
Abstract
Background:
An association between obstructive sleep apnea (OSA) and Alzheimer’s disease has been suggested but little is known about amyloid-β and tau deposition in this syndrome.
Objective:
To determine amyloid and tau burden and cognitive function in OSA in comparison with those without a diagnosis of OSA.
Methods:
The status of OSA was determined by asking participants about history of polysomnographic diagnosis of OSA and the use of Continuous Positive Airway Pressure (CPAP). A comprehensive neuropsychological battery measured cognitive function. Positron emission tomography (PET) was used to measure standardized uptake value ratio (SUVR) of 18F-florbetaben and 18F-AV1451, to quantify amyloid and tau burden.
Results:
119 male Vietnam veterans completed assessment. Impairment in visual attention and processing speed and increased body mass index (BMI) were seen in subjects with OSA compared with those without a diagnosis OSA. The cortical uptake of 18F-florbetaben was higher in the OSA group than in the control group (SUVR: 1.35±0.21 versus 1.27±0.16, p = 0.04). There were more apolipoprotein E ɛ4 allele (APOE ɛ4) carriers in the OSA group than in the control group. In multilinear regression analysis, the significance of OSA in predicting 18F-florbetaben uptake remained independent of age and vascular risk factors but not when BMI or APOE ɛ4 was adjusted. The reported use of CPAP (n = 14) had no effect on cognitive or amyloid PET findings. There was no significant difference in 18F-AV1451 uptake between the two groups.
Conclusions:
Obstructive sleep apnea is associated with Alzheimer’s disease pathology, but this relationship is moderated by APOE ɛ4 and BMI.
INTRODUCTION
Alzheimer’s disease (AD) is the most common cause of dementia [1, 2]. The precise mechanism of the disease is still unknown, but investigations over the past several decades have identified numerous risk factors for AD [3–9]. Age is the strongest risk factor for AD and genetic factors posit substantial risk [5, 8]. Neuritic plaques and neurofibrillary tangles (NFT) are the two cardinal lesions of AD. The plaque contains a central core of amyloid-β (Aβ) and NFT are intracytoplasmic fibrillar structures composed of abnormally phosphorylated tau proteins [10, 11]. Given that amyloid plaques and NFT are cardinal lesions in AD, positron emission tomographic (PET) imaging using specific radioactive ligands that bind to amyloid and tau is a useful technique to evaluate the risk factors of AD. 18F-florbetaben and 18F-AV1451 are radio-ligands that have specific affinity for Aβ and 3R4 R tau aggregates, respectively [12, 13].
Sleep disorders have been investigated as potential risk factors for AD. Obstructive sleep apnea (OSA) is a syndrome that is diagnosed in the presence of clinical symptoms, most commonly excess daytime sleepiness in conjunction with an apnea-hypopnea index (AHI) greater than 5 events per hour [14]. The prevalence of OSA in the community-based cohorts has been estimated as 2% –8% and it increases with age [15, 16]. Early studies demonstrated an association between AD and sleep apnea and a correlation between the severity of apnea and dementia [17, 18]. Recent investigations have demonstrated a link between Aβ deposition and sleep disturbances [19]. OSA is associated with earlier onset of both mild cognitive impairment (MCI) and dementia compared with subjects without OSA [20]. In a small sample of five patients with MCI, higher AHI and oxygen desaturation index were associated with greater amyloid deposition [21]. However, little is known about Aβ and tau imaging in cognitively asymptomatic individuals with OSA. In the present study, we report cognitive function and Aβ and tau imaging findings in cognitively asymptomatic patients with OSA.
