
Abstract
Subjective memory complaints (SMC) are required when diagnosing amnestic mild cognitive impairment (aMCI), although their relationship with objective memory performance and Alzheimer’s disease (AD) pathology remains unclear. We investigated whether the sex of the patient/participant moderates these associations. Participants were 940 normal control (NC) and aMCI participants from the Alzheimer’s Disease Neuroimaging Initiative. SMC were assessed via the memory scale of the Everyday Cognition questionnaire. Discrepancy scores were calculated between self- and informant-reports and categorized into “overestimates,” “comparable estimates”, and “underestimates” of SMC. We conducted linear and logistic regressions to examine the interaction of sex with self- and informant-reported SMC and discrepancy group on the Rey Auditory Verbal Learning Test (RAVLT) Immediate and Delayed Recall and on PET measures of amyloid-β (Aβ) positivity. Diagnosis-stratified analyses were also conducted. Overall, there were sex by self- and informant-reported SMC interactions for Immediate and Delayed Recall. Despite a higher proportion of “overestimates” in women, greater self- and informant-reported SMC showed a stronger relationship to poorer RAVLT scores in women versus men. Diagnosis-stratified analyses revealed that results were driven by aMCI participants. Conversely, overall, greater self- and informant-reported SMC related to greater odds of Aβ positivity regardless of sex. In diagnosis-stratified analyses, only informant-reported SMC related to Aβ positivity in aMCI. Relative to “comparable estimates,” “underestimates” of SMC were associated with poorer RAVLT scores across sexes in the overall sample and in aMCI. The predictive utility of self-report SMC may be limited to women in aMCI. Sex differences should be considered when evaluating SMC.
Keywords
INTRODUCTION
Individuals with amnestic mild cognitive impairment (aMCI) are particularly vulnerable to developing Alzheimer’s disease (AD) at a rate of 10 to 15% per year [1, 2]. Diagnostic criteria for aMCI typically include clinically-evident episodic memory impairment (usually defined as 1.5 standard deviations [SD] or more below normative means on memory tests), normal activities of daily living, a failure to meet dementia criteria, and subjective memory complaints (SMC), preferably verified by an informant [1, 3]. SMC are included in aMCI criteria because they are thought to reflect the initial effects of AD pathology on cognitive functioning that are often not detected using cross-sectional cognitive testing [4]. However, utility of SMC in diagnostic criteria is challenged by inconsistent associations between SMC and objective memory performance in MCI [5–8]. Individuals with MCI underestimate their memory decline suggesting that self-perception of cognitive ability decreases as AD advances [6, 10]. In cognitively normal older adults, the expected pattern of increases in SMC as memory performance decreases are often [7, 11], but not always observed [5, 9]. Thus, the accuracy of SMC is inconsistent across groups and, therefore, its clinical utility in predicting cognitive impairment is controversial. It would be informative to determine when SMC reflect actual performance and identify non-cognitive factors influencing SMC accuracy.
Previously-identified factors influencing SMC and their relationship to memory performance include depressive symptoms [6, 12] and personality factors (e.g., conscientiousness, neuroticism) [12, 13]. Few studies have examined the influence of sex on SMC despite significant sex differences in 1) rates of MCI [14, 15], 2) the MCI-to-AD trajectory [16, 17], 3) psychological symptom reporting [18–20], and 4) depression rates [21]. Prevalence rates of SMC have been reported to be higher in women than men [22, 23] but not consistently [24, 25]. However, the moderating role of sex on the relationship between SMC and memory performance has yet to be examined. Evidence suggests that because of the well-replicated female advantage in verbal memory [26], women have a more precipitous verbal memory decline in the normal-to-AD trajectory. For example, the relative decrease in Logical Memory scores between AD patients and controls is 1.6 times greater in women versus men [27]. Cognitive decline was estimated to be two times more precipitous in MCI women versus MCI men [16]. Moreover, women outperform men in verbal memory when AD biomarker burden (e.g., cortical amyloid-β (Aβ) burden) is low to moderate, but not severe [17, 29] suggesting a more accelerated verbal memory decline in women versus men. Findings raise the question of whether a more precipitous memory decline in women is more perceptible to the individual and others and, thus, whether SMC more accurately reflects memory performance in women than in men.
We examined how self- and informant-reported SMC and the discrepancy between them relate to memory performance and AD pathology (i.e., cortical Aβ deposition) in normal control (NC) and aMCI participants from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) and whether these relationships differ by sex. Because the ability of SMC to discriminate between NC and aMCI is questionable, primary analyses were conducted in the overall sample as well as within diagnostic groups. We hypothesized that greater self- and informant-reported SMC would relate more strongly to poorer verbal memory performance in women versus men, but would relate to greater amyloid deposition similarly in women and men. We hypothesized that results in the overall sample would be driven by the aMCI group whereby greater self- and informant-reported SMC would relate to poorer memory performance in aMCI women but not men. Conversely, greater SMC would be associated with poorer verbal memory performance similarly in NC women and men. We further hypothesized that underestimation of one’s memory performance relative to informant-report would be associated with poorer verbal memory performance in both women and men in the overall sample and this association would be driven by the aMCI group. In order to provide evidence that a more precipitous verbal memory decline in aMCI women versus men may underlie sex differences in SMC accuracy, we sought to support findings consistent with a more precipitous decline in women and determine specificity of findings to verbal memory. Specifically, we compared verbal memory for women and men at quintiles of Aβ deposition and hypothesized that the difference in memory from the highest to lowest quintile would be larger in women versus men. Lastly, we examined sex differences in the relationship between subjective and objective executive function performance and expected no differences in associations between men and women.
METHODS
Participants and data source
Data were obtained from ADNI (http://adni.loni.usc.edu). ADNI is a longitudinal, multi-site, cohort study that began in 2003 as a public-private partnership, led by Michael W. Weiner, MD. The broad aim of ADNI is to test whether neuroimaging markers, other biological markers, and clinical and neuropsychological assessment can be combined to measure the progression of MCI and early AD. Information about ADNI is provided at http://www.adni-info.org. ADNI was approved by the institutional review board at each site and written consent was obtained from all participants.
