
Abstract
Alzheimer’s disease (AD) is a neurodegenerative disease characterized by progressive neuron losses in memory-associated brain structures that rob patients of their dignity and quality of life. Five drugs have been approved by the FDA to treat AD but none modify or significantly slow disease progression. New therapies are needed to delay the course of this disease with the ultimate goal of preventing neuron losses and preserving memory functioning. In this review we describe the renin-angiotensin II (AngII) system (RAS) with specific regard to its deleterious contributions to hypertension, facilitation of neuroinflammation and oxidative stress, reduced cerebral blood flow, tissue remodeling, and disruption of memory consolidation and retrieval. There is evidence that components of the RAS, AngIV and Ang(1–7), are positioned to counter such damaging influences and these systems are detailed with the goal of drawing attention to their importance as drug development targets. Ang(1–7) binds at the Mas receptor, while AngIV binds at the AT4 receptor subtype, and these receptor numbers are significantly decreased in AD patients, accompanied by declines in brain aminopeptidases A and N, enzymes essential for the synthesis of AngIV. Potent analogs may be useful to counter these changes and facilitate neuronal functioning and reduce apoptosis in memory associated brain structures of AD patients.
Keywords
INTRODUCTION
Approximately 5.5 million people in the U.S. are diagnosed with Alzheimer’s disease (AD) [1, 2], while an additional 1 + million Americans are afflicted with mild cognitive impairment (MCI), a predisposing condition to AD [3]. Present treatment and care costs are estimated at $70–100 billion [4, 5], while the number of AD patients is predicted to reach 15 million by 2060 [6]. In the absence of a breakthrough in treatment, these patient numbers and associated costs will overwhelm our health care system. There is also growing concern over concussion-induced cortical damage seen in children and adults who participate in contact sports such as American football (chronic traumatic encephalopathy), boxing, martial arts, and soccer, and our service men and women who have experienced combat associated concussions [7, 8]. Evidence indicates that repeated concussions may encourage MCI [3]. Despite intensive research efforts, only two categories of drugs have been approved by the FDA to treat AD, and none in the past 20 + years. Cholinesterase inhibitors extend the half-life of acetylcholine, while the N-methyl-D-aspartate (NMDA) receptor antagonist, memantine, limits glutamate excitotoxicity and resulting neuronal damage [9–14]. These drugs have demonstrated limited ability to delay the symptoms of AD and none prevent disease progression.
AD patients present extensive distributions of senile plaques and neurofibrillary tangles accompanied by neuroinflammation, oxidative stress-induced damage, and a pronounced loss of synaptic connections predisposing neuronal apoptosis [15]. Plaques composition includes aggregates of amyloid-β peptide (Aβ) due to a significant elevation in the production of neurotoxic Aβ1 - 42 [16, 17]. The Aβ1 - 42 peptide oligomerizes resulting in neuronal toxicity. Neurofibrillary tangles are characterized by aggregated hyperphosphorylated tau protein. These proteins normally act to stabilize microtubules but in AD patients they contribute to a loss of neuronal structural integrity ultimately impacting synaptic connections.
The goal of providing an effective treatment for AD has been elusive in part due to the multifactorial characteristics of the disease process and difficulty in identifying reliable biomarkers [18–20]. It has been speculated that the pathology associated with AD may initiate many years prior to the occurrence of clinical symptoms [11, 22]. A particularly important predisposing factor is chronic reduced cerebral blood flow [23, 24]. Thus, considerable effort is being directed toward the development of early detection techniques via monitoring saliva, serum, cerebrospinal fluid, neuroimaging biomarkers, and behavioral measures of cognitive dysfunction [25–31]. A drug designed to slow pathological changes, and thus major symptoms, would extend the patient’s quality of life and significantly reduce health care costs. de la Torre [32] has calculated that delaying disease onset by 5 years would reduce the number of diagnosed patients by upwards of 50%.
