
Abstract
BACKGROUND:
Monitoring liver changes is crucial in the management of liver fibrosis. Current diagnostic methods include liver function tests such as the Liver Maximum Capacity (LiMAx) test and measurements of liver stiffness. While the LiMAx test quantifies liver function through 13C-methacetin metabolism, ultrasound (US) elastography noninvasively assesses liver stiffness. The relationship between the findings of these methods in patients with liver fibrosis is not fullyunderstood.
OBJECTIVE:
This study evaluated the correlation between LiMAx measurements of liver function and US elastography-based liver stiffness measurements to better understand the interplay between functional and structural liver parameters in fibrotic liver disease. Additionally, the relationship between body mass index (BMI) and these parameters isevaluated.
METHODS:
This retrospective study analysed data from 97 patients who underwent both LiMAx testing and real-time elastography, resulting in a total data set of 108 examinations. The correlations between the results of the LiMAx test and elastography and their relationships with body mass index (BMI) were analysed.
RESULTS:
There was a significant negative correlation (r = –0.25, p < 0.05) between LiMAx test values and liver stiffness measurements. BMI was significantly negatively correlated with LiMAx values (r = –0.29, p < 0.001) but not significantly correlated with liver stiffness values.
CONCLUSIONS:
This retrospective study confirms the results of previous studies showing a notable but weak association between liver function and liver stiffness. Our results highlight the potential value of both tests as complementary tools for the evaluation of liver health, reinforcing the necessity for a multimodal approach to liver assessment.
Introduction
Liver fibrosis and its end stage, cirrhosis, are significant and widespread health problems worldwide. It is estimated that cirrhosis affects approximately 1% of the world population, although the true prevalence of liver fibrosis is likely to be much higher [1]. The consequences of advanced fibrosis are associated with a high risk of complications such as portal hypertension, liver failure and hepatocellular carcinoma. These complications are associated with high morbidity and mortality, increasing the importance of implementing preventive measures, developing effective therapies and conducting intensive research in this area.
The diagnostic gold standard for assessing and quantifying liver fibrosis is liver biopsy. Through direct histological examination of liver tissue, biopsy allows accurate staging of fibrosis, which is essential for prognostication and treatment planning [2]. However, any invasive procedure, including liver biopsy, can lead to significant complications. Liver biopsy these can result in bleeding, infection or injury to nearby organs. In addition, the heterogeneous distribution of fibrosis, needle positioning or inadequate sampling can significantly limit the diagnostic value of these methods. For this reason, efforts to develop noninvasive methods are increasing, and the status and necessity of liver biopsy are becoming increasingly controversial [3]. In addition to numerous other noninvasive methods, ultrasound (US)-based methods of detecting liver fibrosis, especially US elastography, are at the forefront [4–6].
US elastography is based on one of the oldest medical examination techniques: palpation. US elastography is used in the evaluation of many organs and tissues, including the breasts, thyroid, prostate, kidneys, lymph nodes, and liver [7]. US elastography can be used to visualise the mechanical properties of liver tissue and provides information on the degree of fibrosis. US elastography has been shown to have high diagnostic accuracy in assessing liver fibrosis [4, 9].
The 13 C methacetin test has also been studied in the context of liver fibrosis. The effectiveness of the test in visualising declining liver function in the context of progressive fibrosis was confirmed by Lock et al. [10]. Liver Maximum Capacity (LiMAx) test results were shown to be correlated with the degree of fibrosis, and the LiMAx test was demonstrated to be sensitive to early changes in liver function before fibrosis becomes visible on biopsy [11]. The 13 C methacetin test provides a dynamic assessment of liver function on the basis of the metabolism of 13C-methacetin by the hepatocyte-specific cytochrome P450 1A2 system. Although both methods are noninvasive and can provide valuable information about the condition of the liver, many questions remain about the usefulness of both methods, the relationship of their results, and their practical clinical application.