Our sample consisted of 940 ADNI-GO and ADNI-2 participants (393 NC, 547 aMCI). Participants represent a subsample of the larger ADNI population who had concurrent verbal memory testing and SMC. aMCI diagnostic criteria included MMSE score between 24 and 30, CDR of 0.5, SMC (preferably verified by an informant), and objective memory impairment as indicated by education-adjusted scores on the Wechsler Memory Scale Logical Memory II Delayed Recall (LM-Delayed), but no significant impairment in non-memory cognitive domains or interference in everyday activities [30]. Classification as NC required a MMSE score between 24 and 30, CDR of 0, no SMC beyond what one would expect for age, and memory scores on LM-Delayed above the cutoffs for memory impairment.
Neuropsychological outcomes
The Rey Auditory Verbal Learning Test (RAVLT) was used to assess verbal memory [31]. This is a serial word list-learning test that involves reading aloud 15 words and immediately instructing the participant to recall as many words as possible for five successive trials (Immediate Recall score, range: 0–75). A distractor list is read aloud once, followed by free recall of the initial 15 words. Following a 30-min delay, free recall of the original word list is obtained (Delayed Recall score, range: 0–15). The Immediate and Delayed Recall scores were our primary outcomes. In exploratory analysis that tested the specificity of findings to the verbal memory domain, the Trail Making Test (TMT) part B [32] was used to assess executive function (e.g., mental flexibility, set-shifting). The participant is presented with a sheet of paper with randomly-placed circled numbers and letters and instructed to draw a line alternating between numbers and letters in numerical and alphabetical order as quickly as possible. The outcome measure was time to completion. Raw scores on the RAVLT and TMT were converted into education-adjusted, standardized z-scores based on means and SD of the NC group.
Subjective cognitive complaints
Subjective cognitive complaints were assessed via ECog, a 39-item questionnaire with 6 subscales (everyday memory, language, visuospatial abilities, planning, organization, divided attention) [33]. Questions assess an individual’s daily cognitive function relative to years prior according to the following scale: 1 = no change/performs better than 10 years ago; 2 = occasionally performs the task worse than 10 years ago; 3 = consistently performs the task a little worse than 10 years ago; 4 = performs the task much worse than 10 years ago; 5 = do not know (treated as missing). Higher scores reflect greater cognitive decline. We used the memory subscale (eight items) in primary analyses, and secondary analyses used the organization subscale to reflect executive function complaints.
Participants and study-partners (informants) individually completed the questionnaire. Discrepancy scores between self and informant reports were calculated by subtracting the informant’s subscale score from the participant’s subscale score. A positive discrepancy score denotes overestimation of one’s cognitive decline relative to their informant, whereas a negative score denotes underestimation of one’s cognitive decline relative to their informant. The ECog questionnaire has been validated in MCI and AD samples [33].
AD biomarker
Levels of cortical Aβ plaque deposition were available for a subset (n = 823) and were measured by [18F]AV45 (florbetapir) positron emission tomography (18F-AV45 PET) as described at http://www.adni-info.org. Mean florbetapir uptake was measured within four regions (frontal, anterior/posterior cingulate, lateral parietal, lateral temporal) and standardized uptake value ratios (SUVRs) were calculated by averaging across cortical regions and dividing by the whole cerebellum. Participants were dichotomized into Aβ positive and negative groups based on a previously-established SUVR threshold of 1.11 [34].
Procedure
Participants’ “screening” visit included administration of the MMSE, the Clinical Dementia Rating Scale (CDR), and the Geriatric Depression Scale (GDS). Participants’ “baseline” visit occurred ∼28 days after “screening” and included administration of the neuropsychological tests, ECog questionnaire, and [18F]AV45 PET.
Statistical analyses
All analyses were conducted in the overall sample and within diagnostic group. Differences in RAVLT scores, ECog scores, and Aβ positivity between sexes were examined using analyses of variance/analyses of covariance (ANOVA/ANCOVA). Correlational analyses were used to examine the relationship between self-reported ECog memory and GDS scores separately in women and in men. We conducted linear regressions to examine the independent effects of ECog memory outcomes (i.e., self- and informant-reported ECog memory scores and discrepancy group) and their interactive effects with sex on RAVLT Immediate and Delayed Recall z-scores adjusting for age, education, ApoE genotype, and diagnosis (overall sample only). Because the data indicated a non-linear relationship between discrepancy and RAVLT scores, the distribution of discrepancy scores were categorized into equally-sized tertiles in the overall sample that represented those who, relative to their informant, either: 1) underestimated their memory decline (scores <0.0), 2) had comparable memory decline estimates (scores = 0.0–0.5), and 3) overestimated their memory decline (scores >0.5). The under- and overestimate groups were compared to the reference group of comparable estimates in regressions. Sex-stratified analyses were conducted if the interaction term was significant at p < 0.10. Interaction terms at p≥0.10 were removed from the model. We conducted logistic regressions to examine the independent effects of ECog memory outcomes (i.e., self- and informant-reported ECog memory scores and discrepancy group) and their interactive effects with sex on Aβ positivity.
To demonstrate evidence of a more precipitous memory decline in women versus men, we created sex-specific quintiles of [18F]AV45 SUVR. Sex differences in RAVLT means were examined at each SUVR quintile using ANOVA. We ran linear regressions to examine the interactive effects of sex by SUVR quintile on RAVLT scores with the quintile variable treated as continuous (range: 0–5).
We repeated linear regressions using subjective and objective scores for executive function (TMT part B). Among the ECog subscale scores reflecting complaints in executive function, ECog organization showed the strongest correlation with TMT part B (r = 0.19, p < 0.001) and, thus, were used in analyses. The distribution of organization discrepancy scores were categorized into equally-sized tertiles in the overall sample that represented those who, relative to their informant, either: 1) underestimated their organization decline (scores <0.0), 2) had comparable memory decline estimates (scores = 0.0–0.17), and 3) overestimated their memory decline (scores >0.17). Linear regressions adjusting for age, education and ApoE genotype and diagnosis (overall sample only) examined the independent effects of ECog organization outcomes (self- and informant-reported ECog organization scores and discrepancy group) and their interactive effects with sex on TMT part B scores. Analyses were performed using SPSS 24 (SPSS Inc., Chicago, Illinois); significance defined as p≤0.05 (two-sided).