METHODS
Participants recruitment
This was a cross-sectional study evaluating AD risk in the community-based Vietnam Veterans. Veterans were recruited via the Older Veterans Psychiatric Program of the Repatriation Hospital, Austin Health and advertisement in magazines and newsletters of Retired Service League and the Vietnam Veterans Association of Australia. The institutional review board of Austin Health, a major metropolitan health service in Melbourne provided ethical approval for the study. Presence of dementia, existing diagnosis of MCI, psychotic and bipolar affective disorder, current substance abuse, and any unstable medical condition that could have impacted cognitive performance or made participation difficult were exclusions. Assessment consisted of medical history, Pittsburgh Sleep Quality Index (PSQI) [22], neuropsychological examination, apolipoprotein E (APOE) ɛ4 status, vascular risk factors, and Aβ and tau imaging. For the analysis of cognitive functions, subjects with traumatic brain injury (TBI) were excluded given its impact on cognitive outcomes. All subjects were screened for a history of polysomnographic diagnosis of OSA and the use of Continuous Positive Airway Pressure (CPAP) mask. This history was corroborated by documentation from the primary care doctor of participants whenever possible. Those with no polysomnographic diagnosis of OSA or symptoms of OSA were the controls. Considering the poor sensitivity of the global score of PSQI in detecting OSA [23], the global score was not used to diagnose OSA but positive responses to the individual items-cessation of breathing during sleep and excess daytime sleepiness-were exclusion criteria for the controls.
Assessment of cognitive functions and vascular risk factors
The neuropsychological examination included Logical Memory subset test 1 and 2 of Wechsler Memory Scale (WMS) – Anna Thompson story only [24], digit span forward and backwards from the Wechsler Adult Intelligence Scale third edition [25], categorical fluency test from the Delis-Kaplan Executive Function System [26], Rey Osterrieth Complex Figure Test (ROCFT) [27] and Trail Making Test parts A and B [28]. Vascular risk factor score was calculated by giving one point to each of the following: Diabetes mellitus, hypertension, coronary artery disease, hypercholesterolemia, body mass index (BMI) above 30, current smoking status, previous history of stroke, and atrial fibrillation. Sum of all points gave cumulative vascular risk.
PET imaging
The participants underwent a 20-min PET scan (4 x 5-min frames of emission data collected) acquired 90 min after a slow IV bolus administration of 250 MBq (±10%) of 18F-florbetaben and 70 min after the injection of 370 MBq of 18F-AV1451. Acquisition was performed with a Siemens PET/CT mCT128 and CT attenuation correction was applied. Image reconstruction used the Ordered Subset Expected Maximization (OSEM) algorithm. There was no correction for partial volume effect. 18F-florbetaben and 18F-AV1451 PET were both analyzed with Computational Analysis of PET from AIBL (CapAIBL) software developed by the Commonwealth Scientific and Industrial Research Organization (CSIRO) [29]. CapAIBL allows quantitative PET measurements without relying on magnetic resonance imaging [30]. Global Aβ and regional tau burden were calculated by standardized uptake value ratio (SUVR) using cerebellar grey matter uptake as the reference. 18F-Florbetaben scans were also read visually according to the manufacturer’s instructions by three readers and the classification into negative or positive scan was based on majority results. 18F-AV1451 regional uptake in three regions was calculated by CapAIBL software: Mesial temporal (amygdala, hippocampus, entorhinal cortex, and parahippocampus); temporoparietal (inferior and middle temporal lobe, fusiform gyrus, posterior cingulate/precuneus, superior and inferior parietal and lateral occipital cortex); and rest of the neocortex. A visual read of 18F-AV1451 images was not performed as a standard method has yet to be developed.
Statistical analyses
The continuous variables viz., 18F-florbetaben and 18F-AV1451 SUVRs and neuropsychological test scores were analyzed using independent t test while the categorical variables, OSA and APOE ɛ4 status, were analyzed by Chi-square test. All tests were two-tailed with 95% confidence interval. Pearson correlation was used to find correlates of both 18F-florbetaben and 18F-AV1451 SUVRs and cognitive test scores. Multilinear regression analysis was then performed with explanatory variables found to be correlated and associated with 18F-florbetaben or 18F-AV1451 SUVRs and cognitive scores. 18F-florbetaben and 18F-AV1451 SUVRs and cognitive scores were treated as the dependent variables. General linear model was used to test the interaction between OSA and amyloid and tau tracer SUVRs and a visually positive amyloid scan in predicting cognitive function.