In this review we describe those components of the renin-angiotensin system (RAS) positioned to counter the damaging influence of angiotensin II (AngII) acting at the AT1 receptor on memory and cognition. When considering all brain RAS associated receptors and active peptides, it is the AngII/AT1 receptor system that has been linked to dysfunctions predisposing the onset of AD. By contrast there are RAS components positioned to oppose these changes including: AngIII/AT2 receptor, AngIV/insulin-regulated aminopeptidase (IRAP), AngIV/AT4 receptor, and the Ang(1–7)/Mas receptor. Each of these systems is described. We conclude with details concerning drug development strategies that may offer new treatments for AD patients by facilitating positive influences within the RAS.
ANGIOTENSIN II/AT1 RECEPTOR SYSTEM
The RAS is among the phylogenetically oldest hormone systems and is responsible for mediating several classic physiologies such as the regulation of systemic blood pressure and body water/electrolyte balance. The RAS has been a major focus regarding the development of antihypertensive drugs such as angiotensin converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs). This system also influences a number of novel physiologies and behaviors including sexual reproduction and behavior, cerebral blood flow and cerebroprotection, seizures, stress, depression, and memory (reviewed in [14]). The biologically active angiotensin peptides are derived from the protein angiotensinogen (255 amino acids) via a cascade of enzymatic activity and include AngII (Asp-Arg-Val-Tyr-Ile-His-Pro-Phe), AngIII (Arg-Val-Tyr-Ile-His-Pro-Phe), AngIV (Val-Tyr-Ile-His-Pro-Phe), Ang(1-7) (Asp-Arg-Val-Tyr-Ile-His-Pro) and Ang (3–7) (Val-Tyr-Ile-His-Pro) (Fig. 1 [33–35]). The RAS is a major contributor to many of the neurological factors seen in AD. Specifically, AngII binding at the G-protein coupled AT1 receptor subtype can facilitate dysfunctions that encourage the development of AD including sustained elevations in blood pressure, increases in oxidative stress and neuroinflammation, increased amyloid-β protein precursor mRNA, elevated β-secretase activity, reduced cerebral blood flow, and tissue remodeling that disrupts memory consolidation and retrieval [14, 36–45]. These deleterious influences can also result in the over activation of glutamate receptors resulting in neurotoxicity, increased neuronal Aβ protein levels, and tau phosphorylation [46]. These processes contribute to the “neuronal inflammatory response” [47–49].

The angiotensinogen-renin-angiotensin pathway indicating biologically active angiotensins (bold) enzymes, receptors and inhibitors that mediate angiotensin physiologies and behaviors. Angiotensin II and III bind at the AT1 and AT2 receptor subtypes. Angiotensin IV and Ang(3–7) bind at the AT4 receptor subtype. Angiotensin (1–7) binds at the Mas receptor. ACE, angiotensin converting enzyme; ACE2, angiotensin converting enzyme 2; AP-A, aminopeptidase A; AP-N, aminopeptidase N; ARBs, angiotensin receptor blockers; Carb-P, carboxypeptidases; PO, propyl oligopeptidase.
The first non-peptidic angiotensin receptor blocker (ARB) losartan was developed in 1995 [50]. Since then several additional ARBs have been introduced and successfully taken through clinical trials including candesartan, eprosartan, olmesartan, telmisartan, and valsartan [51, 52]. Azilsartan is the most recent to receive FDA approval in 2011 [53]. All are antihypertensive drugs designed to block the AT1 receptor subtype and reduce blood pressure. In addition, both losartan and candesartan have been shown to facilitate cognitive processing in elderly hypertensive patients [54–57].