RESULTS
Sample characteristics
In the overall sample (n = 940), women were younger, less educated, less likely to be white, and reported more depressive symptoms than men (ps < 0.05; Table 1). Men had a higher proportion of individuals with aMCI (p = 0.001) and lower MMSE scores (p = 0.03). As expected, the female verbal memory advantage was evident for RAVLT Immediate and Delayed Recall (ps≤0.001); however, SUVR and rates of Aβ positivity were similar between women and men (ps > 0.05).
Sample characteristics by sex
Differences in sample characteristics between sexes were examined using analyses of variance/analyses of covariance (ANOVA/ANCOVA) for continuous variables and chi-square tests for categorical variables. aMCI, amnestic mild cognitive impairment; AD, Alzheimer’s disease; GDS, Geriatric Depression Scale; MMSE, Mini-Mental State Exam; RAVLT, Rey Auditory Verbal Learning Test; SMC, subjective memory complaint; SUVR, standardized uptake value ratio; Aβ, amyloid-β.
In diagnosis-stratified analyses, women were younger and less educated than men in both NC and aMCI groups (ps < 0.05; Table 2). Women were less likely to be white than men in the aMCI (p < 0.01), but not NC group. The female verbal memory advantage was evident for RAVLT Immediate and Delayed Recall (ps≤0.001) in both groups. Consistent with previous studies [29, 35], SUVR and the prevalence of Aβ positivity was higher in NC women versus men (ps = 0.006), but were similar in aMCI men and women (ps > 0.05).
Sample characteristics by sex and diagnostic group
Differences in sample characteristics between sexes were examined using analyses of variance/analyses of covariance (ANOVA/ANCOVA) for continuous variables and chi-square tests for categorical variables. NC, normal controls; aMCI, amnestic mild cognitive impairment; AD, Alzheimer’s disease; GDS, Geriatric Depression Scale; MMSE, Mini-Mental State Exam; RAVLT, Rey Auditory Verbal Learning Test; SMC, subjective memory complaint; CDR, Clinical Dementia Rating; SUVR, standardized uptake value ratio; Aβ, amyloid-β.
Sex differences in SMC
Overall sample
Mean self-reported ECog memory scores did not differ by sex (Table 1). Informant-reported ECog memory scores were higher in men versus women (p < 0.001), whereas discrepancy scores were higher in women versus men (p < 0.001). The proportion of individuals that overestimated their memory decline relative to informants was higher in women versus men (p = 0.005), whereas the proportion of individuals that underestimated was higher in men versus women (p = 0.002). Regardless of the limited GDS range in the ADNI sample (GDS > 6 were excluded), higher GDS scores were associated with higher self-reported ECog memory scores in both men (r = 0.37, p < 0.001) and women (r = 0.32, p < 0.001). GDS scores did not correlate with RAVLT Immediate (r = –0.05, p = 0.22) or Delayed (r = –0.05, p = 0.23) Recall and, thus, were not adjusted for in regressions.
Diagnostic groups
