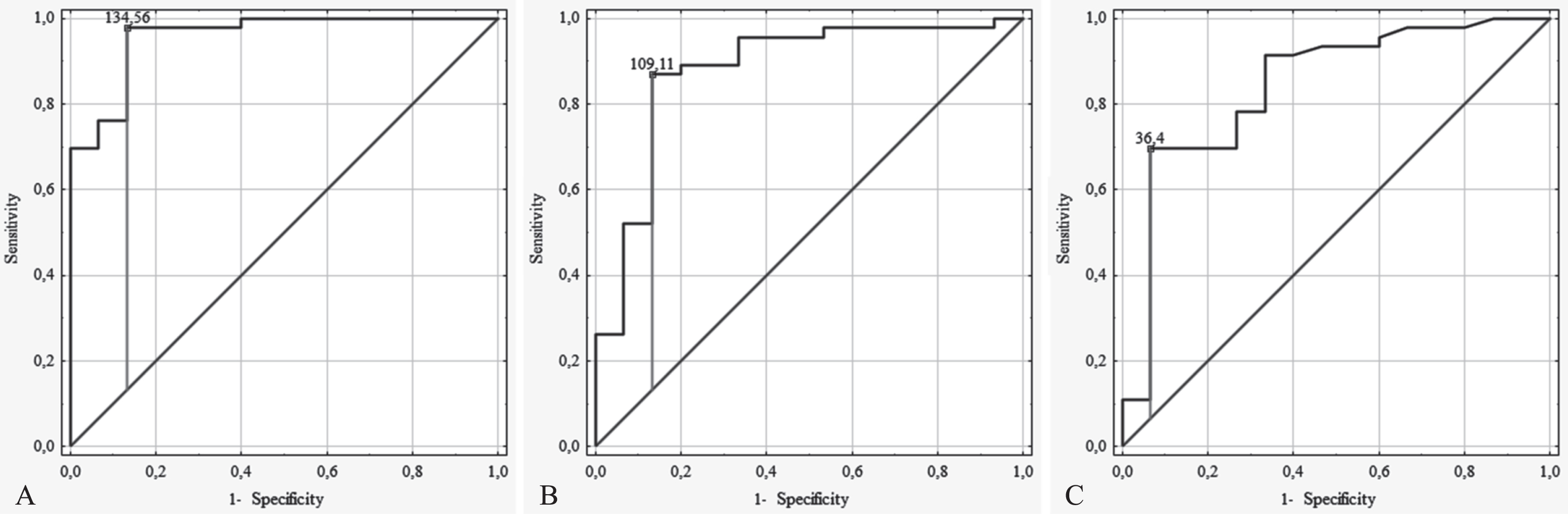
The ROC curve for blood-based biomarkers in PDAC patients. A. VEGF, B. TSA and C. EDP.
The AI, AMP and γthr were significantly higher in the PDAC group, whereas the t1/2 was lower than that in the healthy control group (Table 3).
Changes in RBC properties of blood between the pancreatic cancer and control groups
Changes in RBC properties of blood between the pancreatic cancer and control groups
AI, aggregation index; AMP, amplitude; t1/2, aggregation half-time; γthr, threshold shear rate; au, arbitrary units.
Pancreatic ductal adenocarcinoma (PDAC) is the most common type of pancreatic cancer. It is a relatively uncommon cancer accounting for approximately 3% of all cancers in the US, and approximately 7% of all cancer deaths are slightly more common in men than in women [19]. Early and accurate diagnosis of PDAC can often be challenging and is usually based on a combination of imaging techniques, endoscopic ultrasonography (EUS), tumour marker analyses and clinical presentations. Based on a recent annual report to the nation on the status of cancer, the 5-year survival for adenocarcinoma and neuroendocrine pancreatic cancer improved between 2001 and 2018; however, the overall incidence (2001–2018) and mortality (2001–2019) continued to increase for cancers occurring in this site [20].
