
Abstract
There has been extensive use of machine learning (ML) based tools for mathematical symbol and phrase categorization and prediction. Aiming to thoroughly analyze the existing methods for categorizing brain tumors, this paper considers both machine-learning and non-machine-learning approaches. From 2013 to 2023, the writers compiled and reviewed research papers on brain tumor detection. Wiley, IEEE-Explore, Science-Direct, Scopus, ACM-Digital Library, and others provide the relevant data. A systematic literature review examines the efficacy of research methodologies over the last ten years or more by compiling relevant publications and studies from various sources. Accuracy, sensitivity, specificity, and computing efficiency are some of the criteria that researchers use to evaluate these methods. The availability of labeled data, the required degree of automation and accuracy in the classification process, and the unique dataset are generally the deciding factors in the method choice. This work integrates previous research findings to summarize the current state of brain tumor categorization. This paper summarizes the 169 research papers in brain tumor detection between 2013–2023 and explores the application and development of machine learning methods in brain tumor detection, which has significant research implications and value in the field of brain tumor classification research. All research findings of previous studies are arranged in this paper in the form of research questions and answers format.
Introduction
One major factor that contributes to the global mortality rate is the prevalence of brain tumors. The GLOBOCAN 2020 study states that there were 308,102 new instances of brain cancer and that 2.5% of the population lost their lives to this disease [1]. Among brain tumors, gliomas, meningiomas, pituitary adenomas, and nerve sheath tumors are the four most common kinds. Brain tumors are ranked from least aggressive to most aggressive by the World Health Organization (WHO) according to cell origin and behaviour [2]. Among the many types of brain tumors, two stand out: low-grade gliomas (LGG) (grades I and II) and high-grade gliomas (HGG) (grades III and IV). Although the HGG has a maximum lifespan of only two years, it multiplies rapidly.
On the other hand, LGG develops at a more leisurely pace, which can add years to the subject’s expected lifespan. Indeed, brain tumors exhibit a wide range of features, such as a lack of contrast, heterogeneity in size and shape, and the tendency to overlap with the intensity values of normal brain tissues.
The appearance of brain tumors might vary significantly from one another. It is imperative to understand these distinctions for diagnosis, treatment planning, and prognosis assessment. These are some crucial facts regarding brain tumors that we should be aware of [3]:
Type of Tumor: Primary brain tumors originate in the brain, whereas secondary cancers, often known as metastases, originate in other parts of the body and spread to the brain. Location: The cerebellum, brainstem, cerebral hemispheres, and meninges are just a few brain regions where brain tumors can develop. Size and Growth Pattern: Brain tumors can be large and diffuse into surrounding brain tissue or small and confined. Morphological Features: On MRI or CT scans, tumors may exhibit various morphological features, including shape, boundaries, and enhancement patterns. Vascularity: Blood flow to brain tumors varies; some have many blood vessels, while others have few. Genetic: Advances in molecular screening have made it possible to identify particular genetic alterations and molecular indicators connected to different kinds of brain cancers.
There are ramifications for patient therapy resulting from these traits since they influence the complexity of tumor growth and predict the degree of resection during surgical planning [4]. Consequently, accurate categorization and the differentiation of normal tissues from tumors are challenging. For exact tumor size, location, and type determination, trustworthy segmentation and brain tumor categorization are crucial. Early detection is vital to treat brain tumors successfully. Brain tumor identification relies heavily on non-invasive medical imaging modalities such as positron emission tomography (PET), magnetic resonance imaging (MRI), computed tomography (CT), cerebral angiography, myelography, and cerebral angiography [5]. The detailed scans provided by MRI make it easy to detect brain tumors and other illnesses. In addition, magnetic resonance imaging (MRI) is the gold standard for diagnosing various disorders and developing treatment plans, particularly for brain tumors [6]. Neurological MR images are acquired from three perspectives: axial, coronal, and sagittal, which are used to diagnose brain tumors [7]. Radiologists are first relied upon for identifying brain tumors after thorough picture surveillance and accurate analysis. Unfortunately, there is a lack of readily available domain knowledge experts; therefore, this procedure takes a long time. Radiologists can make faster, more accurate diagnoses of brain tumors with the use of Computer-aided diagnosis (CAD) systems, which in turn reduces the death rate from brain tumor. The primary goal of the CAD is to automate the diagnosis of brain tumors in images with a higher level of authenticity and reliability. When it comes to the identification and treatment of brain tumors, computer-aided diagnosis (CAD) systems are an extremely important diagnostic tool. Imaging techniques play a crucial role in the diagnosis, characterization, treatment planning, and monitoring of brain tumors [8].
Identifying, categorizing, and segmenting brain tumors has been the subject of numerous published articles. Traditional, machine learning-based methods have been the primary emphasis of prior studies. Big data problems, like brain tumor segmentation, are well-suited to machine learning (ML) approaches. Image identification, however, typically necessitates human involvement and knowledge, and it has been utilized to train machines for this task [9]. To distinguish between tumor characteristics and imaging data features, conventional ML approaches use feature extraction techniques based on human design [10]. To anticipate underlying tumor molecular changes using handcrafted attributes, a new study was presented based on a decision tree classifier. Decision tree classifiers simplify brain tumor categorization and allow clinicians to grasp the decision-making process. Tree structure decision rules are easy to understand, helping radiologists, oncologists, and patients communicate [11]. The biopsies of thirteen individuals were used to extract these properties using textural metrics. Conversely, DL methods learn the best features for classification and prediction; therefore, pre-selection is unnecessary. Using multi-level feature extraction, deep learning automatically mines relevant features, assesses patterns, and classifies data. Corners, edges, and simple forms are examples of lower-level features, whereas picture texture, more processed shapes, and specific patterns are examples of higher-level characteristics [12]. In addition, the recommendation procedure incorporates components extracted from supplementary data using deep learning techniques [13]. Nevertheless, it breaks down regarding visual demarcation and spatial consistency. Consequently, hybrid-based approaches have recently become the standard in brain tumor detection, segmentation, and classification research. To improve the overall accuracy, a hybrid approach utilizes many classifier systems’ strengths in one system. We were compelled to do a comprehensive literature study spanning the past ten years on the dramatic change in how brain tumor analysis is approached, which has seen a move away from traditional machine learning methods and toward deep learning and hybrid approaches.
Ensemble methods use multiple base classifiers to improve classification results. In hybrid Methods, a Support Vector Machine (SVM), a Random Forest (RF), and a Convolutional Neural Network (CNN) may all be used together in a hybrid method to classify brain tumors [13].
Deep learning techniques are a powerful way to automatically learn essential features from images of brain tumors. This lets computers classify them correctly and reliably without doing feature engineering by hand. Because of these benefits, deep learning is an excellent way to deal with the difficulties and complexities of brain tumor classification tasks [14].
This review summarizes the literature on segmenting brain tumors, extracting features from brain MRI scans, and classifying them. Recent developments in brain tumor classification serve as essential research objectives to advance the field and improve clinical outcomes. Research findings on enhancing Classification Accuracy with Deep Learning Architectures, Advancements in CNN, Integrating Multi-Modal and Multi-Scale Information, Improving Model Interpretability and Explainability, and Addressing Data Limitations and Model Generalization are the primary concerns of this systematic literature review. All objectives are addressed in a questions-answers format.
This review is an effort to aid researchers in developing cutting-edge computer-aided diagnosis (CAD) technologies that can assist radiologists in the early detection of brain cancers. The goal is to showcase the most recent developments in tumor prognosis using deep learning and a hybrid-based methodology.
The goal is to draw attention to the opportunities and unanswered questions surrounding the development of wholly automated methods for detecting brain tumors.
Finally, there has been research and comparison of the 2013–2023 multi-modal MR scan performance of CAD systems for brain malignancies regarding tumor segmentation, feature extraction, and classification. We have utilized several search queries in publicly available databases such as Science Direct, Scopus, Google-Scholar, IEEE-Explorer, and PubMed to locate the most pertinent papers for this manuscript. For this reason, we will only consider manuscripts published between 2013 and 2023. Among the many combinations of queries we have employed are: “brain cancer diagnosis”, “brain tumor segmentation and classification”, “brain tumor detection using machine learning and deep learning classifiers”, “brain tumor MRI and deep learning”, “brain tumor using Harvard dataset”, “brain tumor detection and Brain Web dataset”, “brain tumor detection and segmentation using TCIA dataset”, “artificial intelligence and brain tumor” and so on. After a comprehensive evaluation of over 300 studies, we selected 169 most applicable to brain tumor detection, segmentation, and classification for this manuscript.
Motivation
Table 1 lists the several reasons why study in this area is essential. The absence of a comprehensive survey that could gather and extract all the critical factors such as classification models, datasets, subprocesses, performance metrics, and other meta-data analysis; while maintaining a clear and transparent selection and synthesis process was the main impetus for writing this research review in this field. This allows for a more refined audience and offers more precise insights from the existing literature on brain tumor classification.
Motivation factors.
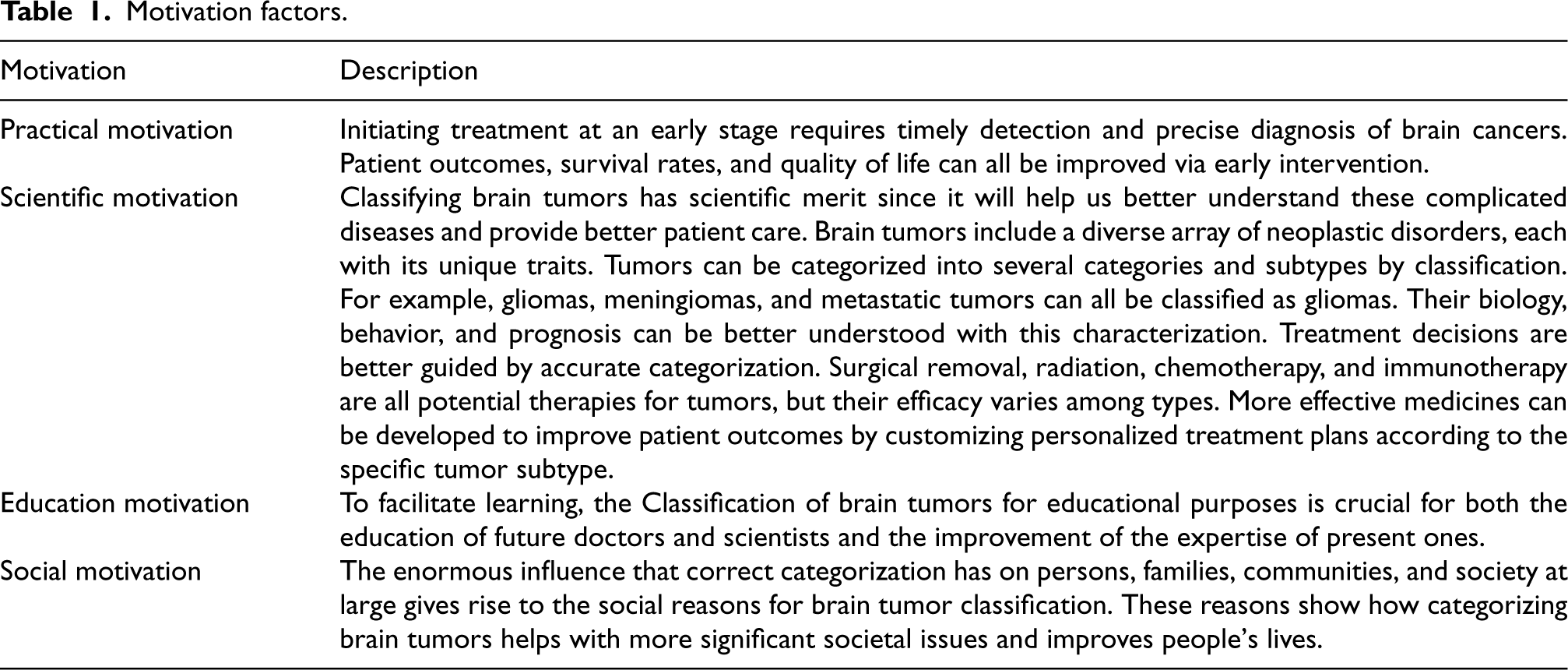
Motivation factors.