Within the NC group, mean self- and informant-reported ECog memory scores, mean discrepancy scores, and the proportion of those who over- and underestimate their memory decline (relative to informants) did not differ between men and women (Table 2). Within the aMCI group, self-report ECog memory scores did not differ between men and women; however, informant-reported ECog memory scores were higher in men versus women (p = 0.02). Conversely, mean discrepancy scores were higher in aMCI women versus aMCI men (p = 0.007). Relative to informant-report, the proportion of aMCI individuals that overestimated their memory decline was higher in women versus men (p = 0.005), whereas the proportion of individuals who underestimated their memory decline was higher in men versus women (p = 0.03). GDS scores were similarly associated with self-reported ECog memory scores in men and women in the NC (Women: r = 0.21, p = 0.04; Men: r = 0.26, p = 0.01) and aMCI (Women: r = 0.20, p < 0.001; Men: r = 0.25, p < 0.001) groups.
Sex differences in relationship between SMC and verbal memory performance
Overall sample
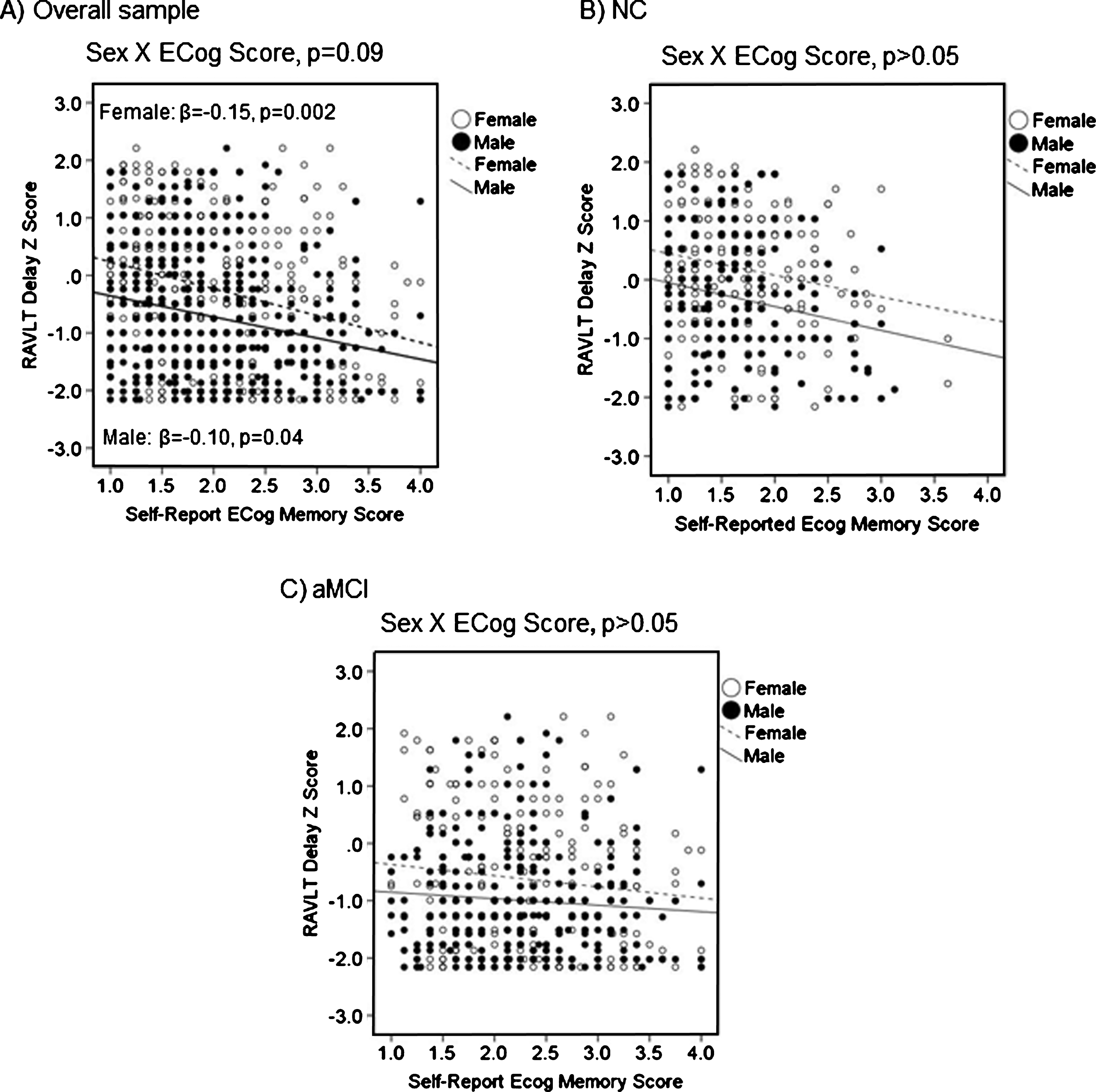
Our hypothesis that the relationship between SMC scores and memory performance would be stronger in women was supported by a sex by self-reported ECog memory scores interaction that was significant for Immediate Recall (B = 0.20, β= 0.19, SE = 0.10, p = 0.04) and a trend for Delayed Recall (B = 0.16, β= 0.16, SE = 0.10, p = 0.09). The association between self-reported ECog memory scores and RAVLT scores was either only significant in women (Immediate Recall; Fig. 1A) or was significant in both sexes but stronger in women (Delayed Recall) as reflected in steeper slopes for women versus men in Fig. 2A. The sex by informant-reported ECog memory scores interaction was significant for both Immediate (B = 0.17, β= 0.16, SE = 0.09, p = 0.04) and Delayed Recall (B = 0.19, β= 0.19, SE = 0.08, p = 0.03). The associations between informant-reported ECog memory scores and RAVLT scores were stronger in women versus men (Immediate Recall: Fig. 3A; Delayed Recall: Fig. 4A). All significant sex by self- or informant-reported ECog memory score interactions were of a moderate and clinically-meaningful effect size according to effect size heuristic for standardized beta coefficients [36]. There were no sex by discrepancy group interactions for RAVLT scores (ps > 0.05; Table 3). Regardless of sex, under- or overestimation of one’s memory decline relative to informant was not associated with Immediate Recall (ps > 0.05); however, underestimation, but not overestimation, was associated with poorer Delayed Recall (p = 0.02).

Self-reported ECog memory scores as a function of sex and RAVLT Immediate Recall in (A) the overall sample, (B) NC, and (C) aMCI. RAVLT, Rey Auditory Verbal Learning Test; β, sex-specific standardized regression coefficient of the relationship between self-reported ECog memory scores and RAVLT scores controlling for age, education, ApoE4, and diagnostic group (overall sample only).
Self-reported ECog memory scores as a function of sex and RAVLT Delayed Recall in (A) the overall sample, (B) NC, and (C) aMCI. RAVLT, Rey Auditory Verbal Learning Test; β, sex-specific standardized regression coefficient of the relationship between self-reported ECog memory scores and RAVLT scores controlling for age, education, ApoE4, and diagnostic group (overall sample only).
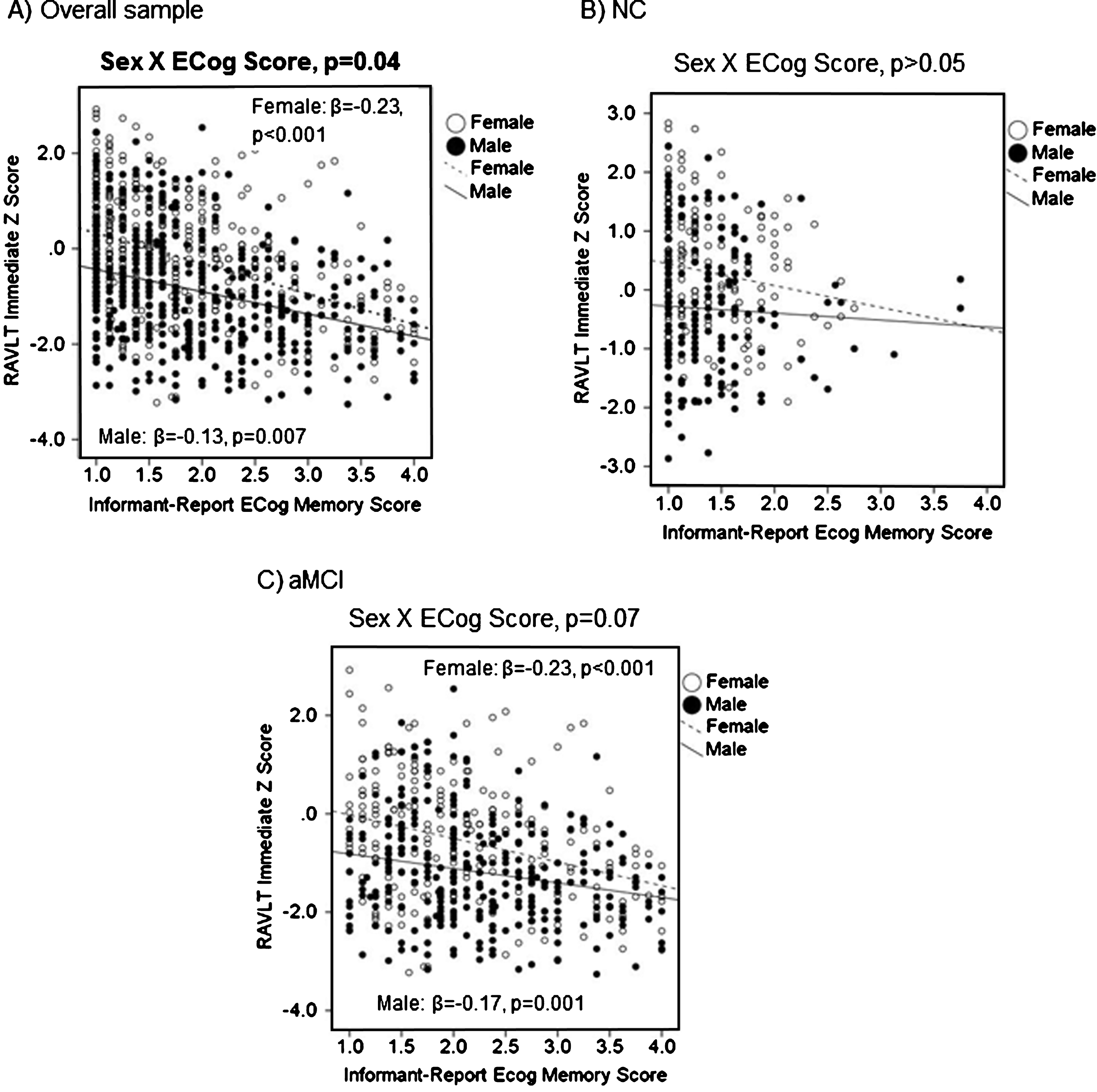
Informant-reported Ecog memory scores as a function of sex and RAVLT Immediate Recall in (A) in the overall sample, (B) NC, and (C) aMCI.. RAVLT, Rey Auditory Verbal Learning Test; β, sex-specific standardized regression coefficient of the relationship between self-reported ECog memory scores and RAVLT scores controlling for age, education, ApoE4, and overall sample.