This retrospective study aimed to investigate the correlation between LiMAx and US elastography findings in patients with liver fibrosis. The focus of the study is on whether the LiMAx test is a reliable method of identifying declining liver function in the context of liver fibrosis and to what extent the results correlate with US elastography findings. To gain insight into the potential role of the 13 C methacetin test in the diagnosis and monitoring of liver fibrosis, a better understanding of the relationship between its results and US elastography findings is needed. This knowledge will help to advance current efforts to diagnose and monitor hepatic fibrosis in a noninvasive manner.
Methods
Study design
This retrospective study was approved by the local ethics committee (No. 12-101-0141). Written informed consent and patient assent were obtained. The study analysed 108 examinations in 97 patients in whom both US elastography (Elasto) and the 13 C methacetin test (LiMAx, Humedics) were performed as part of routine clinical practice. In addition to the patients’ demographic data, their height and weight were collected to determine their body mass index (BMI). BMI was calculated with the following formula: body weight divided by the square of height, expressed in kg/m2.
LiMAx testing
The LiMAx test was carried out as previously described [12–14]. Patients fasted for 3 hours before the examination. The respiratory ratio of 13CO2 to 12CO2 was determined ten minutes before the intravenous injection of 13C-methacetin. The difference between the delta value and the baseline value was determined. When a constant value was reached, a 2 mg/kg body weight dose of methacetin was injected as an intravenous bolus and flushed with 20 ml 0.9% NaCl. The 13CO2 concentration was then analysed via a LiMAx device (Humedics GmbH, Berlin, Germany). The measurement took a maximum of 60 minutes. A LiMAx value above 315 is an indicator of normal liver function, whereas a lower value indicates liver function impairment [11].
US elastography
All US scans were performed by an experienced sonographer who performs more than 5000 scans per year. Real-time elastography (RTE) was performed via a convex multifrequency probe (1–5 MHz, LOGIQ E9, GE Healthcare). A quality indicator (1–5) provides visual feedback to monitor the compression technique and make elastography reproducible. Only elastograms with the highest quality indicator of 4 or 5 were used in this study. In cases where more than one elastogram value was obtained during an examination, the mean value was taken and used for further evaluation. The grade of fibrosis was based on the results of US elastography, in accordance with Colombo et al. (2012) [15].
Statistical analysis
GraphPad Prism for Windows version 10.2.3 was used for the statistical analysis (GraphPad Software, San Diego, California, USA). The categorical variables are presented as absolute values, and the continuous variables are presented as the means with standard deviations (SDs). The data were tested for a normal distribution via the D'Agostino & Pearson test. The LiMAx test results, the elastography values and the BMIs were not normally distributed. For comparability and normal distribution, the elastography, LiMAx and BMIs were normalised, with the lowest value of each data set defined as 0% and the highest as 100%. An outlier analysis was performed beforehand via the ROUT technique and a coefficient Q of 1%. As a result, 3 examinations were excluded from further analyses, and further analyses were performed with n = 105 examinations. Ordinary one-way analysis of variance (ANOVA) with a Tukey post hoc test, simple linear regression and Pearson correlation analysis were performed to compare the results. Following the usual conventions of Cohen (1988), correlations up to 0.1 were interpreted as ‘negligible effects’, those below 0.3 as ‘weak effects’, those below 0.5 as ‘moderate effects’, and those above 0.5 as ‘strong effects’. [16]. In all analyses, a p value of less than 0.05 was considered statistically significant.
Results
In this study, 108 examinations were analysed from 97 patients who had undergone both US elastography (Elasto) and a liver function diagnostic test with the LiMAx test. The characteristics of the study population are shown in Table 1. The mean age of the patients analysed was 63±10 years, and 80% were male. Among the patients, 18% had no fibrosis (grade 0), 36% had grade 1 fibrosis, 12% had grade 2 fibrosis, 28% had grade 3 fibrosis, and 6% had grade 4 fibrosis. The mean height of the patients was 173±9.1 cm, the mean weight was 85±17 kg, and the mean BMI of the patients was 28±5.5 kg/m2.