To better grasp the ever-changing field of brain tumor segmentation and classification. To lay the groundwork for future study by documenting areas where brain tumors are not yet recognized or classified. Concluding and assertions based on the literature’s meta-data and evidence.
A fair and comprehensive analysis based on the evidence acquired from the literature and all the metadata extracted through this method is the primary purpose of this systematic literature review (SLR). The data and conclusions from this study will direct future research on brain tumor classification.
The research questions addressed by this study are tabulated in Table 2.
Motivation and research questions.
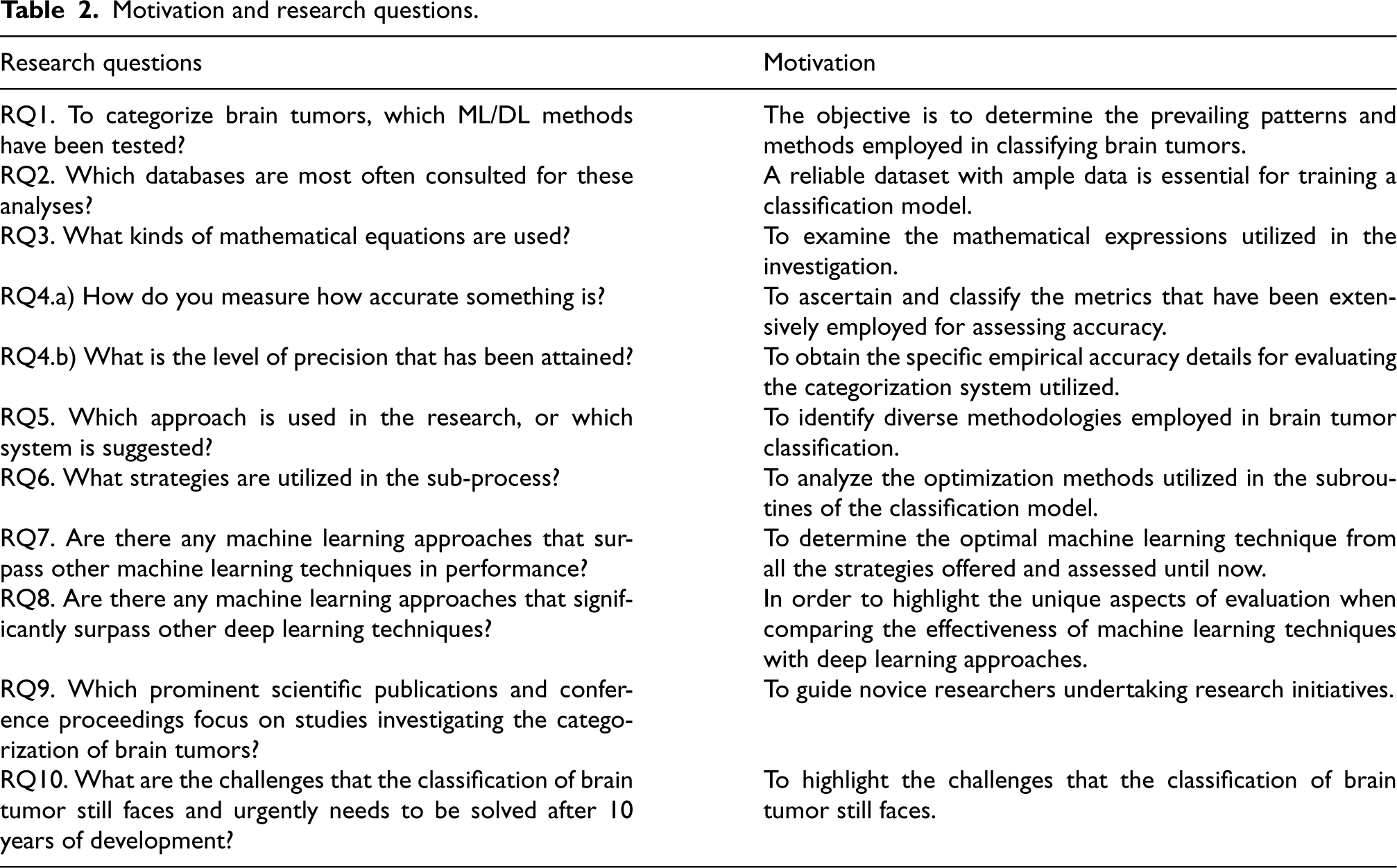
Motivation and research questions.
Section 2 provides an overview of the research background. In Section 3, the complete research methodology is outlined. Section 4 provides a comprehensive statistical analysis of the studies relevant to brain tumors. Section 5 encompasses the outcomes and deliberations about the formulated research inquiries. Section 6 presents a comprehensive analysis of the findings, focusing on critical conclusions and noteworthy facts. This analysis is organized under the heading “Summary and Findings.” The study’s limitations are laid out in Section 7, while the derived findings are presented in Section 8. Figure 1 presents the complete roadmap for organizing the document to improve its readability.
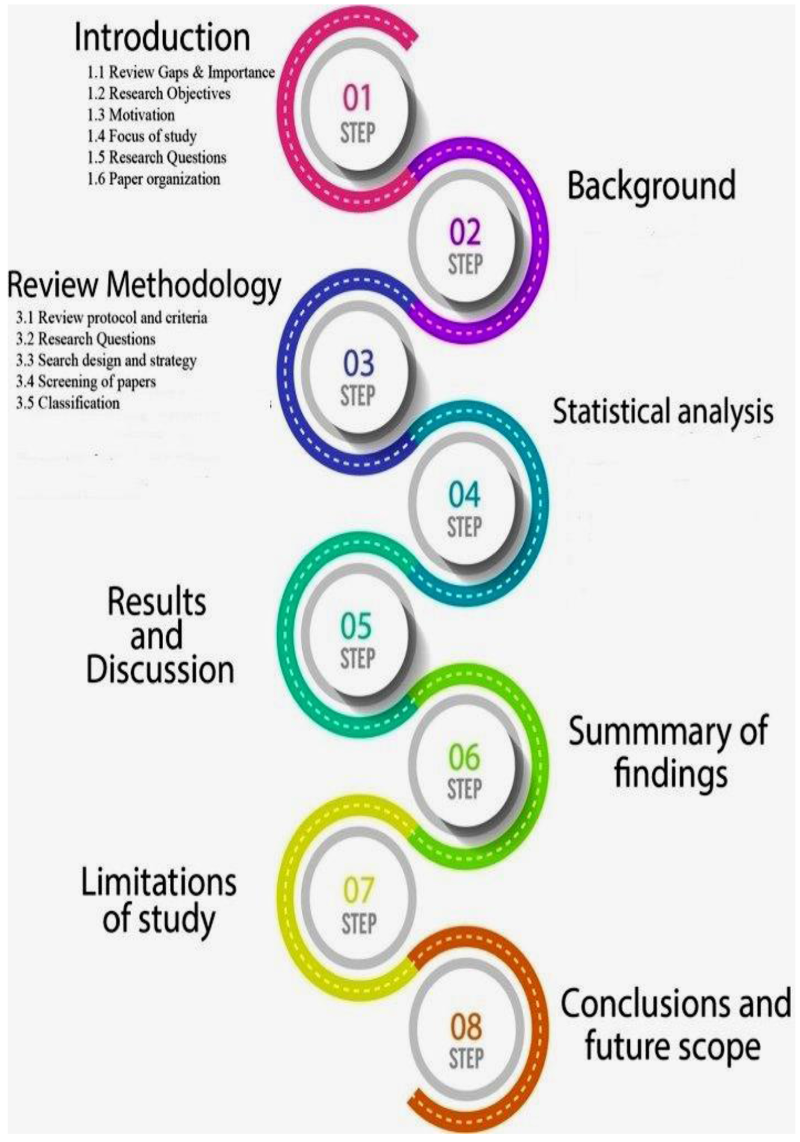
Roadmap for paper organization.
Segmentation refers to dividing a picture into specific regions of interest (ROIs) to facilitate the visualization and analysis of the data. The primary goal of segmentation is to identify the particular areas of the tumor to reduce a more accurate classification of brain tumors by altering the representation of the MR images.
The purpose of this is to distinguish between different areas of the tumor, such as necrotic and edema regions, and places that are not part of the tumor, namely white matter (WM) and gray matter (GM) [3], as shown in Figure 2.
