
Abstract
Ultrasound is the most used interdisciplinary imaging technique in clinical routine for assessment of renal pathologies. This includes the monitoring of cystic renal lesions, which can be classified as non-complicated or complicated and by means of occurrence as solitary or multifocal lesions. The Bosniak-classification (I–IV) classifies renal cysts in 5 different categories and is used for decisions of further clinical treatment. This classification was developed for computed tomography and has been adopted for magnetic resonance imaging as well as contrast-enhanced ultrasound. In the following review article, cystic kidney lesions and their differentiation using contrast-enhanced ultrasound are presented and an overview of the therapy options is given. In interventional procedures, CEUS can make a valuable contribution in histological sampling, reduce radiation exposure and, under certain circumstances, the number of interventions for the patient.
Keywords
Introduction
In recent years, there has been enormous development progress in ultrasound diagnostics of renal lesions, especially the improved access to contrast-enhanced ultrasound (CEUS) brings many advantages for everyday clinical workup and is currently one of the standard diagnostic procedures.
CEUS enables the physician to dynamically assess the vascularization of tissues and vessels in a real-time manner. For this purpose, an ultrasound contrast agent (UCA) is injected intravenously, which allows to examine the precise contrast dynamics of the renal parenchyma as well as solid and cystic lesions.
The recommended volume of UCA for the examination of the kidney varies between 1.0 –1.5 mL depending on the ultrasound system and the ultrasound probe followed by a bolus of up to 10 mL of sterile saline (0.9% NaCl) [1–3].
UCA consist of small microbubbles (e.g. SonoVue®, Bracco, Milan, Italy) generating a nonlinear tissue independent contrast which allows dynamic evaluations at the level of capillary microcirculation with a spatial resolution superior to that of computed tomography (CT) and magnetic resonance tomography (MRI) [4–7]. The higher spatial resolution of ultrasound imaging compared to CT and MRI offers the possibility to characterize kidney lesions and can be used for pre-interventional planning, peri-interventional monitoring and post-interventional success control [8].
The diagnostic challenge for renal masses is in differentiating between benign, malignant and cystic renal lesions, to avoid unnecessary invasive procedures, or missing a renal cell carcinoma (RCC).
UCA have extremely low risk profiles and have no influence on the kidney or thyroid gland function; therefore, they can be administered to a wider range of patients [9, 10]. Safe applications in children and young adults are already widely used in daily routine and first studies have even demonstrated a safe application of CEUS in pregnant women [11–13].
CEUS in the framework of renal lesions
Every examination will start with standard kidney diagnostics of non-enhanced B-mode sonography followed by color or power Doppler examination. Depending on the manufacturer, the frequency range of the multi-frequency transducer used is between 1 and 9 MHz. A linear transducer can also be used to achieve higher spatial resolution. However, these are only suitable for detecting superficial lesions since the higher frequency reduces the penetration depth.
After the B-mode sonography, the UCA is injected. The second-generation contrast medium (SonoVue, Bracco, Milan, Italy) consists of sulfur hexafluoride gas filled microbubbles that are stabilized by a phospholipid shell. This shell represents the interface between the blood and the gas, resulting in many small interfaces with high echogenicity. The microbubbles have a diameter of approx. 2–10μm and correspond to the size of a blood cell, they cannot leave the vascular system and remain in the vascular system. They are exhaled within a few minutes via respiratory system and thus eliminated. The phospholipids of the membrane are degraded via the endogenous metabolism [14, 15]. As already mentioned, UCAs have no effect on kidney or thyroid function and are therefore a suitable alternative for patients with kidney or thyroid diseases. However, as with other contrast media, the anaphylactic reaction must be elucidated [9, 17].
The ultrasonic waves will reflect from the surface of the microbubbles, they have a backscatter behavior called linear behavior. The backscattered sound wave has the same wavelength as the incident sound wave, so they can amplify the signal intensity by more than 30 dB, which is 1000 times the received sound intensity [14, 18]. A good contrast can be ensured with a single contrast medium bolus injection. For this purpose, the use of an 18- gauge needle in an antecubian vein is useful. The injection of 1.0–1.5 mL of UCA is followed by a bolus of 10 mL of 0,9% NaCl saline solution [19, 20].
Renal cysts – Bosniak classification
For everyday clinical practice, it is important to be able to distinguish between benign and malignant cystic renal lesions with a high level of certainty, since 6% of all asymptomatic cysts were found to be renal cell carcinomas [21, 22].Cystic kidney lesions cannot always be reliably characterized in non-enhanced B-mode sonography with the aid of color-coded duplex sonography. Even in CT examination, a clear diagnostic statement is not always possible, especially in the portal venous contrast medium phase. The use of CEUS offers good assistance here, as it can optimally depict the vascularization behavior of the cystic lesion [23, 24].
The prevalence of renal cysts increases with age and is higher in men than in women. From an age of > 70 years, the prevalence increases up to 55% [25].