The zinc-binding thiol compound captopril was the first angiotensin-converting enzyme inhibitor (ACEi) to be developed as an antihypertensive drug [58]. The major side effects of taste disturbances and skin rash were eliminated in most patients by the introduction of enalopril [59]. Several ACEi followed including benazepril, lisinopril, perindopril, quinapril, and ramipril [60, 61]. These drugs are designed to inhibit the conversion of AngI to AngII and reduce activation of the AT1 receptor subtype resulting in a sustained decrease in systemic blood pressure (Fig. 1). It has been shown that captopril and perindopril influence not only the peripheral but also the central RAS [62]. Along these lines, mild to moderate male hypertensive patients treated with captopril evidenced improved mental acuity, less sexual dysfunction, and an improved sense of wellbeing [63]. Amenta and colleagues [64] reviewed clinical trials results concerning the influence of anti-hypertensive treatments on cognitive processing in hypertensive patients. They concluded that ACEi improved cognitive functioning independent of blood pressure effects and superior to β-blockers and diuretics. Stabilization of cognitive performance by ACEi has also been noted in patients with MCI [65, 66]. Hajjar et al. [67] and others [68], have reported a slowed rate of cognitive decline in AD patients placed on ACEi. Further, Yasar et al. [69] noted a reduced risk to develop AD in patients treated with ACEi, ARBs, and diuretics. Recently, Ho and Nation [70] reported somewhat better results with ARBs than ACEi in older non-dementia adults.
These results indicate that controlling hypertension is a useful strategy for preventing the symptoms of AD and specifically reducing the tone of the AngII/AT1 system likely provides additional protective benefits. Despite these intriguing findings, there is a need to collect additional information on the potential beneficial cognitive effects of these drugs. While normotensive individuals at risk to develop MCI and AD may appear to be poor candidates for treatment with ARBs or ACEi for fear of hypotensive effects, such an investigation may be worth considering. Also, at present there is minimal information concerning the potential effectiveness of these drugs at preventing the onset and progression of AD. However, there are two ongoing clinical trials. One is evaluating the ability of losartan, in combination with current therapies, to slow disease progression in mild to moderate AD patients. The other is focused on the efficacy of telmisartan versus an ACEi at reducing ventricular enlargement in AD patients [71]. For thoughtful reviews concerning how these drugs were developed and their chemical structures and targets beyond cardiovascular disease, the reader is referred to the following reviews [60, 73]. As indicated above, the negative influences of the AngII/AT1 receptor subtype system may be offset by other angiotensin ligands acting at their receptor subtypes. These are next described.
ANGIOTENSIN III/AT2 RECEPTOR SYSTEM
In common with the AT1 receptor subtype the AT2 subtype is a 7-transmembrane domain G-protein coupled receptor; however, it exhibits only about 32–34% amino acid sequence identity with the AT1 receptor. Although AngII binds at the AT2 receptor, this protein has a higher affinity for AngIII. The AT2 receptor is maximally expressed in developing fetal tissues but decreases after birth and remains at low levels in adult tissues (Fig. 2) [74–76]. The AT2 receptor subtype appears to modulate cell proliferation, cell differentiation, and apoptosis, as well as regenerative processes and generally opposes actions initiated by the AngII/AT1 system [77, 78]. It is important to note that the AT2 receptor can be upregulated during pathological conditions [79, 80], although it is not clear to what extent this occurs in AD patients. It has yet to be determined whether the AT2 receptor is present in sufficient numbers in brain structures associated with cognitive functioning to warrant the clinical development of metabolically stabilized AngIII analogs as AD therapeutics. The development of a non-peptidic AngIII agonists with extended half-lives that penetrate the blood-brain barrier (BBB) would be a considerable technical challenge.