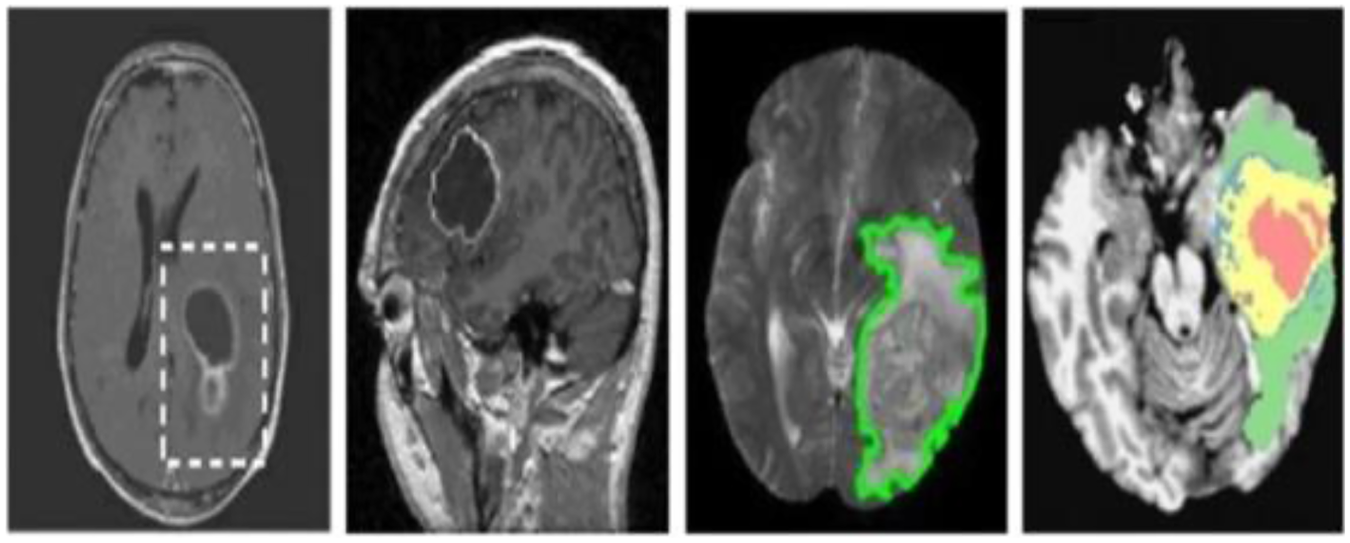
The BRATS 2013 database shows tumor segmentation subregions.
Several traditional methods for brain tumor segmentation have been employed, including contour and shape-based techniques, thresholding-based methods, edge and region-based algorithms, statistical-based approaches, and multi-resolution analysis. The review categorizes all other forms into three distinct groups: conventional/ML-based methods (traditional systems), DL-based methods (emergent method), and hybrid-based approaches (emerging techniques).
Several research have utilized machine-learning methods to divide brain tumors into segments. An algorithm-based network has been created to segment brain tumor MR images automatically. The classification of brain images as malignant or non-cancerous is performed using a support vector machine (SVM) classifier with different kernels. The suggested model’s performance has been evaluated using well-known datasets called Harvard and Rider. The experimental results indicate that the model successfully and efficiently accomplished the segmentation task [14]. A self-organizing map (SOM) clustering technique employed to segment brain lesions [15]. The model’s accuracy was forecasted to be 0.76%. A novel approach called Adaptive Fuzzy K-mean (AFKM) clustering was employed to categorize white matter (WM), cerebrospinal fluid (CSF) spaces, and gray matter (GM) in a comparison of Fuzzy C means (FCM) approaches. According to researchers, using the AFKM algorithm leads to significantly better outcomes than the FCM method, both in terms of quality and quantity [16, 17, 18].
Prior research predominantly concentrated on the technique based on machine learning. Machine learning methods are particularly well-suited for tackling the issues posed by large amounts of data, such as the segmentation of brain tumors. Nevertheless, specific machinelearning techniques rely on training images that have been manually segmented. However, manually segmenting the images is costly, time-consuming, and requires a group of skilled radiologists. Thus, machine learning (ML) often relies on human participation and intelligence [9], as conventional ML approaches utilize feature extraction techniques devised by humans to distinguish tumor traits and characteristics about imaging data [10].
DL-based methods
Deep learning approaches prevent the initial feature selection stage requirement as they can autonomously acquire suitable features for identification. Deep learning (DL) is a subset of machine learning (ML) that can autonomously discover significant characteristics, assess patterns, and classify data by extracting features at many levels [12]. Multiple deep-learning models and techniques are available for segmenting tumors using MRI data.
A Convolutional employed Neural Network (CNN) to carry out brain tumor segmentation tasks [19]. The testing findings demonstrate a dice score improvement of 0.88% and a reduction in segmentation time. A computerized brain tumor delineation system was developed using Convolutional Neural Networks (CNN) that achieved a dice score of 0.88% [20]. In a study conducted by researchers, they showcased a 3D-CNN model that achieved a Dice Similarity Coefficient (DSC) of 0.89% for the segmentation of brain lesions [21]. A brain tumor deep neural network (DNN) model, which operates automatically, was suggested for MRI scans [22]. An observed dice score of 0.72% was recorded. A tumor segmentation task is performed using a fully convolutional residual neural network (FCR-NN), achieving a dice score of 0.87% [23].
Furthermore, [24] utilized a DNN-based automatic segmentation method, achieving a dice score of 0.87%. Moreover, the author employed a Deep Neural Network (DNN), specifically a Fully Convolutional Network (FCN), to achieve pixel-level visual representation for tumor semantic segmentation. The investigation employed MRI scans of T1, T1c, T2, and Flair types. Consequently, the segmentation of tumor areas is enhanced with greater precision [25]. Although deep learning algorithms have demonstrated impressive benchmark results in brain tumor segmentation, they still have difficulty accurately automating this process. For example, there is a restricted ability to define visual objects and an inability to assess the spatial coherence and visual quality of segmentation outcomes [26, 27].
The current requirement is to develop an architecture for brain tumor segmentation that can accurately identify brain regions affected by tumors. This architecture should have a low memory requirement, perform computations quickly, and enhance the delineation of tumor boundaries. Consequently, there has been a movement in the study towards employing practical hybrid approaches.
Hybrid-based methods
The recent triumph of hybrid technology in the medical field exemplifies the keenness of researchers toward computer vision. Hybrid systems integrate multiple techniques to address the challenges of long computing time, low accuracy, and limited effectiveness. Convolutional Neural Networks (CNNs) can learn complex patterns directly from unprocessed image input. These models can extract hierarchical features from images in an automated manner, removing the requirement for manual feature engineering. The acquired features can subsequently be merged with manually generated features or clinical data utilizing conventional machine learning algorithms for categorization.
Brain tumor studies involve a wide range of study efforts focused on comprehending many elements of brain tumors, including their causes, categorization, and identification. The importance of this research lies in the profound influence that brain tumors have on patients’ well-being and the difficulties they provide to healthcare professionals. A comprehensive framework was proposed that utilizes SWT-CNN for brain tumor segmentation to improve the accuracy performance of CNN-based models [28]. The Stationary Wavelet Transform (SWT) strategy was utilized for feature extraction instead of the Fourier transform, as it yields enhanced outcomes for non-continuous data. Subsequently, the random forest (RF) method was employed for the classification work. The proposed methodology produces a 2% enhancement compared to the conventional CNN approach. Berkeley wavelet transform (BWT) combined with a support vector machine (SVM) architecture was introduced to perform tumor segmentation [29]. The feature extraction task utilized the Burrows-Wheeler Transform (BWT) and a Support Vector Machine (SVM) for the classification assignment. The author presents the following findings: an accuracy rate of 96.51%, a specificity rate of 94.2%, and a sensitivity rate of 97.72%. A different research publication employed the RF-SVM fusion approach for segmenting tumor lesions. The system consists of two stages: RF learns from tumor labels, and the resulting output is then used by SVM to categorize the labels [30]. A hybrid technique combining CNN and conditional random fields (CRFs) to achieve effective brain tumor segmentation. A dice score of 0.87% was attained [31]. A comprehensive overview of the advancements in brain tumor segmentation from 2013 to 2023. Based on an extensive survey, which analyzed over fifty segmentation methodologies from 2013 to 2023, we have identified the following key findings:
Numerous approaches and algorithms have recently been developed for brain tumor segmentation. Researchers used specific fusion/hybrid algorithms and some customized versions. The increased use of hybrid approaches is evident. Some researchers struggle to reach threshold performance with simple ML and DL algorithms. Ito et al. segmented brain tumors from MR images using semi-supervised deep learning [32]. Results have improved with this method. An automated Kernel-based FCM with weighted fuzzy kernel clustering was developed to improve brain image segmentation [33]. Results show the combined algorithm improves misclassification to less than 2.36%. CNN method was developed to segment tumors with 89% accuracy in deep learning [34]. The modified CNN model was used and model accuracy was increased to 90.98% [35]. Deep learning techniques have become practical tools for classifying brain tumors because they can automatically learn complex patterns from raw data, such as MRI images, without relying on manually designed features. These techniques utilize neural network structures, namely Convolutional Neural Networks (CNNs), to extract complex patterns and characteristics from image data directly. This results in enhanced accuracy and resilience in classification. Deep learning algorithms, particularly DCNN, have been top performers in recent years [19, 36, 37, 38]. DCNN’s key drawback is its need for enormous training data with professional radiologists’ comments from multiple institutions. The system was designed using prior information and artificial intelligence to improve brain tumor segmentation findings. SVM, FCM, and C-means are the most often used ML methods, whereas CNN and DCNN are the most commonly used DL methods. Two or more ML or DL approaches are used in hybrid ways. Kernel-based CNN with M-SVM deep learning algorithm was used for tumor segmentation with 0.85% dice score [39].
This study will design, execute, and describe the brain tumor recognition outcome analysis. The review protocol consists of five steps: (1) Review protocol and criteria, (2) Research Questions, (3) Search design and strategy, (4) Research paper screening and study filtering, and (5) Classification of brain tumor.
Review protocol and criteria
SLR concepts, philosophy, and measures were considered to create a thorough review methodology. Its primary topics are reviewing backdrop, research objectives, search strategy, data extraction, research study quality assessment standards, and data analysis. The review process distinguishes SLR from narrative literature review. Since researchers must explain the search technique and criteria for including or excluding studies in the review, it improves evaluation consistency and reduces biases. All connected steps in this process are shown in Figure 3.
Systematic review methodology.
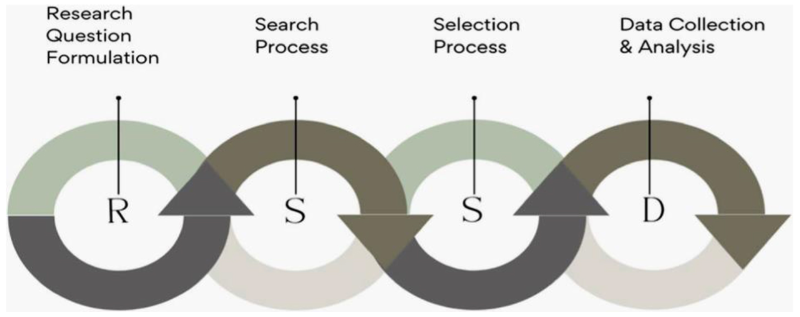
The first element of our review methodology involves the authors setting research questions linked to our study’s goals. These research questions are essential for extracting meaningful information from existing literature. The framework created by these research questions guides this review. When creating research questions, we use numerous methods to evaluate empirical information from studies on brain tumor recognition. This review covers 2013 to 2023. The complete process of related research questions and related answers is shown in Figure 4.