Distinguishing between uncomplicated and complicated cysts and between cystic and solid renal masses is still challenging today, but this differentiation is essential because up to 10% of RCCs can consitute as cystic lesions [26].
The Bosniak classification for renal cysts, originally developed for CT in 1986, has become established in contrast- enhanced ultrasound and with an update proposed in 2019 for CT and MRI, it is still the standard in everyday clinical practice [27, 28].
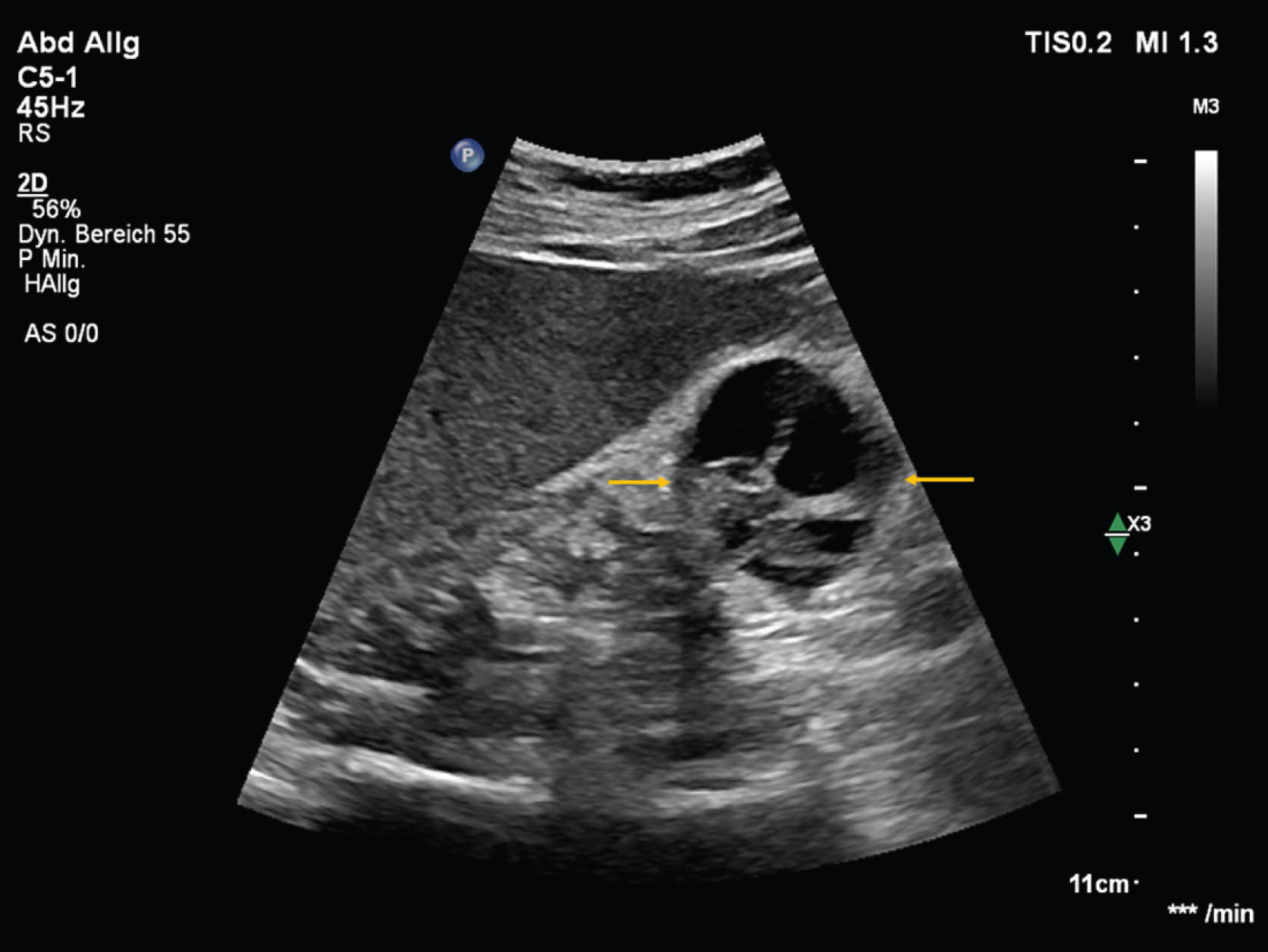
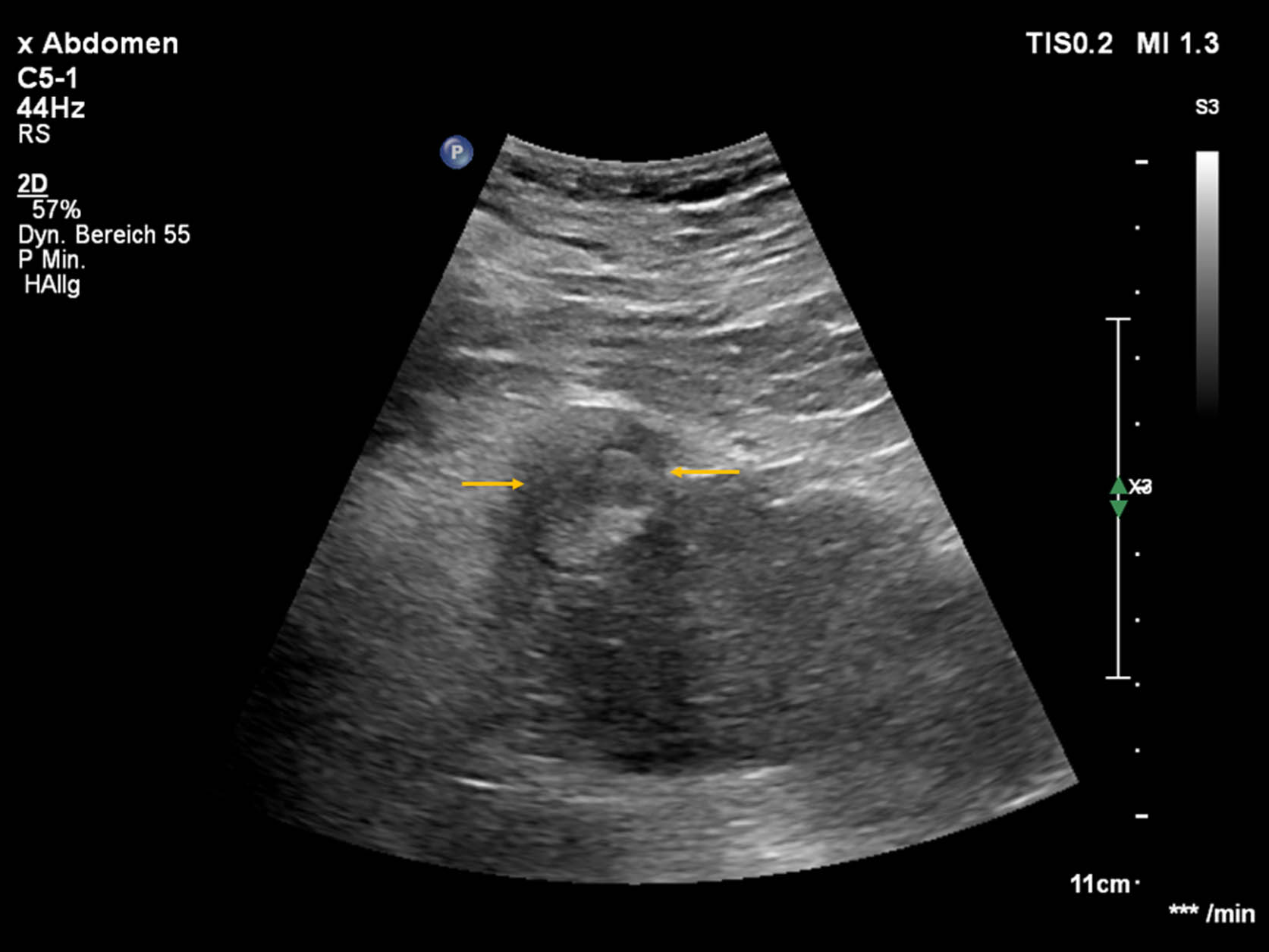
The renal cysts can be divided into 5 different categories according to Bosniak. Simple cysts usually present as a round or oval structure with anechoic contents and a smooth border on native B-mode sonography and no evidence of vascularization on color duplex ultrasound. Sound amplification is evident distal to the renal cyst compared to the surrounding parenchymal tissue. These so called bland or simple cysts are divided into Bosniak classification I. Lesions with 1–3 thin septa less than 2 mm thick are assigned to category II and like category I, do not require any further diagnostic workup [23, 30]. In category IIF of the Bosniak classification, a follow-up is recommended, as there is a 5–10% risk of malignancy. These cysts correspond to the complex cysts and have multiple thin septa [27, 32] (Figs. 1–2).