The role of most useful and routinely adopted tumour markers, such as CA19-9 and CEA, in PC diagnosis is inconclusive because highly elevated serum levels have been found in patients with other malignant tumours, as well as those with nonmalignant diseases [21]. Recent meta-analyses have shown that the analyses of novel protein biomarkers such as macrophage inhibitory cytokine 1 (MIC-1), thrombospondin-2 (THBS2), tissue inhibitor of metalloproteinase 1 (TIMP-1), osteopontin (OPN), intercellular adhesion molecule 1 (ICAM-1), and insulin-like growth factor-binding protein 2 (IGFBP2) have moderate diagnostic accuracy but do not outperform CA19-9 analysis in differentiating pancreatic cancer from benign disease [22]. The analysis of MIC-1 levels had the best performance in distinguishing PDAC from healthy controls and demonstrated higher accuracy than the analysis of CA19-9 levels. However, the combined analysis of MIC-1 and CA19-9 levels did not significantly improve the diagnostic accuracy for differentiating PDAC from benign disease.
There are a large number of factors involved in regulating carcinogenesis and cancer progression. Independent of cancer aetiology, tumour growth and progression are associated with extensive neovascularization, including microvessel growth and vascular network remodelling, in which angiogenesis and vascular remodelling play an important role. Adequate angiogenesis is necessary for tissue enlargement because this process requires efficient blood perfusion for the supplementation of nutrition and oxygen in newly enlarged areas. However, enlarged tumours develop increasing oxygen consumption caused by tissue hypoxia, mostly occurring in solid tumours. Overexpression of HIF-1α plays a pivotal role in and progression of malignant behaviours, such as proliferation, migration and invasion, promoting tumour progression [23]. HIF-1α-mediated biological effects are beneficial for tumour progression, including glycolysis, inhibition of fatty acid β-oxidation, production of cellular reactive oxygen species and epithelial-mesenchymal transitions beneficial for tumour growth [24]. Accumulating studies have indicated that hypoxia and HIF-1 induce the production of signalling molecules and cytokines and dysregulate certain microRNAs important for cancer progression, altering the expression of tumour suppressor genes, promoting angiogenesis by upregulating VEGF and increasing phagocytosis through the CD47 receptor and regulating tumour immune escape under hypoxic conditions [8]. Thus, the effect of hypoxia on the tumour microenvironment and microcirculatory network is biphasic, and the role of hypoxia in both pro- and antitumorigenic pathways was objectively assessed.
In this study, we focused on potential new blood-based protein biomarkers for detecting pancreatic cancer. Previous studies have reported that PDAC is associated with an increased level of VEGF [25, 26]. In contrast, other authors found no differences in VEGF concentration between patients with PDAC and patients with chronic pancreatitis [27].
Sivaprasad et al. [25] found that VEGF levels were five times higher in the PDAC group than in the control group. Consistent with our results, the median VEGF level was four times higher in the PDAC group than in the inflammatory group. Our results suggest that VEGF might be a differentiated marker between PDAC and pancreatic inflammatory tumours. Another study investigated inflammatory and angiogenic markers for PDAC [26]. They found that PDAC patients also had higher levels of VEGF than control participants due to causes other than pancreatic disease, but in a multivariate logistic regression model, VEGF was not an independent risk factor. Other authors found no differences in preoperative VEGF concentrations between patients with PDAC and patients with chronic pancreatitis, and elevated levels of VEGF correlated with poor cancer-specific survival in the postoperative course [27].
The results draw attention to two important facts that have not yet been investigated. We showed that PDAC is associated with higher levels of VEGF, HIF-1α, resistin, EDP and TSA than inflammatory tumours. The literature indicates that HIF-1α is a principal regulator of tumour hypoxia and plays a critical role in promoting PDAC [28], and it has been considered for prognostic stratification and the assessment of the survival of patients with PDAC [29].
Wang et al. reported higher HIF-1 expression in pancreatic cancer tissue than in normal pancreatic tissue, and high HIF-1 expression levels were significantly correlated with decreased disease-free survival [30].