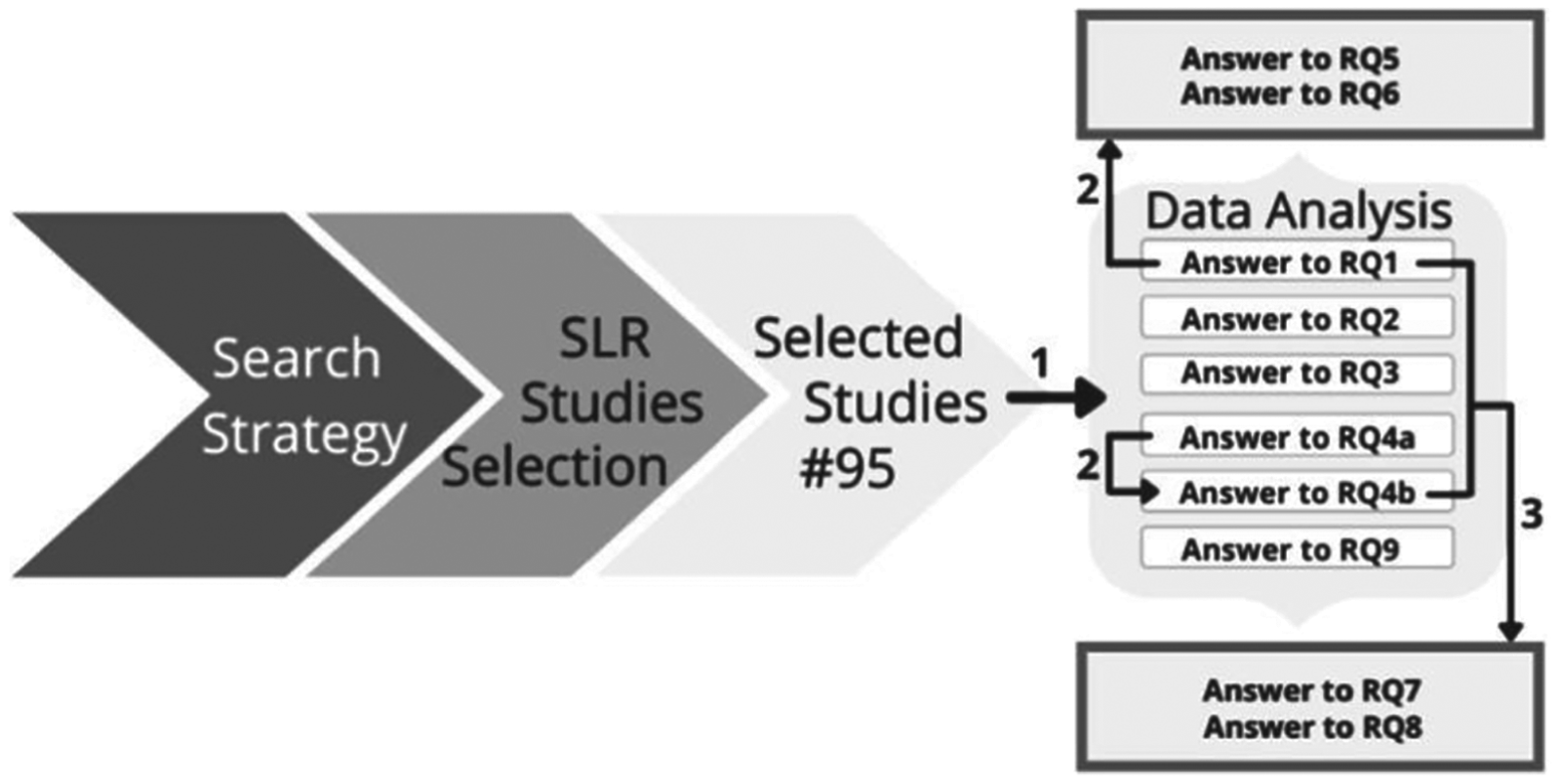
Designing research to address questions. Direct extraction is 1, indirect interpretation is 2, and synthesis-based indirect understanding is 3.
We illustrate our search method and selection procedure in Figure 3. It concentrates on research design to extract data from research questions to answer other questions. According to the authors, there are three types of extraction criteria: direct extraction, indirect interpretation, and synthesis-based indirect interpretation.
Direct extraction: It involved retrieving raw study data and processing. This criterion can answer fundamental research questions directly from the chosen study. Indirect interpretation: It uses prior questions’ information. This information is interpreted and used to answer research questions. These criteria are named because we want to make pre-fetched data more useful and valuable in our study. Answering one research question helps it formulate and answer others. Synthesis-based interpretation: The indirect interpretation criteria are extended by synthesis-based indirect interpretation.
Reading the paper and comparing the criteria to our research questions allows us to answer RQ1 directly. This is direct extraction. RQ5 and RQ6 can be answered using RQ1’s extracted information (focusing on process and sub process approaches). Interpreting RQ1’s response, which analyzes the recognition technique, answers these problems. Indirect synthesis-based interpretation can answer RQ7 and RQ8 by combining RQ1 and RQ4 data. Only the best method with appropriate accuracy is our goal here. Thus, the approach can answer RQ7 and RQ8.
What makes up a search strategy includes search phrases, literature sources, and the procedure itself. The writers culled important ideas and keywords for use in creating search strings. All relevant papers will be found simultaneously by using this search string. Next step of the SLR is to design a search value that will locate the most appropriate literature to address the research questions. Creating a search string and specifying search terms are necessary for searching for publications. To look for relevant research in an unbiased manner, iteratively developing a search string has proved useful. The next stage is finding digital-libraries and retrieving their data retrieval features to retrieve documents. The third step is to apply the study’s inclusion and exclusion criteria to the data [40].
Criteria for search
It is crucial to utilize precise keywords and refine the search queries to receive the most relevant results when searching for brain tumor classification and segmentation papers. Below are many relevant search terms, along with possible research papers:
Search Query: “Classification of brain tumors using deep learning” Search Query: “Brain tumor segmentation using convolutional neural networks.”
Search terms are created using these procedures [41]:
Extract critical terms from the Research questions mentioned in Table 2. Find synonyms and alternative spellings of essential phrases. Search the scientific literature for keywords. The search string will be per the above query and include synonyms and alternative spellings using OR and AND combinations. The authors used boolean OR and AND to build search strings after finding the relevant keywords.
Data was retrieved from digital databases for automatic searching: 1) IEEE-Explore, 2) ACM -Digital Library, 3) Science-Direct, 4) Springer, 5) Wiley Online Library, and 6) Scopus. The entire data retrieval process involved searching each digital library with the correct search term and retrieving relevant research and papers. After snowballing, retrieved studies are added to Mendeley, which helped this study find acceptable references. The 2013–2023 studies are examined.
Research paper screening and study filtering
When the search phrase is conducted on digital libraries, it retrieves a diverse range of studies from different databases. Screening papers involve identifying pertinent studies based on well-specified criteria and research issues. The initial filter is based on the year, specifically restricting research to those conducted in 2013 to 2023. The second filter eliminates redundant studies. Retrieving articles from major digital databases and Scopus leads to increased print redundancy. Scopus comprises most papers from IEEE-Explore, ACM, Springer, and Wiley. The process of eliminating duplication involves two criteria: “Exact Match,” which compares study titles to remove exact duplicates, and “Cross Checking,” which verifies authors, publication dates, and other bibliographic details to identify potential duplicates from different sources or with variations in title wording. The third filter is discarded upon reviewing the title. The search query will retrieve studies that contain the provided keywords.
Classification of brain tumor (2013–2023)
Classification places input features in categories/classes. Feature analysis and selection are crucial before CAD brain tumor categorization and detection. Reduce feature space redundancy with discriminating, suitable, and engaging feature sets to overcome the curse of dimensionality. Ground truth is needed for feature extraction from several MRI slices (axial, coronal, and sagittal planes).
Feature extraction
MRI scans are converted into characteristics for classification. Extracting unique traits is challenging. A lot of different methods are used for this, such as principal component analysis (PCA), spectral mixture analysis (SMA), texture features, Gabor features, nonparametric weighted and decision border feature extraction, wavelet transform feature extraction, discriminant analysis (DA), and more [42]. The most efficient CAD system recently uses DWT [43] to obtain wavelet coefficients at various levels.
Feature reduction further reduces data dimension. ICA, PCA, and LDA are used for this [44]. The combination of feature extraction and feature reduction created a CAD system that classifies images with clinically acceptable accuracy.
Researchers use filters, feature extraction, selection, or fusion to lower the range of MRI strength. The Gabor wavelet features method is used to get details about the texture of an MRI scan. By choosing only a few features, Kernel Principal Component Analysis (KPCA) cuts down on duplicates, and the Gaussian Radial Basis Function gives you the best information from any set [45]. Fine-tuning-based feature extraction is used by the pre-trained CNNs method [46].
Feature extraction and classification of tumors using ML, DL, and hybrid approaches
Tumor categorization classifies tumors as benign or malignant. Brain tumor classification is difficult due to tumor cell form, location, size, and contrast. The extraction of optimal classification features and choosing an appropriate classifier are essential to excellent classification. To select the best classifier, consider accuracy, processing resources, and algorithm performance.
The first step is to use unsupervised algorithms such as hierarchical clustering, FCM, K-mean clustering, SOM, etc., to group input patterns into related classes. Decision trees, support vector machines, linear discriminant analysis, k-nearest neighbors, Bayesian classifiers, and so on are all part of supervised classification [47]. Unsupervised multi-spectral data categorization identifies natural classes or groups. This categorization requires no prior information, recognizes classes as unique units, and reduces operator error [88].