RESULTS
Between March 2014 and June 2017, 170 veterans underwent screening after providing informed consent. From the consecutive sample, 44 veterans were excluded: 11 veterans had medical morbidities making participation difficult; seven met criteria for alcohol abuse; five had existing diagnosis of MCI; five could not cope with psychiatric assessment because of post-traumatic stress disorder and perceived stress; one had bipolar affective disorder; one had claustrophobia; and 14 withdrew from the study because of inconvenience. After exclusion 126 male veterans completed neuropsychological assessments and scans. Seven veterans reported symptoms of OSA according to PSQI but they did not have polysomnographic evaluation and they were therefore excluded from the analyses. The data from the remaining 119 veterans were analyzed. A polysomnographically confirmed diagnosis of OSA was present in 42 (35.2%) subjects. The characteristics of participants are shown in Table 1. Twenty-four patients reported regular use of CPAP; 14 veterans did not use CPAP; and use was indeterminate in four subjects. The mean duration between the diagnosis of OSA and the study assessment was 74.35±27.06 months. Veterans with OSA had significantly higher vascular risk factor score compared with those without OSA (2.37±1.18 versus 1.43±1.16, p < 0.001, CI = –1.45 to –0.42). BMI was significantly higher in the OSA group than in the controls (32.56±4.05 versus 27.82±4.03, p < 0.001). There was no significant difference in age or years of education between the OSA and the control group (Table 1). The characteristics of OSA has been shown in Table 2.
Patients characteristics in OSA
Characteristics of OSA
Veterans with OSA and controls did not differ significantly in the following cognitive functions: Digit span, categorical fluency, Logical Memory Test 1 and 2, ROCFT, ROCFT 3-min and 30-min delayed recall. However, subjects with OSA scored significantly higher on Trail Making Test A (time to completion in seconds: 41.81±12.54 versus 35.63±11.69, p = 0.03, CI = –11.80, to –0.544) and B (time to completion in seconds: 126.70±82.47 versus 97.95±33.79, p = 0.03, CI = –54.29 to –3.22) (Table 3). Both test scores positively correlated with vascular risk factor score (r = 0.24, p = 0.03; r = 0.22, p = 0.04, respectively). The significant relation between OSA and Trail Making Test B did not stay when Trail Making Test A, a measure of visual attention and processing speed was controlled (R2 = 0.23, p = 0.12). The significance of OSA in predicting Trail Making Tests A (R2 = 0.118, p = 0.04) remained upon controlling the effects of age, education and APOE ɛ4, but not when vascular risk factor score was adjusted for (R2 = 0.07, p = 0.16). In the general linear model analysis, there was no significant interaction between 18F-florbetaben SUVR and OSA or visually positive 18F-florbetaben scan and OSA in predicting either Trail Making Test A or B.
Cognitive tests scores in OSA
18F-florbetaben and 18F-AV1451 SUVR
The boxplots for the distribution of 18F-florbetaben SUVR are given in Fig. 1. Independent t test showed that the SUVR of 18F-florbetaben was significantly higher in the OSA group than in the control group (1.35±0.21 versus 1.27±0.16, p = .04, CI = –0.14 to –0.003). A greater number of subjects with a visually positive 18F-florbetaben scan in the OSA group did not reach significance between the OSA and the control group (29.7% versus 17.3%, χ2 = 2.26, p = 0.13). There was no significant increase in 18F-AV1451 SUVR in OSA in any regions studied (Table 3). BMI significantly and positively correlated with 18F-florbetaben SUVR (r = 0.341, p < 0.001) which was significantly higher in those with obesity (BMI more than 30, n = 48) compared with those who were non-obese (1.37±0.22 versus 1.25±0.13, p < 0.001). Vascular risk score showed significant positive correlation with global SUVR of 18F-florbetaben (r = 0.206, p = 0.049) and regional SUVRs of 18F-AV1451 in mesial temporal (r = 0.327, p = 0.004) and temporoparietal (r = 0.26, p = 0.03) regions. When separate analysis was done for the OSA group there was no significant difference between veterans who were regularly using CPAP and the non-users of CPAP in global 18F-florbetaben (1.36±0.23 versus 1.35±0.22, p = 0.82) or regional 18F-AV1451 SUVRs. Baseline sleep diagnostic reports were available for 14 subjects. The negative correlation between nadir oxygen saturation and 18F-florbetaben SUVR did not reach statistical significance (r = –0.563, p = 0.140). There was no significant correlation between AHI and 18F-florbetaben SUVR (r = –0.316, p = 0.317).