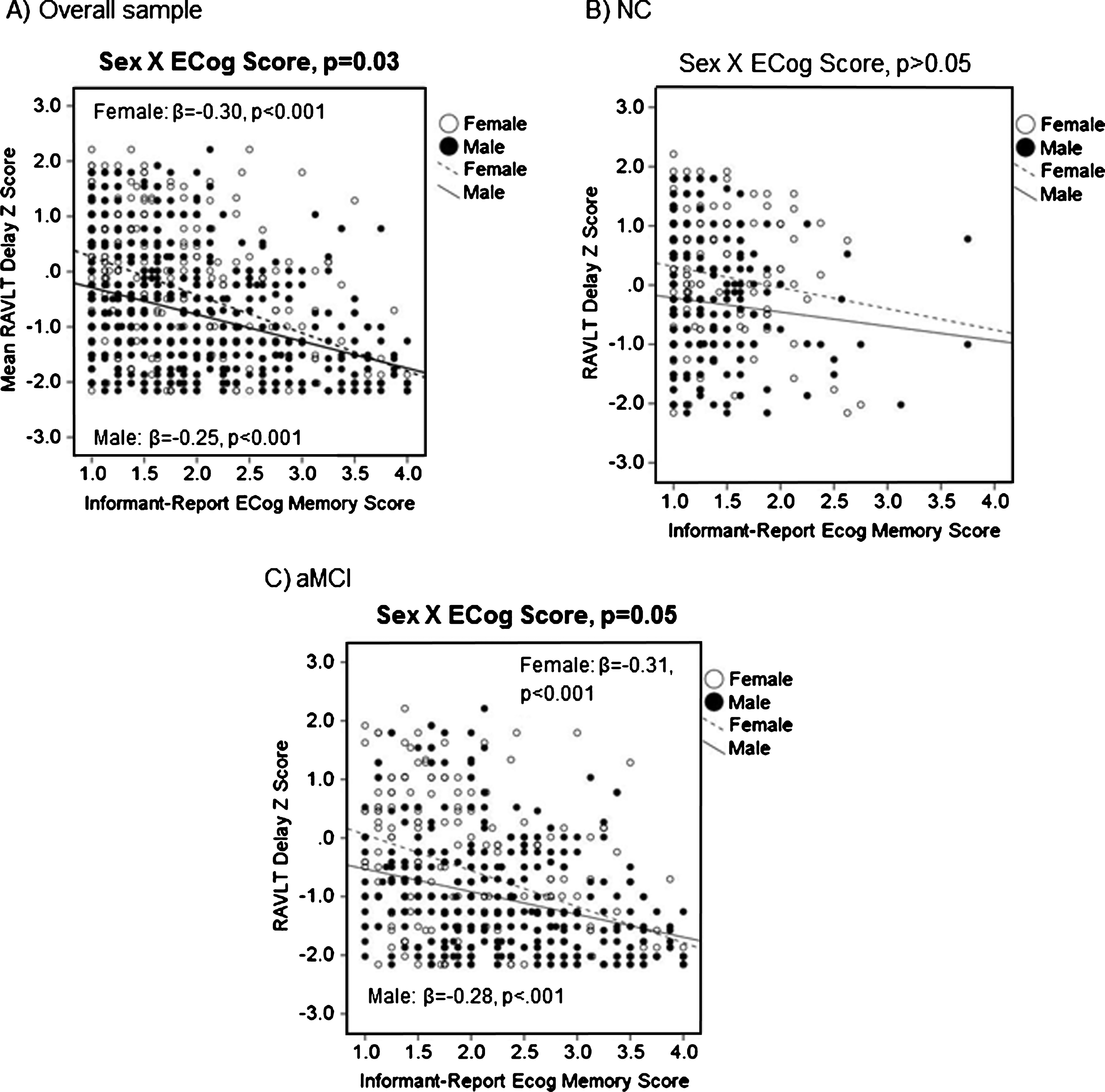
Informant-reported Ecog memory scores as a function of sex and RAVLT Delayed Recall in (A) in the overall sample, (B) NC, and (C) aMCI.. The interactive effect of sex x informant-reported ECog memory scores was significant for both RAVLT Immediate and Delayed Recall (ps<0.05). RAVLT, Rey Auditory Verbal Learning Test; β, sex-specific standardized regression coefficient of the relationship between self-reported ECog memory scores and RAVLT scores controlling for age, education, ApoE4, and diagnosis (overall sample only).