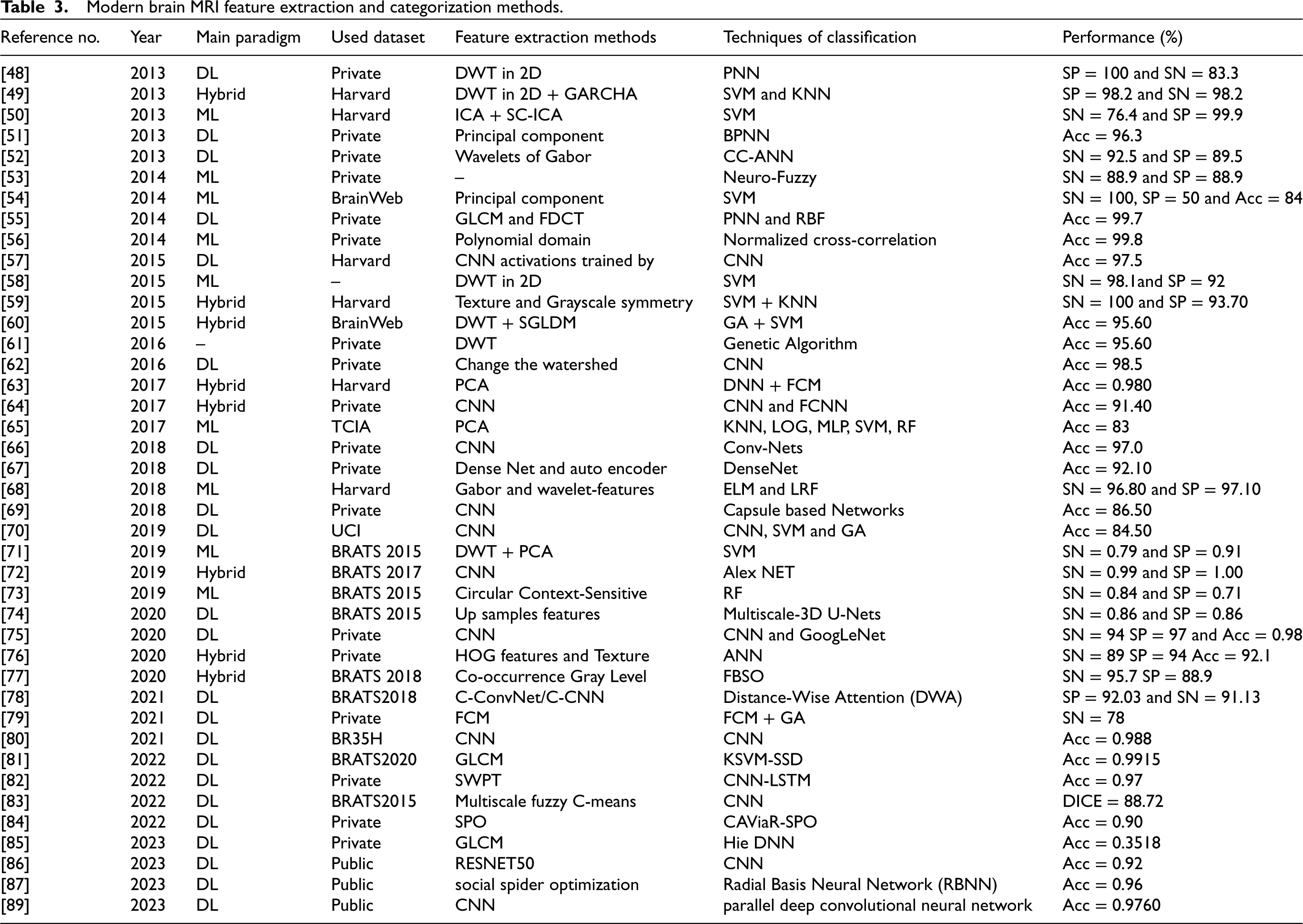
In supervised classification, known-identity samples classify unknown-identity samples. Supervised classification takes prior knowledge, tags the input dataset, and may discover substantial inaccuracies. Table 3 summarizes the 2013–2023 literature on MRI image feature extraction and classification methods.
The paradigm shift in segmentation approaches was also seen in brain tumor categorization. SVMs are used to classify tumors from MR scans [89]. Deep learning was used for classification over the decade. According to [90], segmentation algorithms like Dense CNN extract features and classify recurrent neural networks (RNNs). Most brain tumor DL-based classification algorithms use convolutional and fully connected networks [91].
Recently (20s), hybrid classification algorithms have become popular. Additionally, hybrid intelligent systems are used to design classifiers using soft computing. Neural networks and bio-inspired algorithms like genetic algorithms (GA) produce robust categorization systems in soft computing. A k-mean-FCM method was proposed [92]. MR brain images are denoised using a median filter, and features are extracted using a brain surface extractor. CNN-based Google-Net transfer learning-based classification model classifies glioma, meningioma, and pituitary brain cancers [93]. Multiclass SVM improved the algorithm’s accuracy from 92.3% to 97.8%. FCM, DWT, and DNN was used to classify tumors in 66 T2-W MRI scans [94]. The model classification rate was 96.97%.
CNNs excel in classification and prediction when pre-trained as feature extractors. The CNN
Many brain tumor classification CAD systems are inefficient due to excessive complexity, feature vector size, and generalization capabilities.
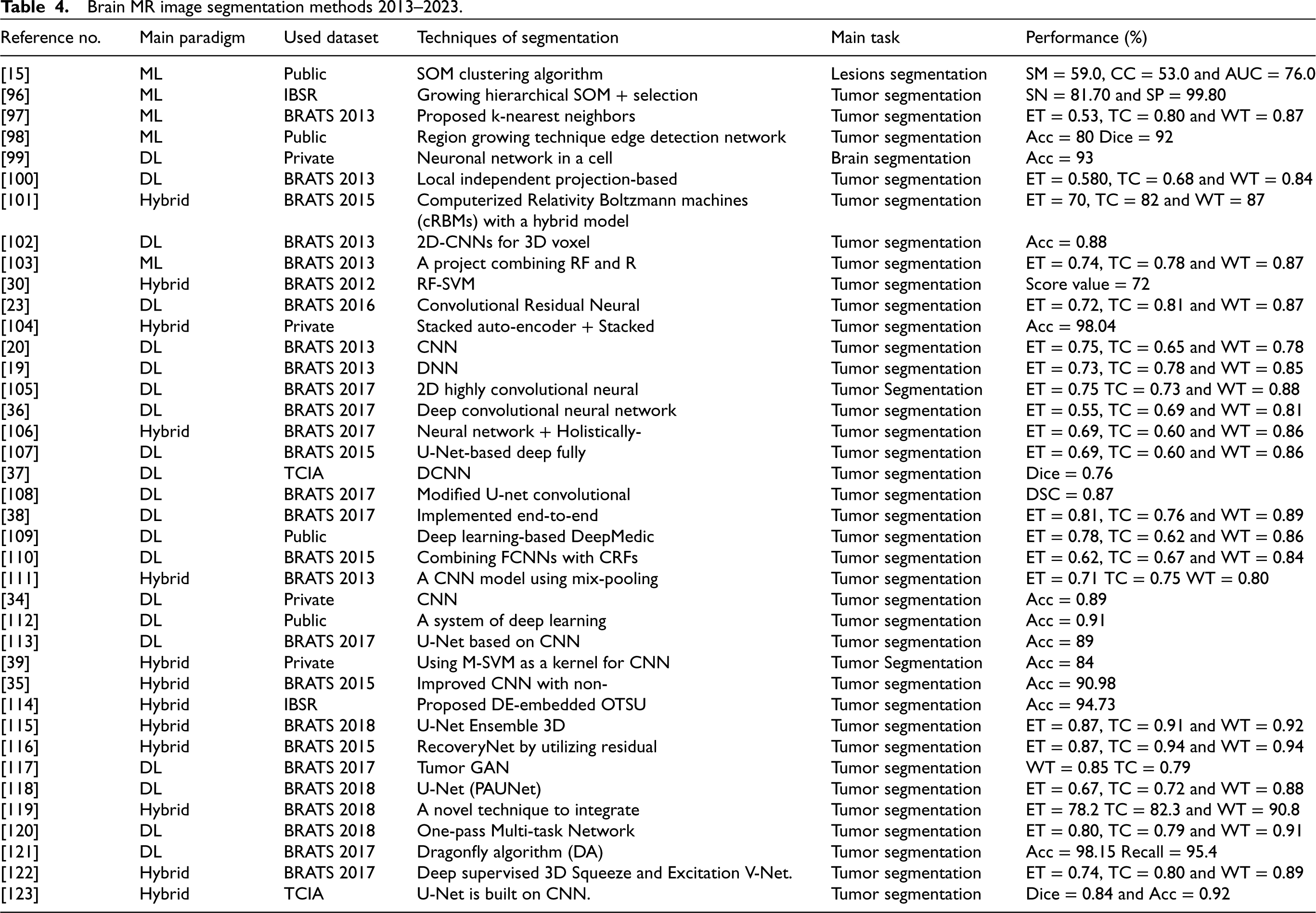
We think that correct classification comes from hybrid intelligent systems that use machine learning and other technologies. This appears to improve classification accuracy by 95%–100%. Table 4 below shows various segmentation methods since 2013 to 2023.
Tables 3 and 4 define key metrics as:
SM (Sensitivity): Sensitivity is a measure of how well a classifier identifies real positives; it is often called true positive rate or recall. Equation (1) can be used to compute it.
CC (Correlation Coefficient): The direction and magnitude of a linear relationship between two variables can be measured using this metric. In classification tasks, it can be used to assess the quality of predictions relative to the actual outcomes. AUC (Area Under the Curve): Model performance in binary classification problems is often measured by AUC. It’s the area under the receiver operating characteristic (ROC) curve, which compares true positive and false positive rates at different thresholds. SN (Specificity): True negative rate and specificity are terms that describe the percentage of real negatives that a classifier accurately identifies. Equation (2) can be used to compute it.
SP (Precision): A classifier’s precision is the fraction of its positive predictions that turn out to be correct for the given data. Equation (3) can be used to compute it.
ET (Execution Time): This term refers to the time taken by a system or algorithm to complete a task or process. It’s not directly a performance metric in the same sense as the others listed, but it’s often considered when evaluating the efficiency of a solution. It can be calculated as Eq. (4)
Dice Score: The Dice score is a metric commonly used in image segmentation tasks to quantify the similarity between two sets. It can be calculated as Eq. (3.5.2)
TC (True Classification Rate): The True Classification Rate (or Accuracy) is a measure of how many instances out of all are correctly classified. It can be calculated as Eq. (6)
DSC (Dice Similarity Coefficient): The Dice Similarity Coefficient, also known as Dice Score or F1 Score. It can be calculated as Eq. (7)
WM (White Matter): White Matter (WM) typically refers to a component of brain tissue. GM (Gray Matter): Gray Matter (GM) is another component of brain tissue. CSF (Cerebrospinal Fluid): The fluid that surrounds the spinal cord and brain is called cerebrospinal fluid (CSF). Modern brain MRI feature extraction and categorization methods. Brain MR image segmentation methods 2013–2023.







The main goal of this extensive section is to answer research questions.
Common MRI modalities
According to studies, MRI is the most common way to classify and divide up brain tumors [124]. This study emphasizes the standard MRI modality. T1-W is the most widely utilized MRI modality (18% of analyzed studies). Figure 5 shows the top of the MRI dataset used in this study.