18F-florbetaben SUVR in OSA and controls.
APOE ɛ4 carrier status was available for 104 veterans. There was increased rate of APOE ɛ4 allele in the OSA group compared with the controls (34.2% versus 15.9%, χ2 = 4.53, p = 0.03). The SUVR for 18F-florbetaben was significantly higher in the APOE ɛ4 carriers than in the non-carriers (1.41±0.21 versus 1.27±0.17, p = 0.02). There were more visually positive 18F-florbetaben scans in APOE ɛ4 carriers than in non-carriers (50% versus 13.2%, χ2 = 14.17, p < 0.001). The SUVR of 18F-AV1451 did not show a significant difference between APOE ɛ4 carriers and non-carriers in any regions. In the multilinear regression analysis with 18F-florbetaben SUVR as the dependent variable, vascular risk factor score and APOE ɛ4 were added to OSA because these variables showed association and correlation with 18F-florbetaben SUVR. Age was also added in view of its well-known correlation with amyloid deposition. The significance of OSA in predicting 18F-florbetaben SUVR remained significant upon controlling for vascular risk score (R2 = 0.10, p = 0.04) and age (R2 = 0.07, p = 0.03). Similarly, APOE e4 continued to be a significant predictor of 18F-florbetaben SUVR when age (R2 = 0.08, p = 0.02) and vascular risk score (R2 = 0.10, p = 0.04) were adjusted. OSA did not retain its significance in predicting a visually positive 18F-florbetaben scan (R2 = 0.11, p = 0.12) or 18F-florbetaben SUVR (R2 = 0.145, p = 0.971) when APOE ɛ4 or BMI was added while APOE ɛ4 (p = 0.037) and BMI remained significant (p = 0.010). In the general linear model there was no significant interaction (F = 0.11, p = 0.73) between APOE ɛ4 and OSA in predicting 18F-florbetaben SUVR (Fig. 2).
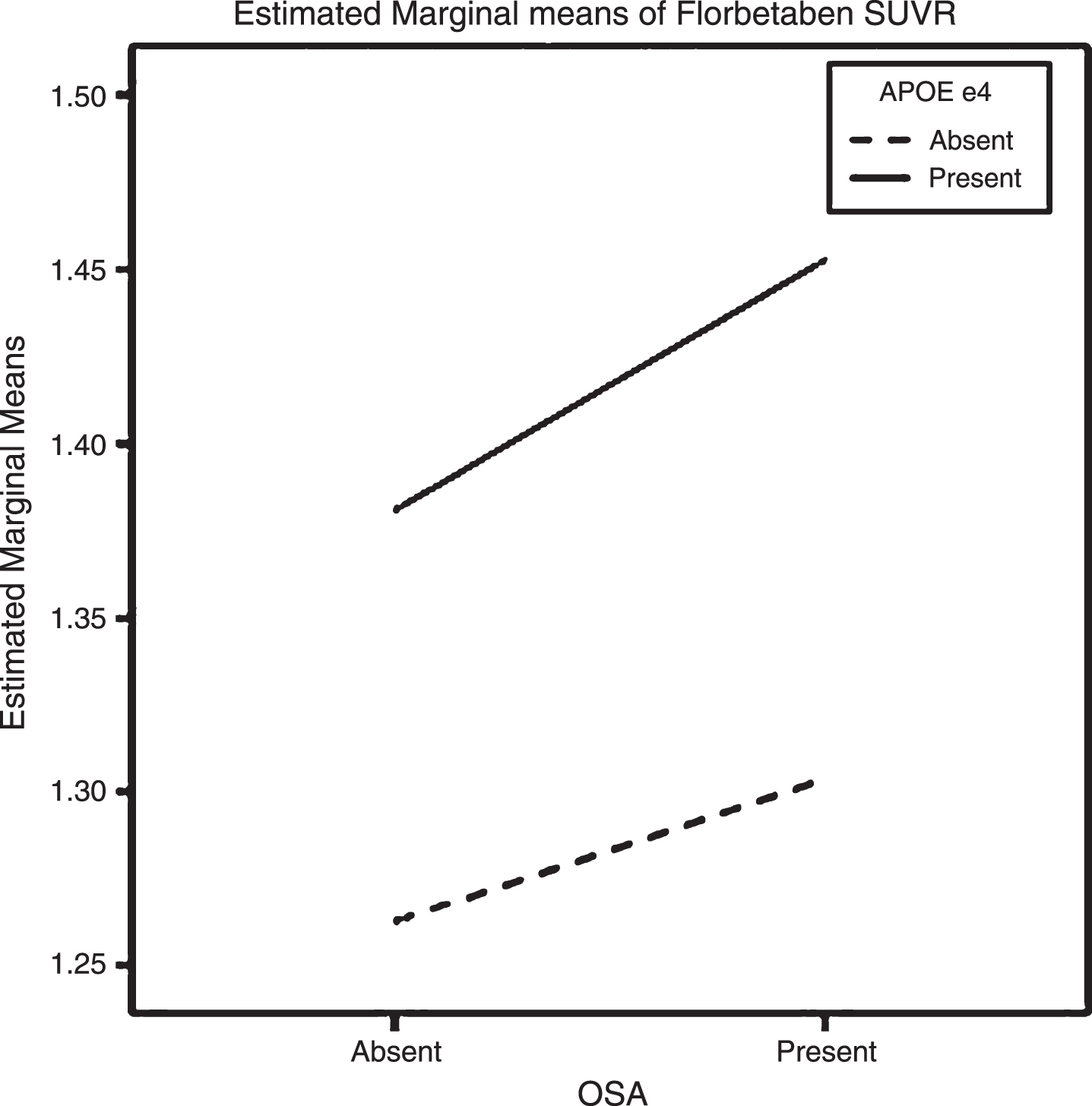