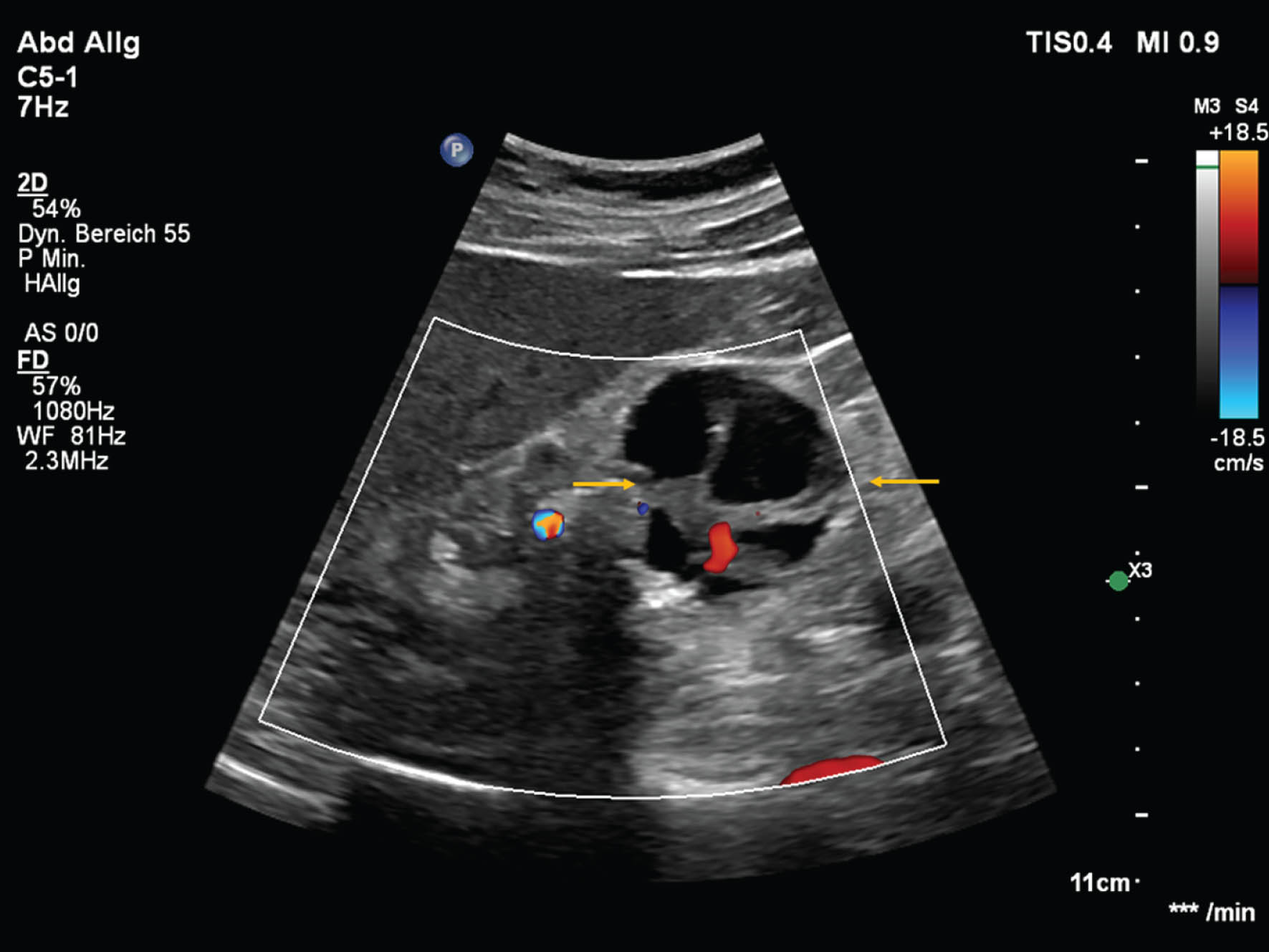
B-mode ultrasound detected a complex cystic lesion (red arrows) with suspicion of an intracystic tumor. In the microflow imaging (yellow arrows) no vascularization is visible.

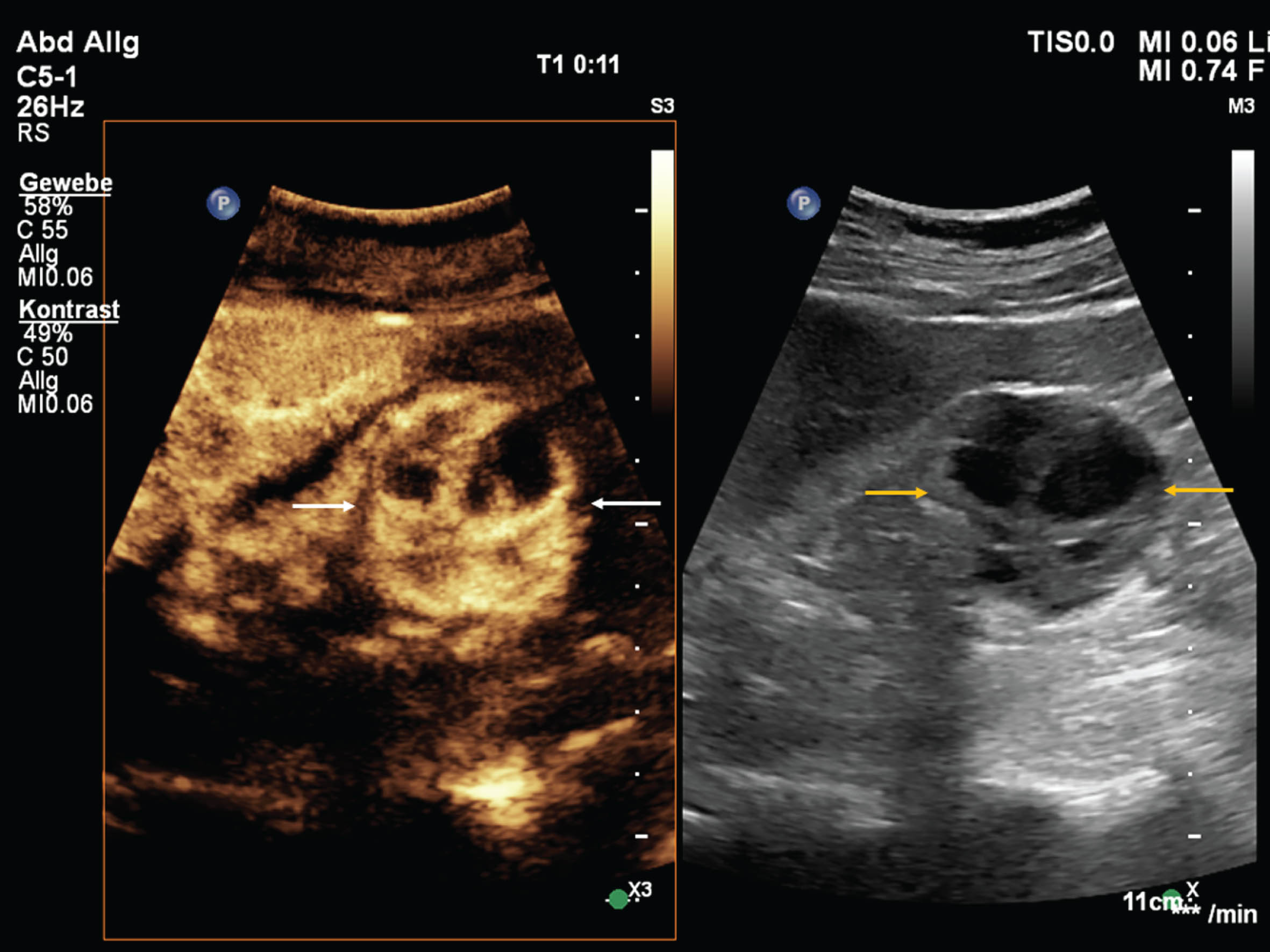