In the current study, the authors classified patients with PDAC into three clusters based on HIF-1 related genes [31]. They established a specific HIF-1 score system to discriminate pancreatic cancers with various degrees of hypoxia, which provides accurate predictive value for patient prognoses. We observed a significantly higher serum concentration of HIF-1α in the PDAC group than in the inflammatory tumour group.
These findings suggest that PDAC is associated with the overexpression of HIF-1α in the tumour microenvironment, and HIF-1α may be used as a potential biomarker for pancreatic cancer when biopsy is unviable or nondiagnostic to confirm malignancy of the pancreas. Elastin and its degradation peptides are important components of the extracellular matrix. EDP plays an important role in physiologic processes, including those involving elastin, and pathological processes, as structural tissue differs from the most important organs. EDP has been found to be involved in cardiovascular processes, including aneurysm of the aorta, lung diseases, some diabetes complications and cancer [9]. The results of this study indicate that the enzymatic activity of the neuraminidase of the elastin receptor complex is responsible for its signal transduction [32] through sialic acid generation [33].
Rodriguez et al. have shown that pancreatic adenocarcinoma tumour cells exhibited an increased expression of sialic acid detected by the myeloid receptors Siglec-7 and Siglec-9 [16]. The authors show that sialic acids modulate monocytes to produce IL-10 and IL-6 and differentiate monocytes to immune-suppressive macrophages by action of the Siglec-9 receptor. Our results are not opposite to those of Rodriguez et al. but rather expand the knowledge about the role of TSA in PDAC. We show that PDAC is associated with higher blood TSA concentrations than in patients with inflammatory pancreatic tumours.
Recent animal studies have characterized for the first time the effect of two EDPs on PDAC [17]. The results suggest that EDPs, especially AG-9, strongly increase PDAC progression through an increase in tumour vascularisation. This study found that EDP and TSA levels were significantly higher in the PDAC group than in the inflammatory tumour group. The multivariate model indicated that EDP and TSA levels were predictors of pancreatic cancer. These results indicated that PDAC is associated with the overexpression of both biomarkers. These results confirmed the previously described relationship between EDP and TSA in the signal transduction pathways involved in pancreatic cancer.
Resistin was originally described as an adipocyte-specific hormone modulating insulin resistance. Its role is not clear. Circulating resistin levels have been associated with obesity as well as insulin resistance, and resistin may exhibit proliferative, antiapoptotic, proinflammatory, proangiogenic and metastatic properties [34]. There are data supporting that resistin levels increase in PDAC patients and may be a potential diagnostic biomarker associated with pancreatic cancer [35, 36].
The synthesis of VEGF is correlated with intracellular hypoxia and the intracellular signalling mechanisms associated with the NOTCH pathway. In ovarian cancer, there is a correlation between increased expression of NOTCH and production of VEGFR1 and 2 and, therefore, with metastasis [37]. This is a very important pathway in therapy with the antibody bevacizumab, which inhibits angiogenesis. VEGF inhibitors may have a significant effect in the treatment of advanced breast cancer [38] or renal cancer [39].
Disturbances in the blood’s rheological behaviour in malignancies such as breast cancer, melanoma, head/neck cancer, lung cancer and gynaecological cancer were presented [41–43]. This study confirmed haemorheological alterations, such as enhanced RBC aggregation, and evidence of a lower ability to disaggregate in PDAC.
Studies have revealed that the rheological properties of blood disorders are markers of the pathological changes associated with cancer [41, 42], which appear to be related to the evaluation and prognosis of disease, but the exact biochemical mechanism of RBC hyperaggregation is not clear. Our study confirmed that PDAC is associated with complex disturbances in RBC aggregation, and evidence suggests that PDAC is associated with hyperaggregation of RBCs. The aggregation index, syllectogram amplitude and threshold shear rate were significantly higher in the PDAC patients than in the other patients, which indicated an increased extent of total aggregation and the spontaneous ability for aggregation. Alterations in the kinetics of RBC aggregation expressed by shortening the aggregation half-time indicate that RBCs form both aggregates and rouleaux in a shorter time after their disaggregation in PDAC patients than in normal individuals. Similar results were confirmed in patients with other medical conditions associated with hyperaggeration of RBCs, which may be the cause of blood flow condition disorders [44–46].