Results of multivariable linear regression analyses modeling the independent effect of under- or overestimation of one’s memory decline (relative to informant) and their interactive effects with sex on RAVLT scores
All analyses were adjusted for age, education, ApoE status and diagnosis (overall sample only). B, unstandardized regression coefficient; β, standardized regression coefficient; SE, standard error; NC, normal controls; aMCI, amnestic mild cognitive impairment; RAVLT, Rey Auditory Verbal Learning Test.
Diagnostic groups
In the NC group, there were no interactive effects between sex and self- or informant-reported ECog memory score or discrepancy group on Immediate or Delayed Recall (ps > 0.05). Regardless of sex, higher self-reported ECog memory scores were associated with poorer Immediate (B = –0.24, β=–0.11, SE = 0.10, p = 0.01; Fig. 1B) and Delayed (B = –0.38, β=–0.18, SE = 0.10, p < 0.001; Fig. 2B) Recall and higher informant-reported ECog memory scores were associated with poorer Delayed Recall (B = –0.27, β=–0.11, SE = 0.12, p = 0.02; Fig. 4B); trend for Immediate Recall (B = –0.20, β=–0.08, SE = 0.12, p = 0.09; Fig. 3B). There were no associations between under- or overestimation of one’s memory decline (relative to informant) and RAVLT scores in the NC group (ps > 0.05).
In the aMCI group, there was a sex by self-reported ECog memory score interaction for Immediate Recall (B = 0.30, β= 0.31, SE = 0.13, p = 0.02; Fig. 1C), but not for Delayed Recall (p = 0.24; Fig. 2C). Higher self-reported ECog memory scores were associated with poorer Immediate Recall in aMCI women (B = –0.22, β= –0.12, SE = 0.11, p = 0.04) but not in aMCI men (p = 0.55). Regardless of sex, there was no association between self-reported ECog memory scores and Delayed Recall in aMCI (p = 0.32). There was a sex by informant-reported ECog memory score interaction for Delayed Recall (B = 0.20, β= 0.23, SE = 0.11, p = 0.05; Fig. 4C); trend for Immediate Recall (B = 0.21, β= 0.22, SE = 0.11, p = 0.07; Fig. 3C). Informant-reported ECog memory scores were associated with Immediate and Delayed Recall in both aMCI women and men; however, associations were stronger in women (Immediate Recall: B = –0.36, β= –0.23, SE = 0.09, p < 0.001; Delayed Recall: B = –0.47, β= –0.31, SE = 0.09, p < 0.001) versus men (Immediate Recall: B = –0.23, β= –0.17, SE = 0.07, p = 0.001; Delayed Recall: B = –0.35, β= –0.28, SE = 0.06, p < 0.001). In aMCI, there were no sex by discrepancy group interactions for RAVLT scores. Regardless of sex, underestimation, but not overestimation, of one’s memory decline (relative to informant) was associated with poorer Immediate and Delayed Recall (ps < 0.01).
Sex differences in relationship between SMC and AD biomarker
Overall sample
There were no interactive effects between sex and self- or informant-reported ECog memory score or discrepancy group on the odds of Aβ positivity (ps > 0.05; Table 4). Regardless of sex, higher self- and informant-reported ECog memory scores was associated with greater odds of Aβ positivity (p < 0.001), although this association was a trend for self-reported ECog memory scores (p = 0.09). Underestimation, but not overestimation, one’s memory decline (relative to informant) was associated with greater odds of Aβ positivity (p = 0.04).
Results of multivariable logistic regression analyses modeling the independent effects of ECog memory variables (i.e., self- and informant-reported ECog memory scores and discrepancy group) and their interactive effects with sex on Aβ positivity
All analyses were adjusted for age, education, ApoE status, and diagnosis (overall sample only). OR, odds ratio; CI, confidence interval; NC, normal controls; aMCI, amnestic mild cognitive impairment; Aβ, amyloid-β.
Diagnostic groups
There were no interactive effects between sex and self- or informant-reported ECog memory scores or discrepancy group on the odds of Aβ positivity in the NC or aMCI groups (ps > 0.05). Regardless of sex, self- or informant-reported ECog memory scores or discrepancy group was not associated with odds of Aβ positivity in the NC group (ps > 0.05). In the aMCI group, self-reported ECog memory scores was not associated with Aβ positivity (p = 0.15); however, higher informant-reported scores were associated with greater odds of Aβ positivity (p < 0.001). Underestimation, but not overestimation, of one’s memory decline relative to informant was also associated with greater odds of Aβ positivity in aMCI (p = 0.01).
Sex differences in verbal memory performance across [18F]AV45 SUVR quintiles
The sex by [18F]AV45 SUVR quintile interaction was not significant for Immediate Recall (B = 0.05, β= 0.08, SE = 0.05, p = 0.31); however, the decrease in mean Immediate Recall z-score from quintile 1 to 5 was larger in women (mean z-score decrease = –0.87 SUVR) versus men (mean z-score decrease = –0.55). The sex by SUVR quintile interaction was significant for Delayed Recall (B = 0.13, β= 0.20, SE = 0.05, p = 0.01; Fig. 3). The association between SUVR quintile and Delayed Recall scores was stronger in women (B = –0.18, β= –0.22, SE = 0.04, p < 0.001) versus men (B = –0.10, β= –0.13, SE = 0.04, p = 0.01). Among individuals in quintiles one to four (indicative of mild-to-moderate amyloid deposition), women outperformed men on RAVLT outcomes (ps < 0.05), but, in the highest quintile (indicative of severe amyloid deposition), this female advantage was eliminated for Delayed Recall and diminished for Immediate Recall.
Testing specificity of findings: Analysis of executive function
In the overall sample, there were no sex differences in self-reported, informant-reported or mean discrepancy scores for ECog organization scores; however, a higher proportion of women overestimated their organization decline relative to informants (p = 0.05). There were no interactive effects between sex and self- or informant-reported ECog organization scores or organization discrepancy group on TMT part B (ps > 0.05). Higher self- and informant-reported ECog organization scores were similarly related to poorer TMT Part B performance in men (self-reported: B = 0.47, β= 0.22, SE = 0.09, p < 0.001; informant-reported: B = 0.28, β= 0.14, SE = 0.09, p = 0.003) and women (self-reported: B = 0.29, β= 0.13, SE = 0.10, p = 0.005; informant-reported: B = 0.33, β= 0.19, SE = 0.07, p < 0.001). Regardless of sex, under- or overestimation of one’s organization decline was not associated with TMT Part B scores (ps > 0.05). Results were unchanged within diagnostic groups.