Characteristics of the population studied. Number of subjects (n) = 97 for a total of 108 examinations
Characteristics of the population studied. Number of subjects (n) = 97 for a total of 108 examinations
Data are presented as the mean (±standard deviation) for continuous variables and n (%) for categorical variables. LiMAx = Liver Maximum Capacity.
The mean LiMAx value was 212±121 μg/kg/h, and the mean Elasto value was 1.8±0.53 m/s. The relationships among the Elasto values, LiMAx values and patient BMI are shown in Fig. 1. For all three variables, the values were not normally distributed. Therefore, for further analysis, the values were normalised by defining the lowest value as 0% and the highest value as 100%. All outliers were removed beforehand. As a result, only 105 examinations were subjected to further analysis. Moreover, this procedure enables a direct comparison of these three variables.
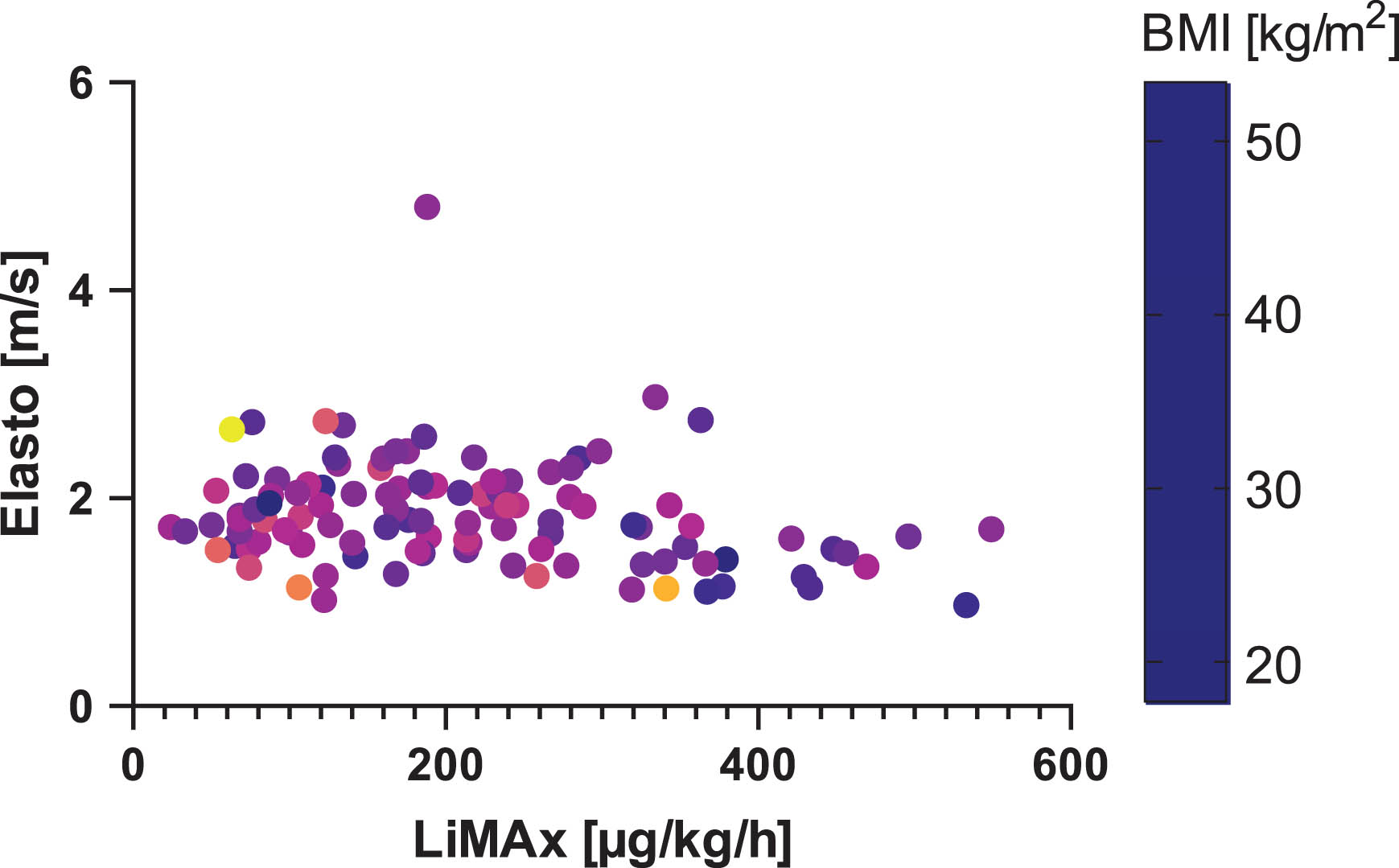
Scatter plot of the collected data. BMI = body mass index, Elasto = ultrasound elastography, LiMAx = Liver Maximum Capacity.