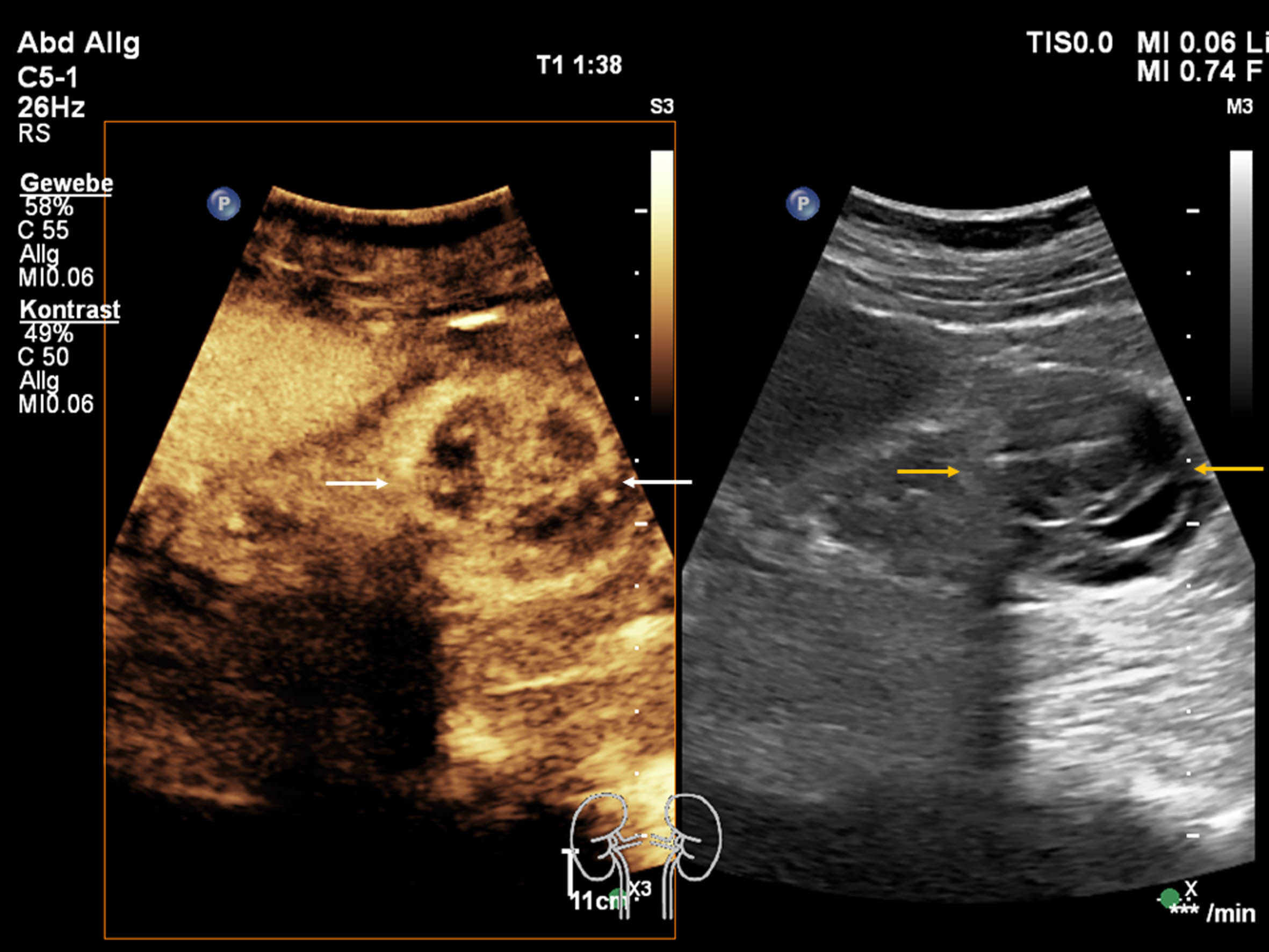
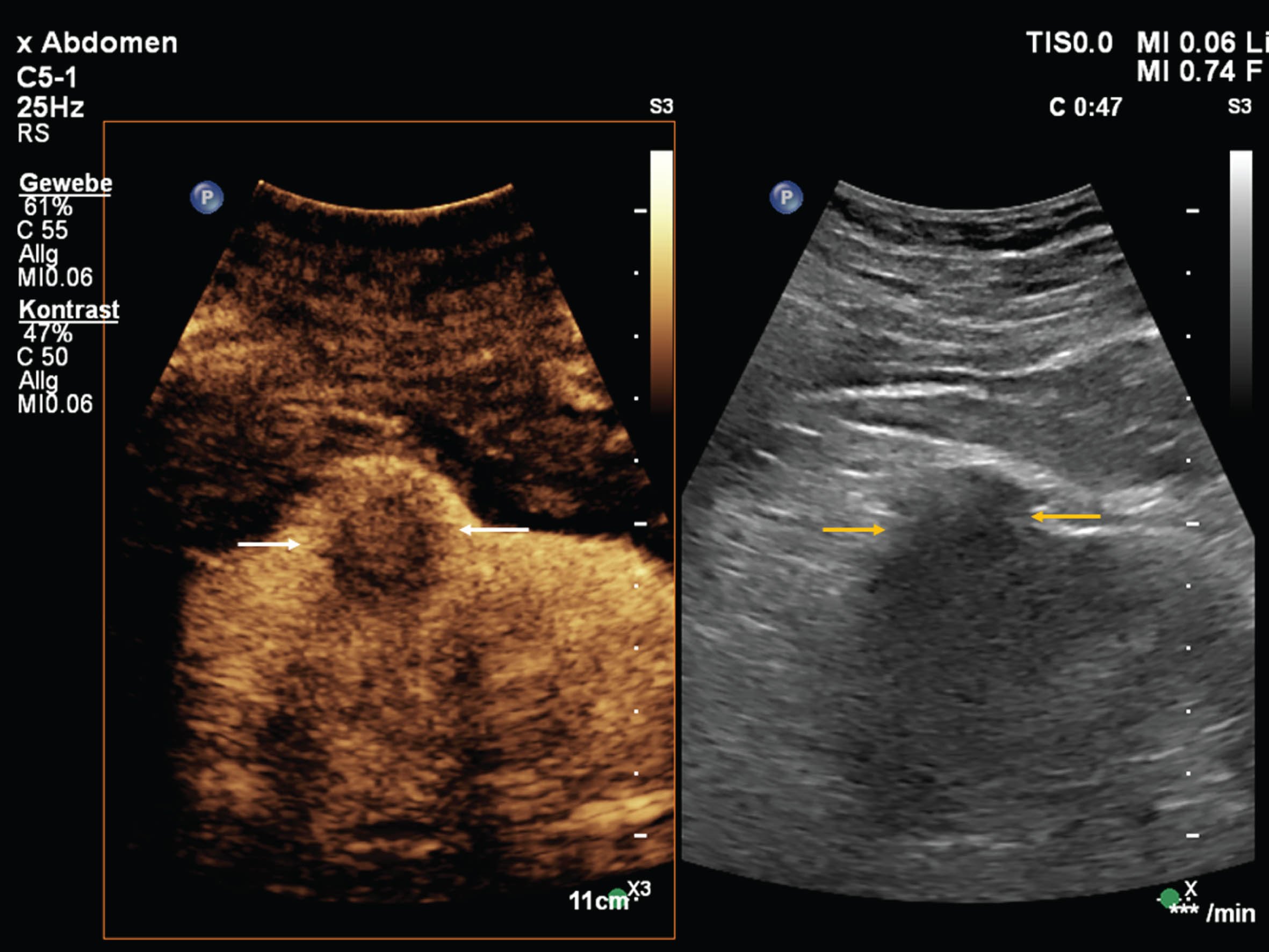
Using the dual imaging CEUS setting, with CEUS image of the cyst (white arrows) on the left side and greyscale image on the right side (yellow arrows) of the image. During the contrast examination the lesion doesn't show any contrast uptake. The final diagnosis will be a complex cystic lesion but no malignant finding. According to the Bosniak classification the lesion will be classified as a Bosniak 2F cyst.