Sex X ApoE interaction
Because of evidence indicating a moderating role of sex on the effects of ApoE on AD-related outcomes [37–39], all analyses were repeated while adjusting for a sex by ApoE interaction and results remained the same.
DISCUSSION
Findings show that the sex of the participant impacts the ability of SMC to predict impairment on objective memory tests in aMCI. As hypothesized, the significant relationship between self- and informant-reported SMC and verbal memory performance was stronger in women versus men in the overall sample; however, this finding was driven by the aMCI group. Similar to most previous findings, we found that higher self-reported SMC was associated with poorer memory in NC regardless of sex. Conversely, self-reported SMC were associated with verbal memory performance in aMCI women but not aMCI men. This result suggests that the lack of association between subjective and objective memory performance in MCI in previous studies may be driven by over-representation of men or because of an effect dilution due to failure to consider sex. Given the higher prevalence of aMCI in men versus women [14, 15], men likely represent the majority in most aMCI samples. This was true of our ADNI sample where men comprised 57% of the sample. Results highlight the importance of considering sex when examining the clinical utility of SMC and suggest that sex differences may contribute to disparate findings across previous studies.
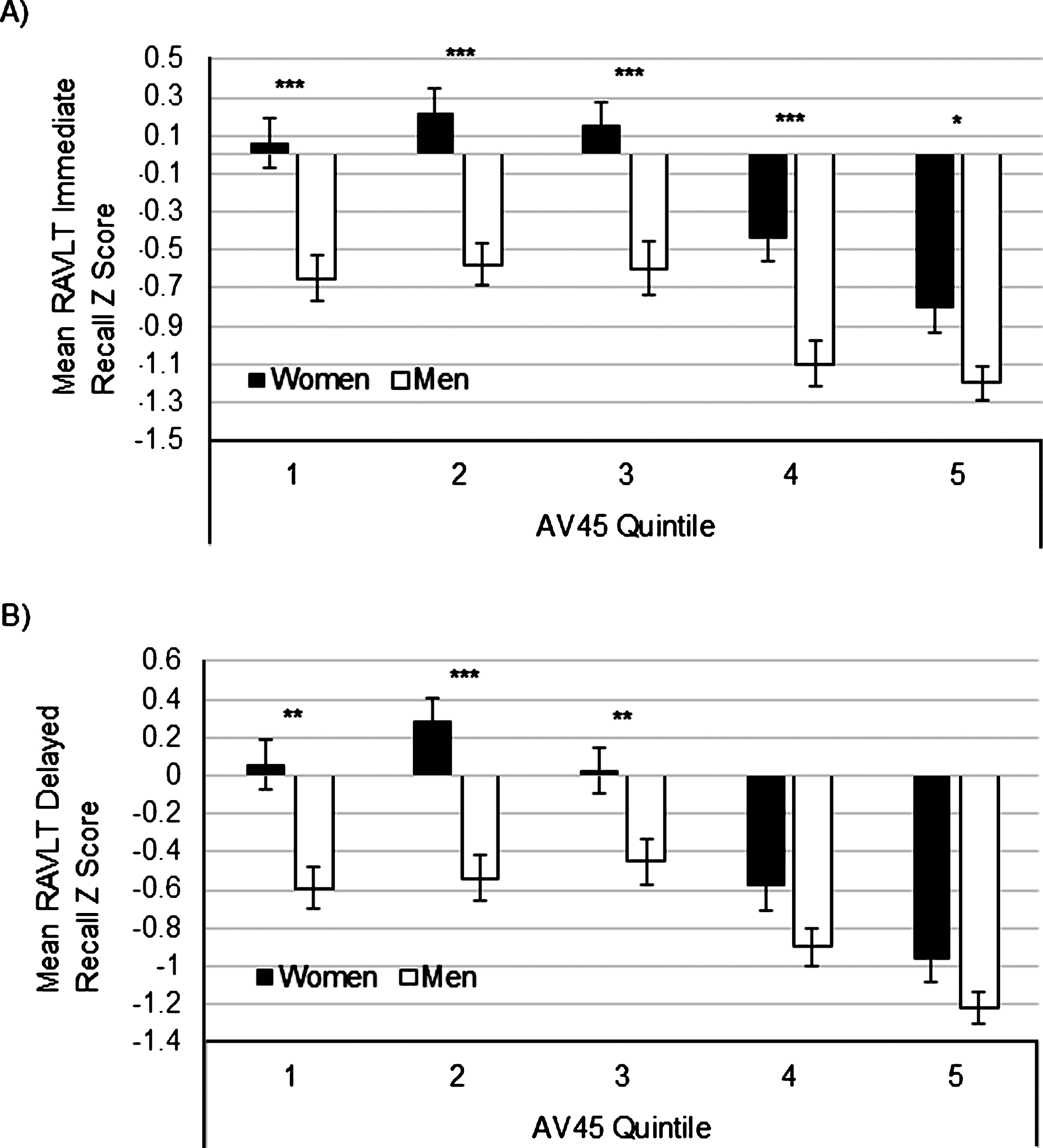
Sex differences in RAVLT Immediate (A) and Delayed (B) Recall scores across [18F]AV45 SUVR quintiles. *p <0.05, **p <0.01, ***p <0.001.
We found a relationship between higher self-reported SMC and poorer memory in NC suggesting that SMC is beneficial in detecting early cognitive decline. However, the relationship between higher SMC and poorer memory was weaker (i.e., Immediate Recall) or non-existent (i.e., Delayed Recall) in aMCI. Findings were opposite with informant-reported SMC. Higher informant-reported SMC was associated with poorer memory in aMCI, but this relationship was weaker (i.e., Delayed Recall) or non-existent (i.e., Immediate Recall) in NC. These results provide converging evidence that self-reported SMC can reflect objective memory in healthy, older adults, and may be superior to informant-reported SMC, but self-perception of cognitive ability decreases as disease develops. We extend these findings by demonstrating that, among individuals with aMCI, self-reported SMC may continue to have predictive value in women only.