The normalised values are presented as a box plot in Fig. 2. The mean normalised LiMAx value was 36±23%, the mean normalised Elasto value was 42±21%, and the mean normalised BMI was 29±13%. An ordinary one-way ANOVA revealed a statistically significant difference in group means, F (2,318) = 9.083, p < 0.0001. Post hoc analysis indicated that the means of all the groups were significantly different from each other (see Fig. 2).
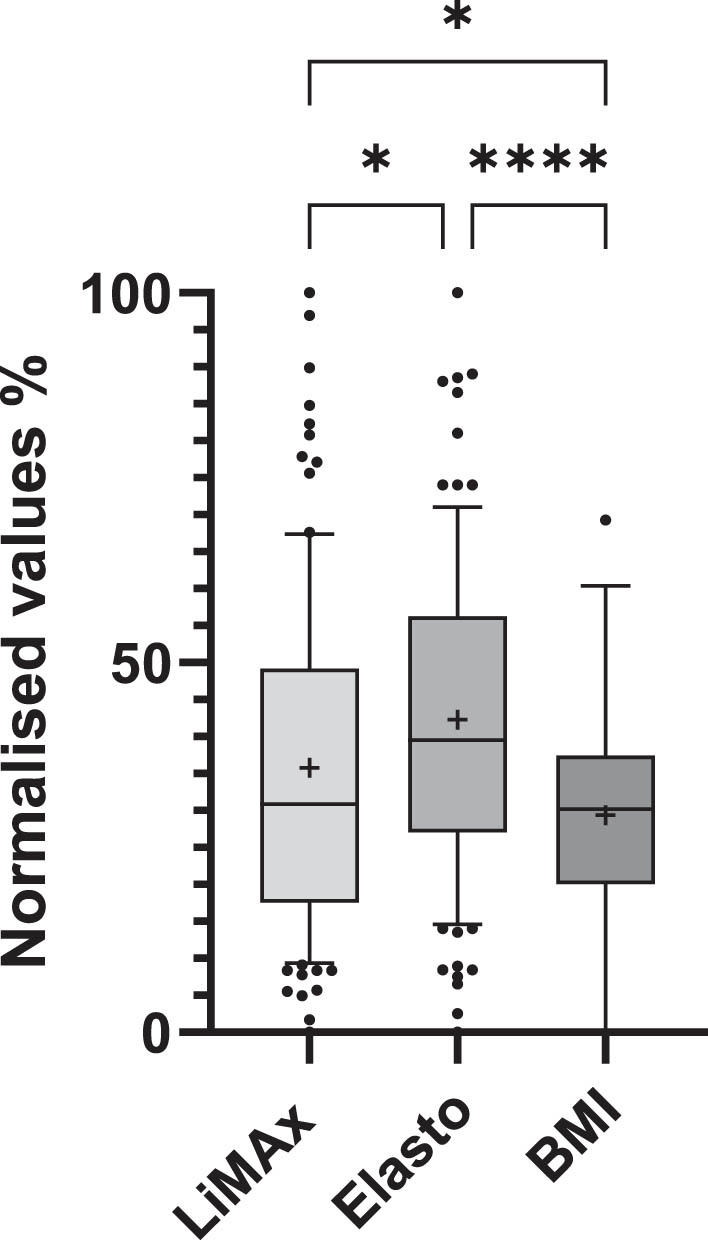
Comparison of normalised LiMAx values, Elasto values and BMIs. The data are based on n = 105 examinations. The median is shown as a box plot with the 25th to 75th percentiles, and the whiskers represent the 10th to 90th percentiles. The+represents the mean. Pairwise differences were calculated via ordinal one-way ANOVA. The interpretation of the two-tailed p value analysis is shown as (* = <0.05; **** = <0.0001). ANOVA = analysis of variance, BMI = body mass index. Elasto = ultrasound elastography, LiMAx = Liver Maximum Capacity.