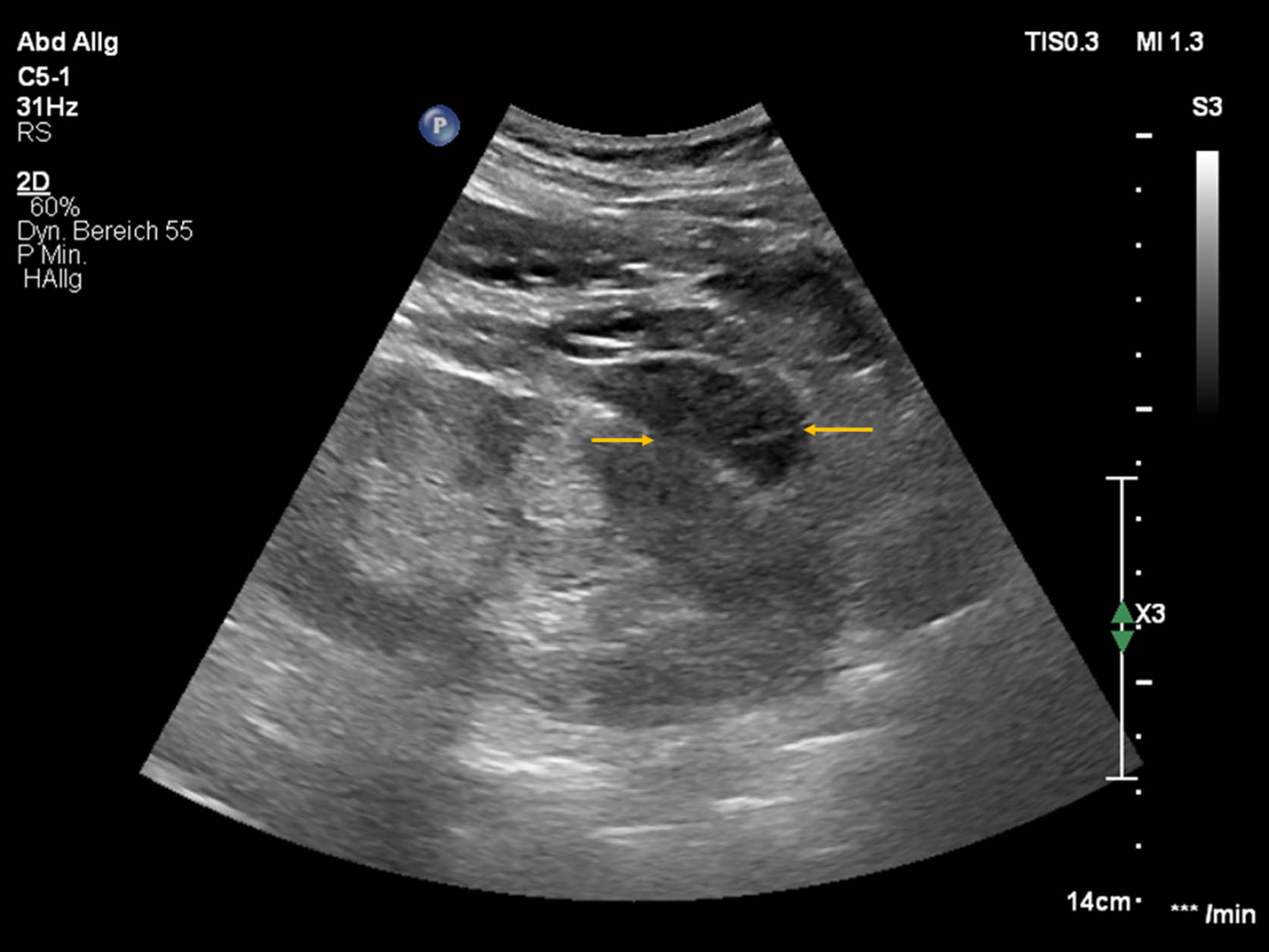
If the cysts show irregular thickening of the septa or walls that are greater than 3 mm, of if they show calcifications, these lesions are classified as category III and about 54% of the cases are malignant and must be clarified surgically [27, 33–36] (Figs. 3–6).
B-mode ultrasound shows an exophytic growing cystic lesion with some enlarged septums (yellow arrows).
In color doppler examination the lesion (yellow arrows) shows no vascularization only one vessel could be detected.
Using the dual imaging CEUS setting, with CEUS image of the cystic lesion (white arrows) on the left side and greyscale image on the right side (yellow arrows) of the image. During the contrast arterial examination, the lesion shows a strong contrast uptake.