Interaction between OSA and APOE ɛ4: In the presence of APOE ɛ4, amyloid burden was more greatly increased in OSA.
DISCUSSION
Cognitive functions
The cognitive functions previously reported to be impaired in OSA include attention, procedural memory and episodic memory [31–33], processing speed [34], spatial memory [33], and executive function [35, 36]. Executive dysfunction has been reported in Vietnam veterans with OSA [35]. Language ability and psychomotor functions remain relatively unaffected. In the present study, subjects with OSA performed poorly on Trail Making Tests A and B. The Trail Making Test A measures visual attention and processing speed whereas Trail Making Test B assesses executive function. Felver-Gant et al. reported impaired performance on Trail Making Test B in OSA [35]. We have replicated this finding in subjects with OSA, but when we controlled for the score of Trail Making Test A, the effect of visual attention and processing speed the significance of Trail Making Test B did not remain indicating that the deficit was actually in the processing speed rather than executive function. The association between OSA and impairment in these cognitive domains was independent of age, APOE ɛ4, and education of the subjects, but not vascular risk burden, which was associated with OSA. The confounding effect of vascular burden was not adequately addressed in previous studies. A review of cognitive deficits in OSA has revealed varying cognitive deficits across studies [37]. The pattern of cognitive deficits varied according to the assessment settings (community cohorts against sleep medicine clinic), treatment with CPAP and age [38, 39]. A study that compared cognitive functions between young and older individuals found more attentional deficits in the older patients, a pattern supported by our study [37].