A Pearson correlation analysis was performed to examine the relationships the LiMAx value, Elasto value and BMI. The results are shown in Table 2. The LiMAx value shows a statistically significant weak negative correlation with both the Elasto value (r = –0.25) and the BMI (r = –0.29). Conversely, no statistically significant relationship was observed between the Elasto value and the BMI (r = 0.01). To further investigate the relationship between LiMAx and Elasto values, a linear regression analysis was performed. The results are illustrated in the scatterplot in Fig. 3. The linear regression revealed a slight negative relationship between LiMAx and Elasto values. However, the coefficient of determination (r2) was notably low at 0.06, indicating that only 6% of the variance in Elasto values can be explained by LiMAx values. This weak linear relationship suggests that LiMAx has limited predictive power for Elasto values.
Pearson correlation matrix of the normalised values (n = 105)
* < 0,05, ** < 0,01, BMI = body mass index, Elasto = ultrasound elastography, LiMAx = Liver Maximum Capacity.
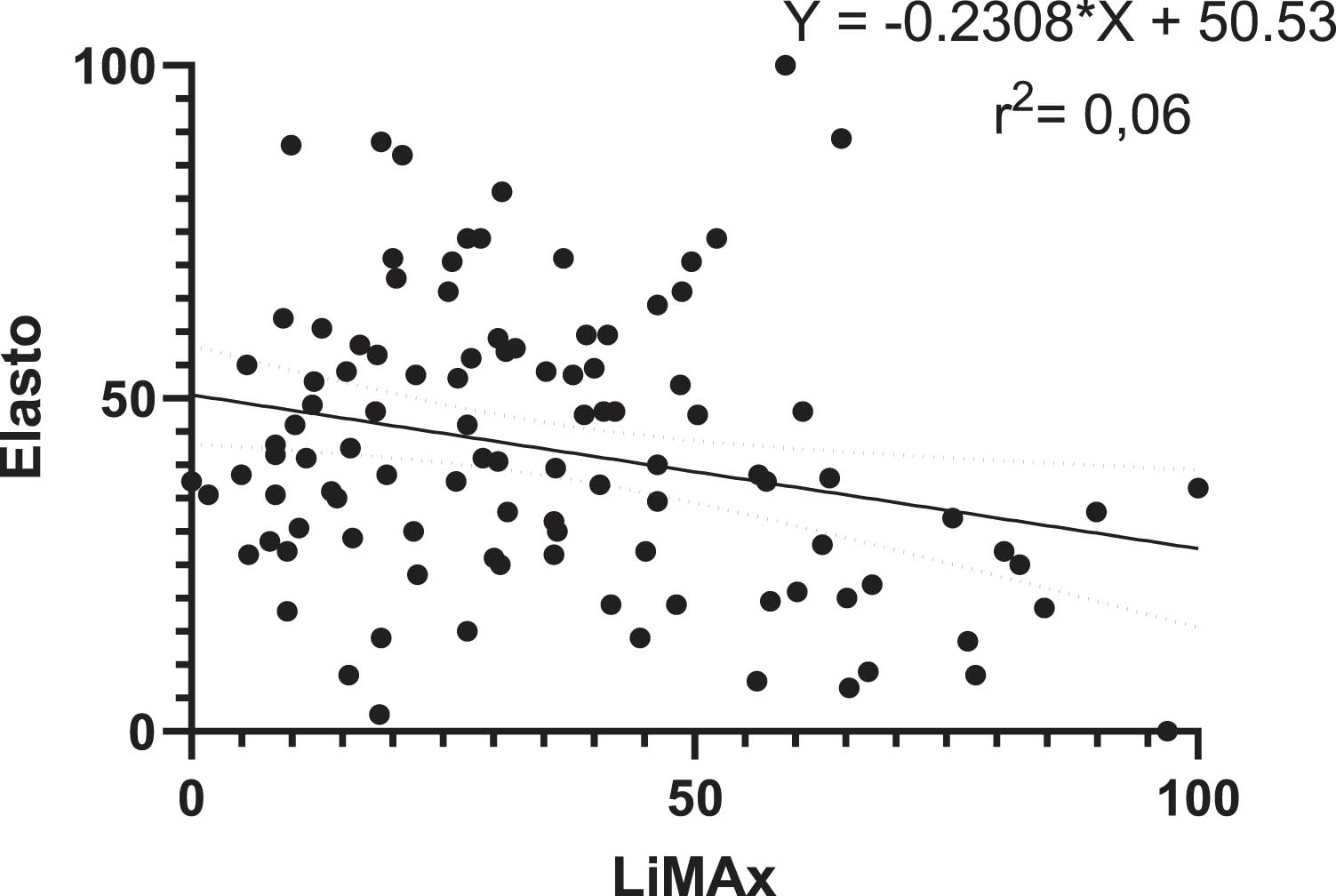
Scatter plot of the normalised Elasto and LiMAx values in %. The number of examinations is n = 105. The solid line represents the results of linear regression, and the 95% confidence interval is shown as a dashed line. The linear regression formula is shown with the coefficient of determination. BMI = body mass index. Elasto = ultrasound elastography, LiMAx = Liver Maximum Capacity.
The aim of this exploratory study was to investigate the relationship between US elastography findings and the LiMAx test results in the context of fibrosis. Both tests measure two different liver characteristics, US elastography measures the elasticity of the whole liver and the LiMAx test measures liver function, more specifically, hepatocyte function. Both are important noninvasive methods for assessing patients with liver disease and monitoring disease progression. However, how the results of the two methods are related to each other is unclear. The results of this study demonstrated a significant but weak correlation between LiMax and Elasto, with a near absence of a linear relationship between these variables. This highlights the potential value of both tests as supplementary tools for the evaluation of liver health, reinforcing the necessity for a multimodal approach to liver assessment.
US elastography measures tissue rigidity, i.e., tissue stiffness or elasticity, in other words, the mechanical properties of liver tissue [17]. Several factors, including the deposition of collagen and other extracellular matrix proteins, tissue inflammation and fat accumulation in the liver, contribute to tissue stiffness [18]. However, tissue stiffness is influenced primarily by the extracellular matrix and structural components, not by specific cells. However, some cells contribute to liver stiffness. These include hepatic stellate cells (HSCs), which, when activated, transform into myofibroblasts and produce extracellular matrix proteins, particularly collagen [18]. This increased collagen deposition leads to an increase in liver