Common usage datasets
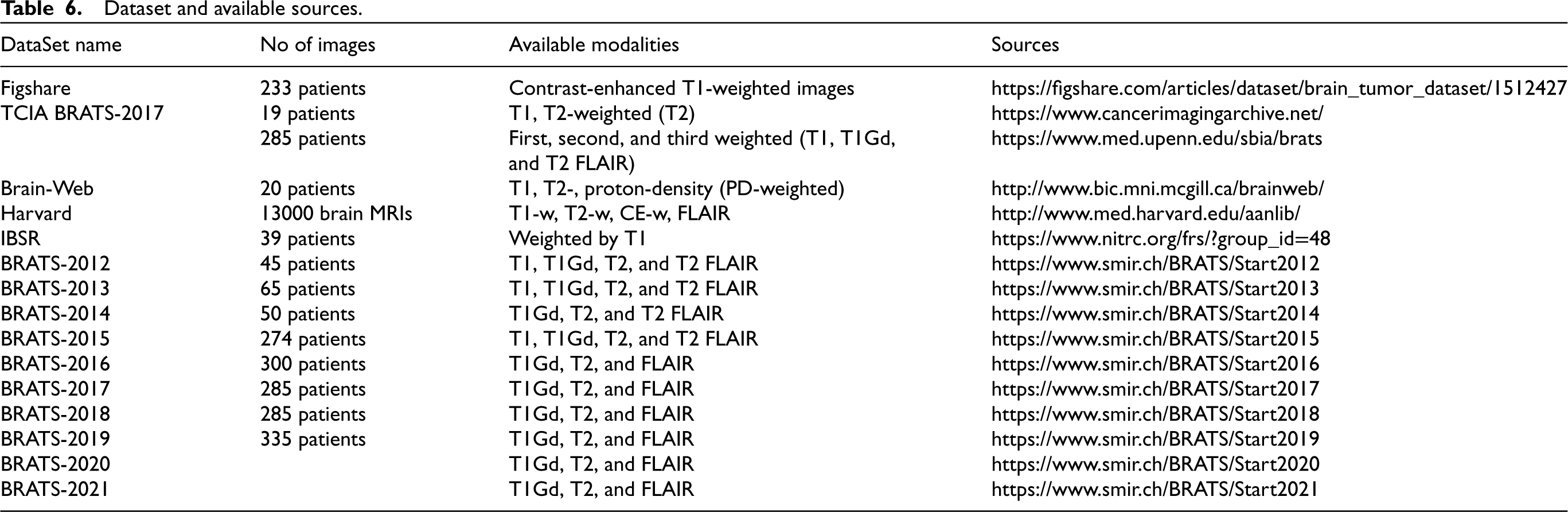
Brain tumor dataset acquisition is the primary objective. There are several publicly available resources for testing, including the Cancer Imaging Archive (TCIA), Oasis, BrainWeb, BRATS [125], Harvard, and others. 30% of the papers that were reviewed utilized BRATS data sets. Figure 6 shows that 25% of the articles evaluated were from the private dataset, putting it in second place. Before the sample BRATS dataset came out, researchers used private datasets from hospitals and labs in the area. Researchers continue to use the private dataset for model comparisons.
Publication statistics using classifiers
Using deep learning, it was possible to analyze brain tumor images in a realistic way [116]. Utilizing convolutional neural networks (CNNs) aids disease prediction by classifying, segmenting, and detecting brain tumors [20]. Many more CNN-based solutions (CNN merged with various architectures) were created between 2013 and 2023 [14, 126, 127, 128]. Retrospective analysis shows that methods based on convolutional neural networks (CNN) are superior at detecting brain cancers. Brain tumors are examined in this review employing 64 CNN and CNN-based designs (26%). With 39 articles, support vector machines (an ML method) comprise 16% of the current research. Figure 7 displays publishing data derived from classifiers. In Figure 7 other classifiers are based on ensembled and hybrid CNN, SVM, KNN, FCM, RF, K-means, DNN, ANN, UNET, and SOM.
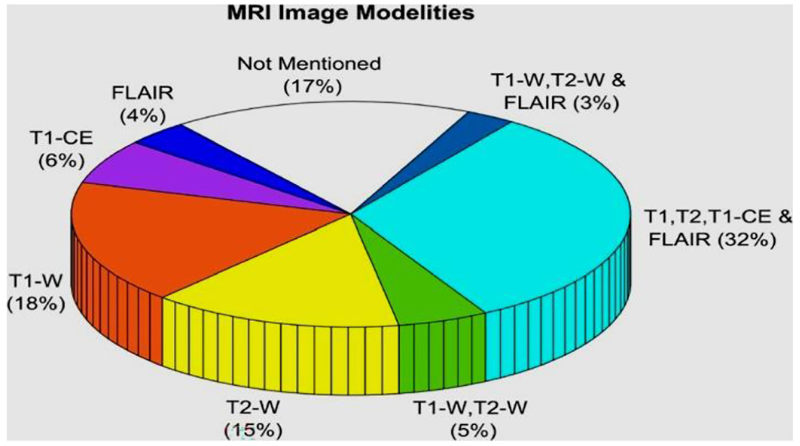
The current study analyzed common brain tumor MRI scan modalities (in %).
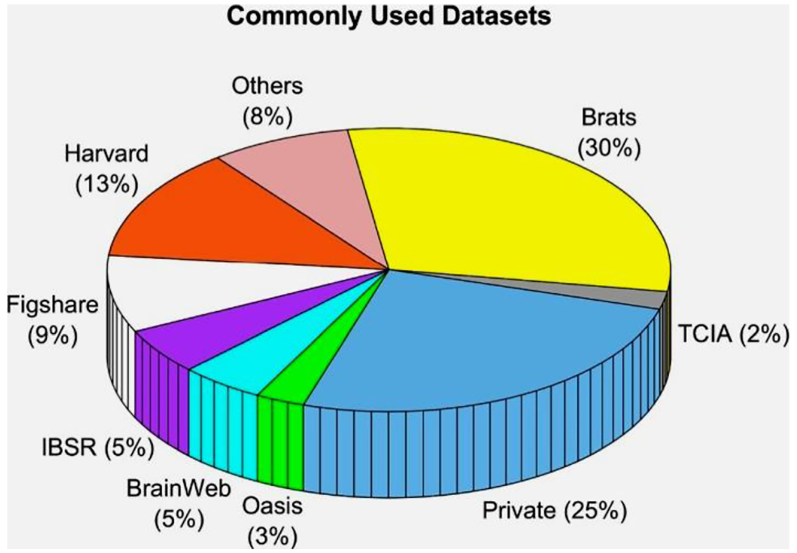
The most widely used database.
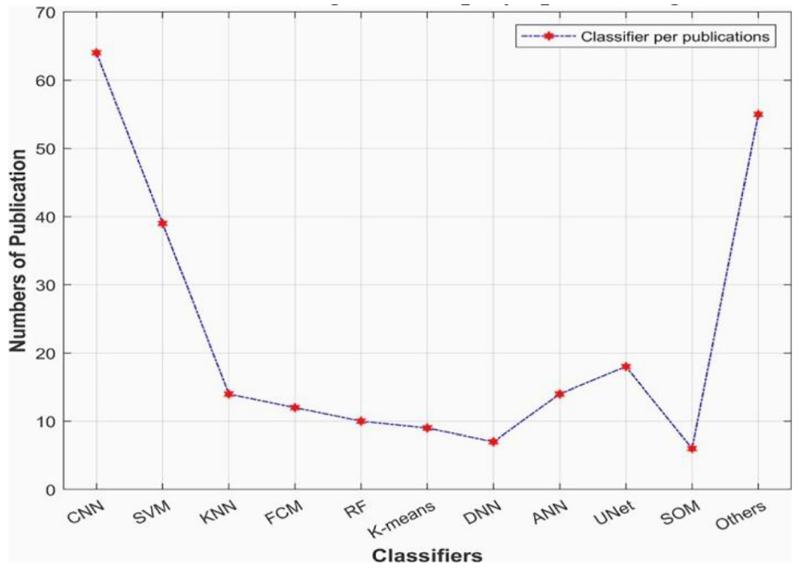
Statistics on publications using classifiers.
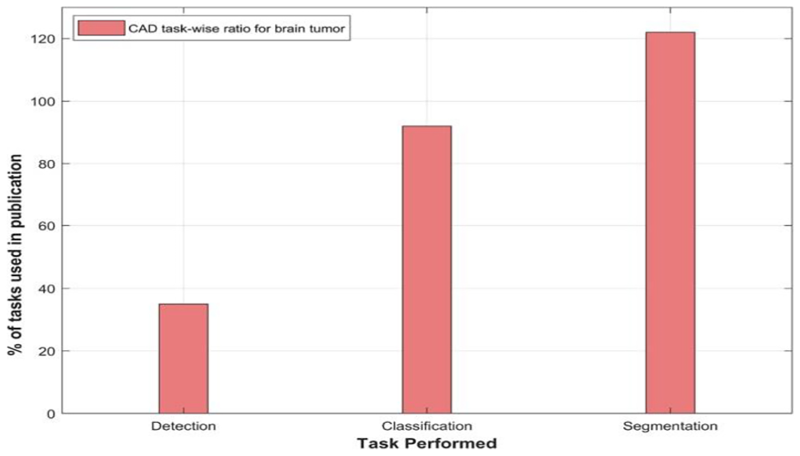
Primary CAD assignment (2013–2023).
Brain tumor segmentation has received the most amount of attention from researchers studying CAD issues throughout the past decade. As seen in Figure 8, categorization and detection rank second and third. Radiologists struggle to split tumors from MR images to classify them. More study on brain tumor segmentation helps radiologists and doctors diagnose brain tumors and subregions. Automated segmentation quickly distinguishes tumors from non-tumors.
Summarizing previous works
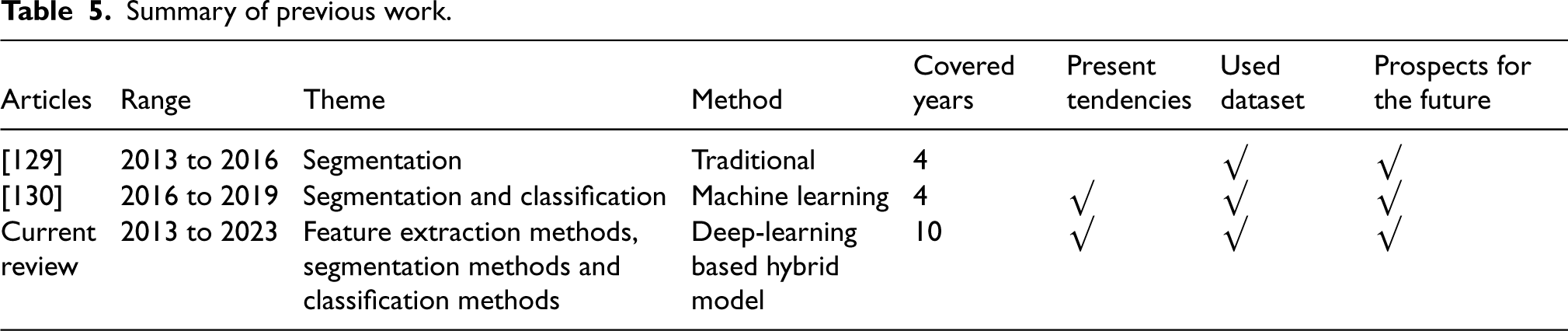
From 2013 until 2023, this study compiles all available reviews on brain tumor segmentation, classification, and detection. Most of the literature on brain tumor analysis employs conventional ML-based methods, as seen in Table 5. Deep learning and hybrid approaches are the main topics of this study’s comparison of ML-based methodologies. It demonstrates that the current review has addressed all survey constraints and gaps.