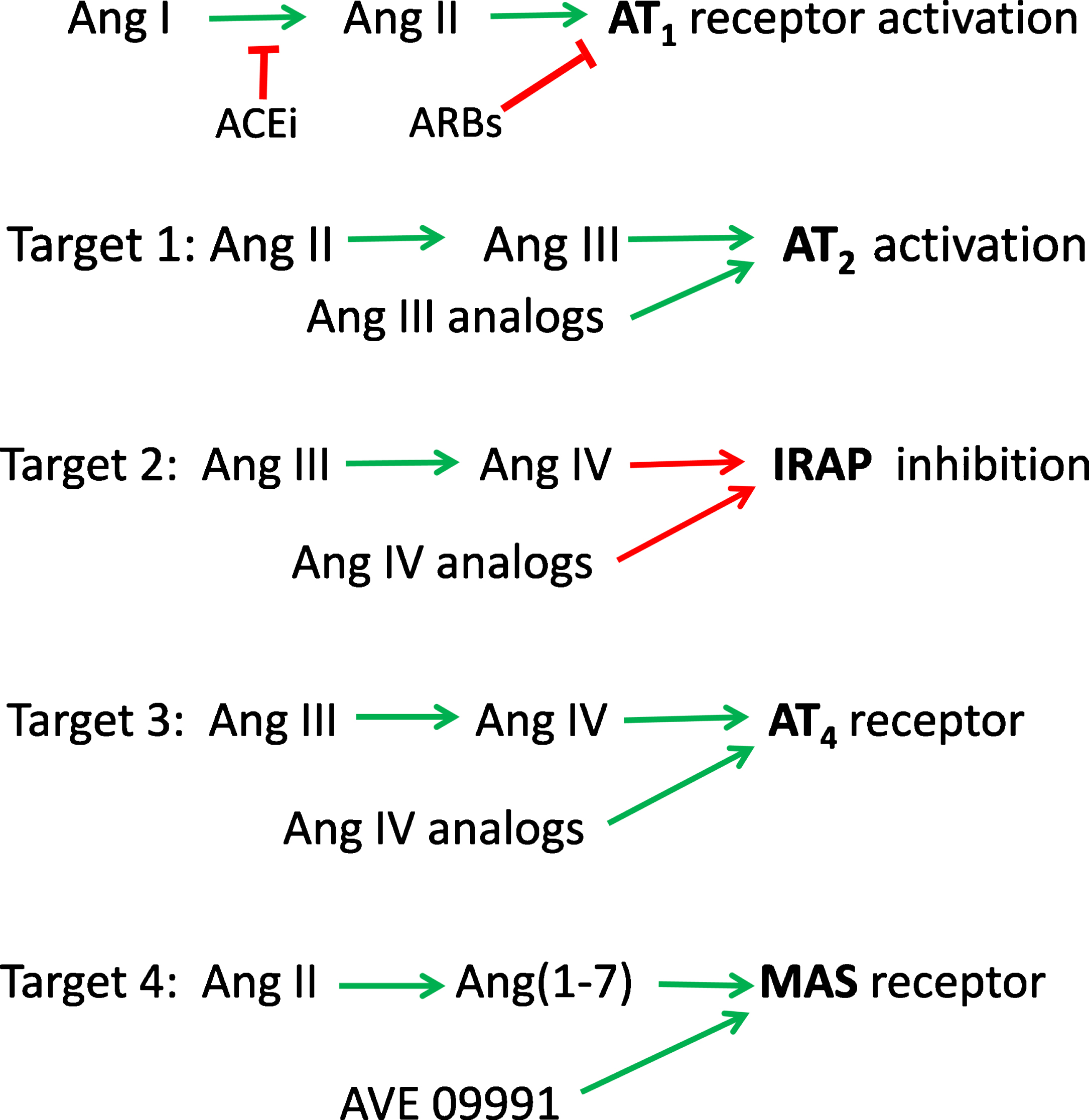
Possible pharmacological targets to offset the deleterious effects of an overactive Ang II/AT1 receptor subtype system. Target 1: activation of the AT2 receptor by AngIII (and AngIII analogs) to initiate cellular proliferation and differentiation accompanied by regenerative processes. Target 2: AngIV acts at IRAP to inhibit this enzyme resulting in the potentiation of several memory enhancing peptides including AngIV, vasopressin, oxytocin, somatostatin and cholecystokinin-8. Target 3: AngIV (and analogs) act at the AT4 subtype resulting in facilitated cerebral blood flow, increased neuroprotection, synaptogenesis and LTP thus promoting memory consolidation and retrieval. Target 4: Ang(1–7) (and analogs) act via the Mas receptor to encourage the release of nitric oxide promoting anti-thrombosis and facilitated LTP resulting in enhanced memory.