Sleep apnea and Alzheimer’s disease
Apart from cognitive impairment, existing data suggest an association between OSA and MCI and dementia. A seminal longitudinal study found a two-fold risk for MCI or dementia in patients with OSA over five-year follow-up [20]. Following early observations of association between OSA and dementia further findings have accrued recently supporting the link between sleep disordered breathing and both MCI and dementia [18–20]. A recent study demonstrated annual decline in the level of cerebrospinal fluid (CSF) Aβ42 over a two-year period in cognitively asymptomatic elderly patients with OSA, implying increased risk of AD in this condition [40]. The change in CSF Aβ42 correlated with the severity of OSA independent of APOE. However, there was no association between OSA and increased amyloid uptake on PET scan. The results of the present study show that patients with a polysomnographic diagnosis of OSA have slight but significantly higher global uptake of 18F-florbetaben compared with subjects without a diagnosis OSA. This association was independent of age and vascular risk factors, but not APOE ɛ4 or BMI. Both BMI and APOE ɛ4 were associated with 18F-florbetaben SUVR. Previous studies have suggested a negative correlation between BMI and amyloid load [41, 42]. The relationship between dementia and BMI is two-phased, increased risk of dementia was seen with BMI when weight was measured 20 years or more prior to dementia diagnosis and this association was reversed when weight was measured in 10 years or less before dementia diagnosis [43]. The first phase may represent a causal effect of obesity on dementia and the second phase is due to weight loss from metabolic changes arising from damage to medial temporal lobe during long preclinical stage of AD. The mean age of our subjects was 68.36 years suggesting that the participants have not yet reached the stage of declining weight which may commence with increasing amyloid accumulation at any stage later.
There was no significant difference in regional uptakes of 18F-AV-1451 between the groups. Recently a small study found increased amyloid deposition in elderly patients with MCI and OSA in correlation with oxygen desaturation index [21]. Such a correlation was not found in cognitively normal individuals with OSA [21], but the sample sizes of this study were very small, eight patients with normal cognitive function and five patients with MCI. Our subjects were elderly without an existing diagnosis of MCI.
Interaction between sleep apnea and APOE ɛ4
The mechanism through which OSA is associated with dementia and Aβ deposits is not precisely known. Aβ binding to APOE ɛ4 results in Aβ-APOE ɛ4 complex which is internalized by Very Low-Density Lipoprotein (VLDL) receptor more slowly than Aβ-APOE ɛ2 and Aβ-APOE ɛ3 complexes leading to decreased clearance of Aβ with APOE ɛ4 [44]. In the general population and clinical samples, OSA was found to be associated with the APOE ɛ4 allele [45–47] but other studies and a meta-analysis did not find such an association [48]. We found a significantly increased rate of APOE ɛ4 in OSA in our sample but the significantly increased Aβ tracer retention in OSA was no longer observed when the effect of APOE ɛ4 was controlled. APOE ɛ4 had stronger association with Aβ burden than OSA. The influence of OSA on 18F-florbetaben SUVR was higher in the presence of APOE ɛ4, than in its absence (Fig. 2). We did not find a significant difference in tau retention between the OSA group and controls but considering that cortical tau deposition follows Aβ accumulation and may be more closely associated with cognitive deficits, or dementia, this is not unexpected as our sample excluded subjects with MCI.
Limitations
While the diagnosis of OSA was made with polysomnographic studies, subjects without a diagnosis of OSA did not have laboratory sleep evaluation. The corollary is that some of the control subjects may have undiagnosed OSA. Therefore, the control group is not really a group without OSA; rather it is a group without symptoms of OSA. In our study we used PSQI, a sleep questionnaire that elicits symptoms of arrested breathing during sleep and daytime sleepiness. One study has reported that PSQI has poor sensitivity (38%) in screening for OSA, but this study used global PSQI score, not the responses to individual questions that are most relevant to OSA [23]. We excluded the participants who reported symptoms of OSA on PSQI. The rate of OSA in our sample (35.2%) is higher than the prevalence of OSA reported in the older general community (17% –24%) suggesting that Australian Vietnam veterans are well monitored for this condition and at low risk for missed diagnosis [49]. Our sample was primarily veterans with military deployment. This may limit generalizability of the above findings. The correlational analysis between nadir oxygen saturation and 18F-florbetaben SUVR involved a small sample and type II error needs to be considered in this context. It is noteworthy that the subject with highest 18F-florbetaben SUVR (2.01) had the lowest oxygen saturation (74%). Therefore, an association between oxygen desaturation and Aβ in OSA cannot be ruled out.
CONCLUSION
We identify an association between obstructive sleep apnea and increased Aβ deposition. However, the association with Aβ deposition was moderated by APOE ɛ4 and BMI. Overall the study does not support a direct association between OSA and increased Aβ deposition. Likewise, an association between obstructive sleep apnea and increased tau retention was not established in this study.