Summary of previous work.
Summary of previous work.
This section discusses the replies to the extracted research questions.
Accuracy Equation (8) defines Accuracy (Acc).

Precision Equation (9) defines Precision (Pre).

Recall Equation (10) defines Recall (Rec).

Dataset and available sources.
Mathematical equations and performance metrics table.
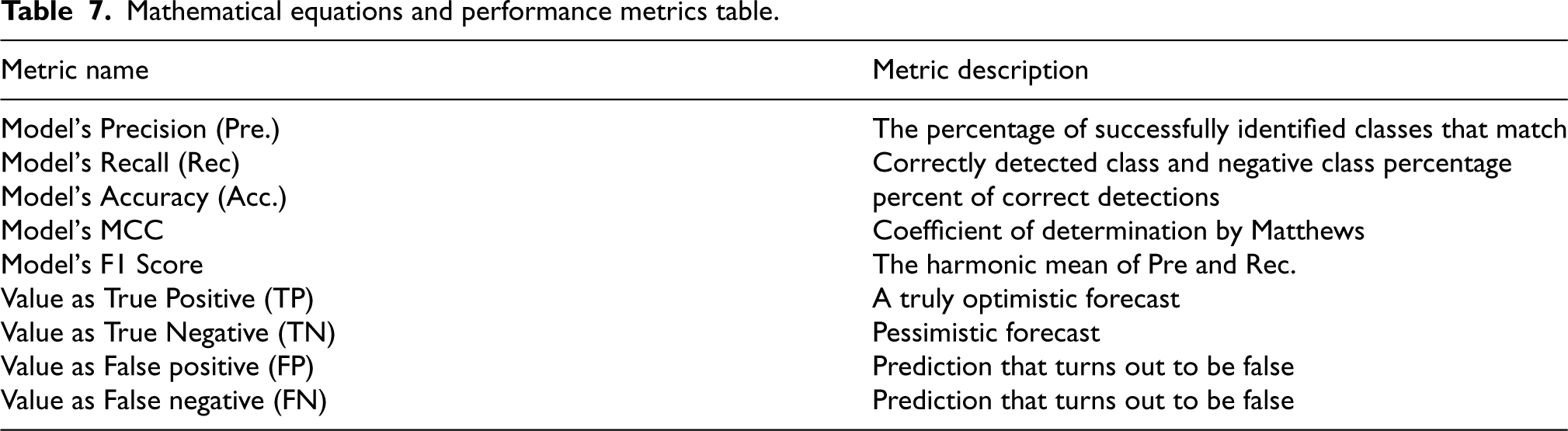
F1-Score Equation (11) defines F1-Score.


Picture segmentation, feature extraction, and classification heavily relied on traditional/machine learning techniques for diagnosing brain tumors between 2013 to 2023, algorithms based on deep learning replaced ML in medical image analysis, particularly in investigating brain tumors. Analysing Tables 4, 5 and 9 critically reveals that ML and DL-based algorithms achieve an accuracy rate of 75–95%. Using support vector machines (SVMs) [145], Divided 105 patients with high-grade gliomas (HGG) into groups with varying prognoses, including those with long-term and short-term symptoms. An 82% to 85% accuracy rate is achieved at the architectural stage [146]. Used a support vector machine classifier to analyse 235 patients’ histogram data in order to predict glioma patients’ survival rates. When looking at the overall survival prediction at six months, the sensitivity was 78%, the specificity was 81%, and at three years it was 0.85%, 85%, and 86% [147]. Provide evidence that machine learning can identify gliomas; with a specificity of 76.5–95% and a sensitivity of 78.0–93%, the results are in.
Nevertheless, hybrid approaches started to emerge in the 1920s. Hybrid methods utilizing deep learning or hybrid methodology are currently used in neuroimaging analysis pipelines. These techniques increase accuracy and efficiency in classification by 92% to 100%. When compared to bare models, survival prediction is improved when SVM is hybridized with a deep learning framework [148]. The novel conventional/Machine learning Deep Hybrid approach to analysing brain tumors was the subject of a comprehensive evaluation. There are other factors outside flawless ML, DL, and hybrid-based design/architecture that contribute to meaningful outcomes. By the end of this research study, readers will have a better idea of applying the highaccuracy architectural method to individual problems, such as detecting brain tumors. The results of this study demonstrated that deep learning and hybrid-based
Brain tumor MRI methods that combine hybrid techniques.
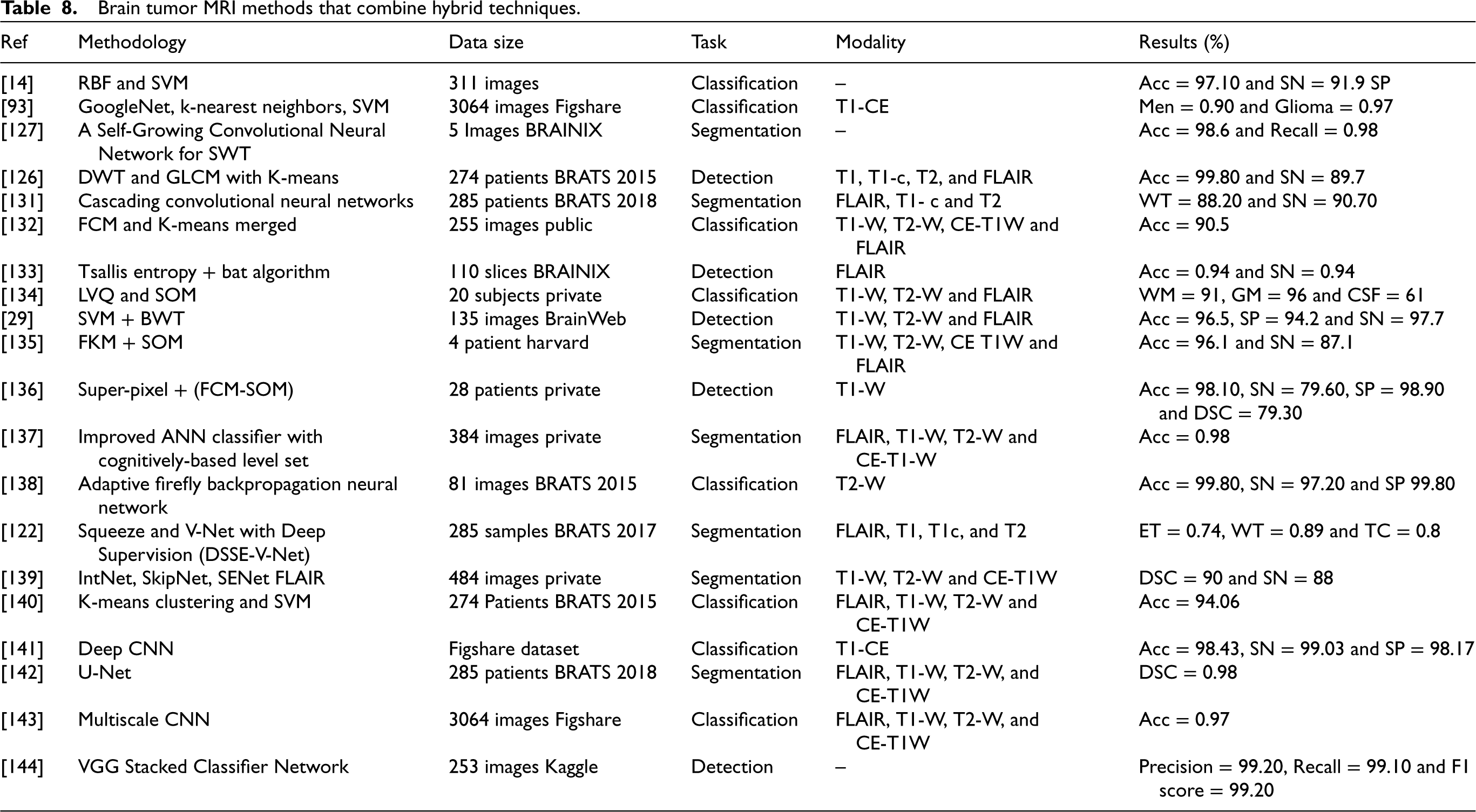
architectures are rivals when it comes to the classification and segmentation of brain tumors. If researchers find that ML or DL-based systems outperform hybrid systems, it could be because of trade-offs outside the network, including data augmentation or pre-processing normalization. To classify gliomas, 120 cases were evaluated [149]. Researchers achieved a 94% to 96% accuracy rate when classifying LGG and HGG using SVM and SMOTE. Even using the same network design, the outcomes of various BRATS challenges were drastically different. Adding framework layers can also improve accuracy [150, 151].
Compared to machine learning and deep learning, the results obtained from using hybrid architecture for specific task features are superior. Choosing the right system(s) and integrating them to get the desired results might be possible in the mixed-mode configuration. It is possible that the top augmentation and pre-processing methods were applied by researchers who produce strong performance with hybrid approaches. Improving a network’s generalizability without making structural changes is as easy as pie using this method.
Expert manual segmentation of brain tumors is necessary for radiotherapy treatment planning, but this process is time-consuming, complex, and delicate because doctors sometimes disagree on how to approach the problem best. Many algorithms and approaches for precise and automatic glioma segmentation have been proposed and developed since the 10s [152, 153]. Researchers gather annually for the BRATS (multi-modal brain tumor segmentation challenge) to solve this complicated problem [154, 155]. Most BRATS methods rely on 3D-CNNs and other deep learning architectures [156]. Ensembles of deep learning architectures or hybridization with evolving hybrid techniques like conditional random fields (CRFs) [159] are used by top-performing algorithms [157, 158]. Generic U-Net architecture with data augmentation and post-processing for brain tumor segmentation [161], cascaded networks [160], and multi-view and multiscale techniques [160] all did well in the BRATS 2017 and 2018 contests. Developing hybrid methods is a realistic way to improve rugged segmentation results.