ANGIOTENSIN IV/INSULIN-REGULATED AMINOPEPTIDASE
A potentially important advance in our understanding of the RAS was the finding that AngIV’s actions may be mediated in part by IRAP (EC 3.4.11.3) and the hypothesis that this enzyme is the AT4 receptor [81, 82]. IRAP is a Type 2 transmembrane protein of the gluzincin aminopeptidase family which includes homologous aminopeptidases such as aminopeptidases A (AP-A, EC 3.4.11.7) and N (AP-N, EC 3.4.11.2) (reviewed in [60, 83]). IRAP co-distributes with the GLUT4 transporter [84, 85]. IRAP has been variously identified as oxytocinase, cysteine aminopeptidase, placental leucine aminopeptidase, gp160, and vp165 [86]. The key substrates acted upon by this enzyme are arginine-vasopressin and oxytocin [87], although IRAP has the capacity to cleave N-terminal amino acids from additional peptides including met-enkephalin, dynorphin, lysine-bradykinin, neurokinin A1, somatostatin, neuromedin B, and cholecystokinin-8. Thus, IRAP inhibition by AngIV results in the potentiation of several pro-cognitive endogenous peptides including arginine-vasopressin, oxytocin, somatostatin and cholecystokinin-8 [88]. In a recent report [89], an absence of IRAP in the postnatal forebrain of a neuron-specific IRAP knockout mouse line was linked with dysfunctions in spatial and object recognition memory. Although these data are in conflict with the notion that AngIV’s pro-cognitive effects are the result of reduced IRAP activity, they nonetheless support an important role for IRAP in memory.
IRAP inhibitors (e.g., LVVhaemorphin7) have shown preclinical promise in enhancing memory on tasks used to evaluate the performance of animal models [9, 90]. Several specific inhibitors to IRAP have been developed that enhance spatial memory and fear avoidance in animal models [9, 91]. Andersson and Hallberg [60] have been particularly successful in designing and synthesizing IRAP inhibitors. Also, IRAP knockout mice have been shown to suffer significantly reduced cerebral infarct volume 24 hours following a 2-hour transient cerebral artery occlusion as compared with wild type mice [92]. These results were attributed to an increase in compensatory cerebral blood flow during the occlusion process. A growing research literature on IRAP strongly indicates that it is an important target regarding the treatment of ischemic stroke as well as AD.
ANGIOTENSIN IV/AT4 RECEPTOR SYSTEM
Several years ago, our laboratory, and others, discovered a binding site with nanomolar affinity for AngIV using bovine adrenal cortex membranes [93–95] and guinea pig hippocampal tissues [96]. The pharmacological profile of this receptor was shown to be distinct from the AT1 and AT2 subtypes. It was also determined that [125I]-AngIV binds at the AT4 site reversibly, saturably, and with high affinity. Binding was found to be insensitive to guanine nucleotides, indicating that this receptor protein is not G-protein-linked. Further, the AT4 receptor evidenced as a dimer, as seen in growth factors, with a molecular weight of 160–190 kDa as determined by reduced SDS-polyacrylamide gel electrophoresis (reviewed in [97]). Recently we have noted an interaction between AngIV-based analogs and the hepatocyte growth factor (HGF)/Met system with evidence suggesting that the AngIV/AT4 receptor system coincides with the HGF/Met receptor system [45]. This subtype is distributed within a number of brain structures with heavy concentrations in the hippocampus, nucleus basalis of Meynert, piriform cortex and neocortex, structures concerned with the mediation of cognition, learning and memory (reviewed in [83]).