stiffness. Kupffer cells can also contribute to the progression of fibrosis by modulating inflammation, cytokine production and HSC activation, thus playing a central role in fibrogenic processes and indirectly influencing liver stiffness. [19]. Sinusoidal endothelial cells can also contribute to fibrosis in the event of liver dysfunction [20, 21]. Although hepatocytes, which are particularly important for liver function, are not directly responsible for liver stiffness, damaged or inflamed hepatocytes can trigger fibrogenic reactions and thus indirectly contribute to liver stiffness [22, 23]. On the other hand, LiMAx test results reflect hepatocyte function [11, 24]. The LiMAx test is based on the metabolism of 13C-methacetin by hepatocytes, specifically by the cytochrome P450 1A2 (CYP1A2) enzyme system. This enzyme system is found mainly in hepatocytes. [25]. The LiMAx test is a dynamic test, and its results reflect a patient’s actual liver function at the time of measurement. Importantly, liver function can be assessed through a variety of methods [26]. These include both the analysis of conventional laboratory parameters and the assessment of hepatic metabolic capacity using specific enzymes that are predominantly expressed in hepatocytes. An example of the latter is the LiMAx test, which quantifies the activity of cytochrome P450 1A2 [25]. In the context of fibrosis, a liver function test is particularly important for monitoring patients, as the structural damage to the liver that occurs in fibrosis and cirrhosis is often accompanied by a decline in liver function. This explains why a linear correlation between the results of these two methods was not expected. On the other hand, the weak correlation between a functional value and a tissue property value has also been demonstrated in other studies. For example, a weak correlation was found between liver stiffness measured by transient elastography and liver function measured by the indocyanine green (ICG R15) test [27]. However, another study found a strong correlation of liver stiffness measured by using acoustic radiation force impulse imaging and liver function measured with the ICG R15 test [28]. Similarly, another study found a strong correlation between liver stiffness measured by magnetic resonance (MR) elastography and liver function measured with the ICG-R15 test in patients with hepatocellular carcinoma [29]. These studies all used the ICG R15 test to determine liver function, but the use of other nonblood liver function tests has not been widely investigated. There has been only one study examined the correlation between liver function measured with the LiMAx test and liver stiffness measured as shear wave velocity by 2D temporal harmonic elastography (THE) [30]. A strong negative correlation was found. The main differences between their study and this study were that they used a different elastography technique than the one used in this study and they included a control group of healthy volunteers in their study. In addition, the mean LiMAx value of the patients in their study was greater than that found in this study (308 vs. 212 μg/kg/h), indicating that the patients in