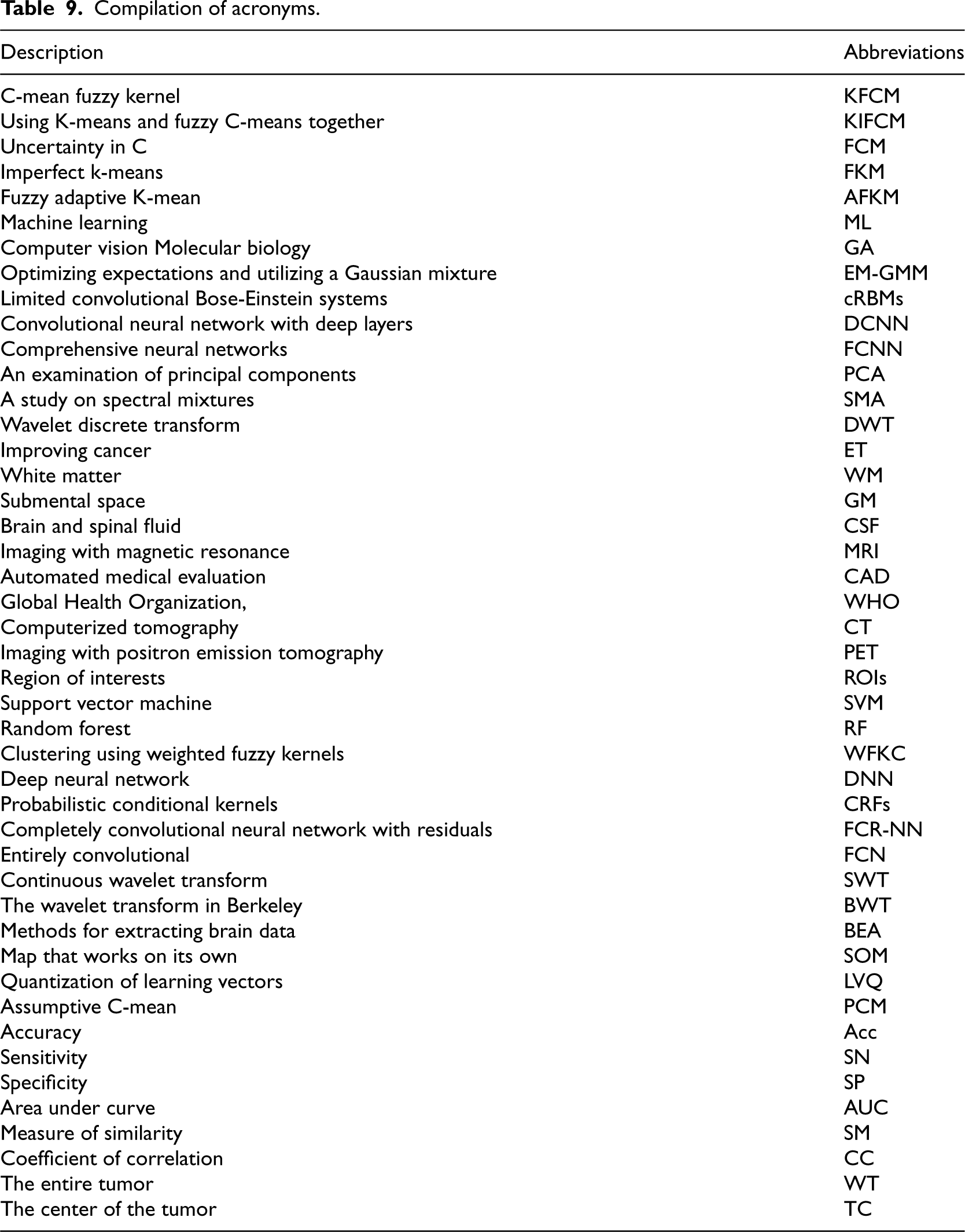
The compilation of various acronyms used to answer the above research questions is shown below in Table 9.
Compilation of acronyms.
Incorporate the research method, dataset, accuracy metric, and accuracy value into a database. Find the accuracy metric that is most often used. Compare accuracy values for identified metrics (step 2) across various ML approaches.
Moreover, 10% of other publications include theses, forums, meeting proceedings, technical reports, and symposiums.
Access to high-quality, well-annotated information is a significant barrier in brain tumor classification. Genetic mutations and histology vary widely in brain tumors. This heterogeneity makes tumor classification difficult and requires powerful machine-learning approaches that can capture complicated patterns. In many real-life situations, the spread of tumor subtypes may not be balanced, with some subtypes needing to be present more in the dataset. The classification of brain tumors generally uses MRI, CT, PET, and histological data.
The author meticulously examined and provided the findings of the systematic review analysis of the brain tumor recognition approach. Based on the guidelines in [162, 163], we searched the digital libraries of Scopus, IEEE-Explore, Science-Direct, Wiley, Springer, and ACM. Papers published between January 2013 and June 2023 are incorporated into this review.
In contrast to the study’s multi-faceted strategy, this review takes a systematic approach. The writers chose prospective studies from the pool of possible studies based on their suitability for answering the research questions. Citation counts were not a priority for the review writers, who strictly adhered to quality assessment ratings in their study selection process.
This research has not been comprehensive and systematic. The screening database collects, analyzes, and stores these investigations for reference. Few review studies have been done on brain tumor classification. We analyzed these reviews to summarize the topics. We could get a better direction before framing this investigation. It was also found that no systematic literature review study has been done on this challenging research subject. Thus, a new analysis is needed to fill the ten-year gap and provide a routine dimension to this topic’s investigation.
The purpose of this SLR is to summarize previous research on the issue and offer a variety of perspectives to current and future researchers so that they can better define and refine the field’s broad requirements. It also discusses methods and analyzes most metadata for the selected papers for review. Reviewers selected 169 studies for quality assessment. Quality assessment questions assess the relevance and quality score of these studies. These 169 publications appear in top journals, conferences, workshops, symposiums, technical reports, and thesis work.
The writers carefully examined all relevant factors to establish conclusions and answer research questions. Data from chosen studies is evaluated subjectively and quantitatively utilizing storytelling, vote counting, and grounded theory. The review categorizes studies by method.
This review study analyzes the trend of brain tumor segmentation and classification methods. The research topics focus on ML-based studies published between 2013 and 2023, but the SLR has also assessed non-ML or profound learning works. This systematic SLR has been different from all other review studies since 2013. To our knowledge, this is the first SLR in brain tumor classification research. This SLR achieves all criteria by determining researchers’ new priorities regarding recognition techniques, data sets, accuracy measures, methodology, and sub-techniques used in their studies.
Limitations of this study
This assessment examines recent brain tumor diagnosis research and suggests further progress. MRI scans are noisy during image capture, making noise removal difficult [20, 21, 22, 23]. Brain tumors include tentacles and scattered characteristics, making segmentation difficult [23, 24, 25]. Selecting and retrieving optimum parts and determining the right amount of training and testing samples are crucial to better categorization [26, 27]. Deep learning models are popular because they can automatically learn new features. These models require some memory and high dispensing control. Developing a lightweight computing framework that can yield a high ACC quickly is still essential. These are the primary brain tumor detection challenges. Glioma and stroke tumors contrast poorly. Tentacles and scattered parts make segmentation and categorization challenging [47]. A tiny tumor volume can be mistaken for a standard area, making detection challenging [29]. Some techniques work well for a complete tumor region but not for other areas (enhanced or not) [48, 49, 50].
The focus is limited to analyzing approaches and comparing their accuracy. There is much more to say about the research outcomes. Still, we tabulated and listed the study’s highlights and major conclusions to convey the findings.
Conclusion and future scope
This study analyzed strategies for segmenting brain tumors, extracting features, and classifying them from 2013 to 2023. Looking back ten years reveals the evolution of tumor segmentation and classification approaches based on artificial intelligence. It will be helpful for doctors and radiologists in the early detection and treatment of brain malignancies. Last but not least, researchers should build robust CAD systems using deep learning, ensemble, or hybrid-based methodologies, according to decades of statistical analysis.
According to future studies, the segmentation and classification of brain tumors may be better accomplished with few-shot learning and CNN. An advanced method called few-shot learning trains networks with fewer pictures. In every subject, obtaining large volumes of data annotated by experts from various universities is challenging. Brain tumor diagnosis and classification can also be accomplished using other medical modalities, such as CT.
Research into brain tumors using magnetic resonance imaging (MRI) has progressed over the last decade into a hybrid intelligent system that relies on networks and algorithms [19, 20, 38, 96, 98, 103, 116, 131]. The most straightforward approach to using strengths and weaknesses results in better performance in the CAD system. Despite their strength, accuracy, and popularity, conventional machine learning and deep learning approaches, notably CNNs, have many obstacles. It could be challenging to collect enough training data for each required domain. Accuracy in solving the goal problem might also be challenging [164]. An increase in deep learning model layers does not ensure a boost in classification accuracy. GPUs and RAM make DL models computationally expensive. Due to computing power constraints, network training takes longer, depending on dataset size. Thus, real-time clinical practice using DL models is unknown [165].
The BRATS competition provided researchers with many images and a platform to compare and assess brain tumor algorithms using pre-operative MRI scans for sub-region identification. The dataset grows annually. While ML and DL methods improved accuracy, hybrid approaches have replaced them in neuroimaging operations.
Deep learning is hindered by an extensive dataset’s need to train the framework, which demands more computing. However, gathering so much medical data is challenging. Many architectures have been developed to close this gap. Consider GAN [166]. The network needs little training data. Additional data boosts performance, no doubt. The dataset grows annually. More public datasets with expert labeling, like BRATS, may be created.
Data augmentation may also improve training datasets. Second, most DL-based systems suffer from spatial consistency and segmentation of visual objects [26, 27]. Thus, robust hybrid/fusion segmentation (a new learning-based technique) is recommended. Despite studies to overcome the problem, machine-learned and hand-crafted characteristics can improve hybrid brain tumor segmentation accuracy and efficiency [167, 168]. However, research advances this industry. Current brain tumor MRI segmentation and classification designs need to be more accurate, processing time, cost, extensive training data, and specialists for evaluation. Research is needed for excellent accuracy. A report compares SVM, KNN, LDA, and LR ML/DL accuracy. The algorithms are evaluated on 163 BRATS 2017 instances. The study indicated that LDA and CNN classifiers improve recognition [169]. Two or more algorithms that remove ambiguity in brain tumor segmentation and classification using brain MRI data can overcome all other ML and DL drawbacks.
Footnotes
Declarations
The authors assert that they have no conflicts of interest. There are no known conflicts of interest, whether they are related to finances.
Data availability
There is no accompanying data for this manuscript.