The AT4 receptor subtype has a positive influence on a number of physiological and behavioral functions including cerebral blood flow (CBF), neuroprotection, synaptogenesis, long-term potentiation (LTP), and memory consolidation and retrieval [14, 45]. Braszko and colleagues [98, 99] were the first to report that intracerebroventricular injected AngIV facilitated exploratory behavior in rats tested in an open field, and improved recall of passive avoidance conditioning and the memory acquisition of active avoidance conditioning. This laboratory has further determined that L-type and T-type voltage-gated calcium channels mediate AngIV activation of AT4 receptors and the facilitative effects of this peptide on recall during object recognition and inhibitory avoidance conditioning tasks [100]. Members of our laboratory confirmed these memory enhancing results and further reported AngIV-induced dose dependent increases in CBF without significant changes in systemic blood pressure [101, 102]. These effects could not be blocked by AT1 or AT2 receptor antagonists, but were prevented by pretreatment with the AT4 receptor antagonist divalinal. Related to this, Naveri and colleagues [103] have shown that AngIV infusion restored CBF following subarachnoid hemorrhage. Further, Dalmay et al. [104] reported that AngIV infusion following pretreatment with the AT1 receptor blocker candesartan slightly decreased mortality at post-surgery Day 3 in the gerbil model of unilateral carotid artery ligation, but significantly decreased lisinopril-induced mortality. These results support the hypothesis that the activation of AT4 receptors contributes to cerebroprotection. This neuroprotective role is consistent with the notion that AngIV increases blood flow by a nitric oxide (NO)-dependent mechanism [100]. In agreement with this hypothesis, Faure et al. [105] has shown that internal carotid artery administration of increasing doses of AngIV significantly decreased mortality and cerebral infarct size in rats 24 hours following embolic stroke due to the intracarotid injection of calibrated microspheres. Pretreatment with divalinal abolished this protective effect. Sequential cerebral arteriography indicated that AngIV facilitated the redistribution of blood flow to ischemic areas within a few minutes. It is hypothesized that AngIV may yield its neuroprotective effect against acute cerebral ischemia via an intracerebro-hemodynamic AT4 receptor-mediated NO-dependent mechanism.
There is now substantial evidence that the AngIV/AT4 receptor system is critically involved in memory formation and may overcome the memory inhibiting influences of AngII [45, 106–109]. Early on a positive role for AngII in the facilitation of memory and cognition was proposed (reviewed in [74, 109–111]); however, subsequent animal studies indicated that intracerebroventricular delivery of AngII interfered with performance on most memory tasks used with animal models (reviewed in [14]). Initially there were difficulties in evaluating the role of AngIV in memory formation given that endogenous AngIV has a short half-life and thus appears to be over powered by AngII levels. In an effort to develop an AngIV analog, members of our laboratory initially synthesized a number of AngIV-based compounds possessing extended half-lives [112, 113]. This resulted in the development of two potent receptor antagonists, divalinal and Norleual-AngIV [114–117], and one promising agonist, Nle1-AngIV. We determined that the memory facilitating effects of Nle1-AngIV derived from its N-terminal region given that fragments as small as tetra- and tripeptides retained the ability to overcome scopolamine-induced amnesia in animal models [109, 118]. Further, Nle1-AngIV, as well as these shorter fragments, augmented hippocampal synaptic connectivity via the formation of new synapses [118]. Functionality of these synapses was established via evidence of analog-induced spinogenesis and the colocalization of synaptic markers in newly formed dendritic spines which were coupled with enhanced miniature excitatory postsynaptic currents. These results encouraged the possibility that a clinically useful non-peptidic small molecule could be designed possessing increased metabolic stability with an extended half-life, and BBB penetrability offering facilitated cognitive functioning. Subsequent design and synthesis efforts yielded a small molecule with increased hydrophobicity, decreased hydrogen bonding potential, and significantly increased metabolic stability, dihexa. This compound induces spinogenesis and synaptogenesis at picomolar concentrations, is slowly cleared from the blood (plasma stability t1/2 = 5–6 hours) and can be delivered via parenteral routes of administration [119]. Dihexa binds with high affinity to HGF and stimulates dimerization, a prerequisite to binding at the Met receptor. Dihexa induces Met phosphorylation in the presence of subthreshold levels of HGF. It also stimulates hippocampal spinogenesis and synaptogenesis equivalent with HGF [118, 120]. Further, dihexa penetrates the BBB in sufficient quantity to facilitate memory consolidation and retrieval in the scopolamine-induced amnesic rat model of AD, as well as in aged rats employing the Morris water maze task of spatial memory (reviewed in [14]). The reader is referred to the following excellent reviews concerned with detailed characterization of the angiotensin receptor subtypes [121, 122].