Consistent with hypotheses, we found that underestimating one’s memory decline relative to informant-report was associated with poorer verbal memory performance in aMCI and this association was similar in women and men. This finding provides further support for the theory that underestimation is a harbinger for cognitive decline. Conversely, overestimation of one’s memory decline was not associated with verbal memory performance across or within diagnostic groups. Edmonds et al. [6] previously found that that one-third or more of individuals that were diagnosed with MCI using conventional diagnostic criteria perform normally on more extensive cognitive testing despite their MCI diagnosis. This “cognitively-normal” MCI subgroup overestimated their cognitive problems relative to their informant [6]. Together, findings suggest that overestimation of cognitive deficits may be characteristic of normal cognitive aging. Overestimation was more prevalent in women versus men and this may reflect a gender bias in reporting health-related symptoms. Evidence suggests that women endorse more health-related symptoms than men that are not correlated with objective measures of health possibly due to gender differences in willingness to disclose discomfort or sensitivity to minor health-related perturbations [40, 41]. Given women’s tendency to overestimate cognitive compromise in normal cognitive aging, underestimating may be more meaningful and reflective of real cognitive decline in women versus men.
Biological and/or psychosocial factors could explain the sex difference we observed. Depressive symptoms were higher in women, but likely do not underlie the sex difference since they related similarly to SMC in men and women. As mentioned previously, there is a gender difference in reporting health-related symptoms which may underlie the higher rates of SMC overestimation in women versus men; however, it likely does not underlie the greater predictive utility of informant-reported SMC in women versus men since it is reasonable to assume that the majority of women’s informants were a male spouse (although sex of the informant was unavailable).
As mentioned previously, another potential explanation for the sex difference may be a more precipitous and perceptible memory decline in women versus men in the aMCI to AD transition. We found a significant sex by Aβ quintile interaction on Delayed Recall where women outperformed men at lower quintiles of Aβ deposition, yet men and women performed similarly at the highest quintile. This interaction suggests women have greater and more accelerated disease-related decline in verbal memory. The more precipitous decline in women despite their initial advantage in verbal memory is consistent with the cognitive reserve theory. This theory proposes that favorable premorbid factors (e.g., advanced education) confer a “reserve” capacity to engage compensatory brain networks and/or cognitive strategies as to maintain cognition despite encroaching brain pathology [42–44]. Those with higher cognitive reserve are better able to delay clinical onset of cognitive impairment until a later disease stage [42–44]; however, once brain pathology depletes brain resources past a threshold level, cognitive decline begins and is more accelerated because of the more advanced pathology. The female advantage in verbal memory may serve as a form of cognitive reserve allowing women to maintain normal verbal memory operations for longer than men despite comparable AD pathology [17, 29]. In support of this theory, [18F]AV45 SUVR and the prevalence of Aβ positivity was higher in NC women versus men suggesting that women are better able to maintain normal verbal memory performance despite accumulating pathology. However, women may have more accelerated decline after pathology reaches a threshold point [43, 44] which appears to be quintile 3 (Fig. 3).
Our hypothesis that greater self- or informant-reported SMC would relate to greater odds of Aβ positivity similarly in women and men was supported in the overall sample. This finding is somewhat counterintuitive given that self- and informant-reported SMC were more predictive of memory performance in women than men; however, it is consistent with the possibility that greater cognitive reserve may delay onset of memory decline in women despite accumulating AD pathology. A delayed onset of memory decline despite accumulating pathology in women would create a misalignment between memory and AD biomarkers, whereas, in men, the trajectories of memory decline and advancing pathology are more linear and concordant. In diagnosis-stratified analyses, informant-reported scores were associated with the odds of Aβ positivity in both aMCI women and men; however, self-reported SMC were not related to Aβ positivity in either diagnostic group. This could be due to a weak relationship that is undetectable when statistical power decreases in diagnosis-specific analyses. However, the weak Aβ and SMC relationship is expected given reports of no relationships between Aβ and subjective and objective memory in NC [45–47], and the low variability in SMC in aMCI considering that SMC is required for aMCI diagnosis.
In contrast to our findings with SMC, ECog organization scores were consistently associated with executive function performance in both NC and aMCI men and women suggesting that individuals may be more perceptive of declines in executive function perhaps because of the large degree to which executive function contributes to everyday activities. This disparity in findings suggests that the sex differences in the relationship between subjective cognitive complaints and objective performance does not generalize to all cognitive domains and may be specific to verbal memory. The fact that the executive function domain does not typically show a sex difference may support our theory that a female-specific cognitive reserve in verbal memory may contribute to our sex difference findings with memory.
Strengths of the current study include 1) use of sex by SMC interaction terms and sex-stratified analyses to examine a sex difference in SMC utility in a large cohort of cognitively normal older adults and those with MCI; 2) comparison of SMC to an AD biomarker in addition to objective memory performance; and 3) testing the generalizability of results to executive function. A limitation is that cross-sectional analysis precluded examination of sex differences in the relationship between change in subjective and objective memory performance over time. Another limitation is that results cannot be easily generalized to other types of memory or to populations that differ significantly from the predominantly white and well-educated convenience sample of ADNI.
In summary, our results are consistent with the broader literature in finding that self-reported SMC predict memory performance in NC, suggesting that they may be a harbinger of later cognitive decline. However, the predictive ability of self-reported SMC in aMCI is limited to women. This sex difference may contribute to disparities in findings from previous studies of SMC to the degree that studies vary in the proportion of men they contain. A more precipitous and perceptible decline in verbal memory with advancing AD pathology in women than in men may underlie the sex difference in the clinical utility of SMC. Taken together, these results indicate the importance of conducting sex-stratified analyses when examining SMC and their correlates. From a clinical perspective, the requirement for SMC in aMCI diagnostic criteria is challenged given its dependence on sex, its relationship to other previously-identified correlates (e.g., depressive symptoms), and variable self-awareness or memory changes. Clinicians should consider the patient’s sex when evaluating SMC.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the NIH (grant numbers AG049810, AG05131, and K24 AG026431).
Data collection and sharing for this project was funded by the Alzheimer’s Disease Neuroimaging Initiative (ADNI) [National Institutes of Health Grant U01 AG024904] and DOD ADNI [Department of Defense award number W81XWH-12-2-0012]. ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.