their study had superior liver function. However, although only a weak negative correlation was found in this study, the results listed here show that a correlation exists between the liver function score and liver stiffness and that although all the studies mentioned here used different elastographic measurements, each with its own advantages and disadvantages [17, 31–33], they all found a correlation between the liver function score and liver stiffness. Future controlled prospective studies with healthy control groups need to be performed to investigate the strength of this correlation and the details of the relationship.
In the context of fibrosis, BMI and obesity are often discussed as risk factors for the development of fibrosis [34–37]. This was the rationale for examining BMI as part of this study. Here, we revealed a weak significant correlation between the LiMAx test score and BMI but no significant correlation between BMI and liver stiffness. This was also reported by Heucke et al., but in their study, they did not find a correlation between the LiMAx score and BMI [30].
This study has several limitations. The exploratory nature of the study did not allow consideration of the underlying disease, resulting in a heterogeneous cohort of patients. This also meant that the majority of the data came from male patients. Even the measurement methods used have limitations and disadvantages, such as limitations in obese patients, which make correct elastography measurements difficult to obtain. The LiMAx test also has its limitations [38]. In addition, bias due to intra- and interreader variability was not considered in this study. Furthermore, the use of different elastography measurement methods makes comparisons with other studies difficult.
In conclusion, there is only a weak relationship between LiMAx and Elasto representing liver function and liver tissue characteristics, respectively. Therefore, structural changes in the liver should not be considered in isolation but rather in conjunction with functional impairments, which together provide a comprehensive picture of liver pathology. Furthermore, for the noninvasive diagnosis of both fibrosis and cirrhosis, these methods could provide significant added value. On the one hand, LiMAx and Elasto could complement each other, with one method compensating for a possible over- or underestimation of fibrosis by the other method. On the other hand, the consistency of the findings of both methods significantly increases diagnostic confidence. Future research should use combined diagnostic methods, preferably in a defined patient population with healthy controls, to optimise the use of these methods in clinical practice and improve outcomes for patients with liver disease. Investigating the linear and temporal relationships of liver function and liver stiffness could not only shed light on the longitudinal course of fibrosis but also provide insights into the causal relationship between progressive stiffening and the associated loss of function. These findings greatly increase our understanding of the pathogenesis of liver fibrosis and may provide new targets for therapeutic intervention.