ANGIOTENSIN (1–7)/Mas RECEPTOR SYSTEM
Ang(1–7) binds at the G-protein-coupled Mas receptor and this system has been shown to counteract peripheral organ inflammation and fibrosis, increase glucose utilization, and decrease insulin resistance [123–126]. The Mas receptor is present in brain structures associated with memory and cognition including hippocampal and piriform cortices [127]. Consistent with these observations Ang(1–7) has been shown to facilitate LTP, a presumed building block of memory formation, in the CA1 region of the hippocampus [125]. Further, Ang(1–7) has been shown to improve memory while blockade of the Mas receptor reduced fear associated memory recall [107].
Increased activation of the Ang(1–7)/Mas receptor system has been shown to stimulate the release of NO from vascular endothelial and smooth muscle cells thus opposing both AngII and vasopressin-induced vasoconstriction [128, 129]. This peptide also protects cardiac and endothelium functioning as well as coronary perfusion as demonstrated in heart failure models [130]. It is of interest that Ang(1–7) has been shown to facilitate baroreceptor reflex sensitivity and modulate circadian rhythm influences on heart rate and blood pressure [131, 132]. It is well established that AngII promotes thrombosis primarily via expression of plasminogen activator inhibitor 1 [133, 134]. Kucharewicz and colleagues [135, 136] have reported that Ang(1–7) functions as an antithrombotic agent when administered to renal hypertensive rats that served as a venous thrombosis model. A first step toward the use of this peptide to offset AngII’s influence has been accomplished with the development of a non-peptidic Ang(1–7) analog, AVE09991 [137]. However, much additional preclinical testing will be required to establish this system’s relative importance regarding AD.
CONCLUDING REMARKS
The ability of cholinesterase inhibitors to treat AD has been disappointing, while patients given memantine have shown some improvement [138]. Although the RAS plays a central role in mediating many of the factors predisposing patients to MCI and AD, clinical exploration of this system has been minimal. The AngII/AT1 receptor system is a major contributor to the “neuronal inflammatory response”, a collection of dysfunctions predisposing the onset of neurodegenerative diseases. The most promising approaches to counter these factors are the use of ARBs and ACEi to reduce activation of the AngII/AT1 system, and the use of compounds to inhibit IRAP, and AngIV analogs to activate brain AT4 receptors. There is evidence that hippocampal AT4 (Met) receptor numbers are significantly decreased in AD patients [139], accompanied by decreases in serum aminopeptidases A, B, N, and IRAP [140]. Kehoe and colleagues [141] have reported that both AngII and AngIII levels were significantly elevated in AD postmortem mid-frontal cortex tissue as compared with age-matched controls. AP-A levels were decreased in AD, while AP-A enzyme activity was equivalent. AP-N activity was reduced in AD tissue, while AP-N protein level was unchanged. Aminopeptidases A and N are essential for the synthesis of AngIII and AngIV, respectively. The reduction in AP-N activity may suggest decreased synthesis of AngIV in these patients. Perhaps AngIV analogs could be used to counter these changes and facilitate neuronal functioning and reduce apoptosis in memory associated brain structures. Members of our laboratory have developed stable non-peptidic AngIV analogs capable of activating the AT4 receptor subtype. Our lead compound, dihexa, penetrates the BBB, encourages the formation of new functional synaptic connections, and promotes neuroprotection and the replacement of damaged neurons from available neural stem cell populations. This drug has also demonstrated the ability to facilitate LTP in hippocampal slices and overcome the memory losses seen in animal models of AD.
Footnotes
ACKNOWLEDGMENTS
All experiments utilizing animal models conducted in our laboratory and referred to in this review adhered to the Guidelines for the Care and Use of Laboratory Animals as required by the National Institutes of Health (NIH Publication No. 80–23), and the protocols were approved by the Washington State University Institutional Animal Care and Use Committee. The preparation of this paper was supported by the Michael J Fox Foundation, and the Alzheimer’s Drug Discovery Foundation. Drs. Wright and Harding are co-founders of M3 Biotechnology, Inc. and hold stock in this company which is involved in the development of drugs to treat Alzheimer’s and Parkinson’s diseases. No funds from this company were used to conduct the animal research presented in this manuscript or in the preparation of this manuscript.