RBC aggregation is a complex process that forms rouleaux and 3D networks, and it depends on both plasma-dependent RBC aggregation and RBC surface properties. Macromolecules play a dominant role among the plasma factors affecting RBC aggregation because bridges connecting RBC surfaces are created in the presence of plasma proteins. A very interesting problem is the interactions between circulating tumour cells and blood cells. Helwa et al. found that endogenous or exogenous galectin-4-expressing pancreatic tumour cells interact directly with RBCs via galectin-4 [47]. It cannot be ruled out that some measured and unregulated markers, especially sialic acid, one of the main elements of the glycocalyx, may affect RBCs, but further study is needed. The mechanism of disorders accompanying RBC blood rheology, especially in neoplasm patients, is complex and still not fully clarified, and further study is needed.
Red blood cells have the spontaneous ability to form linear and three-dimensional aggregates in resting whole blood. The general phenomenon of increasing blood viscosity with increasing RBC aggregates at low shear rates is known. At low shear rates, the RBC aggregates form rouleaux structures with larger geometries, which cause an increase in blood viscosity, but high shear rates cause disaggregation of the rouleaux and cell deformations, which decrease blood viscosity. Studies have shown that RBC aggregation promotes the axial accumulation of RBCs in ex vivo investigations in tube flow [48] and the microcirculation of animal models [49, 50], resulting in a two-phase flow consisting of a core of aggregates and a cell-free layer and that the magnitude of the effect depends on the intensity of RBC aggregation in the microcirculation network. The ability of RBCs to aggregate and slow-moving plasma layers are the most important factors affecting hydrodynamic resistance at low flow rates in tubes [51] and capillaries [52], and the dimension of the effect increases with red cell hyperaggregation. Other authors indicated that red blood cell aggregation may alter the cell-free layer variability, especially at low shear rates [53, 54]. The effect of RBC aggregation on tissue blood flow is not unidirectional because the haemodynamic consequences of RBC aggregation can affect decreasing or increasing tissue perfusion as a result of interrelated mechanisms. These mechanisms include the axial accumulation of RBCs, viscosity and resistance in the cell-free layer and haematocrit of the microvessels or wall shear stress, which depends on RBC aggregation behaviour. Hyperaggregation of RBCs results in decreased tissue blood perfusion and may also increase thrombosis risk [55]. Hyperaggregation of RBCs results in a decrease in tissue blood perfusion, which leads to tissue hypoxia, mostly occurring in solid tumours. Hypoxia and HIF-1 induce the production of signalling molecules and cytokines that promote angiogenesis by upregulating VEGF. Both parameters were overexpressed in the blood of patients with PDAC in this study. On the other hand, haemorheological alternation was confirmed by enhanced RBC aggregation and evidence of a lower ability to disaggregate in PDAC patients. There are no strong predictors of PDAC. CA19-9 is the only serum biomarker routinely used in clinical practice, but its sensitivity and specificity are relatively low. We studied biomarkers that may have some value in diagnostic accuracy in PDAC patents. Our results suggest that VEGF might be considered a serum pancreatic cancer marker in addition to CA-19-9, but further study isnecessary.
Conclusion
This study indicated that there are significant differences in the investigated blood-based protein biomarkers for differentiating between PDAC and inflammatory tumours of the pancreas. We found a strong association between PDAC and VEGF, TSA and EDP levels. We also confirmed that PDAC is associated with RBC rheological disturbances, which leads to hyperaageration of RBCs. The presented data suggest that blood-based protein biomarkers may be of value for the efficient, accurate, and noninvasive diagnosis of pancreatic cancer.