Using the dual imaging CEUS setting, with CEUS image of the cyst lesion (white arrows) on the left side and greyscale image on the right side (yellow arrows) of the image. During the contrast examination in the late phase the lesion shows a washout in comparison to the surrounding renal tissue. The final diagnosis will be tumor with some cystic component. According to the Bosniak classification the lesion was classify as a Bosniak 3 cyst. The patient undergoes surgery and the final diagnosis was a cystic renal clear cell carcinoma,
In category IV of the Bosniak classification, kidney lesions were found to show up to 91% of which can be classified as malignant masses [62]. In addition to the category III criteria, they show nodular or irregular soft-tissue lesions that show contrast enhancement. They are also treated surgically since a fine-needle biopsy is considered contraindicated here due to the possible tumor seeding through the puncture canal [37].
90% of kidney tumors are renal cell carcinoma and it is one of the most common malignancies in adults [37, 38]. Here the clear cell carcinoma dominates with approx. 70%, the papillary NCC with 10–15% (Figs. 7–9) and the chromophobic with about 5% [63–64]. The challenge with renal cell carcinoma is that it usually only becomes symptomatic in the advanced stages and it is often only detected as an incidental finding during examinations [34].
B-mode ultrasound shows an exophytic growing cystic lesion (yellow arrows).

Using the dual imaging CEUS setting, with CEUS image of the renal lesion (white arrows) on the left side and greyscale image on the right side (yellow arrows) of the image. During the contrast arterial examination, the lesion shows a moderate contrast uptake, less in comparison to the surrounding renal tissue.
Using the dual imaging CEUS setting, with CEUS image of the lesion (white arrows) on the left side and greyscale image on the right side (yellow arrows) of the image. During the contrast examination in the late phase the lesion shows a washout in comparison to the surrounding renal tissue. According to finding high suspicion of a papillary renal cell cancer which was later confirmed by surgery and histological workup.
In renal cysts, the solid parts of the renal masses or their vascularization behavior are usually used for differentiation. Standard therapy depends on the size of the lesion and consists of either partial nephrectomy or total nephrectomy [43]. Thus, the assessment of the dignity and also the most accurate determination of the tumor size is an essential factor in the therapy decision. With the conventional B-mode and color doppler sonography, vascularity, septation and the solid components can be evaluated. However, there is often a limitation in the detection of slow flows of small vessels [44, 45]. CEUS has been shown in a series of studies to be an accurate method for diagnosing NCC [6, 47]. It shows a heterogeneous enhancement due to intratumoral necrosis and hemorrhage as well as a marginal enhancement, which is due to the pseudocapsule of the tumor, also showing an early wash-out [48].
One of the main benefits performing an CEUS-guided puncture or biopsy is the ability to obtain morphological information regarding the microvascular blood supply and blood flow in lesions that could otherwise only be obtained by CT or MRI. This advantage makes it possible to differentiate between vascularized and non-vascularized tumor tissue in order to perform a targeted puncture/biopsy and, conversely, to obtain a higher quantity tissue for histopathological analysis. This fact is mainly relevant in partially necrotic lesions which offers a great benefit in contrast to non-dynamic investigations like CT or MRI.
Renal artery pseudoaneurysm can occur after renal biopsy, renal trauma or surgery [49–53]. Patients often present with non-specific symptoms such as abdominal or flank pain within a few days to months, e.g. after partial nephrectomy [51, 55]. A ruptured renal artery pseudoaneurysm can lead to potentially life-threatening haemorrhage and usually requires immediate therapy. The treatment of choice is selective embolisation of the aneursyma [56, 57] (Figs. 10–14). The couple of papers describe the possible applications of CEUS in primary diagnostics, during intervention and in follow-up. The authors conclude that CEUS is a suitable instrument for monitoring angiographic embolisation [58–61].

Patient with deterioration from acute to chronic renal insufficiency underwent renal biopsy to clarify the status. In the follow up ultrasound was performed and detected a peripheral subcapsular pseudoaneurysm (white arrows).

Using the dual imaging CEUS setting, with CEUS image of the renal lesion (white arrows) on the left side and greyscale image on the right side (yellow arrows) of the image. During the contrast arterial examination, the lesion shows a strong contrast uptake with only one feeding vessel. Additionally, a subcapsular hematoma was detected.

Patient underwent invention of the kidney. Pseudoaneusyma is seen pre-interventional (white arrows) and after microcoil embolization (yellow arrows).
B-mode ultrasound detected in the follow up the subcapsular hematoma (yellow arrows) the old pseudoaneurysm is not visible.

Using the dual imaging CEUS setting, with CEUS image on the left side and greyscale image on the right side of the image. CEUS detected the subcapsular hematoma (white arrow) and confirmed the complete occlusion of the pseudoaneurysm.
Today, CEUS is a clinical standard for the most common unclear renal lesions, because of the low cost and the good availability. In the hands of the experienced examiner, it enables effective diagnosis and characterisation of kidney tumours. Thus, this technique represents an examination with a wide range of possible clinical applications in daily routine. Since UCA are blood pool contrast agents and the possibility to acquire image data sets in real time, it is possible to gain additional information about the vascularization of renal cystic tissue with a high temporal resolution. CEUS is especially a benefit for patients with contraindications for other imaging modalities like MRI or CT.